
Abstract
Psychiatric disorder is 3–4 times more prevalent in children with intellectual disability (ID) than in the general population, affecting approximately 40% [1].
The dual disability of psychiatric disorder and ID is a source of major handicap and impairment of adaptive behaviour through loss of educational and social opportunity [2]. Psychiatric disorder is also often associated with physical injury to self or others and adds considerably to the burden of care, personal distress and suffering experienced by the parents and family [3]. The presence of psychiatric disorder add considerable extra cost to the community, for example through the costs of required residential care, injuries to residential care staff and inability to participate in employment programs [4–6].
The majority of prevalence studies of psychiatric disorder in ID have been cross-sectional but have suggested that there is no significant change throughout childhood into adult life [7]. There have only been several longer term follow-up studies of young people with ID which provide data on the trajectory of their psychiatric disorders. A study by Richardson and Koller [8] indicated that the prevalence of behaviour disturbance in persons with ID remains virtually the same from childhood to young adulthood. This epidemiological study involved 192 subjects and reported on psychiatric disorder only in general terms based on a semi-structured interview of the parents and child and the conclusions are thus necessarily limited. The longitudinal study by Pack, Wallander and Browne [9] also demonstrated persistence of psychiatric disorder but was restricted to African American adolescents with mild ID and therefore its findings might not be applicable to the general population and it does not elucidate the course of psychiatric disorders in younger children and in persons with moderate and more severe levels of ID. In the general community the nature of psychiatric disturbance and relative prevalence of certain disorders varies from childhood into adult life [10]. However, it is not known if the pattern of psychiatric disorder varies over time in persons with ID. Only longitudinal data can provide information about the trajectory of various psychiatric disorders and changes in case status which is necessary in order to understand the contribution of various biopsychosocial risk and protective factors implicated in aetiology, adjustment and adaptation. This paper addresses the question of how levels and patterns of psychiatric disorders change from childhood to adolescence in young persons with ID.
Method
Subjects
The Australian Child and Adolescent Development Study provides longitudinal data on a cohort of young people with ID. The cohort consists of an epidemiologically derived representative sample of young persons aged 4–19 years with ID (n = 582) recruited in 1991 from six urban and rural census districts in the States of New South Wales and Victoria. This cohort represents a population of approximately 179 000 young people and reflects the general Australian community in terms of mix of social class and rural/urban environment. The sample is a near complete ascertainment of those with moderate and severe ID, but, in common with other epidemiological studies, under-identifies those with mild ID since these blend in with the rest of the community. Further details about this epidemiological sample are provided in Einfeld and Tonge [11]. The 582 subjects (341 males) of average age 12.2 years (SD = 4.4), were assessed in 1991–1992 (time 1). At time 1, 27.1% of the subjects were aged 3–8 years, 26.4% aged 9–12 years, 29.9% aged 13–16 years, and 16.5% aged 17–19 years. The subjects were reassessed 4 years later in 1995–1996 (time 2) when valid data were obtained from a total of 467 participants, a participation rate of 80.2%. Consistent with longitudinal studies, this reduction in the participation rate is unavoidable. However, there was no difference in the distribution of age (t = 1.26, df = 566, p > 0.05), sex (χ2 = 0.512, df = 1, p = 0.474) and IQ range (U = 19941.5, z = −1.671, p = 0.095), and no difference between the overall scores of psychiatric disorder at time 1 between the participants and non-participants at time 2 (t = 1.43, df = 559, p > 0.05).
Procedures
Data were collected by a questionnaire mailed to parents or principal care givers. A medical and genetic history examination and, where necessary, further investigations were undertaken to establish the cause of ID. In addition, the level of ID as either profound, severe, moderate, mild or borderline was determined by experienced psychometricians based on standard IQ tests.
Measures
The measure of levels of psychiatric disorder was the developmental behaviour checklist (DBC) [12,13]. The DBC is a 96-item questionnaire completed by parents or carers which assesses psychiatric disorder in young people with ID over a 6-month period. It has robust reliability and validity characteristics. The total score on the DBC provides a measure of overall severity of psychiatric disturbance and correlates with child psychiatrists' ratings of severity of psychopathology using Cox and Rutter's definition [14]. The DBC also has six subscale scores derived from factor analysis which describe specific syndromes or patterns of psychiatric disturbance. These subscales are termed ‘disruptive’, ‘self-absorbed’, ‘communication disturbance’, ‘anxiety’, ‘social relating’ and ‘antisocial’. Scores are also available for individual items. Subjects who have DBC total scores greater than 46 have clinically significant levels of psychiatric disorder, as determined by receiver operating characteristic (ROC) analysis, and are regarded as ‘cases’.
Data analysis
Repeated measures analysis of covariance was used to test for within-subjects effects of time on the level of psychiatric disorder, and the interaction between age and time. Sex and IQ level were entered as covariates. Change in overall prevalence of caseness was compared across time points, and change in case status within subjects was assessed using McNemar's Chi-squared for correlated proportions.
Results
Change in psychopathology over time
The mean scores for overall level of psychiatric disturbance and subscale scores at time 1 and time 2 are shown in Table 1. Repeated measures analysis of covariance revealed no within-subjects effect of time (F = 1.79, df = 1, 427, p = 0.18). That is, there was no significant change in overall prevalence of psychiatric disturbance in the 4 years from 1991–1992 to 1995–1996. Similarly, there were no significant changes in the pattern of disturbance as reflected in the subscale scores, specifically; disruptive behaviour (F = 0.71, df = 1, 426, p = 0.40), self-absorbed behaviour (F = 1.66, df = 1, 427, p = 0.20), communications disturbance (F = 0.35, df = 1, 429, p = 0.55), anxiety problems (F = 3.018, df = 1, 432, p = 0.08), social relating problems (F = 0.31, df = 1, 424, p = 0.57), or antisocial behaviour (F = 0.94, df = 1, 434, p = 0.33) across the 4 years.
Means (M) and confidence intervals (CI) of overall behavioural and emotional problems and sub-scale scores at time 1 and time 2, adjusted for sex and IQ level
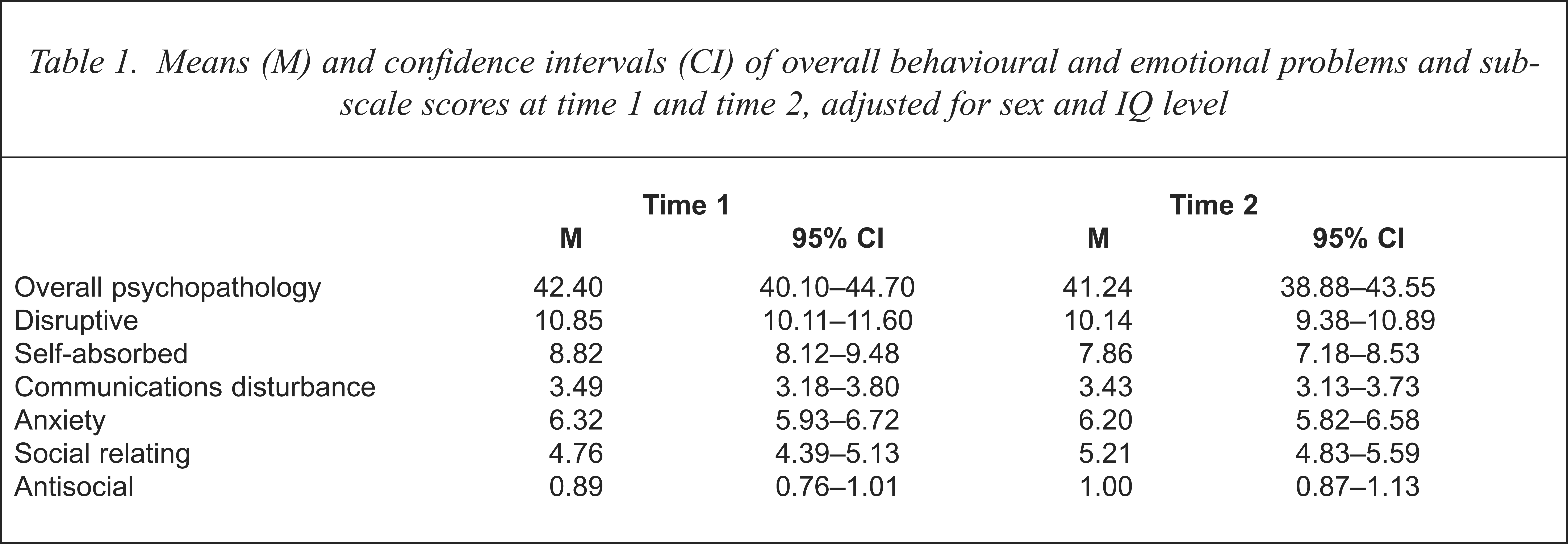
There was no interaction between age and time for overall level of psychiatric disturbance (F = 0.25, df = 3, 427, p = 0.87), disruptive behaviour (F = 0.62, df = 3, 426, p = 0.60), self-absorbed behaviour (F = 1.134, df = 3, 426, p = 0.34), communications disturbance (F = 0.40, df = 3, 429, p = 0.75), anxiety problems (F = 0.07, df = 3, 432, p = 0.98), social relating problems (F = 0.36, df = 3, 424, p = 0.78), or antisocial behaviour (F = 1.14, df = 3, 434, p = 0.34).
Change in clinical status over time
Time 1 and time 2 data were analysed for change in case status over the 4 years. A DBC cut-off score of 46 was used as defined by the receiver operating characteristic (ROC) curve to determine caseness [12]. The proportion of subjects classified as a psychiatric ‘case’ changed from a prevalence of 43.3% at time 1 (n = 563), to 38.6% at time 2 four years later (n = 464). Examination of the change in case status between times 1 and 2 was based on 450 matched subjects. While 18.5% of time 1 non-cases became cases at time 2 and 34.2% of cases at time 1 became non-cases at time 2, the overall change in case status was not significant (McNemar's χ2 = 2.265, p = 0.132).
An alternative method of examining clinically significant change is to use Hageman and Arrindell's [15] reliable change index which indicates that a change of 20 points on the total score of the DBC is considered to be a clinically significant change in overall level of psychiatric disturbance. The results show an approximately equal movement either way with 15% of subjects improving and 13% of subjects deteriorating.
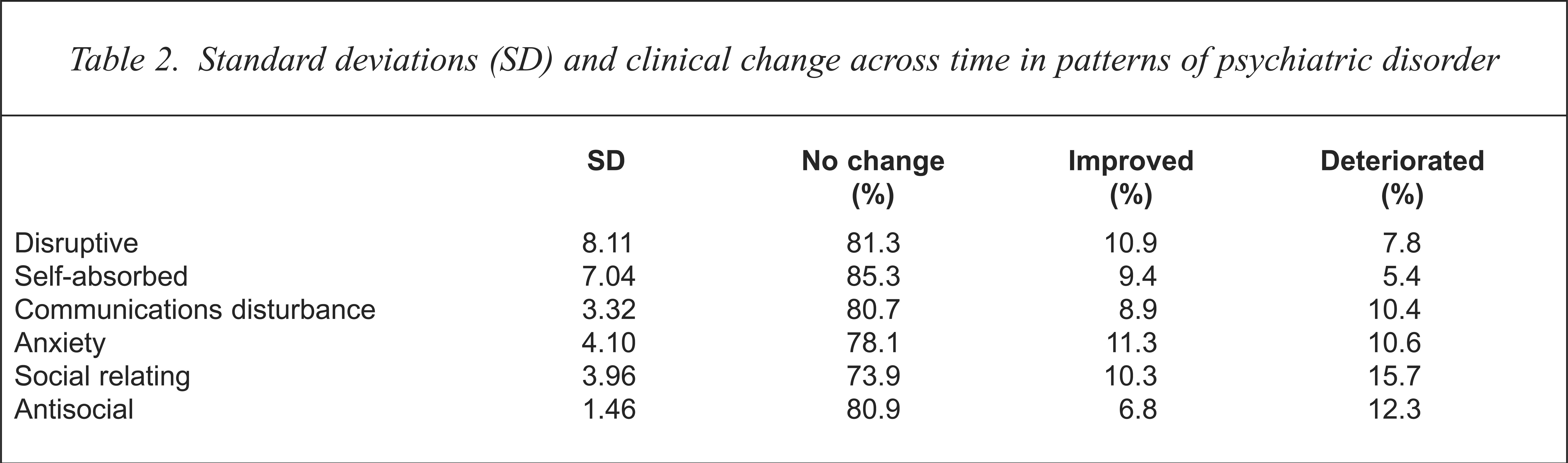
The pattern of disturbance across the six measured dimensions of psychiatric disorder was examined by calculating a change score from time 1 to time 2 using the standard deviations at time 1 for each sub-scale (see Table 2). A change by more than one standard deviation in the subscale score is considered to be a clinically significant change in pattern of psychiatric disturbance. The results show that the majority of subjects did not have a clinically significant change in patterns of disturbance, with approximately equal movements either way (see Table 2).
Standard deviations (SD) and clinical change across time in patterns of psychiatric disorder
Discussion
The main finding of this study is that young Australians with ID have high levels of psychopathology which persist over a 4-year period. The pattern of presenting symptoms in these young people, as reflected in the distribution of subscale or syndrome scores, also does not change during this 4-year period of child and adolescent development. The mean scores for overall psychiatric disturbance at both time 1 and time 2 are near the DBC cut-off score (46) for psychiatric caseness [12] which is a further reflection of the high prevalence of disorder in this group, where psychiatric disorder is the norm rather than the exception. Although there is considerable persistence in psychiatric disorders experienced by these young people, there is still a degree of clinically significant change in both directions with approximately 14% either deteriorating or showing improvement. Given the prevalence of ID of 1.5–2.0% [16–18] and the prevalence of psychiatric ‘caseness’ within ID of approximately 40%, then the number of persons with ID and psychiatric ‘caseness’ is approximately equal to those with schizophrenia which has a lifetime prevalence of 1% [19]. In spite of the finding that this dual disability is numerically as large as the problem of schizophrenia, we have previously found that less than 10% of young people with ID and clinically significant psychiatric disorder receive specialist mental health services [1]. It has been estimated that the provision of a more satisfactory clinical service to persons with ID and psychiatric disorder would require the equivalent of approximately 54 full-time psychiatrists across Australia [20]. The under-recognition of dual disability is in part due to diagnostic overshadowing when a clinician regards the ID as a sufficient explanation and does not make a dual diagnosis and attribute the presenting symptoms to a psychiatric disorder [21,22]. The persistence of serious mental health problems already present at a young age justifies improvements in the availability of early assessment intervention and treatment services for these young people and their families, combined with further research into the contribution of various potential biopsychosocial contributing factors to the development of psychiatric disorder in this population.
A number of factors might have given a false indication of the current observations, however, this is unlikely. Statistical comparisons of time 2 participants and time 2 non-participants provided evidence that there was not a participation bias at time 2. Appropriate statistical controls were employed to account for the influence of severity of within-child factors on the change of psychiatric disorder, and for type 1 error, therefore supporting the findings as true reflections of change. The possibility that a type 2 error occurred is minimal because the sample size provided a high likelihood of finding true changes. Practice effects were unlikely given the 4-year period between data collections. Finally, the results may represent peculiarities and idiosyncrasies in the experiences of those with ID and their families in Australia in the period 1991–1996, and therefore not represent the true natural history of the condition. This is unlikely because our sample came from a variety of rural and urban areas and from two States of Australia with different systems of service delivery.
Conclusion
This study provides the first detailed follow-up information on the course of psychiatric disorders in young people with ID over a period of 4 years. Psychiatric disorder is 3–4 times more prevalent in young people with ID than in the general population [1] and the results of this study indicate no significant change in this prevalence of disorder over a 4-year period. Further, the level of disturbance is generally persistent although an approximately equal proportion of children show either clinically significant improvement or deterioration. These findings of persistent psychiatric disorder, which is of similar dimensions to the problem of schizophrenia, justify a call for research into effective early intervention mental health services for young people with ID and research into the biopsychosocial correlates of improvement or deterioration.
Acknowledgements
This study was funded by Public Health Research and Development Committee, NH&MRC Program Grant 954614. Collection of data was assisted by Kylie Gray. Heather Siddons and Vaughan Rees provided data analyses. Trevor Parmenter, Centre for Developmental Disabilities Studies, University of Sydney, and Gillian Turner, University of Newcastle supported this study as co-chief investigators of the program grant. We acknowledge the contribution of participating families.