
Abstract
Population studies have often found that the level of utilization of mental health services in the community do not match their need for such services. In Canada [1–3] and the US [4], population surveys have found that between 7.8% and 14.7% of the adolescent and adult populations had received some sort of professional help for mental or emotional problems in the past year. In the Australian National Survey of Mental Health and Well Being [5], the rate of mental health utilization is about 8%. Although persons with psychiatric morbidity constitute the group in greatest need of mental health services, many surveys have shown that only a minority of such people received some form of professional help. This is 614 as low as 18% in Canada and the US [6, 7], and although higher in the Netherlands [8], is only about 34%. In Australia, too, only 35% of people with a mental disorder in a 12 month period had consulted for a mental problem during the year, and most had seen a general practitioner [5]. The majority of people in the community with psychological disorders who do not receive care constitute a situation of unmet need. Few populationbased surveys of mental health services utilization matched against the needs and use of such services have been reported in the less developed countries of the world.
The prevailing attitude of the community toward mental health services for mental and emotional problems is an important enabling factor in the utilization of mental health services. Among the few studies that have been done, one has shown a positive disposition toward the use of professional care to be associated with better utilization [9], but not others [3].
Sociodemographic factors like gender, age, marital status, often considered as predisposing and enabling factors [10], have been shown to be associated with mental health service utilization in previous studies [3, 9, 11]. A very limited number of studies have shown ethnic differences in mental health service utilization. Help-seeking for mental health problems meets with greater approval among certain ethnic groups, such as Jewish Americians in the US, and French-speaking Canadians compared to English-speaking Canadian in Quebec, Canada [12, 13]. In the Australian National Survey [14], people from non-English-speaking backgrounds and English-speaking backgrounds were equally likely to use services for mental health problems, and to report that their needs were fully met. Such ethnic differences have not been documented in multi-ethnic Asian populations in the East.
The objectives of this study were to ascertain the extent to which the community prefers (or were inclined) to seek professional help for their mental and emotional problems, the extent of needs for mental health services, and the extent to which they actually sought professional help, and their socio-demographic determinants. The extent to which their need for mental health services, their acceptance of professional help, and other enabling and predisposing factors determine their likelihood to seek professional help was also examined.
Method
Sample
An estimated 92% of Singaporeans (comprising 77% Chinese, 14% Malays and 8% Indians) live in high-rise flats which are located in defined regions (New Towns) around the island. These regions are subdivided in turn, into ‘neighbourhoods’. A representative sample of individuals was selected from households located in five randomly selected regions. A random 1-in-10 sample of housing blocks was drawn, proportionally stratified by ‘neighbourhoods’ within each of the five regions. Disproportionate stratified quota-sampling was employed to obtain about equal-sized samples of respondents from the three ethnic groups (Chinese, Malay and Indians). All household units in each selected block were sampled and one subject each, in the age range 13–64 years was selected randomly for interview. The final sample consisted of 2947 subjects from among 3032 eligible subjects, after excluding a small number of subjects of ‘other races’.
The interview
A team of trained field-workers conducted face-to-face interviews with eligible subjects of the selected households, using structured questionnaires. The questionnaire elicited information on their biodata, recent psychiatric morbidity, their receptivity and preference for mental health services, and actual utilization of mental health services in the past month. The need for mental health services was assessed by the presence of recent psychiatric morbidity, using the 28-item General Health Questionnaire (GHQ-28) [15, 16]. Three language versions of the GHQ-28 were made available: English, Chinese and Malay. Indians in Singapore are usually literate in English or Malay and did not require an Indian-language version. Subjects chose the language version they were most comfortable with. The field interviewer read the questions out to those who were illiterate and assisted those who had difficulties answering the questionnaire. The ‘traditional GHQ scoring’ method was used, with a bimodal response scale of ‘0’ for the first two ordered responses and ‘1’ for the third and fourth ordered response choices. Cultural-linguistic differences between populations in optimum cut-off values used to define a ‘case’ have been documented [17]. In Singapore, we determined different cutoffs of 4/5 for Chinese and 5/6 for Malays and Indians to be appropriate, based on the results of receiver operating characteristics (ROC) analyses using the ICD-10 psychiatric diagnoses derived from the Composite International Diagnostic Interview (CIDI) as gold standard in a subsample of the population sample [18].
To ascertain the community's preference for (or inclination to use) professional help with mental health problems, the respondents were asked: ‘If you were to experience an emotional or mental problem (such as depression or anxiety) that was severe (that is interfering with work or lifestyle) or prolonged (that is, lasting a month or more) would you seek professional help?’ Respondents were also asked about the types of professional caregivers (including GPs, psychiatrists, psychologists, medical social workers, traditional healers and religious counselors) they would seek if they had an emotional or mental problem. The utilization of mental health services was ascertained by asking the respondents whether they had sought any professional help for any emotional or mental problem (such as anxiety or depression) in the past 4 weeks, and the type of professional caregiver they sought help from. We also assessed the adequacy of personal copingresponses to stressful life event situations by the frequency (on a 4-point Likert scale) with which they ‘faced the problem squarely and try to solve it’, or ‘passively resign and withdraw’, or ‘deny and avoid the problem’, or ‘seek support from close relatives and friends’.
Data analysis
Given the stratified random sampling strategy employed in the survey, weighted analyses of the data were employed to provide unbiased population-based estimates of prevalence and associations between variables, with weights for the sample data derived from the demographic distribution of the general population. Differences in proportions between groups were tested for statistical significance (twotailed) with χ 2 tests. Logistic regression techniques were used to identify significant independent predictors of utilization of mental services and estimate odds ratios and their 95% confidence intervals; modelbuilding was performed with forward stepwise selection procedures, with p-values of 0.05 for entry and 0.10 for removal. The analyses were performed using the Statistical Analysis for the Social Sciences (SPSS) package [19].
Results
Only an estimated 37% of the general population indicated they would seek professional help if they experienced a serious emotional or mental problem (Table 1). Although an estimated 16.9% of the population were determined by their high GHQ score to be likely to benefit from mental health services, only 2.6% of the population actually used the services of any professional caregiver. Of the estimated 498 persons with high GHQ scores, only 5.9% sought any professional help. Among those with a high GHQ score and who were receptive to professional help (n = 211), 10.4% actively sought professional help (Fig. 1). General practitioners were the most commonly preferred caregiver (49.3%), and were used by 41.1% of those who sought help (Table 2).
Need, preference and use of mental health services, Singapore National Mental Health Survey, 1996.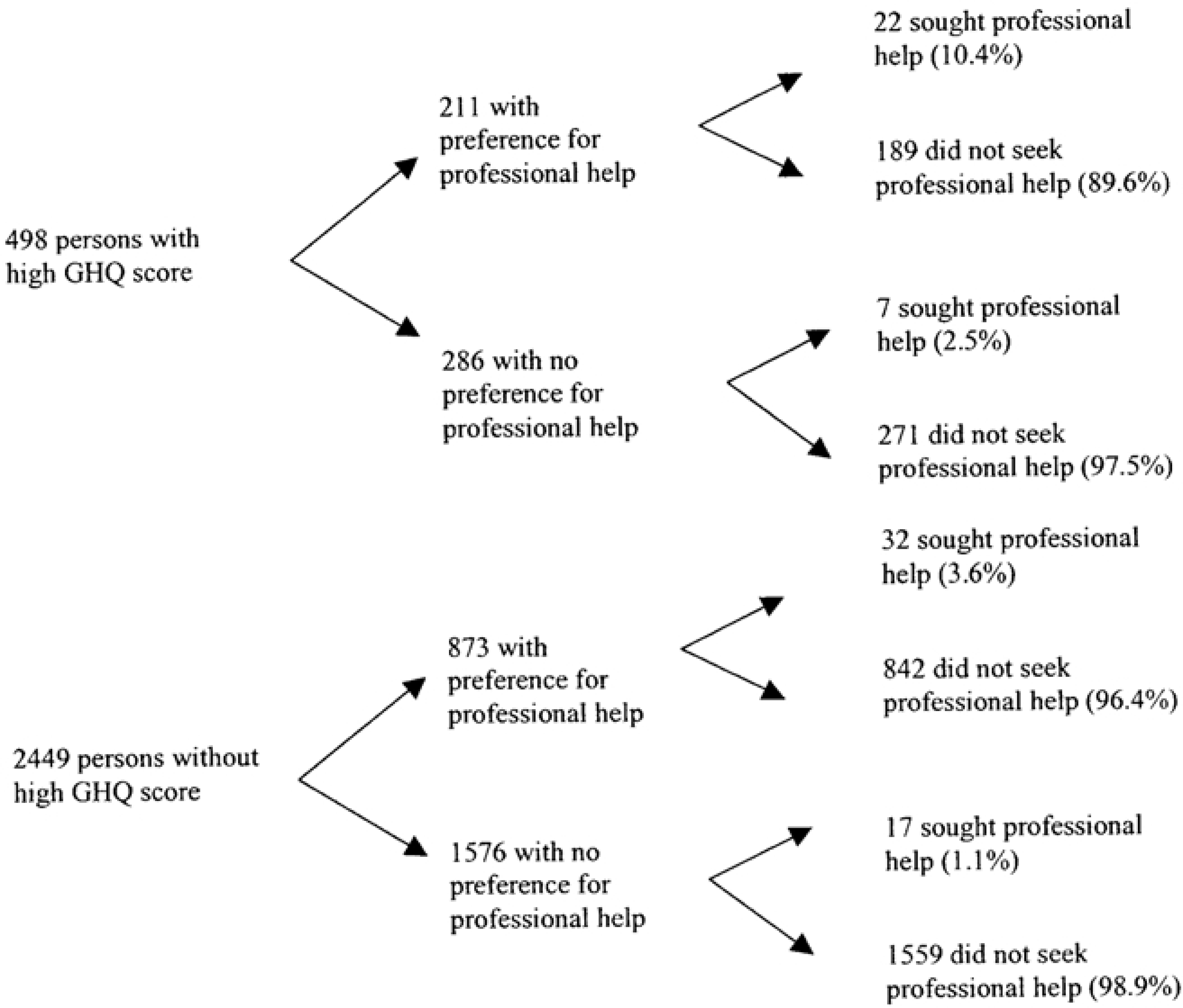
Preference, need and utilization of mental health services (population-weighted estimates), Singapore National Mental Health Survey, 1996
Preferred and realized sources of professional help for emotional and mental problems
Those who were receptive to professional help were significantly more likely to be those with a high GHQ score, who were better educated, and those who were able to cope satisfactorily with stressful life events.
Those with high GHQ scores were significantly more likely to have unsatisfactory coping, to be adolescents and young adults, separated/ divorced/widowed, and those with better education.
Those who seek professional help were significantly more likely to have a high GHQ score, and to be inclined to seek professional help. Malays used mental health services more than Chinese, but they did not show a significantly greater prevalence of high GHQ score, or a greater preference to seek professional help.
In logistic regression modelling, the likelihood of utilization, high GHQ score, receptivity to professional help, and Malay ethnicity were the independent significant predictors of use of mental health services (Table 3).
Significant variables predicting likelihood of seeking help (stepwise selection logistic regression model)
Discussion
Population prevalence estimates of mental health needs, preferences and utilization were derived from survey data collected using clustered stratified probability sampling strategies, with over-sampling of minority ethnic groups (Malays and Indians). To address the biases and errors inherent in this complex sampling design, weighted analyses of the data were performed. The reported estimates of prevalence and odds ratios could therefore be extrapolated to the population from which the sample was derived. Nevertheless, the effect of uncorrected clustering could nevertheless yield different results. Given the high intragroup correlation arising from cluster sampling, the standard errors surrounding the estimates may be wider than observed. Nevertheless, the 95% CI that surround the point estimate of the adjusted odds ratios from the logistic regression modelling were narrow. Given this, we believe the results would not alter substantially the main conclusions in the study.
We have used the GHQ-28, which measures psychological distress, to formally assess the need for mental health care. Studies in recent years have also used instruments such as CIDI to categorize needs in terms of specific psychiatric disorders. The GHQ is short and simple to administer. Also, people's perception and interpretation of their psychological symptoms, particularly with reference to resulting problems of functioning, often determine whether they seek treatment or help, even when their symptoms do not fulfil diagnostic criteria [20, 21]). There is also growing recognition of the value of using screening instruments such as the GHQ to identify psychiatric disturbances for treatment in the primary care setting [22, 23].
In this study, we found that 2.6% of the population used the services of a health care professional, and that only 5.9% of persons with psychiatric disturbance sought professional help. As the GHQ is intended for use in the primary care setting to screen for recent psychiatric disturbance, we had therefore recorded the use of mental health services over the past 4 week period. These utilization rates therefore cannot be directly compared to those reported in other studies, because they are based on different time-periods. Nevertheless, it is clear that, in line with the findings from developed countries, there was a situation of unmet need in Singapore. Although 16.9% of the population was deemed by high GHQ scores to be experiencing some degree of psychological distress, 94% of these people with identifiable need for mental health care, do not seek help. On the other hand, we also found that 2.0% of people with low scores on the GHQ nevertheless had sought professional help for emotional and mental problems. Although this may suggest a situation of overmet need, the results of the Australian National Survey [24] indicated that such people (4.4% of the population) actually showed high levels of perceived met need, and that such findings may often represent successful intervention instead.
As has been uniformly shown in other studies, psychiatric disturbance was clearly the single-most important factor determining the use of mental health services. We have also shown that attitudes toward seeking professional help are important enabling factors of mental health services utilization. This has been reported in few previous studies. The apparent lack of acceptance of professional help for mental health problems is an important reason for unmet needs. Only a little more than one-third of people in the community viewed mental health services as a source of help to solve their mental health problems, unlike other studies that found most people in the West are positively disposed toward the use of these services [8]. It should be noted that we have ascertained this acceptance of mental health services for severe emotional or mental problems (such as depression or anxiety) that incorporates elements of poor functioning and chronicity, thus clearly warranting professional care; yet it was clear that there was a low inclination to seek professional help. A previous study of Chinese university students in Hong Kong who were asked to indicate their inclination to seek help and the resources for consultation on emotional and mental problems showed similarly that they were generally not inclined to seek help and when they did, would most often seek help from medical doctors [25]. Our results concur with a previous study showing that attitudes toward the use of mental health services were affected by the age, sex, race, education, and income of the subjects [8]. Nevertheless, why people do not choose to use mental health services is an area of research that should be investigated further in future studies.
In other studies, residual relationships between sociodemographic factors and the utilization of mental health services were shown after allowing for need factors [3, 8]. Our results, however, showed that although gender and marital status were associated with utilization in this Asian population, they were explained by higher rates of psychological distress and differences in attitude toward seeking professional help. This affirms the overwhelming importance of need and attitudinal factors, and suggests that predisposing socio-demographic factors play subsidiary roles in utilization in this population.
In logistic regression analyses, after allowing for psychological distress and attitude toward mental health services, we found that ethnicity remained a significant predictor of utilization. Such ethnic differences in use of mental health services have also been reported in a limited number of studies. The Malays' help-seeking behaviour suggests that there is better acceptance and tolerance of mental illness among them. However, whether this represents a significant predictor of utilization independent of need should be confirmed by further studies. The best threshold of GHQ score to determine ‘caseness’ has been shown to vary greatly in different settings and cultural linguistic groups [17, 18]. It is possible that if a cutoff lower than 5/6 had been employed for case definition in our study, Malays might indeed have a higher prevalence of psychological distress that could explain greater utilization. Re-analyzing the data using the same cutoff of 4/5 for all ethnic groups resulted in a reduced odds ratio and a logistic regression model that no longer retain ethnicity as a significant independent predictor of utilization.
The low rate of mental health service utilization among Chinese despite a higher level of psychiatric morbidity was not surprising, as their cultural beliefs greatly influence their illness behaviour and helpseeking. It is well known among specialist mental health service providers that fear and shame often cause them to avoid seeking help from mental health professionals until the problem becomes too severe or difficult to handle at home. Many Chinese patients seek help from traditional healers before going to mental health professionals. Among Chinese psychiatric patients, 22% believed that they were possessed by spirits causing them to behave and think abnormally, and 36% consulted a temple medium before coming to the hospital [26].
In conclusion, we found that high GHQ score, attitude toward professional help and Malay ethnicity were the most significant predictors of use of mental health service among adult Singaporeans. Despite this, they still do not explain why a large majority of the population choose not to use mental health services. More studies are needed to understand their help-seeking behaviour for mental health problems.
Footnotes
Acknowledgements
This study was supported by a grant from the National Medical Research Council of Singapore.