
Abstract
Keywords
Significant adult emotional trauma is a well-recognised antecedent to a variety of symptoms, sometimes persistent, which can include nightmares, intrusive memories, flashbacks and emotional numbing. There may also be impairment in domains such as social confidence, competency and occupational performance. Such reactions have been codified in the DSM-IV with the category of posttraumatic stress disorder (PTSD). As a diagnostic entity, PTSD has caused a burgeoning research field in adult trauma, not only in war-related events, but in civilian circumstances such as assault and hostage situations, domestic violence, rape and natural disaster.
The research in children and adolescents has been more recent and has included descriptive studies and reports following disasters such as a school bus hostage scenario [1,2], shipping disasters [3,4], cyclones [5,6], bushfires [7,8] and war-related trauma [9]. With age appropriate modifications [10] research has demonstrated that children in later primary and high school years suffer many symptoms similar to the adult population. Impairments more specific to children include posttrauma diminished academic achievement [9] and the possibility of an altered family style of interaction following a traumatic event [7].
Research into the effects of motor vehicle accidents (MVA) on both adults and children has been limited. This is somewhat unusual given the high prevalence of MVAs, which in Australia until 1995 were the commonest cause of death in the 19–24 years age group. An MVA may fulfil DSM criterion A for PTSD: that is an MVA may cause actual or threatened death or a perception of threatening the physical integrity of the person(s) involved and intense fear, helplessness or horror were features of the victims emotional response. Further, clinical experience presents face validity to the potentially traumatic nature of MVA's with children. Indeed, forensic and insurance bodies frequently request the assessment of the psychological impact to the child following their involvement in a motor vehicle accident.
Research with adult samples has reported that anxiety, intrusive and avoidance symptoms are common reactions during the initial period following an MVA. Blanchard et al [11] found that 46% of adults seeking medical attention following a MVA met diagnostic criteria for PTSD when assessed with the Clinician Administered PTSD Scale [12]. A further 20% had a subsyndromal version. Other prospective studies have found varying rates of PTSD in adult populations ranging from 11% [13] to 25% [14]. Other psychological sequelae include changed attitudes toward driving among PTSD sufferers, discrete travel-related phobias, generalised avoidance behaviour or avoidance of all non-essential travel [11,13,15,16]. In some cases, travel anxiety can be chronic and debilitating [13,16]. In addition to continued physical and medical disability, MVA victims report increased levels of mood disturbance, anxiety, depression, somatisation, help-seeking behaviour and impaired social- and work-related functioning [3,13,17–20].
In MVA trauma the extent of physical injury sustained was found to be predictive of poor psychological outcome [21]. Fear of death and perceived life threat during or immediately post-MVA were also found to be predictive of PTSD independent of the extent of physical injury; this is consistent with findings following disasters [22]. Blanchard et al. found a 39% rate of PTSD in a self-selected sample of adult MVA victims [23]. They retrospectively defined four variables predictive of 70% of PTSD: prior major depression, fear of dying in the MVA, extent of physical injury and litigation proceedings. While other studies have confirmed that perceived life threat is predictive of PTSD, the association with extent of physical injury has not been consistently reported [13,14].
Symptom chronicity has been reported in MVA victims. In one study of 98 MVA victims, 40 met criteria for PTSD at 3 months. Of these, 50% no longer met criteria at 6 months and two-thirds had remitted by 12 months [24]. Others report 12-month remission rates of 39% [13,14]. Those who met criteria at 12 months continued to show impaired functioning. Blanchard et al. found three variables predictive of 79% of remitting cases: initial ‘relatively lower scores’ on irritability, sense of foreshortened future and degree of vulnerability felt in a car at the time of assessment [24]. Little is known of the longitudinal course of those who had persistent PTSD.
Despite the frequent involvement of children and adolescents in MVAs, research concerning the emotional sequelae of such trauma lags significantly behind that in the adult population. The aim of this study is to determine the prevalence of PTSD and general levels of psychopathology in a population of school children involved in motor vehicle accidents.
Method
Study population
All patients aged 8–13 years presenting to the Emergency Department of Princess Margaret Hospital for Children, Perth following a motor vehicle accident between June 1996 and September 1997 were reviewed. Subjects were involved in an MVA either as a passenger, pedestrian or bike rider. Children were excluded if they had suffered a severe head injury, a period of loss of consciousness of more than 15 min, a Glasgow Coma Score of less than 12 at presentation or if a significant person also involved in the MVA sustained physical injuries which led either to death or major physical impairment. Children or parents who were non-English-speaking or whose travelling time to the interview exceeded 2 h were also excluded. Demographic and study participation data for all children is presented in Table 1.
Demographic and accident-related data
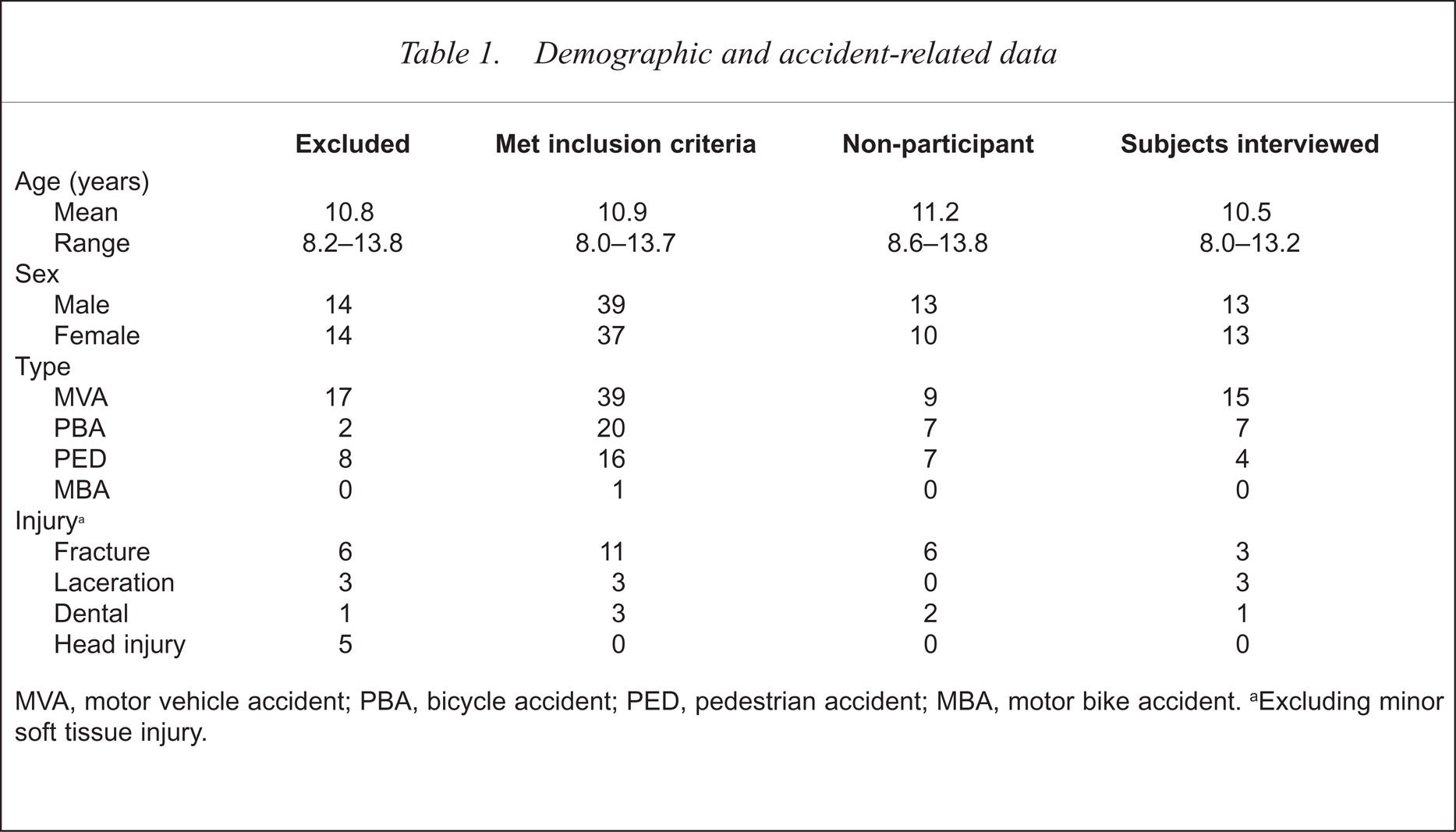
MVA, motor vehicle accident; PBA, bicycle accident; PED, pedestrian accident; MBA, motor bike accident.
Excluding minor soft tissue injury.
Procedure
Individuals who met the inclusion criteria were contacted by letter 1 month after the MVA with information regarding the study and consent to participate was subsequently sought by telephone. Participants were seen 3 months after the MVA by either one of the two investigators. After written informed consent was obtained, a structured clinical interview was conducted. The 3-month interval was chosen to allow sufficient time for the natural resolution of distress in some children and to reduce the rate of false positive diagnosis of PTSD.
Specific instruments
General psychopathology was measured by the Child Behaviour Checklist (CBCL) [25]. To control for the possible confounding effect of parental distress on parental reports of children's symptoms the General Health Questionnaire [26] and the Impact of Events Scale (IES) [27] were also completed by the parent. Child emotional distress was measured by the Post Traumatic Stress Disorder Reaction Index for Children (PTSD-RI) [28], administered by structured interview and described by the following categories: doubtful PTSD (scores 0–10), mild (11–24), moderate (25–39), severe (46–59), very severe PTSD (60–80). The internal reliability of the PTSD-RI and the IES scales were calculated for this sample using Cronbach's alpha. The PTSD-RI scale had a reliability coefficient 0.7820, indicating acceptable internal consistency for this sample. The reliability coefficient for the IES scale was 0.9353, indicating high internal consistency of items. Data were entered and analysed using the Statistical Package for Social Sciences version 7.0 (
Results
Of individuals identified as involved in an MVA, 28 were excluded on the basis of predefined criteria: significant head injury sustained in the MVA (10), death of a parent in the MVA (2), subjects and/or parents non-English-speaking (8), or distance from the hospital more than 2 hours (8). There were 76 subjects who met the inclusion criteria. Twenty-three (30%) of the 76 elected not to participate. They differed from participants only in the smaller number who sustained an injury. Of the 53 who agreed to participate, 27 (51%) did not attend the interview despite a second appointment being offered. The 26 subjects for whom data are available therefore represent 49% of those who agreed to participate but only 34% of those who met the inclusion criteria.
The study sample consisted of 13 males and 13 females with an average age of 10.5 years (8.0–13.2 years). Twenty-three (88.5%) lived in a two parent family, 19 (73.1%) with two biological parents, one (3.8%) with adoptive parents, three (11.5%) lived with a single mother. Two had been seen previously by a mental health professional, one receiving outpatient therapy, and one-third of subjects had a family history of mental illness. None had previous episodes of school refusal or perceived problems at school.
Fifteen (58%) were involved as passengers, seven (27%) on a bicycle and four (17%) as pedestrians. Some form of injury was sustained in 20 (77%) of the subjects, seven of whom (27%) had either fracture (3), laceration (3) or dental trauma (1). Others in the MVA were injured in 42% of cases (parent = 7, sibling = 3, friend = 1). Sixteen subjects (61%) said they saw the moment of the crash. Those who didn't witness the crash were usually bicycle riders struck from behind. Some (44%) saw broken glass and many (64%) remembered seeing car damage or someone at the scene crying (67%). One subject reported seeing a fatality. Some (27%) feared at the time of the accident they would die and seven (37%) perceived some threat to a friend. Two children with a parent involved in the MVA felt their parent may have died. Of all subjects presenting to the Emergency Department at PMH 85% arrived by ambulance. Eighteen (72%) were hospitalised, all but two for less than 1 week. In six cases, one or more other persons were also taken to hospital, all of whom were hospitalised. Following the MVA three subjects (11%) reported a perceived decline in their school achievement while six (23%) reported an improvement. There was no perceived change in the remainder. Only one revealed a sense of foreshortened future or poor future achievement.
Of the two procedures used in this study (clinical assessment and a semistructured research interview) to measure post-MVA PTSD following psychiatric clinical assessment, only two subjects (8%) met all four of the DSM-IV criteria for PTSD: 16% met three, 22% met two, 40% met one. In 16% of cases the child involved did not describe the incident in a manner that fulfilled DSM-IV criteria A. In order of frequency validated: 84% were positive for criteria A (event exposure), 40% for criteria B (re-experiencing phenomena), only 8% for criteria C (avoidance and numbing) and 28% for criteria D (hyperarousal).
Post-motor vehicle accident posttraumatic disorder symptoms
Using the semistructured interview, the PTSD-RL, the most validated symptoms were: feeling the MVA would upset most children (mean score = 1.92), ‘things’ sometimes making the child think it might happen again (mean score = 1.27), being more jumpy or nervous than before the MVA (mean score = 1.23) and going over in their mind what happened (mean score = 1.19). The least-validated symptoms were: has dreams about the MVA or bad dreams since then (mean score 0.19), doing things he or she wouldn't have done before such as fighting or swearing (mean = score 0.23), doing things he or she had stopped doing when younger (mean score = 0.3 1) and feeling so scared, upset or sad he or she couldn't talk or cry about it (mean score = 0.46). While most children validated some symptoms of PTSD at 3 months, the scores were widely distributed with both the mean (16–6) and the median (14.5) in the reported mild range. Of the 26 subjects in our series, there were 11 (42%) doubtful cases of PTSD, 9 mild (35%), 3 moderate (11%) and 3 severe cases (11%). No subject scored in the very severe range.
Concordance of DSM-IV diagnosis and PTSD-RI score
The concordance between a clinical DSM-IV diagnosis of PTSD and the PTSD-RI scores was assessed using three methods. First, the number of DSM-IV criteria met was correlated with total PTSD-Rl scores, revealing a strong positive correlation (r = 0.827, p < 0.01), see Table 2. Second, given the small sample size the number of DSM-IV criteria met was grouped into few (0 or 1) and many (2, 3 or 4) criteria. The mean PTSD-RI scores of the two groups were compared using an independent samples t-test, adjusting for unequal variances. Children meeting two or more DSM criteria had significantly higher PTSD-RI scores (mean = 25.0, sd = 14.1) than children meeting one criterion or none (mean = 9.5, sd = 5.5; t(12) = −3.44, p < 0.01). Third, multiple regression was used to identify the DSM-IV criteria that best predict PTSD-RI scores in children. The four DSM criteria (coded absent or present) were entered simultaneously into a multiple regression with PTSD-RI scores as the dependent variable. The four criteria combined accounted for 73.6% of the variance (adjusted R square) in PTSD-RI scores, F(4,20) = 17.77, p < 0.001. The DSM-IV criterion C (avoidance and numbing; t(23) = 2.76, p < 0.05) and criterion D (hyperarousal; t(23) = 3.43, p < 0.1) were the only significant predictors of PTSD-Rl scores.
General psychopathology in the motor vehicle accident (MVA) sample and the West Australian (WA) Child Health Survey
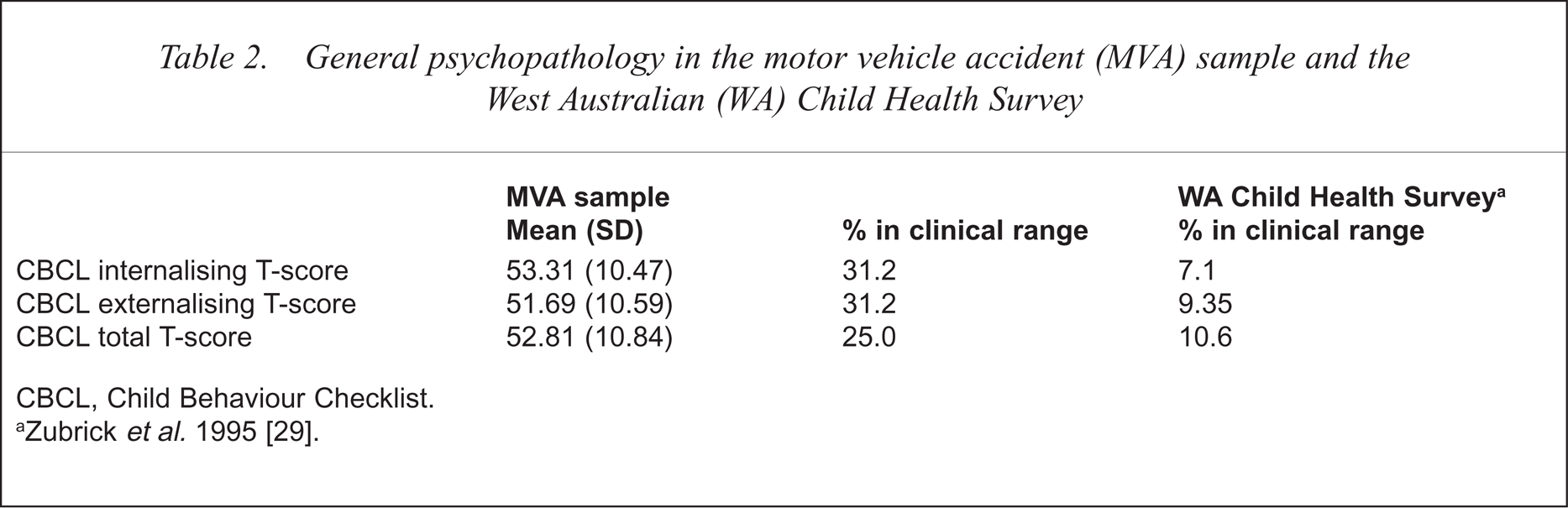
CBCL, Child Behaviour Checklist.
Zubrick et al.1995 [29].
Posttraumatic stress disorder and event-related variables
The relationship between the PTSD-RI scores and other event-related variables was analysed using independent measures t-tests. Children who reported a fear of dying at the time, or immediately after the accident had significantly greater PTSD-RI scores (mean = 26.43, sd = 13) than children who did not (mean = 13.00, sd = 10.28; t(24) = 2.76, p < 05). There were no significant differences in PTSD-RI scores between injured and non-injured children, or between children who had been evacuated to hospital by ambulance and those who had not.
PTSD-RI and parent distress
The IES was completed by 15 parents who were involved in the motor vehicle accident or who witnessed their child's accident. Six parents (40%) were found to be in the mild range (IES total score between 20 and 40) and three (20%) were severe (score > 40) for posttraumatic emotional distress. However, parent's trauma as measured by IES scores was not significantly correlated to either children's general psychopathology measured by the CBCL or the child's PTSD-RI score.
General psychopathology symptoms
The prevalence of mental health problems, defined by a total T-score greater than 60 on the CBCL, was higher than community normative data reported in the Western Australian Child Health Survey [29]: 22.7% versus 16% [t(15.3) = 2.55, p < 05]. The relationship between PTSD and general psychopathology was tested by correlating PTSD-RI scores with T-scores on the CBCL total problems scale and the internalising (anxiety and depression symptoms) and externalising (disruptive behaviour symptoms) subscales (Table 2). There was a significant positive correlation between internalising T-scores and PTSD scores (r = 0.429, p < 05). No significant relationship was found between externalising or total problem T-scores and PTSD-RI.
Discussion
Anxiety, nightmares, intrusive memories and flashbacks are common initial reactions to an MVA. Generally, these symptoms resolve rapidly, but in some, the persistence of symptoms can result in continued emotional distress and impaired social, academic and work-related functioning. This study investigated post-MVA reactions of 26 children who had been involved in an MVA and at that time sought medical attention at a major children's hospital; children were interviewed for this study 3 months after the accident.
The subject population represented 34% of those who met our inclusion criteria and consented to participate. The sample's demographic profile was similar to that of the total hospital-presenting, MVA population for this age range. Low study participation was due to both low levels of parent consent to a psychological evaluation of the child (30%), and failure to attend an interview despite consent being given (35%). Parental consent to participate was less likely if the child sustained injuries more serious than minor soft tissue injury or abrasions. The low participation rate requires caution when interpreting results, however, the skew of the study sample away from the more seriously injured suggests our reported PTSD prevalence may be an under-estimation of the true prevalence in children who present at hospital emergency departments following a motor vehicle accident.
Our study population demonstrated a higher prevalence of emotional and behavioural problems than is seen in the general Western Australian childhood population as measured by the CBCL. The CBCL internalising subscale, which includes anxiety and depression items, was significantly correlated with PTSD symptoms on the PTSD-RI. This finding is consistent with the present DSM-IV placement of PTSD with the anxiety disorders, and gives concurrent validity that this was a sample with significant mental health problems.
Self-report of PTSD symptoms using the PTSD-Reaction Index revealed six (22%) subjects in the moderate or severe range, 35% were of mild severity while a further 42% were doubtful cases. Of importance to the clinician, following the use of several statistical techniques the significant concordance between the total PTSD-RI scores and a clinical diagnosis using DSM-IV criteria remained robust. Following multiple regression analysis, the variables most predictive of elevated PTSD-RI scores were criteria C (avoidance and numbing) and D (hyper-arousal) symptoms. This finding should be regarded as tentative given the small sample size. Nevertheless, report of increased post-MVA autonomic arousal, often reported by parents and teachers in the form of hypervigilance and exaggerated startle-response, should alert clinicians to a potential case of PTSD. Similarly, avoidance and numbing symptoms, often reported by parent as a ‘personality’ change post-MVA, should be followed by a detailed clinical assessment for PTSD.
Event-related variables were generally found not to be significantly related to PTSD, although the statistical power of the study dictates caution in this area. However, the child's perception of threat and fear of death at the time, or immediately after the accident was found to be significantly correlated with total PTSD-RI scores. This supports the findings of previous studies of PTSD in adults following MVAs [13,14,23] and studies of PTSD in children in other settings [30,8]. While 15 adults were involved in, or witnessed, their child's accident, there was no correlation between parental distress measured by the IES and child PTSD-RI scores.
Given the frequency of motor vehicle accidents and the prevalence of PTSD, in this study 22% of the sample were in the moderate to severe range on the PTSD-RI, it is the authors' view that emotional distress in children and adolescents following MVAs is an underrecognised public health problem in Australia and other countries with similar widespread access to motor vehicles. We note the limitations of this study: sample acquisition from a tertiary hospital, a reticience by many parents to allow psychological assessment of their child and a feeling by many parents that their child, in their opinion, was ‘unaffected’ or will ‘get over it’. Further research with children and families is needed to better understand the aetiology of MVA related PTSD, to define the natural history of the condition, the breadth of impairment in social and academic functioning, possible neurobehavioural sequelae and altered family dynamics post-MVA. Future research should include children with more serious physical injuries including those hospitalised post-MVA, a control group of non-MVA and emergency attenders, and a larger sample size that will allow investigation of the differences between individuals who experience a MVA as a car passenger or a pedestrian.