
Abstract
Since the landmark Epidemiologic Catchment Area (ECA) Survey [1], a number of representative general population surveys conducted around the world have examined the prevalence of exposure to traumatic events which may lead to post-traumatic stress disorder (PTSD). The estimates derived from these studies vary considerably (16%–90%), with more recent studies demonstrating higher rates of exposure [2–10]. This variability may be explained by changes in the way trauma exposure has been conceptualized and operationalized over time.
Since PTSD was first recognized as a diagnostic entity in the third revision of the Diagnostic and statistical manual of mental disorders (DSM-III) [11], the experiencing of a traumatic event has been the first criterion that must be met (criterion A) to obtain the diagnosis [12]. The definition of what constitutes a traumatic event, however, has broadened considerably over time. At the time of DSM-III, traumatic events were defined as events that would ‘evoke significant symptoms of distress in almost anyone’ [11]. DSM-III-R introduced an additional feature; namely, that the events were ‘outside the range of usual human experience’ [13]. Thus, in DSM-III and DSM-III-R, the experiencing of such an event was automatically assumed to be traumatic.
The definition was further revised in DSM-IV [14] when it was recognized that the experiencing of an event was not sufficient for a person to be traumatized by it. Criterion A was split into two parts. According to criterion A1, the person must have been exposed to a potentially traumatic event (PTE) in which they experienced, witnessed, or were confronted with ‘an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others.’ For the event to be considered traumatic, the person's response to that event must have involved ‘intense fear, helplessness, or horror’ (criterion A2).
Changes in the way epidemiological surveys have measured exposure to PTEs may also explain the differences in prevalence estimates observed across time. As summarized by Breslau [15], earlier surveys elicited a history of exposure using a single question incorporating examples of PTEs as defined by the DSM, whereas more recent surveys have utilized lists of events which enquire about exposure to different event types individually. The use of multiple-item measures has been shown to result in estimates of exposure approximately 20% higher than those obtained using single item measures among samples of clinical populations and college students [16–19].
The use of lists of events has become standard practice in measuring exposure to PTEs in general population surveys. The number of event types enquired about has, however, increased over time. To a degree, this increase has reflected the broadening of the stressor criteria through revisions to the DSM; however, increases have also been observed independent of changes to the diagnostic criteria. For example, the Composite International Diagnostic Interview (CIDI), one of the most commonly used instruments in epidemiological studies of mental health, has increased the number of events listed from 11 in the previous version (CIDI 2.1) [20], to 29 in the current version (WMH-CIDI) [21] yet both versions purport to measure trauma exposure according to DSM-IV.
There is evidence to suggest that higher prevalence estimates are derived when longer lists of PTEs used. Research examining the prevalence of sexual abuse among women has found that asking more specific questions about exposure results in more reports than asking fewer, more general questions [22,23]. Thus, epidemiological surveys that have utilized less comprehensive measures are likely to produce lower estimates of the prevalence of PTE exposure in the general population. To our knowledge, only one study has empirically examined the effect of increasing the number of events listed on the prevalence of exposure in a population survey. Using data from the 1996 Detroit Area Survey of Trauma, Breslau and Kessler [24] examined the impact of the broadening the stressor criteria from DSM-III-R to DSM-IV. The authors found the expanded list of events included in DSM-IV increased the lifetime prevalence of PTE exposure from 68.1% to 89.6%. The present study sought to extend on these findings by examining the impact of the number of PTE types assessed on the overall prevalence of PTE exposure longitudinally, as well as the differential impact according to sex.
The prevalence of exposure to PTEs in the Australian general population was first examined in the 1997 National Survey of Mental Health and Wellbeing (NSMHWB) using the CIDI 2.1. It was estimated that 64.6% of men and 49.5% of women had experienced at least one PTE [5]. In 2007, the second NSMHWB was conducted in Australia, enabling more recent estimates of PTE exposure to be derived. These estimates were obtained using the WMH-CIDI. Using data from both the 1997 and 2007 NSMHWB, the present study aimed to:
examine the lifetime prevalence of exposure to PTEs in the Australian general population in 2007 using the WMH-CIDI; and
compare these estimates with those obtained in 1997 using the CIDI 2.1.
It is hypothesized that estimates of the prevalence of trauma exposure in 2007 will be higher than those obtained in 1997.
Methods
Sample
The 1997 and 2007 NSMHWB were nationally representative population surveys conducted by the Australian Bureau of Statistics under the Census and Statistics Act, 1905. For both surveys, respondents were selected at random from a stratified, multistage area probability sample of private dwellings. Data were weighted according to the inverse probability of an individual being selected for interview. The 1997 NSMHWB surveyed 10 641 Australians aged 18 years and over (78% response rate). The 2007 NSMHWB surveyed 8841 Australians aged 16–85 years (60% response rate). Interviews were conducted in person and responses were recorded on a laptop computer. More detailed discussions of the sampling design and methodology of the 1997 and 2007 NSMHWB are available elsewhere [25,26].
Assessment of trauma exposure
Lifetime history of exposure to PTEs was assessed for all respondents in both the 1997 and 2007 NSMHWB. The 1997 NSMHWB utilized the CIDI 2.1 [20] which assessed exposure to nine specific PTEs (see Table 1). In addition to these events, respondents were asked whether they had ever experienced any ‘other extremely stressful or upsetting event’, or ‘suffered great shock’ because one of the nine events had happened to someone close.
Traumatic events asked about in the 1997 NSMHWB and the corresponding events asked about in the 2007 NSMHWB
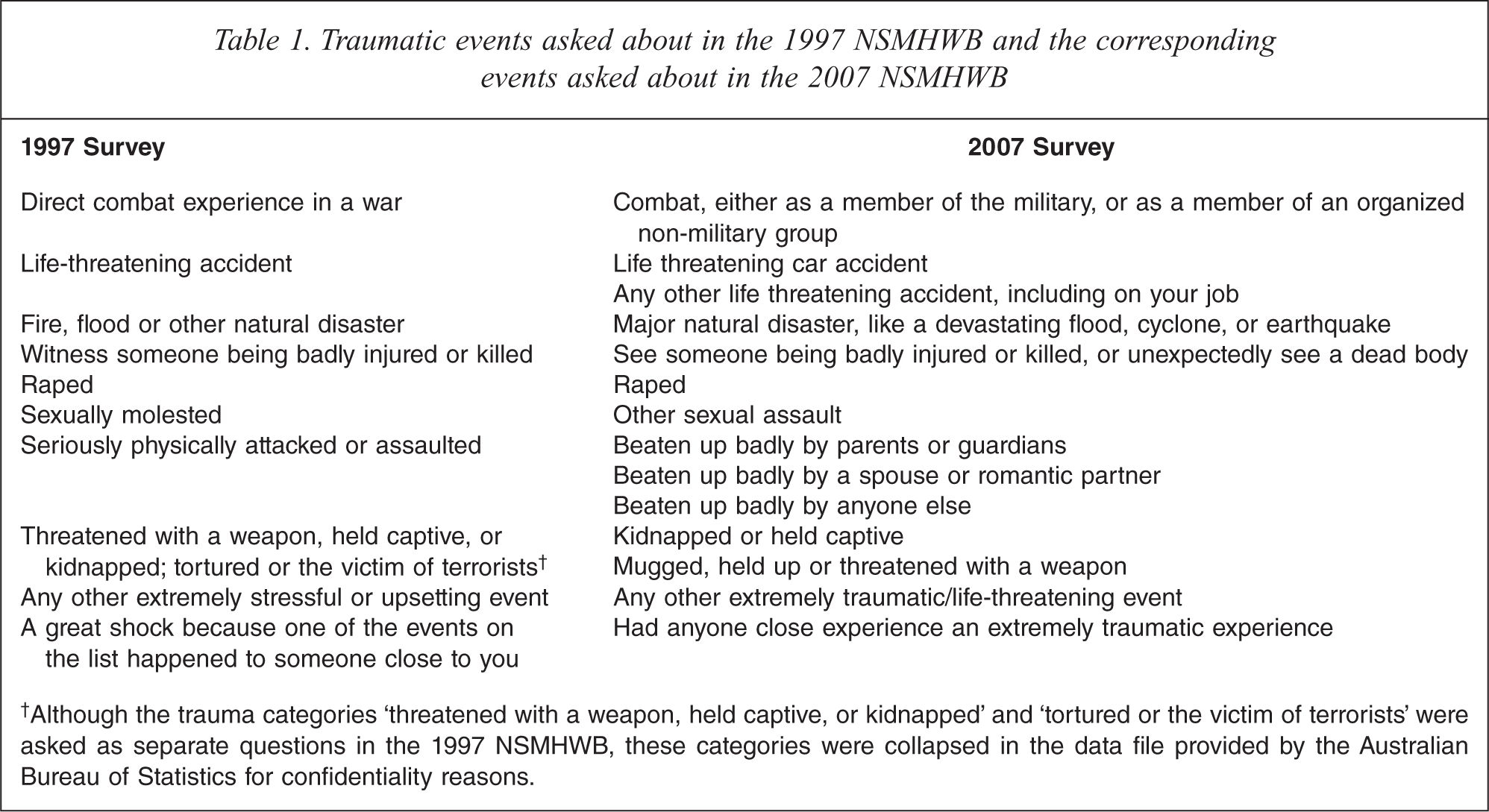
†Although the trauma categories ‘threatened with a weapon, held captive, or kidnapped’ and ‘tortured or the victim of terrorists’ were asked as separate questions in the 1997 NSMHWB, these categories were collapsed in the data file provided by the Australian Bureau of Statistics for confidentiality reasons.
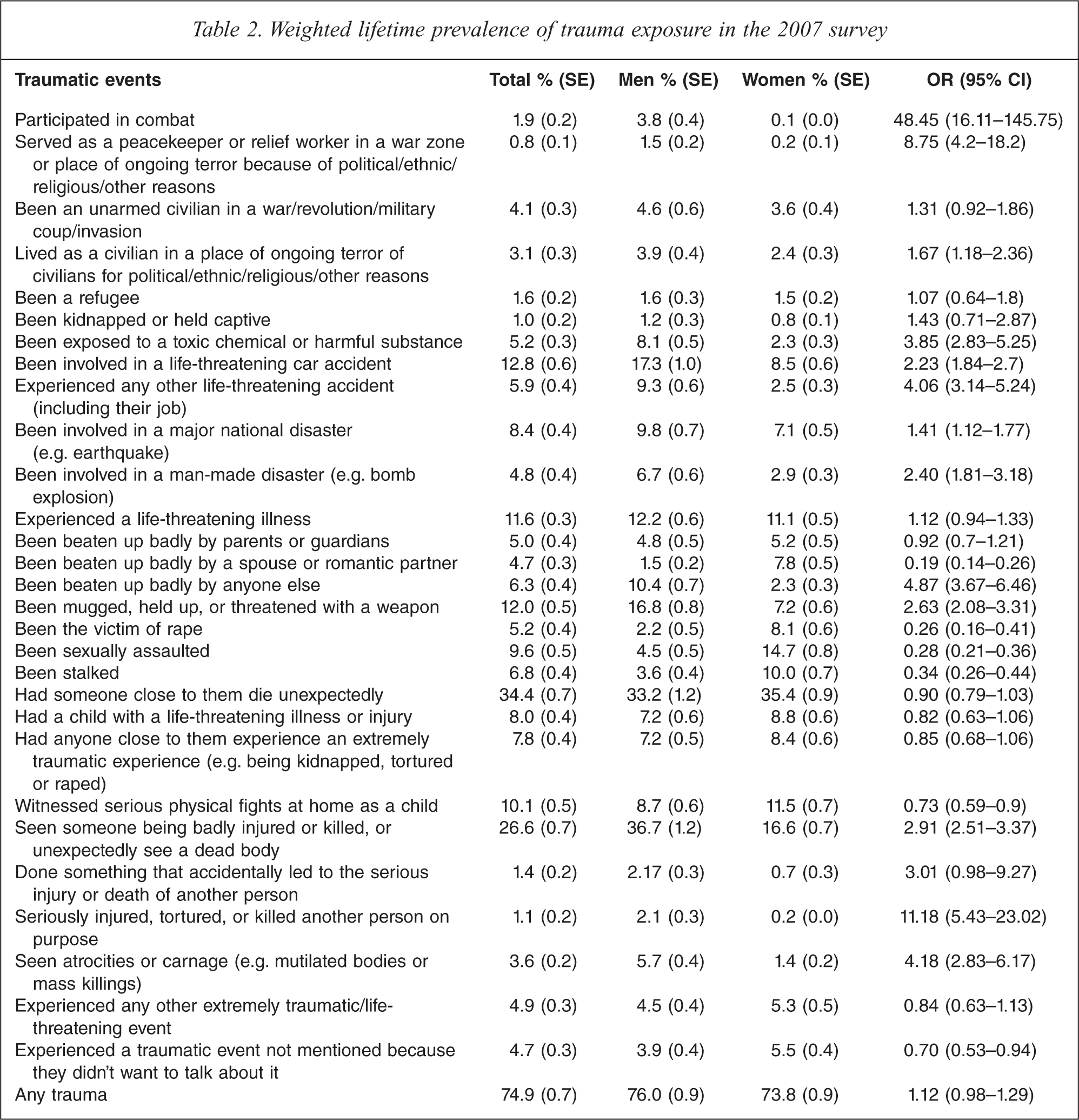
The 2007 NSMHWB utilized the WMH-CIDI [21]. Respondents were asked whether they had ever experienced 27 specific PTEs (Table 2). In addition to these events, respondents were asked whether they had ever experienced any ‘other extremely traumatic or life-threatening event’, or a ‘private event’ they did not wish to talk about. For each event endorsed respondents were asked the number of times the event occurred.
Weighted lifetime prevalence of trauma exposure in the 2007 survey
Analyses
Analyses were undertaken using SAS version 9.2 complex survey procedures. Prevalence estimates were weighted to conform to independent population estimates by state, part of state, age and sex. The standard errors on estimates were obtained through the delete-a-group jack-knife variance technique. Differences between the sexes with regard to exposure to trauma in the 2007 NSMHWB were examined using logistic regression analyses.
The overall prevalence of exposure to PTEs obtained in 1997 was compared to that obtained in 2007 for men and women. To determine whether differences between the prevalence estimates obtained in the two surveys were due to respondents having been asked about an increased number of event types in the latter survey, analyses were restricted to include only those events that corresponded to those asked about in the 1997 NSMHWB. The first column of Table 1 presents the PTEs asked about in the 1997 NSMHWB, and column 2 presents the corresponding events from the 2007 NSMHWB. If the difference between the prevalence estimates derived was statistically significant, this would imply that the differences observed were due to factors other than changes to the trauma assessment (e.g. a true change in the prevalence of trauma exposure). As direct comparisons between the two surveys may be confounded by differences in the age composition of the samples, the prevalence of exposure for matched age-groups from the 1997 and 2007 NSMHWB were compared. These analyses were restricted to respondents aged 20–69 years and split into five age groupings that could be derived from both the 1997 and 2007 NSMHWB (20–29 years, 30–39 years, 40–49 years, 50–59 years, and 60–69 years). This allows for the comparison of adjacent, non-overlapping birth cohorts across surveys, thereby controlling for age-related effects [27]. Analyses were conducted only on the pooled estimate of trauma exposure (i.e. the overall prevalence and not according to trauma type) due to sample size limitations. Differences were considered statistically significant if the 95% confidence intervals did not overlap.
Results
Prevalence of trauma exposure in 2007
Three quarters (74.9%) of Australian men and women had experienced at least one PTE representing 11 994 136 Australians (Table 2). Men and women were equally likely to have experienced a PTE (76% versus 73.8%). The most commonly experienced event among men was having seen someone being badly injured or killed, or having unexpectedly seen a dead body (36.7%). Among women, the most commonly experienced event was having had someone close die unexpectedly (35.4%).
There were a number of sex differences in the likelihood of exposure to different event types. Men were more likely than women to have experienced combat exposure (OR 48.5), seriously injured, tortured, or killed another person on purpose (OR 11.2), been beaten up badly by someone other than their parents or romantic partner (OR 10.4), served as a peacekeeper or relief worker in a war zone or place of ongoing terror (OR 8.8), seen atrocities or carnage (OR 4.2), been involved in a life-threatening car accident (OR 2.2), experienced any other life-threatening accident (OR 4.1), been exposed to a toxic chemical or harmful substance (OR 3.9), seen someone being badly injured or killed, or unexpectedly see a dead body (OR 2.9), been mugged, held up, or threatened with a weapon (OR 2.6), been involved in a man-made disaster (OR 2.4), lived as a civilian in a place of ongoing terror (OR 1.7), and been involved in a major national disaster (OR 1.4).
On the other hand, men were less likely than women to have been beaten up badly by a spouse or romantic partner (OR 0.2), been the victim of rape (OR 0.3), been sexually assaulted (OR 0.3), been stalked (OR 0.3), witnessed serious physical fights at home as a child (OR 0.7), experienced a traumatic event not mentioned because they didn't want to talk about it (OR 0.7).
Among those who had experienced PTEs, 66.8% (SE 0.9) had experienced multiple event types (i.e. more than one of the event types listed in Table 1) and 73.9% (SE 0.9) had experienced multiple episodes of PTEs. Men were more likely to have experienced multiple event types (men: 70.1%, SE 1.3; women: 63.5%, SE 1.2; OR 1.35, 95% CI: 1.15–1.59), and multiple episodes compared to women (men: 76.5%, SE 1.3; women: 71.3%, SE 1.1; OR 1.32, 95% CI: 1.10–1.56).
Comparisons between the 1997 and 2007 NSMHWB
The overall prevalence of exposure to PTEs in the 2007 NSMHWB was considerably higher than that found in the 1997 survey (74.9% versus 56.9%). The difference was more pronounced among women than men. In 1997 it was estimated that 64.6% of men and 49.5% of women had experienced PTEs [5]. The corresponding figures in 2007 were 76% and 73.8% for men and women respectively.
Comparisons between surveys may be confounded by differences in the age composition of the samples. To control for this effect and determine whether the differences observed were an artefact of changes to the survey instrument (i.e. asking about the experiencing of 29 events compared to 11 in the 1997 survey) the prevalence of exposure for matched age groups from the 1997 and 2007 NSMHWB were compared in relation to event types assessed in both surveys. Same-aged subgroups from the 1997 and 2007 NSMHWB correspond to temporally adjacent birth cohorts whose birth year range differs by 10 years. Results of cross-cohort comparisons for men and women are presented in Figures 1 and 2 respectively. No cross-cohort differences were observed. The prevalence of exposure to the matched event types did not change for the matched age groups from 1997 to 2007. These findings indicate that the difference in prevalence estimates obtained between the two surveys is related to differences in the assessment of trauma exposure.
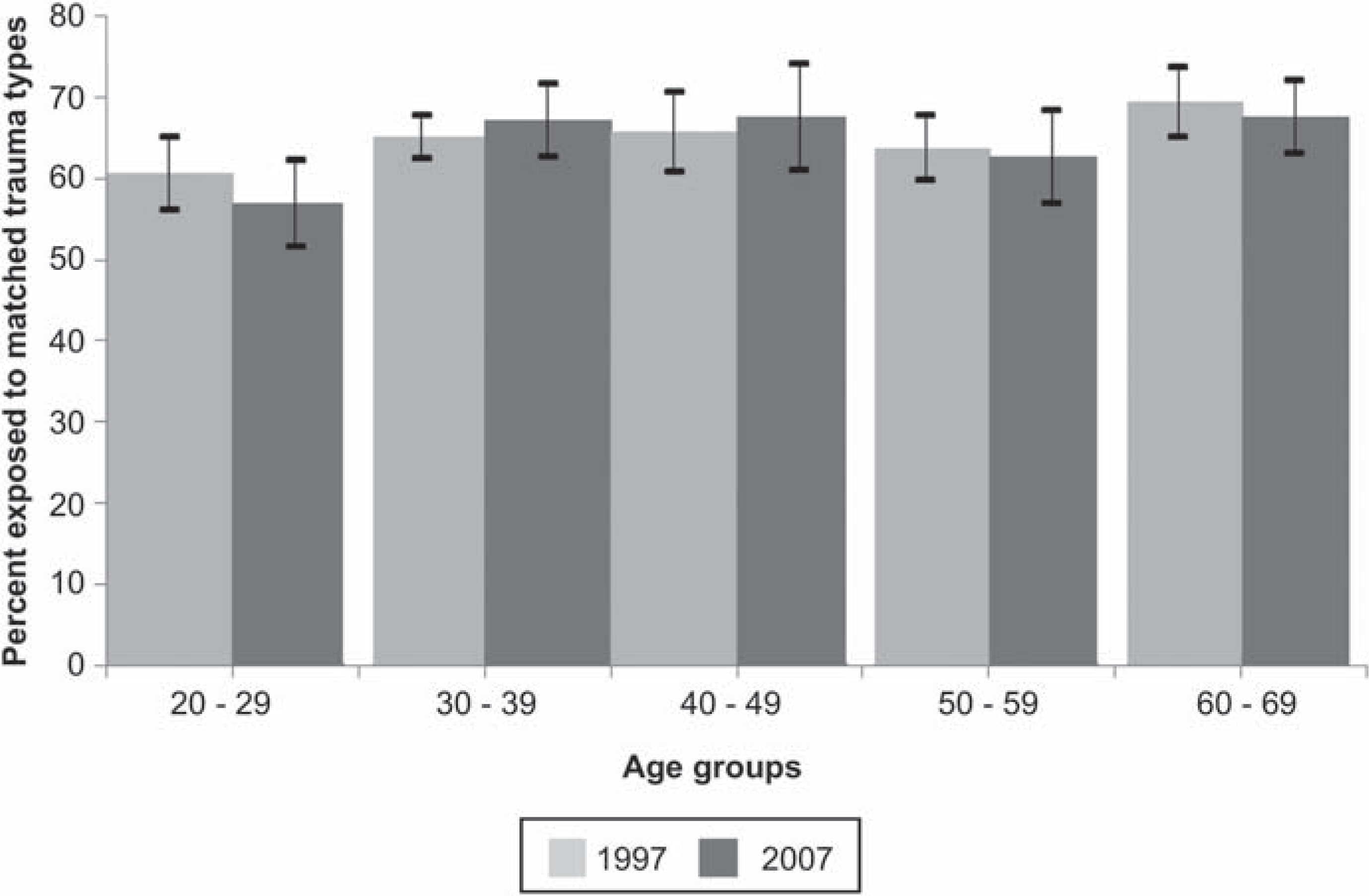
Comparison of the prevalence of exposure to matched events among age-matched men in the 1997 and 2007 NSMHWB.
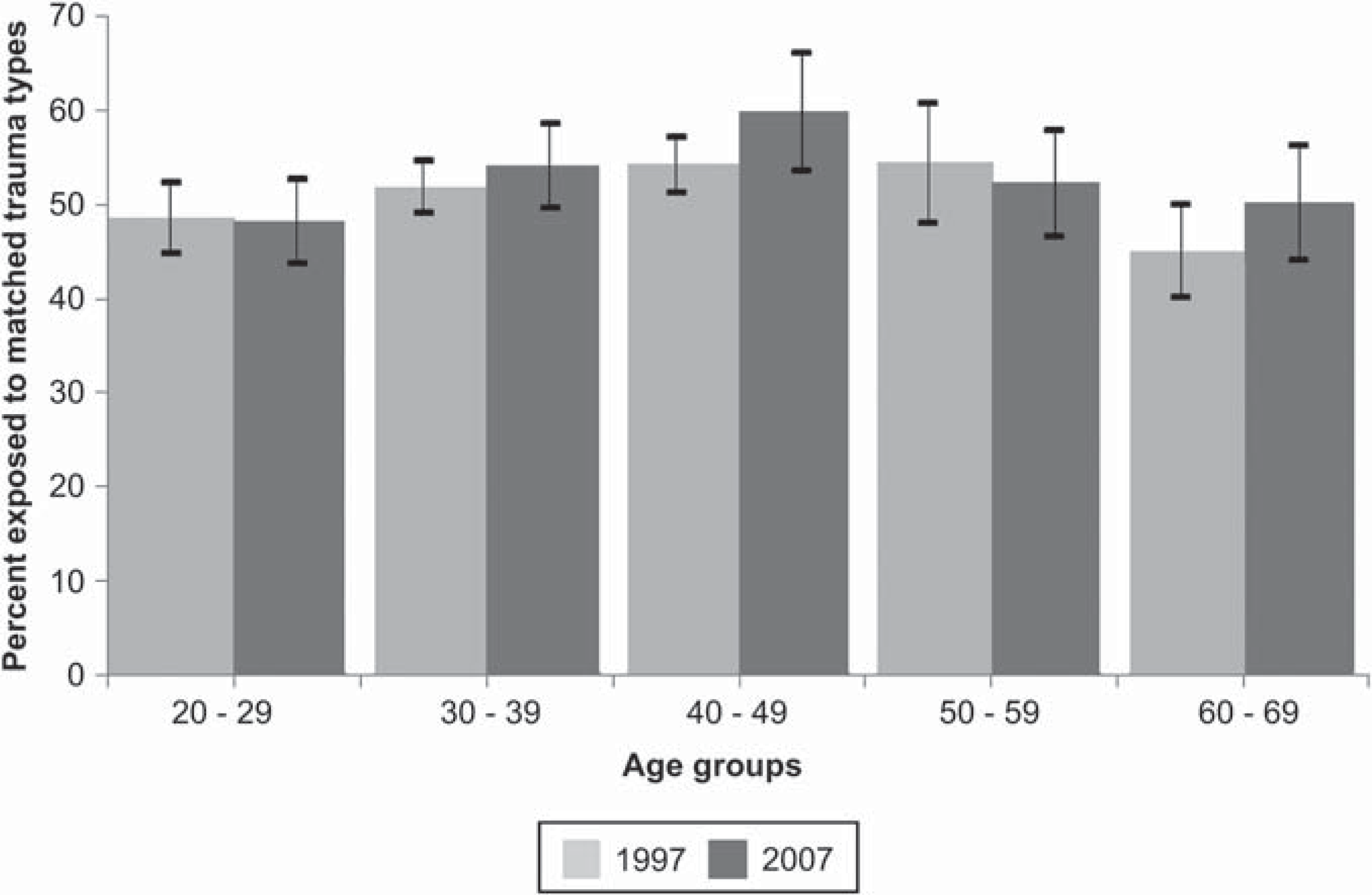
Comparison of the prevalence of exposure to matched events among age-matched women in the 1997 and 2007 NSMHWB.
Discussion
The present study is one of the first to examine the impact of increasing the number of potentially traumatic events listed in population surveys on the prevalence of trauma exposure. To our knowledge, it is the first study to examine this issue longitudinally. Consistent with the findings of Breslau and Kessler [24], the effect of increasing the number of trauma types listed in the CIDI from 11 to 29 was to increase the overall population prevalence of trauma exposure by 18%. In 1997 the population prevalence of trauma exposure was 56.9% compared to 74.9% in 2007. Our cross-cohort analyses revealed that these differences are not indicative of an increase in trauma exposure over time; after controlling for age there were no differences in the prevalence of exposure to matched trauma types among men and women from 1997 to 2007. Rather, the increase was explained by endorsement of new, potentially traumatic events that were not listed in the earlier survey. Thus, epidemiological surveys that utilize less comprehensive measures to assess exposure are likely to result in lower prevalence estimates.
Consistent with many previous studies, these findings suggest that PTEs may not be as rare as originally conceptualized [28]. However, the extent to which the higher rates derived from more comprehensive surveys accurately reflects the level of trauma exposure in the community is a matter of some debate. It might be argued that the list has been expanded to include events beyond what may truly be conceptualized as potentially traumatic, and into the realm of other stressful life events. There is currently significant contention in the PTSD field regarding the issue of ‘conceptual bracket creep’ and its implications for the diagnosis of PTSD [29–31]. While this is a valid debate, it is important to not lose sight of the major public health significance of failing to identify those who have been exposed to potentially traumatic or otherwise stressful life events. Regardless of what they are called, the potential psychological sequelae of such events need to be acknowledged. In their analysis of the Detroit Area Survey, Breslau and Kessler [24] found that the expanded definition of events contributed to a considerable increase in PTSD cases. Close to 40% of the PTSD cases identified were attributable to the five additional events listed. Unfortunately there were a number of differences between the 1997 and 2007 NSMHWB in the assessment of PTSD that precluded such an analysis with this data. Most notably, the 1997 survey obtained a 12-month diagnosis. The 2007 survey on the other hand obtained a lifetime diagnosis, but no 12-month diagnosis (those who reported having any symptoms in the preceding 12 months were categorized as having 12-month PTSD). The method used in the 2007 survey inevitably produces higher 12-month estimates than those used in 1997.
Importantly, the present study observed that the difference in prevalence estimates of trauma exposure obtained from 1997 to 2007 was more pronounced in women than in men. From 1997 to 2007 the prevalence estimates increased from 64.6% to 76% for men, and from 49.5% to 73.8% for women. To our knowledge, the differential impact of varying the number of trauma types enquired about on the prevalence of trauma exposure according to sex has not previously been investigated. However, among a clinical sample, Pierce et al. [17] found that there was a greater increase in the number of event types reported by women than men when comparing a multi-item and a single item trauma assessment. The sex differences observed have important implications regrading the conclusions drawn from previous epidemiological studies. A number of studies have concluded that men are more likely than women to experience PTEs, including the 1997 NSMHWB [4,5,15,32]. The present findings would suggest however, that this result is dependent on the types of traumas enquired about. The present analyses of the 2007 NSMHWB found that men and women did not differ in regard to the likelihood of trauma exposure; however, consistent with previous findings [5,15,32], there were differences in the types of events each gender was likely to have experienced. The inclusion of specific questions relating to partner violence, having been stalked, or having experienced a ‘private event’ in the 2007 NSMHWB may have increased reporting of these events [22,23] which were shown to be more prevalent among women compared to men. Thus, failure to comprehensively assess a broad range of trauma types may lead to erroneous conclusions about sex differences in relation to the prevalence of trauma exposure. It is important to note that differences in reporting of events between the sexes may also reflect differences in the interpretation of events as traumatic as well as actual differences in the occurrence of these events.
While the present study examined the impact of the number of trauma items assessed on trauma prevalence, there are a number of other methodological factors that may influence estimates of trauma exposure which require further examination. In particular, which methods produce the most valid and reliable estimates of trauma exposure: Should self-report checklists or interviewer administered questionnaires be utilized? Should questions be structured, semi-structured, or open-ended? Do estimates differ according to whether the assessment is conducted by a lay or clinical interviewer? While there is some evidence to suggest that estimates are affected by the choice of assessment and assessor [16–19,33], further research is required to determine which conditions are optimal.
Limitations
These findings need to be considered in light of the following limitations. Like other general population surveys, the assessment of trauma exposure in the 1997 and 2007 NSMHWB relied on the use of retrospective self-reports. As such, the results may be subject to recall bias. Other potential sources of bias include selective mortality (particularly that which might result from trauma exposure) and non-response bias, in which exposed or non-exposed individuals may have been more likely to refuse participation [34]. It is unlikely that the 1997 and 2007 NSMHWB have been affected disproportionately by recall bias or selective mortality; however, as the response rate for the 2007 NSMHWB was considerably lower than that achieved in 1997 (60% versus 78%), the former is more likely to have been affected by non-response bias.
Comparisons of the prevalence of trauma exposure between the two surveys must also be interpreted with caution. Differences in methodology between the two surveys mean that the results are not directly comparable. We attempted to increase the comparability of the two surveys by limiting comparisons to matched events among aged-matched cohorts. However, in doing so a number of definitional assumptions were made. For example, it was assumed that in 1997 respondents answered the question pertaining to physical assault with respect to having been assaulted by their parents/guardian, spouse/partner, or someone else; however, this may not have been the case. Additionally, asking about potentially traumatic events that were not included in the 1997 NSMHWB, and the changed ordering of questions in the 2007 NSMHWB may have influenced respondents’ endorsement of the trauma types that were compared across surveys. That is, asking about some trauma types may prompt respondents to remember other trauma types. While this may affect the prevalence of exposure to specific trauma types, it is unlikely to impact of the prevalence of trauma exposure at the aggregate level. Nonetheless, future research comparing alternate methodologies should utilize more rigorous designs such as randomized assignment.
Conclusions
In spite of the limitations detailed above, the present study represents a significant contribution to the literature on the assessment of exposure to PTEs. It is one of the first to examine the impact of increasing the number of PTEs assessed on the population prevalence of trauma exposure, and the first to examine the impact according to sex. The findings underscore the importance of using comprehensive assessments in the measurement of trauma exposure. Previous epidemiological surveys have failed to do so and as such, may have underestimated the prevalence of exposure, particularly among women. While there is considerable debate surrounding what events should be considered as potentially traumatic, prevalence estimates of exposure to a wide range of potentially traumatic, or otherwise stressful, life events is important for the planning and provision of appropriate health care and support services to reduce the burden associated with exposure [28].
Footnotes
Acknowledgements
The authors would like to thank the NSMHWB Reference Group for their input in the survey's design. The authors would also like to thank all those who participated in the survey.