
Abstract
Schizophrenia is a heterogeneous disorder in terms of clinical presentation, pattern of response to medication, and long-term outcome. While some patients make relatively satisfactory progress, others experience a severe deteriorating course, and in the early stage of the illness it is very difficult to identify patients with characteristics that predict a poor long-term outcome. Predictors of treatment response and long-term outcome are needed to offer appropriate intervention. The outcome predictive power of baseline characteristics has been investigated in several studies [1–6], and the results have shown that delay of initial treatment, negative symptoms [3], [7], [8], male gender [1], [6], [9–12], low education level [1], [9], and poor premorbid adjustment are predictors of negative outcome.
Numerous studies that examined the relationship between duration of untreated psychosis (DUP) and outcome have been published, and most of them showed that longer DUP resulted in poorer outcome [13], [14]. Based on this evidence a number of early intervention programmes have been developed around the world, and some reports have shown that such programmes shortened DUP and improved outcome [15], [16].
These findings have drawn attention to the need for early intervention in first-episode psychosis. But psychiatric services in Japan are different from those in Western countries in several respects. The treatment of mental illness in Japan is hospital based, and there are a large number of psychiatric beds (28 beds per 10 000 population). The average length of hospital stay is 327.2 days, and 53.5% of inpatients have stays longer than 1 year. DUP in Japan, however, is similar (mean = 13.7 months) to that reported in studies abroad [17].
Great attention has recently been paid to cognitive dysfunction as a core feature of schizophrenia. A number of studies on cognitive deficits of first-episode schizophrenia have been carried out because the first episode of schizophrenia provides an optimal occasion to investigate the neurobiology of the disorder. This is because confounding factors such as hospitalization, long-term medication, and chronicity can be avoided. It has recently been said that cognitive deficits may occur even during the premorbid period, and impairments in attentional and executive performance, in particular, have been suggested as deficits that are evident many years before the onset of the first episode[18].
The present study focused on associations between DUP, premorbid functioning, and cognitive function and the outcome in a Japanese sample. Because few prospective studies of first-episode schizophrenia have been conducted in Japan, careful observation should provide valuable information in regard to the treatment of mental illness in Japan.
Methods
Subjects
Subjects were recruited from consecutive referrals to two hospitals in Tokyo between February 2001 and February 2003. All subjects met the ICD-10 criteria for schizophrenia and were treated by psychiatrists for the first time. The subjects fulfilled the following inclusion criteria: (i) age 16–44 years inclusive at the onset of the first episode; (ii) no history of psychiatric treatment; (iii) neuroleptic naïve; (iv) not suffering from organic brain syndrome. None of the patients had a history of abuse of psychoactive substances including alcohol. Written informed consent was obtained after a complete description of the study was provided to the subjects and their relatives. This study complied with the ethical guidelines for research involving human participants as set out in the Declaration of Helsinki in 1995 (as revised in Edinburgh 2000). Approval to collect data from medical records and informants was obtained from the ethics committees of the institutions involved.
Baseline assessment
Clinical assessment
We collected information from subjects, their family, and any other informant at the first consultation. Best-estimate age at onset based on all available information was used to determine DUP. We defined DUP as the interval between the onset of psychotic symptoms and the first prescription of neuroleptics for psychosis [17]. We identified the onset of psychotic symptoms as the time of first appearance of either (i) at least one of the first-rank symptoms of Schneider; or (ii) at least one of the four ICD-10 criteria in F20 (a–d). Negative symptoms and a reduction in social functioning were not considered in the assessment of DUP. We used the Premorbid Adjustment Scale (PAS) to assess premorbid functioning [19]. PAS yields measures of premorbid functioning in two different phases of life prior to the onset of illness: childhood (6–12 years) and adolescence and young adulthood (13–21 years). Higher scores indicate poorer premorbid functioning. Psychiatric symptoms were measured with the Positive and Negative Syndrome Scale (PANSS) [20]. Global social functioning was measured on the Global Assessment of Functioning (GAF) [21]. The initial evaluation was performed within a few days after first consultation.
Neuropsychological assessment
The neuropsychological assessment was completed soon after subjects became able to cooperate with the tests. The neuropsychological test battery consisted of the following: (i) Letter Cancellation Test as a measure of visual search and attention [22]; (ii) Digit Span as a measure of immediate recall and verbal working memory [23]; (iii) Trail-Making Test as a measure of visuomotor sequencing involving connection of consecutive numbers randomly arranged on the page (part A) and of numbers and letters in alternating order (part B) [24]; and (iv) Word Fluency Test (letter and category) as a measure of verbal fluency [25].
Outcome assessment
One year later the subjects were reassessed by means of the GAF, and the severity of psychiatric symptoms was assessed by means of the PANSS. At the same time we evaluated social functioning during the past 3 months by means of the Social Functioning Scale (SFS) [26]. The SFS is a self-report scale, and the subjects filled out a questionnaire. A higher score on the SFS indicates better social functioning.
Data analysis
All statistical analyses were performed using SPSS for Windows version 11 (SPSS, Chicago, IL, USA). Because a few subjects in all previous studies had an extremely long DUP, and they may have had an undue influence on the results, analyses based on raw DUP measurements involve various statistical difficulties. To avoid this problem the present subjects were divided into two groups according to the length of DUP, with the median DUP value as the dividing line. The Mann–Whitney U-test was used to assess differences between groups. Following Haas et al. [27] and Larsen et al. [28] we dichotomized the subjects on the basis of their PAS scores into a low-PAS group and a high-PAS group at the median value. Spearman's correlation analysis was used to examine the relationship between neuropsychological test score at first consultation and outcome.
Results
Sample characteristics
During the 2 year recruitment period 34 eligible patients agreed to take part in the study. None of the subjects had a lifetime history of any substance (including alcohol) abuse disorder. There were 10 dropouts between baseline and follow up. The dropouts were untraceable or had changed hospitals for geographical reasons, and one had committed suicide. There were no significant differences in demographic characteristics between those who completed the study and the dropouts.
The final sample consisted of 11 men (45.8%) and 13 women (54.2%), and their mean age was 27.0 years (SD = 6.57, range = 16–44). Ten of the 24 were inpatients at the time of the baseline assessment. Mean DUP was 8.3 months (SD = 13.42, range = 0.1–48), and the median DUP was 3 months. The demographic and clinical profiles of the subjects are shown in Table 1.
Subject characteristics
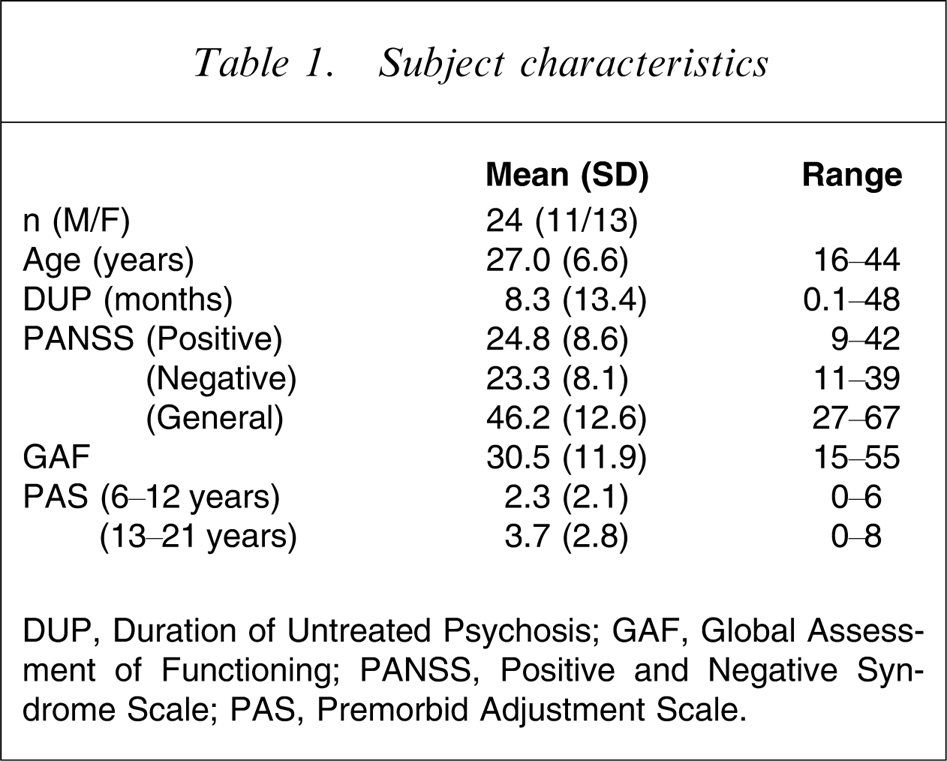
DUP, Duration of Untreated Psychosis; GAF, Global Assessment of Functioning; PANSS, Positive and Negative Syndrome Scale; PAS, Premorbid Adjustment Scale.
DUP and outcome
Table 2 shows the mean scores on the PANSS, GAF, and SFS of both the long-DUP group and short-DUP group. At follow up the negative symptom score of the short-DUP group was significantly better than that of the long-DUP group. The differences between the two groups in positive symptom score and GAF score were not significant.
DUP and outcome
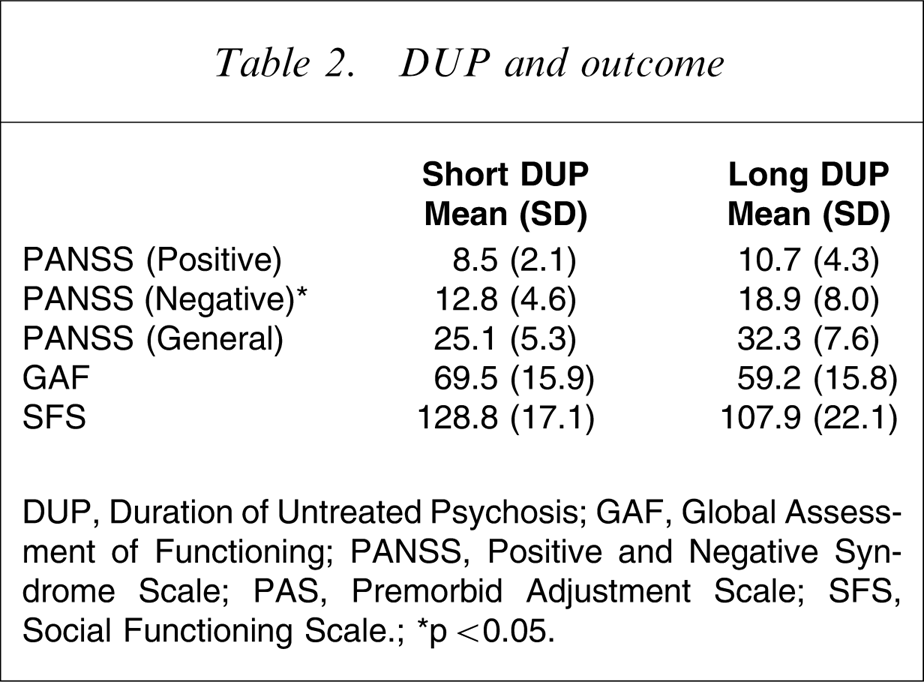
DUP, Duration of Untreated Psychosis; GAF, Global Assessment of Functioning; PANSS, Positive and Negative Syndrome Scale; PAS, Premorbid Adjustment Scale; SFS, Social Functioning Scale.; ∗p < 0.05.
Premorbid functioning and outcome
Table 3 shows the mean scores on the PANSS, GAF, and SFS of the low-PAS group and the high-PAS group. The PAS scores of childhood were associated with outcome: the scores on the PANSS (negative and general) and GAF in the low-PAS group were better than in the high-PAS group. But the results for the PAS scores of adolescence were not significantly associated with outcome.
Premorbid functioning (PAS score) and outcome
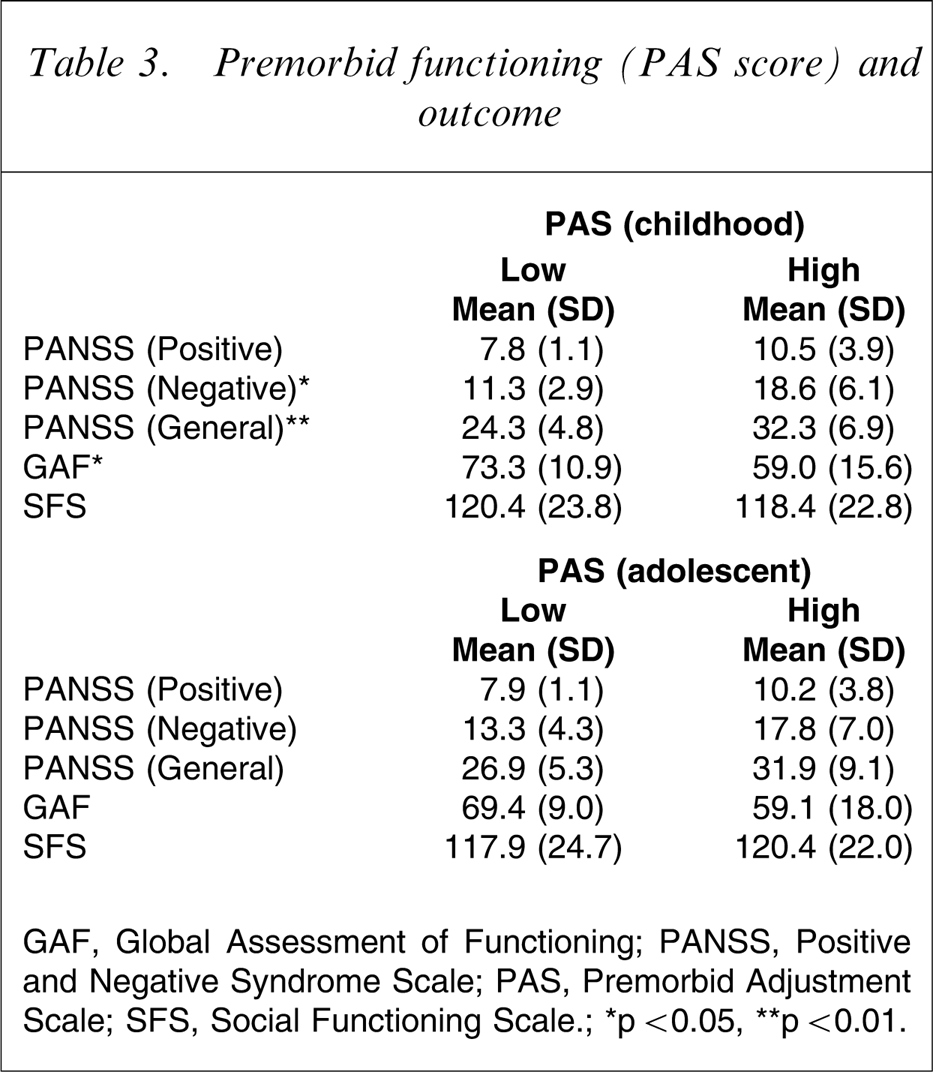
GAF, Global Assessment of Functioning; PANSS, Positive and Negative Syndrome Scale; PAS, Premorbid Adjustment Scale; SFS, Social Functioning Scale.; ∗p < 0.05, ∗∗p < 0.01.
Cognitive performance and outcome
The relationships between cognitive performance at baseline and clinical and social outcome are shown in Table 4. Significant correlations were found between attention and outcome: the lower the number of correct answers on the Letter Cancellation Test, the poorer the scores on the PANSS (general) and the GAF; the lower the number of correct answers on the Digit Span, the poorer the scores on the PANSS (negative) and the SFS. Moreover, significant correlations were found between word fluency and outcome: the poorer the performance at the word fluency test (letter), the poorer score of the PANSS (positive, negative and general), and the GAF. No significant association was found between cognitive performance and SFS scores at follow up.
Neuropsychological scale scores and outcome (Spearman's coefficients)
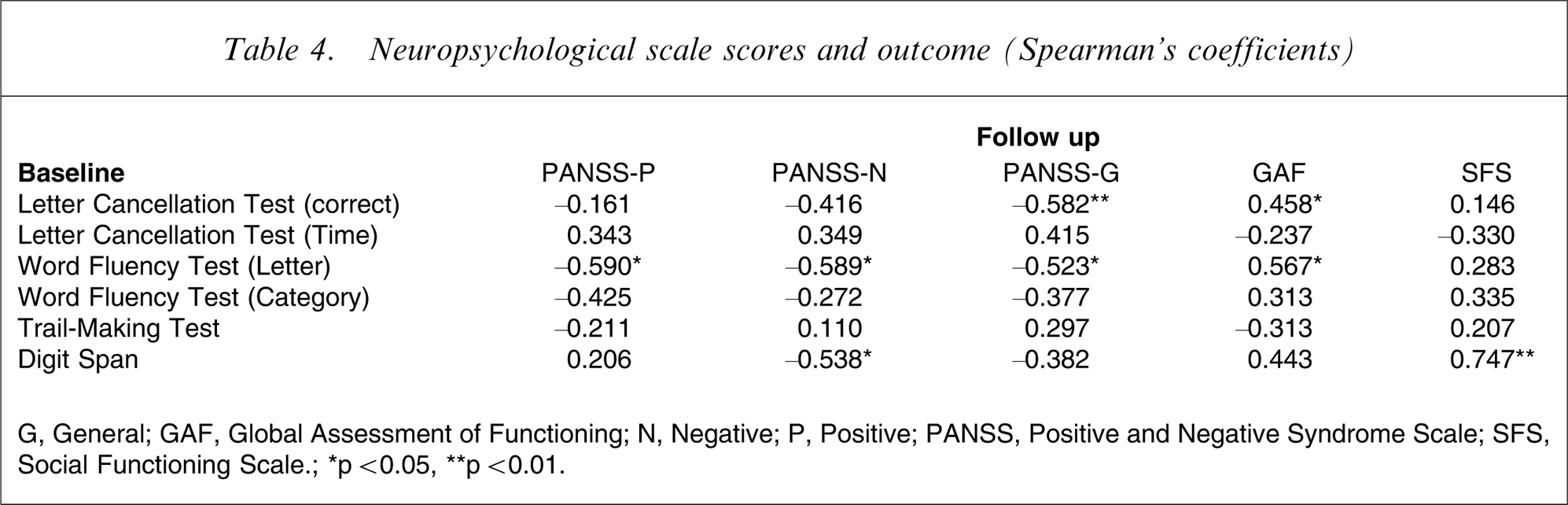
G, General; GAF, Global Assessment of Functioning; N, Negative; P, Positive; PANSS, Positive and Negative Syndrome Scale; SFS, Social Functioning Scale.; ∗p < 0.05, ∗∗p < 0.01.
Discussion
The aim of the present study was to identify variables associated with the outcome of patients with first-episode schizophrenia in Japan, and DUP, premorbid function, attention, and verbal fluency were found to be associated with outcome.
DUP and outcome
A number of studies have reported a statistically significant relationship not only between DUP and outcome [2], [3], [5], [12], [29–37], but between DUP and time to treatment response [34], [38]. These findings have provided support for the idea that intervention at or even before the onset of the first episode might improve response to treatment and long-term outcome. Lieberman et al. and Wyatt et al. hypothesized that untreated psychosis is biologically toxic [39], [40], and Birchwood et al. suggested the critical period hypothesis, which suggested that deterioration occurs in the first 2–3 years of the illness, and that this deterioration might be arrested with appropriate and effective treatment [41]. DUP has also been found to influence long-term outcome in recent studies [9], [42], [43]. As a result numerous early detection and intervention programmes have been developed all over the world, and they have produced excellent results [13], [15], [16], [44–47].
Perkins et al. reviewed the 43 reports on the association of DUP and treatment outcome and conducted a meta-analysis of the relationship [14]. The results of the meta-analysis showed that shorter DUP was associated with greater response to antipsychotic treatment, as measured by improvement or end-point severity of global psychopathology, positive symptom severity, and negative symptom severity, and the effect size for DUP and response for the combined statistic (all studies) was consistently significant.
In the present study the negative symptom score at follow up was better in the short-DUP group than in the long-DUP group, similar to the results of previous studies abroad. Our previous study showed a significantly longer duration of the first admission in the long-DUP group than in the short-DUP group. Thus, ameliorating the symptoms of the initial psychotic episode may not only lessen the immediate suffering experienced by patients and their relatives, but improve the long-term outcome by limiting progression of the disease and maintaining the patient's ability to respond to treatment.
Premorbid functioning and outcome
A number of studies have attempted to demonstrate an association between premorbid function and outcome, and PAS has been used most frequently to assess premorbid functioning.
Larsen et al. suggested that poor premorbid functioning was significantly correlated with more PANSS negative and general symptoms and poorer GAF score at 1 year [2]. Perkins et al. and Malla et al. reported that poor premorbid functioning was associated with poor outcome [5], [12]. Hafner et al. reported that negative symptoms developed over a longer period even prior to the onset of the first psychotic episode and that early development of negative symptoms is likely to represent deficits in premorbid functioning [48]. Thus, premorbid functioning may be predictive of outcome. In the present study the PANSS (negative and general) and GAF scores at follow up were better in the low-PAS (childhood) group than in the high-PAS group. This finding was consistent with the results of previous studies. But in the present study the PAS scores for adolescence were not significantly correlated with outcome. Table 3 shows that the mean PANSS and GAF scores at follow up were better in the low-PAS adolescence group than in the high-PAS group. Although the differences were not statistically significant, they suggest that poor premorbid functioning at this age may be associated with poor outcome.
Cognitive performance and outcome
Cognitive dysfunction is considered a core feature of schizophrenia, and a number of studies that have assessed cognitive dysfunction in schizophrenia have been published. Because the subjects in many of the studies were chronic patients, the neuropsychological test scores may have been influenced not only by the severity of the illness itself but by long-term medication, duration of illness, and hospitalization. Cognitive function in first-episode schizophrenia with short duration of morbidity and medication has attracted the attention of many researchers as a means of understanding the essence of the cognitive dysfunction in schizophrenia. They have compared first-episode psychosis patients, chronic patients, and healthy control subjects on a comprehensive battery of neuropsychological tests to determine the degree of cognitive impairment [49–56]. These studies have shown that first-episode patients had larger generalized neuropsychological deficits than the healthy control subjects, and poor performance on measures of verbal learning and memory, attention, processing speed, and executive function. These findings suggested that cognitive deficits may be present at a very early stage in the course of the illness.
Some studies assessed neuropsychological performance as a possible predictor of outcome in first-episode psychotic patients [57–59]. Robinson et al. reported poor attention at baseline as well as male gender, obstetric complication, and severe hallucinations and delusions as variables associated with less likelihood of response to treatment [6]. Verdoux et al. reported that poor memory performance during the first admission was associated with risk of presenting with psychotic symptoms and rehospitalization at 2 year follow up [8]. Because some studies have reported an association between cognitive functioning and outcome [57], [60], [61], psychosocial interventions might potentially improve outcome.
In the present study attention and verbal fluency were found to be significantly associated with clinical outcome, consistent with the results of previous studies. None of the present subjects had a lifetime history of substance abuse or alcoholism. The present results, involving subjects who were relatively homogeneous and uninfluenced by psychoactive substances, reflect the true nature of the disorder itself. Cognitive deficits are considered a core feature of the disorder and reflect the vulnerability of patients to the disorder. Neuropsychological performance at the first consultation may enable prediction of the course and outcome.
It is also said that signs of cognitive deficits have been found to occur during the premorbid period and in early childhood. Caspi et al. assessed subjects’ cognitive function as part of the Israeli Draft Board aptitude assessments at ages 16–17 when all were in good mental health, and again following manifestation of the first psychotic episode, and they compared their performance with that of healthy controls assessed at the same time [62]. No significant change in the patients with schizophrenia was found between the first and second assessment, and the schizophrenia patients performed worse than the controls on both the first and the second assessments. Some studies have reported that ultra-high-risk individuals had significant cognitive deficits [63]. Cannon et al. suggested that neuropsychological performance, particularly attentional and executive deficits at 13 years of age, were related to adult psychiatric outcome [18], and assessing cognitive function in detail may therefore make it possible to predict the development of the first episode of psychosis.
In summary, the results of the present study in Japan are consistent with previous evidence in Western countries that delay of initial treatment, premorbid functioning, and cognitive deficits are associated with outcome. A major limitation of the present study was the small size of the subject population, which may limit the generalizability of the results. But because the subject group was relatively homogeneous and not influenced by psychoactive substances, the results reflect the essence of the disorder. Early detection and suitable intervention are regarded as important issues. The present results suggest that psychosocial interventions that shorten DUP and enhance cognitive function may be useful to improve outcome. In Japan the government has been making an effort to implement deinstitutionalization in recent years, although a little too late, and Japanese care for psychotic patients is behind the level of care in Western countries. The importance of early intervention and the factors associated with outcome were confirmed in this Japanese study, but further study to detect predictive factors not only of outcome but of the development to psychosis is needed.