
Abstract
Objective:
Rates of suicidality are higher in military than comparable civilian populations. The period of transition from regular military service may be a time of particular vulnerability. In order to best inform early intervention and prevention strategies, we sought to investigate the childhood determinants (trauma and disorder) of self-reported past-year suicidality (thoughts, plans or attempts) in a population of Australian Defence Force men who had recently (in the previous 5 years) transitioned from regular military service.
Methods:
We analysed self-report, and detailed interview, cross-sectional data to investigate the association between retrospectively reported past-year suicidality and childhood factors (disorder and trauma) and whether these relationships were independent of each other and adult-onset trauma and disorder. We utilised logistic regression techniques and generalised structural equation modelling.
Results:
The prevalence of suicidality in transitioned men was 21.6% (95% confidence interval [CI]: [19.9, 23.3]). Suicidality was associated with childhood-onset interpersonal trauma and anxiety and adult-onset anxiety and depression. Generalised structural equation modelling demonstrated that the pathway between childhood interpersonal trauma and suicidality was not fully mediated by childhood anxiety. Restricting the analyses to those previously deployed demonstrated that suicidality had a direct and significant association with childhood-onset factors (anxiety and interpersonal trauma) and adult-onset trauma (deployment and non-deployment related).
Conclusion:
This study sheds light onto the significance of childhood factors (interpersonal trauma and anxiety) in a population undergoing transition that may revive pre-existing vulnerabilities. These findings have the potential to aid early intervention and prevention strategies in identifying those at risk prior to transition. These findings also imply that early interventions targeting anxiety and interventions to reduce social instability during the transition period may be useful in reducing suicidality during this time. Further prospective studies are needed to further explore these novel findings.
Keywords
Background
The impact of military service on mental health and suicidality are a focus for research internationally (Gradus et al., 2013). Between 2001 and 2015, there were 325 certified suicide deaths among serving or ex-serving Australian Defence Force (ADF) personnel, of which 93% (303 deaths) were men. Rates of death by suicide were substantially higher in ex-serving than in those currently serving in the ADF (Australian Institute of Health and Welfare [AIHW], 2017). Studies in the United States demonstrate that the rate of death by suicide in veterans has increased in recent years (Bruce and Laporte, 2015).
While suicide itself is a rare outcome, it is strongly predicted by the broader measure of suicidality (suicidal thoughts, plans and attempts). Research on suicidality in military populations (Kuehn, 2009) has traditionally concentrated on occupational risk factors. However, several studies have not found a significant impact of deployment (Kang et al., 2015; LeardMann et al., 2013; Schoenbaum et al., 2014). It is possible, therefore, that other factors also impact the rates of suicidality in military personnel (Afifi et al., 2016).
The period of transition from military to civilian life is becoming recognised as a particularly stressful period in the life of military personnel but remains an emerging field of international research (Shields et al., 2016). For example, it is as yet unclear how childhood and military factors interact to determine suicidality in transitioning military populations. However, an improved understanding of these potentially important aetiological factors is likely to prove a fruitful avenue to better inform early intervention and prevention strategies in these populations. Especially the possibility that people with vulnerabilities can be identified before leaving regular military service to ensure adequate social and health service provision (Syed Sheriff et al., 2020a).
Previous research demonstrated that the proportion of ADF men reporting suicidality (3.78%, 95% confidence interval [CI]: [3.70, 3.87]) was higher than the proportion of employed civilian men reporting suicidality (1.42%, 95% CI: [0.87, 1.99]) (Syed Sheriff et al., 2019b). Suicidality was associated with childhood interpersonal trauma, high loads of childhood trauma, high loads of adult trauma and childhood-onset anxiety. In ADF men (but not civilian employed men), childhood anxiety fully mediated the relationship between childhood trauma and past-year suicidality. However, this previous study was unable to shed light on the rates and determinants of suicidality in transitioning military populations.
As in previous studies (Syed Sheriff et al., 2019a, 2019b), due to marked sex differences in non-lethal suicidal behaviour rates (Nock et al., 2014; Ursano et al., 2015), and the relatively low number of females in the ADF, which limited statistical power, we confined analyses in this current paper to men, as in previous studies (Syed Sheriff et al., 2019a, 2019b, 2019c, 2020b). We aimed to analyse the associations between childhood trauma and childhood disorder and suicidality in a sample of recently transitioned ADF men. In addition, we aimed to investigate whether the associations between childhood factors and past-year suicidality were independent of deployment trauma, in those who had been previously deployed. We also aimed to examine mediator pathways from childhood trauma to suicidality via childhood anxiety. We hypothesised that elucidation of these associations would provide vital information to better inform early intervention and prevention strategies.
Method
Procedure
This analysis utilised data from the Transition and Wellbeing Research Programme (the Programme), a comprehensive research programme undertaken to establish the prevalence of mental disorders in a representative cohort of ADF members who transitioned out of regular ADF service between 2010 and 2014. The methodologies utilised in this study are described in more detail elsewhere (Van Hooff et al., 2018).
However, in brief, ethical approval for the Programme was provided by the DVA Human Research Ethics Committee (E014/018). Ethical approval for this particular analysis was provided by the Departments of Defence and Veterans Affairs Human Research Ethics Committee (057-18). Data were collected in 2015–2016. The sample was drawn from the Military and Veteran Research Study Roll generated for the Programme and held at the AIHW. The Study Roll was generated using identifying information from Defence and DVA and contact details from ComSuper and cross-referenced against the National Death Index. All potential participants were given the opportunity to opt out of the study roll, prior to study commencement. Contact information for those who did not opt out was passed on to the University of Adelaide and used to invite study participants to enrol in the research. Participants were informed that neither DVA nor Defence would have access to their study data nor be informed of their decision regarding participation. This provided participants with an additional degree of certainty that their responses would not affect their employment or compensation entitlements. The DVA and Defence were, however, able to access de-identified data.
The Programme utilised a two-phase design. At Phase 1, transitioned ADF members were screened for mental health problems using a 60-minute self-report questionnaire, online or in hard copy. This questionnaire included items relating to previous deployment, deployment trauma and suicidality as well as demographic and service factors.
At Phase 2, a sub-sample of Transitioned ADF members surveyed in Phase 1 were selected to participate in a 1-hour diagnostic telephone interview using the World Mental Health Survey Initiative Version of the World Health Organization Composite International Diagnostic Interview – version 3.0 (CIDI) (Kessler and Ustun, 2004). This instrument was chosen because it is widely used in epidemiological surveys worldwide and is fully structured. The Hunter Research Foundation conducted the interviews. All interviewers were trained in the computer-assisted personal interview version of CIDI and had experience working with veterans. Selection for this interview was based on strata derived from rank, sex, Service and scores on the Post-traumatic Stress Disorder Checklist (PCL) and the Alcohol Use Disorders Identification Test (AUDIT).
Weighting and stratification
Basic demographic characteristics to be used in weighting were held for both respondents and non-respondents by the AIHW until the end of the data collection. These data were then provided to researchers in either identified or de-identified form, depending on participation and consent status in order to allow the data from respondents to be weighted up to the entire population.
All survey data for the Transitioned ADF was weighted using distinct strata for sex, Service, rank and medical fitness. CIDI weights were derived for the Transitioned ADF, based on strata including band (cut-offs were based on PCL and AUDIT), sex and Service. Post-stratification by the variables of sex, Service and rank were used to adjust the weights so that the known population totals were reproduced by the estimates, and to correct for differential non-response by rank.
Sample
Out of a total of 21,671 men who transitioned between 2010 and 2014, 20,713 were invited, and 3646 (17.6%) completed the self-report questionnaire. Those not invited represented individuals who may have opted out of the study or did not have any usable contact information and included those who transitioned into the Active and Inactive Reserves as well as those who had discharged completely from the Current ADF (Ex-Serving). All individuals were given the opportunity to opt out of being invited to participate in the research. A total of 1511 men were selected for a CIDI interview and 901 (59.6%) completed it.
Variables
Demographic and service characteristics
Information regarding demographics (age, highest educational attainment and relationship status) and previous deployments were obtained from the self-report questionnaire completed at Phase 1. Information regarding service characteristics was available from ADF administrative data. Military ranks were grouped into three categories: other ranks (Private to Corporal equivalents), Non-Commissioned Officers (NCOs) (Sergeant to Warrant Officer equivalents), and Commissioned Officers (COs) (Lieutenant to General equivalents).
Suicidality
The self-report questionnaire included the following specific questions regarding suicidality:
In the last 12 months, have you ever felt so low that you thought about committing suicide?
In the last 12 months, have you made a suicide plan?
In the last 12 months, have you attempted suicide?
The variable, ‘past-year suicidality’ comprised those who responded yes to any of these three questions.
Deployment trauma
Deployment trauma exposure was calculated as the sum of 12 traumatic deployment exposure items from the self-report questionnaire. Previously, similar trauma count variables have shown consistent significant associations with mental disorder outcomes (Sareen et al., 2013).
Childhood trauma
Childhood trauma variables were collected from the CIDI interview as part of the post-traumatic stress disorder (PTSD) module. All ‘criteria A’ events listed in the CIDI were examined. Childhood trauma refers to trauma types with a reported age of onset below the age of 18 years. We used mutually exclusive categorisation of childhood trauma utilised in numerous previous studies (Syed Sheriff et al., 2019a, 2019b, 2019c, 2020c). ‘Interpersonal’ childhood trauma included those reporting the following trauma types: sexual assault, raped, stalked, kidnapped, mugged, beaten by spouse/romantic partner and badly beaten by anyone else (these are abbreviations of the listed criteria A events). ‘Non-Interpersonal’ childhood trauma included those who reported the following trauma types (in the absence of interpersonal trauma): life-threatening automobile accident, other life-threatening accident, natural disaster, man-made disaster and life-threatening illness. ‘Other’ childhood trauma included those who reported the following trauma types (but neither non-interpersonal nor interpersonal trauma types): combat, refugee, peacekeeper, someone close died unexpectedly, someone close had traumatic experience, saw atrocities or carnage, experience don’t want to talk about, unarmed civilian in a place of conflict, lived as a civilian in a place of ongoing terror, accidentally injured/killed someone, saw someone badly injured/killed, child illness, and purposefully injured or killed someone else.
Adult-onset non-deployment-related trauma
Adult-onset trauma variables were also collected from the CIDI interview as part of the PTSD module. Adult trauma included trauma types which first occurred at the age of 18 years or older. As data regarding deployment trauma were taken from the self-report questionnaire, we separated out trauma types unlikely to be deployment related, as per a previous study (Frank et al., 2018). These non-deployment-related traumas were further categorised as ‘Interpersonal’ (sexual assault, raped, stalked, beaten by spouse/romantic partner, badly beaten by anyone else) or ‘Non-interpersonal/other’ (unarmed civilian in a place of conflict, lived as a civilian in a place of ongoing terror, refugee, life-threatening automobile accident, child illness, life-threatening illness, someone close had traumatic experience).
Mental disorder
The CIDI was utilised to examine mental disorder prevalence. The CIDI consists of a structured diagnostic assessment of lifetime, 12-month and 30-day ICD-10 (International Classification of Diseases) disorder. Past-year disorder was assessed based on standard CIDI algorithms with ICD hierarchical rules applied. Childhood disorder was defined as disorder with age of onset below 18 years and was grouped as follows: any depression (mild, moderate or severe depressive episode), any anxiety (social phobia, Obsessive Compulsive Disorder, Generalised Anxiety Disorder, agoraphobia, panic attack, panic disorder, PTSD) and any alcohol use disorder (abuse or dependence). Those who had a past-year, 30-day or lifetime anxiety disorder, but no childhood anxiety disorder, were coded as having adult-onset anxiety disorder. Coding was performed in a similar way for adult-onset depression and adult-onset alcohol use disorders.
Analysis
All analyses were performed in STATA version 14.2. Descriptive analyses were utilised to describe demographic and service characteristics as well as trauma and mental disorder and analyse associations with past-year suicidality of the male transitioned population.
Logistic regression analyses were utilised to calculate the association of past-year suicidality with childhood trauma, controlling for demographic (age, education and relationship status) and service (service and rank) factors as well as previous deployment (Model 1). We then also controlled for adult trauma (Model 2) and childhood- and adult-onset disorder (Model 3).
We then restricted our analyses to the previously deployed population only and carried out similar descriptive statistics as for the entire male transitioned population. We then conducted logistic regression analyses in order to assess whether the association between past-year suicidality and childhood factors were independent of adult trauma (deployment and non-deployment related).
We examined mediator pathways via childhood anxiety between childhood trauma and past-year suicidality using logistic regression models. As the outcome of interest was dichotomous, we utilised generalised structural equation modelling (GSEM) to assess mediation by childhood-onset disorder. The GSEM pathway utilised the link ‘logit’ and the family ‘Bernoulli’ within STATA. First, we calculated associations between childhood trauma and suicidality. We then reran the GSEM analysis adding childhood-onset anxiety as a mediator (Acock, 2006). The total indirect pathways were calculated utilising the ‘nlcom’ command which calculates nonlinear combinations of estimators (StataCorp, 2013).
Results
The prevalence of suicidality was very high (21.6%, 95% CI: [19.9, 23.3]) (see Table 1). Most participants reported experiencing childhood trauma. About a quarter reported at least one type of interpersonal trauma in childhood. Almost a third (28.7%, 95% CI: [24.1, 33.7]) experienced a childhood disorder, by far the most common category of which were anxiety disorders (21.1%, 95% CI: [17.1, 25.6]).
ADF transitioned men, characteristics and associations with any suicidality.
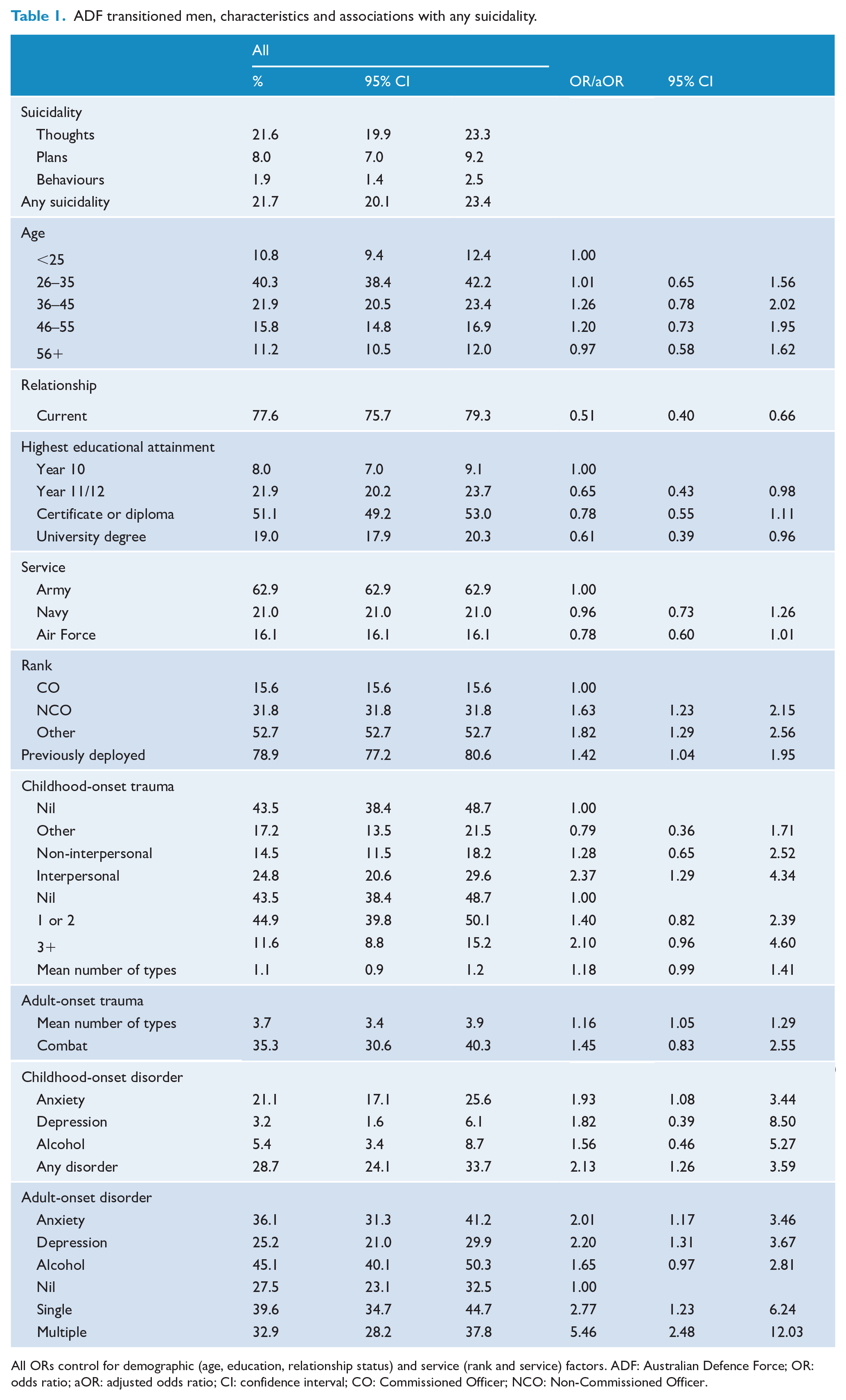
All ORs control for demographic (age, education, relationship status) and service (rank and service) factors. ADF: Australian Defence Force; OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval; CO: Commissioned Officer; NCO: Non-Commissioned Officer.
Most participants had been previously deployed (78.9%, 95% CI: [77.2, 80.6]). The vast majority (92.2%, 95% CI: [88.3, 94.9]) experienced at least one type of new trauma in adulthood. Most participants also reported the onset of a category of mental disorder in adulthood (72.5%, 95% CI: [67.3, 76.9]).
Controlling for other demographic and service factors, past-year suicidality was associated with being single, lower educational attainment, being an NCO or other rank, and being previously deployed. Past-year suicidality was also associated with childhood interpersonal trauma (but not other types of childhood trauma or even the number of types of childhood trauma) and childhood-onset anxiety. Past-year suicidality was associated with adult-onset anxiety and depression (but not alcohol use disorders). Past-year suicidality was associated with adult-onset trauma types, including both non-deployment non-interpersonal and interpersonal trauma and adult combat (see Table 1).
Logistic regression analyses demonstrated that even controlling for adult-onset trauma types, and previous deployment, childhood interpersonal trauma had a direct and significant association with past-year suicidality. In the final model (Model 3) when also controlling for childhood and adult-onset disorders, childhood anxiety as well as childhood interpersonal trauma had a direct and significant association with past-year suicidality. Adult-onset anxiety and depression were also associated with past-year suicidality whereas adult-onset trauma types were no longer associated with past-year suicidality (see Table 2).
Regression analysis for any suicidality in transitioned ADF men.
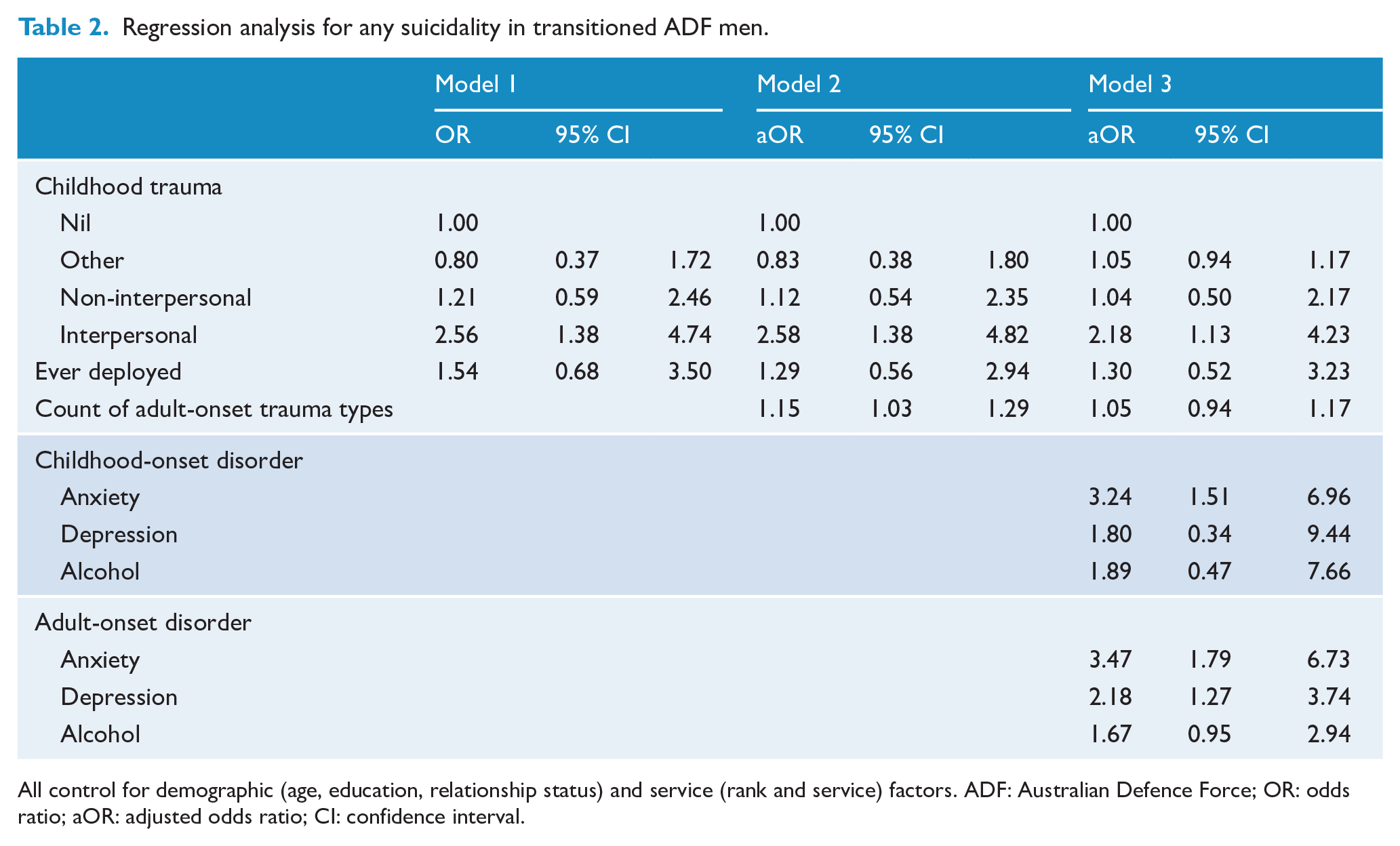
All control for demographic (age, education, relationship status) and service (rank and service) factors. ADF: Australian Defence Force; OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
GSEM demonstrated that there was a direct and significant association between childhood interpersonal trauma and past-year suicidality. When childhood-onset anxiety was added as a mediator, a significant pathway remained between childhood interpersonal trauma and past-year suicidality but was of a smaller magnitude. The pathway via childhood anxiety was significant, suggesting the possibility of partial but not full mediation (see Figure 1).
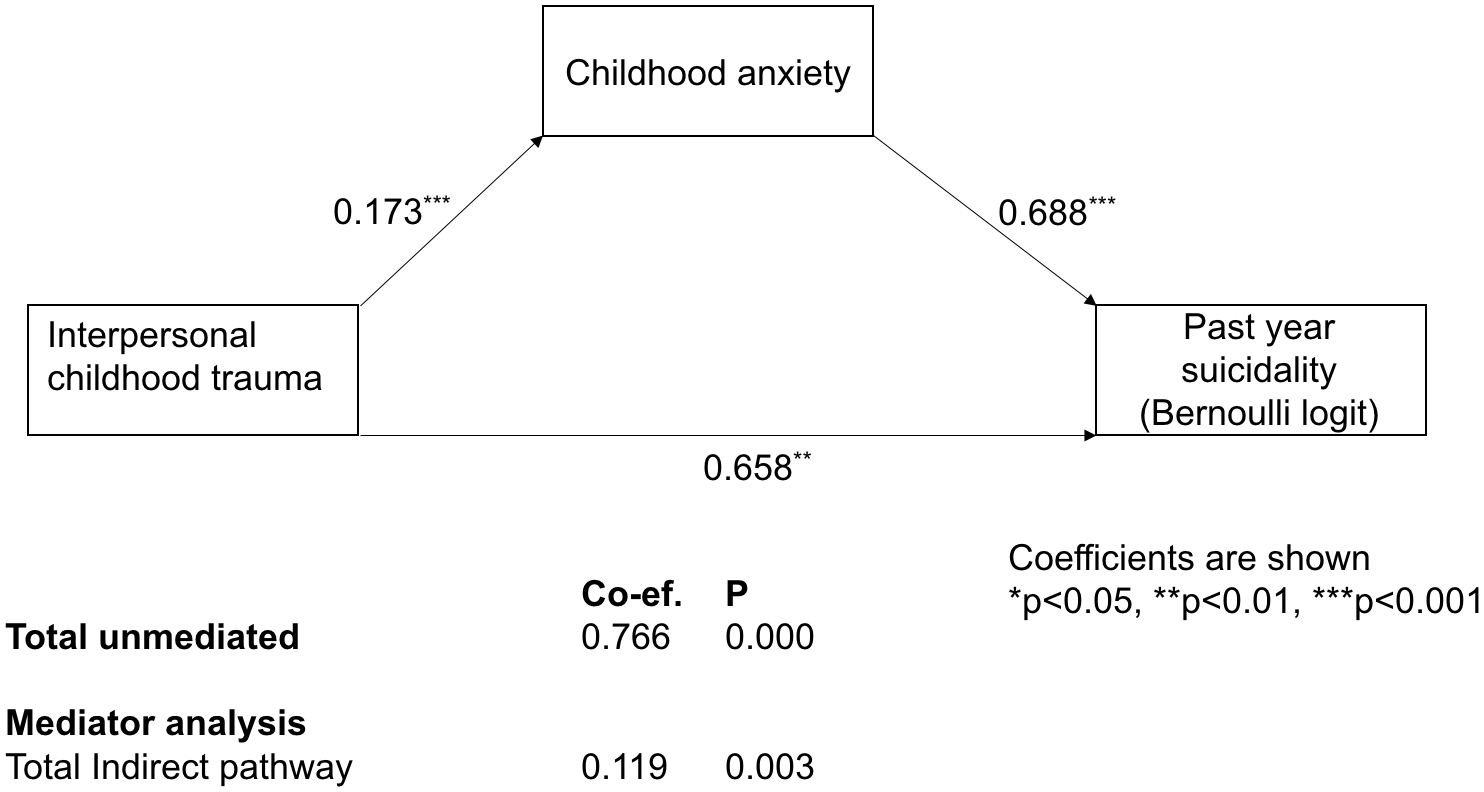
Mediator analysis through childhood anxiety, controlling for demographics (age, education and current relationship status) and service factors (rank, service, previous deployment).
As most of the transitioned male population reported that they had been previously deployed when we restricted the analyses to previously deployed only, the population characteristics remained broadly similar (see Table 3). However, in the previously deployed population, controlling for demographic and service factors, there was no association of past-year suicidality with either educational attainment or service. Past-year suicidality was associated with being single, and with being an NCO or Other rank (rather than a CO). Past-year suicidality was associated with childhood-onset anxiety and adult-onset disorders (anxiety, depression and alcohol). Past year suicidality was also significantly associated with deployment trauma and non-deployment trauma (multiple types) in adulthood (see Table 3).
Previously deployed ADF transitioned men associations with any suicidality.
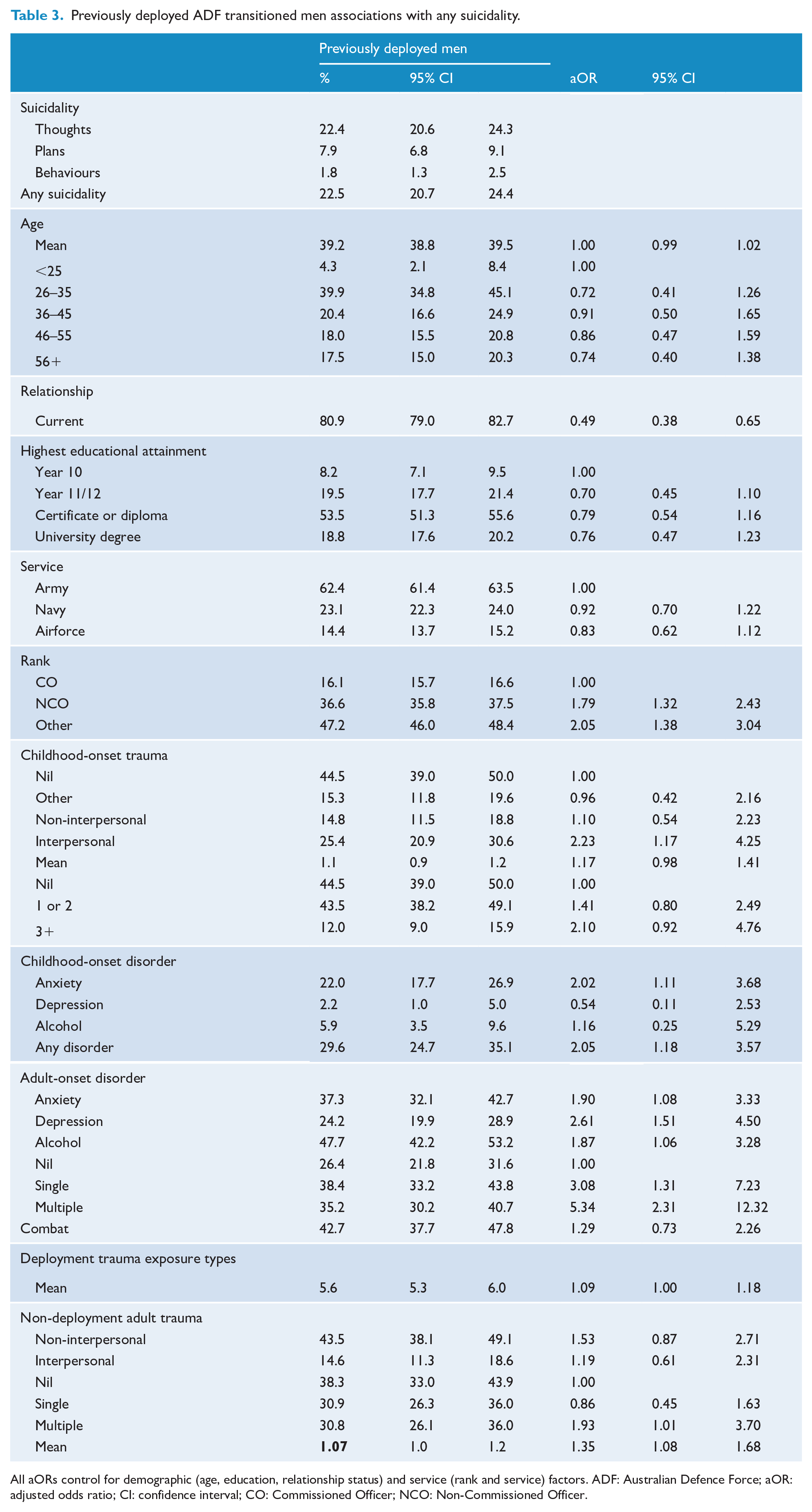
All aORs control for demographic (age, education, relationship status) and service (rank and service) factors. ADF: Australian Defence Force; aOR: adjusted odds ratio; CI: confidence interval; CO: Commissioned Officer; NCO: Non-Commissioned Officer.
Logistic regression analyses demonstrated that controlling for adult deployment and non-deployment trauma types (Model 1), childhood interpersonal trauma had a direct and significant association with past-year suicidality. In the fully adjusted model adult-onset trauma, (deployment trauma exposure and other types of adult trauma) appeared to have a weak but significant association with past-year suicidality. Childhood interpersonal trauma and childhood anxiety had a direct and significant association with past-year suicidality (see Table 4).
Regression analysis for any suicidality in previously deployed transitioned men.
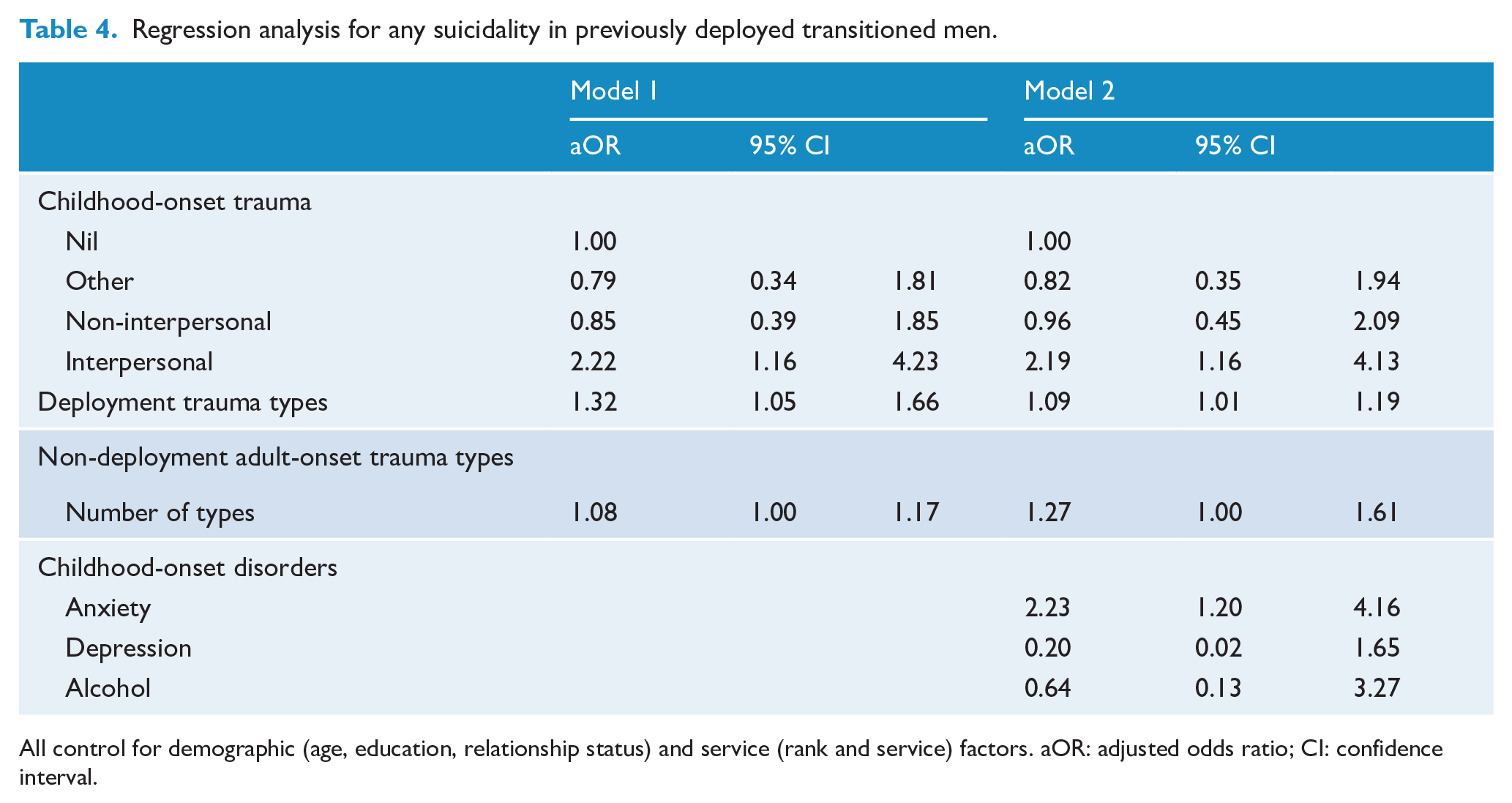
All control for demographic (age, education, relationship status) and service (rank and service) factors. aOR: adjusted odds ratio; CI: confidence interval.
Discussion
There are concerningly high rates of suicidal ideation and attempts in recently transitioned ADF males. Several factors which are associated with suicidality are common in this population and are potentially identifiable early, such as childhood interpersonal trauma and childhood-onset anxiety. In contrast to previous research in the regular ADF (Syed Sheriff et al., 2019b), it does not appear that childhood anxiety fully mediated the relationship between childhood trauma and past-year suicidality in men who had recently transitioned from the regular ADF.
The proportion of this transitioned male ADF population with past-year suicidality (21.7%, 95% CI: [19.9, 23.3]) was considerably higher than both the 2010 current ADF male population (2010) (3.8%, 95% CI: [3.7, 3.9]) and 2007 employed civilian men (1.4%, 95% CI: [0.9, 2.0]) (Syed Sheriff et al., 2019b). This implies that the transition may be a particularly vulnerable period for military males or that a particularly vulnerable group was transitioning at that particular time. The Interpersonal-Psychological theory of suicidal behaviour (Schonfelder et al., 2019) states that feelings of thwarted belongingness and perceived burdensomeness (feelings of being a burden to friends, family or society) lead to suicidal ideation. This might provide some explanation as to why the proportions of past-year suicidality were so much higher in the period of transition from the military.
In addition, interpersonal theories of suicidal behaviour (Joiner, 2005) might explain why childhood interpersonal trauma was an important determinant of suicidality in particular during the period of transition. Some studies suggest that childhood interpersonal trauma results in dysfunctional emotional regulation, which leads to suicidality in the context of challenging social circumstances (Lemaigre and Taylor, 2019).
Childhood trauma is associated with mental disorder, and mental disorder is also known to impact on suicidality throughout the lifespan. Therefore, other studies have highlighted the importance of including mental disorder in assessing the association between childhood trauma and suicidality. Specifically, it is important to assess whether suicidality is fully explained by psychopathology resulting from childhood trauma or if there is a direct association of childhood trauma and suicidality. Several studies have demonstrated that mental disorder can act as a mediator (Enns et al., 2006; Fergusson et al., 2000) of the association between childhood interpersonal trauma and adult suicidality. However, in agreement with this current study, childhood disorder may not fully mediate the relationship.
There have been contrasting results as to the impact of deployment and/or adult trauma on suicidality in military populations. However, a longitudinal study of serving and ex-serving military personnel found that suicide risk was independently associated with mental disorders but not with military-specific variables (LeardMann et al., 2013). This is important in the transitioning population as rates of current disorder are particularly high (Van Hooff et al., 2018).
While we are not aware of previous studies in the military that have analysed the impact of childhood disorders on past-year suicidality, there are civilian studies with which we can compare our findings. Recently, studies in general populations have highlighted childhood anxiety as an important determinant of suicidality (Sareen et al., 2005) and also as a mediator of the relationship between childhood trauma and suicidality (Bahk et al., 2017). These studies found evidence for state and trait anxiety as risk factors for adolescent suicidal behaviours (Ohring et al., 1996) and also features of anxiety within affective disorders as risk factors for adult suicidality (Fawcett et al., 1990). Importantly, there is evidence of anxiety disorders (particularly panic and PTSD) as predictors of adult suicidality, including attempts (Cougle et al., 2009), in men.
Strengths
This is the first study, of which we are aware, to investigate childhood experiences and childhood disorder simultaneously in determining suicidality in a recently transitioned military population. The generation of mutually exclusive categories according to the types of trauma experienced as children allowed the disentangling of trauma type from trauma load which has been a particular challenge for research on childhood experiences (Finkelhor et al., 2007). We also analysed the association of past-year suicidality by the number of types of childhood trauma experienced, along with mediator pathways through childhood anxiety. This also allowed us to compare our findings with a previous analysis of a regular ADF and employed civilian men (Syed Sheriff et al., 2019b).
Limitations
We analysed the associations between self-reported past-year suicidality and detailed structured interview data regarding childhood trauma and childhood disorder in a sample of recently transitioned ADF men. Therefore, the main predictor variables utilised in this analysis were childhood experiences recalled from adulthood, thus rendering the responses vulnerable to autobiographical bias. A recent systematic review highlights differences between prospective and retrospective reporting of childhood maltreatment (Baldwin et al., 2019). While it appears that retrospective and prospective reporting of childhood maltreatment varies, it is likely that attempts to identify these men would occur in adulthood, for example, at entry or exit from military service. Therefore, we have identified that certain retrospectively reported childhood and adult-onset factors were associated with past-year suicidality in recently transitioned men. While this may assist in identifying men at risk of suicidality, as usual with analyses of cross-sectional data, conclusions regarding the etiological significance of these childhood factors should be treated with caution.
In addition, in this study, as is fairly common in cross-sectional surveys, there appears to be a low response rate. However, in contrast to most surveys, the demographic and health status was known for those who did not respond at each stage. This was accounted for in the back-weighting of the sample to minimise error.
In order to aid comparability, as in a previous paper (Syed Sheriff et al., 2019b), we analysed the broad outcome of suicidality against childhood trauma and disorder, rather than suicidal ideation and suicide attempts separately, or the factors associated with transition between the two. Psychological factors such as impulsivity and irritability, military factors such as length of time in the military and type of discharge, as well as social factors such as employment after transition are also likely to impact suicidal ideation, attempts and the transition between these and other risky behaviours (Syed Sheriff et al., 2015). However, this is beyond the scope of this paper.
We accounted for the number of types of childhood trauma that were experienced, however, not for the number of times each trauma occurred during childhood. Thus, reflecting the range, rather than frequency or severity of trauma experienced. However, as stated previously, similar trauma count variables have previously shown consistent significant associations with outcomes (Sareen et al., 2013).
Implications
This research has implications for military and transitioned men, clinicians and policymakers. A high proportion of military men have suicidality during the transition period. Men with a history of childhood interpersonal trauma and/or anxiety should be aware that they may be vulnerable to suicidality when they transition from the military, as are those with adult-onset depression and anxiety and multiple types of adult-onset trauma (deployment and non-deployment related). Increased awareness of these associations may aid people in making informed choices about their career, help-seeking behaviour and assist them in identifying friends and colleagues who might be at risk. These findings reinforce the importance for clinicians of assessing suicidality in transitioned military men. This research implies that taking a thorough lifelong history, identifying the types of trauma and disorder and when they first occurred (childhood or adulthood), is essential in assessing the risk of suicidality in men transitioning from military service. The high prevalence of suicidality in transitioned ADF men makes this a priority for policymakers. Not only is the prevalence high, but the risk factors are common and can potentially allow enhanced early identification of those at risk prior to the transition period. Policymakers now need to focus efforts into prospective studies to further elucidate early risk factors, and intervention studies to prevent and/or reduce suicidality during the transition period.
Conclusion
Self-reported suicidality was relatively high in men who have recently transitioned from regular military service. Suicidality may be precipitated by the period of relative social instability associated with transitioning. Risk factors, such as childhood interpersonal trauma, childhood anxiety and multiple types of adult trauma (deployment and non-deployment related) are potentially recognisable early and could allow enhanced early identification of those at risk prior to the transition period. These findings also imply that early interventions targeting anxiety and interventions to reduce social instability during the transition period may be useful in reducing suicidality during this time. Further prospective studies are needed to further explore these novel findings.
Footnotes
Acknowledgements
We thank all investigators and scientific advisors for their contribution to the design of the Programme. Most importantly, we thank all of the current and transitioned ADF personnel who participated in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: A.M. and M.V.H. receive funding from the Departments of Veterans Affairs and the Australian Department of Defence. A.M. is the principal adviser in psychiatry to the Department of Veterans Affairs and has advisory roles with the Australian Department of Defence. G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, Ramsay Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca and Servier; has been a speaker for AstraZeneca, Janssen Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen Cilag, Lundbeck, Otsuka and Servier. There is no conflict of interest in the present study for any of the other authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Data analysed in this study were derived from the Transition and Wellbeing Research Programme (the Programme). R.S.S. received funding from Australian Rotary Health in the form of a PhD scholarship. R.S.S. is supported by the National Institute for Health Research (NIHR) Oxford Health Biomedical Research Centre (grant BRC-1215-20005) and by the NIHR Research Professorship awarded to Professor Andrea Cipriani (grant RP-2017-08-ST2-006). The views expressed are those of the authors and not necessarily those of the UK National Health Service, the NIHR or the UK Department of Health.