
Abstract
Approximately 7.3 million Australians aged 16–85 years have had a mental disorder at some stage in their lifetime and 20% of all Australians in this age group will have experienced symptoms in the past twelve months [1]. Furthermore, in the June quarter of 2007, 192 246 Australians were receiving government assistance because they had a psychiatric or psychological illness (Australian Government/Centrelink, personal communication, October 2008) that had an impact on their ability to function in society (e.g. inability to work for the next two years) [2]. In 2008, mental illness accounted for 10.3% of total years lived with disability [3] and this is projected to increase to 12.6% in 2030 [4].
Australia has made considerable progress in tobacco control resulting in a halving of overall smoking rates to less than 20% since 1983 [5]. However, the rate of smoking among people with a mental illness is still very high [6]. Extrapolations of Australian estimates indicate that 36% of adults with an affective, anxiety or substance use mental disorder at some time in the previous 12 months smoked regularly compared to 19% of Australian adults who did not have a mental illness in the previous twelve months [1].
In addition to higher overall smoking rates, daily tobacco consumption is higher among people with a mental illness than those without [7]. A recent New Zealand study observing a 12-month population prevalence of mental illness of 21% confirmed the association between smoking and mental illness and indicated that approximately 33% of all cigarettes are consumed by people with a mental illness [8].
Epidemiological studies reveal that consequent to their higher smoking rates, people with a mental illness have higher levels of cardiovascular and other diseases [9]. In addition, mortality rates for cardiovascular disease in this population are increasing; indeed, it is cardiovascular disease rather than suicide that causes the most deaths [10].
Individuals with a mental illness are marginalized both socially and economically [11]. It has been argued that tobacco control has not focused sufficiently on the needs of these individuals [12] and their smoking behaviour is also often overlooked by mental health professionals. Furthermore, barriers to promoting cessation exist as mental health workers and health professionals (i) lack confidence, or the skills and knowledge required to undertake cessation interventions; (ii) believe that their patients are either not interested or not able to quit [13]; (iii) believe that cigarettes serve as a calming device [14]; or (iv) believe that smoking is one of the few pleasures available to them [15]. There is a growing body of evidence demonstrating that people with a severe mental illness can and are able to quit; however these studies have tended to focus on inpatient populations [16–18].
Whilst it is well established that people with a mental illness have higher rates of smoking and that they are interested in quitting, most of these data are based on studies of inpatient populations and there is a dearth of recent, population-based, representative data on this issue. In addition, this study adds value to the literature as it examines factors associated with smoking prevalence including measures of smoking dependence, awareness of the health effects of active and passive smoking, the presence of smoke-free homes and cars and awareness of various anti-smoking media among both smokers with and without a mental illness.
Materials and methods
Ethics approval was obtained for this research from Cancer Council SA's Human Research Ethics Committee and the SA Department of Health Research Ethics Committee. Data were collected as part of the South Australian Health Omnibus Survey in 2005, 2006 and 2007 [19]. The Health Omnibus Survey is conducted face-to-face. It uses a multistaged, systematic clustered area sample of households in the Adelaide metropolitan area and regional centres. Each survey draws independent samples of 4,400 households with an observed response rate in the order of 70% yielding approximately 3000 completed interviews per annum. All data presented in this paper are weighted to the South Australian population by age, sex and geographic area.
Two questions were included to assess mental illness. ‘Are you currently receiving treatment for anxiety, depression, or any other mental health problem?’ was designed to assess ‘general’ mental illness and ‘Are you currently receiving the disability pension on the basis of a psychological or psychiatric illness?’ was designed to assess ‘severe’ mental illness. The questions were derived from previous population measures of mental illness used by the South Australian Department of Health.
Smoking status was determined by asking respondents whether they currently smoke cigarettes, cigars, pipes or other tobacco products on a ‘daily’, ‘at least weekly’, ‘less often than weekly’ basis or ‘not at all’. Those who indicated that they smoked daily, at least weekly, or less often than weekly, were classified as current smokers. In addition, the surveys included indicators such as awareness of the health effects of active and passive smoking, tobacco consumption, time to the first cigarette in the morning, quitting behaviour, quitting intent, and exposure to passive smoking (e.g. smoke-free homes and cars). Postcode data were merged with the Socio-economic Index for Areas 2001: Index of Disadvantage to allow analyses by ecological measures of level of disadvantage [20].
Data for 2005–2007 were merged yielding a total sample size of 8417. Statistical analyses were undertaken using StataSE 8 the estimating tools of which account for the clustered, stratified survey design. Single variable logistic regression models compared smoking rates by mental illness status, levels of dependence, knowledge and behaviour among smokers, and cessation aids and methods used. Those with a severe and general mental illness were compared to the reference group with no mental illness. When there were no differential effects across the two mental illness categories on the dependent variable, a combined mental illness group (general or severe) was compared to the reference group.
Results
Prevalence of mental illness
Overall, 1.6% of the sample was classified as having a severe mental illness and 6.9% as having a general mental illness. The two groups combined represented 8.5% of the population.
Demographic characteristics
Table 1 demonstrates that people with a general mental illness did not differ in terms of age, education or level of disadvantage compared to those without a mental illness. However, those with a general mental illness were more likely to be female, less likely to be married or in a de-facto relationship and more likely to be separated, divorced or widowed than those with no mental illness. Those with a severe mental illness were skewed towards middle age, less educated and tended to live in areas of more disadvantage compared to those without a mental illness. Similarly to those with a general mental illness, those with a severe mental illness were also less likely to be married, and more likely to be separated, divorced or widowed compared to those with no mental illness.
Demographic characteristics by mental illness status among South Australians aged 15 years and over, 2005–2007†
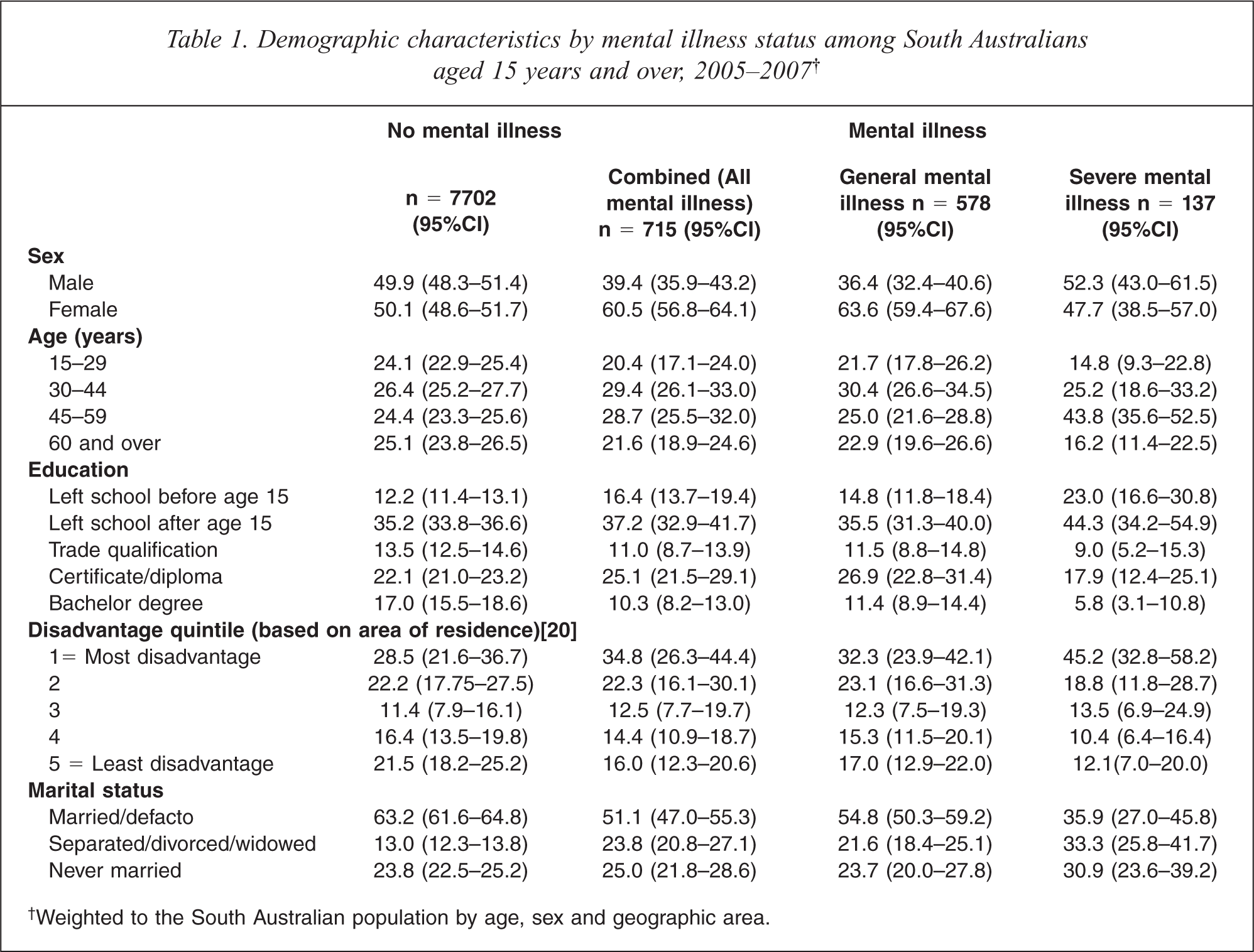
†Weighted to the South Australian population by age, sex and geographic area.
Comparison of smoking rates
Individuals with a mental illness were more likely to be current smokers and more likely to smoke more than 20 cigarettes a day (Table 2). Further analysis revealed that current smokers with no mental illness smoked a mean of 14.9 cigarettes per day (95%CI = 14.2–15.5); those with a general mental illness smoked a mean of 17.0 cigarettes per day (95%CI = 15.4–18.5) and those with a severe mental illness smoked a mean of 21.4 cigarettes per day (95%CI = 18.7–24.1). Among smokers, those with a severe mental illness were more likely than those without a mental illness to smoke within the first fifteen minutes of waking, a marker of severity of addiction. In addition, they were less likely to report that they were seriously considering quitting in the next 6 months.
Smoking status and smoking dependence†
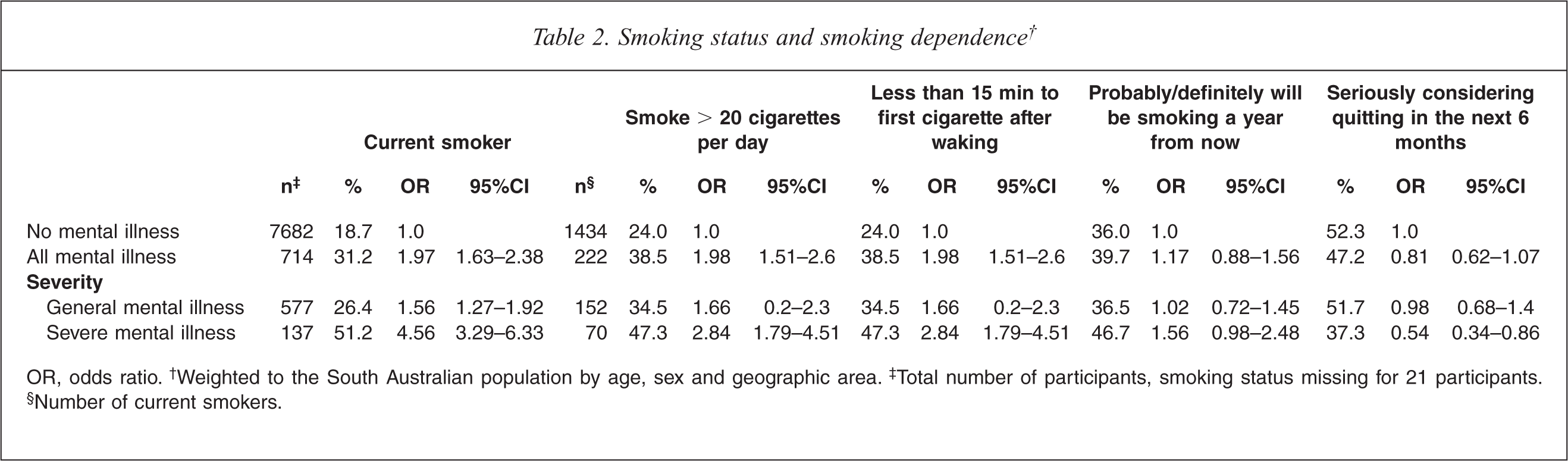
OR, odds ratio.† Weighted to the South Australian population by age, sex and geographic area.‡ Total number of participants, smoking status missing for 21 participants.§ Number of current smokers.
Table 3 shows high awareness of the health effects of active smoking among smokers. Smokers with a severe mental illness were, however, less likely to be aware of the health effects of passive smoking than those without a mental illness. Smokers with a severe mental illness were significantly less likely to live in smoke-free homes than smokers without a mental illness. There was no significant difference between groups on smoking in cars, among those who owned cars. However, further analysis revealed that having a ‘smoke-free’ car was significantly less prevalent among the broader population with a severe mental illness (including non-smokers) compared to the broader population without a mental illness (OR = 0.27, 95%CI 0.16–0.46).
Awareness of the health effects of active and passive smoking and smoke-free homes and cars among smokers†
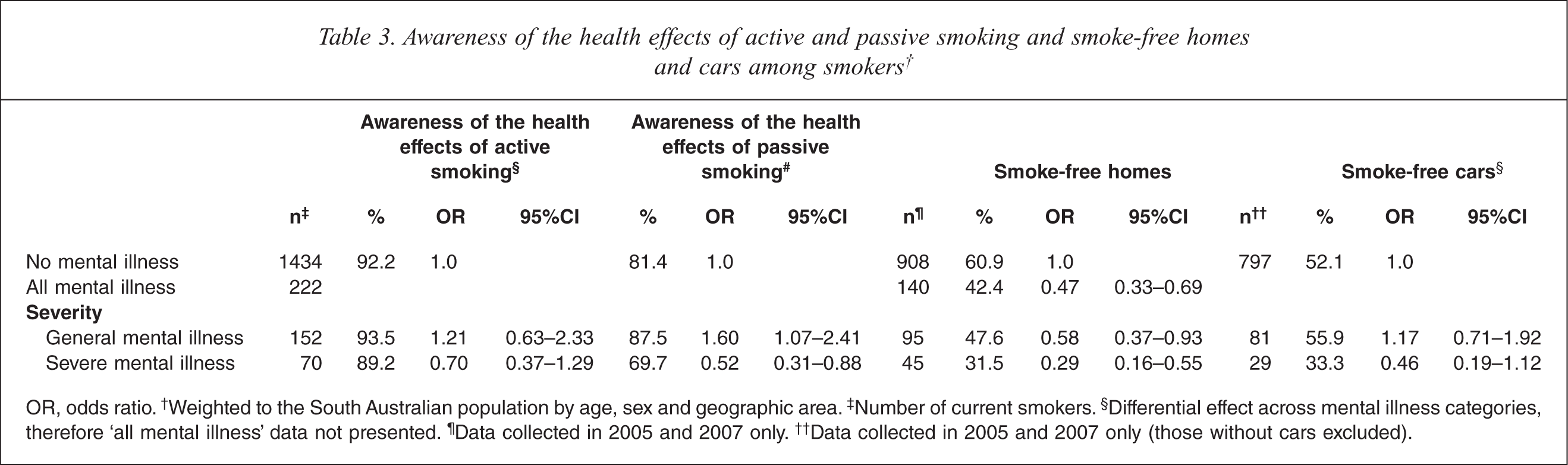
OR, odds ratio.† Weighted to the South Australian population by age, sex and geographic area.‡ Number of current smokers.§ Differential effect across mental illness categories, therefore ‘all mental illness’ data not presented.¶ Data collected in 2005 and 2007 only.†† Data collected in 2005 and 2007 only (those without cars excluded).
Among smokers there was high recall of television advertising about the health effects of smoking for all groups (Table 4). In addition, all groups were equally likely to recall seeing health warnings on cigarette packets, post-implementation of compulsory graphic health warnings in 2006. However, smokers with a mental illness were significantly less likely to recall hearing anti-smoking messages on the radio.
Proportion of smokers noticing warnings of the health effects of smoking through various media and use of cessation aids among smokers who had tried to quit in past year†
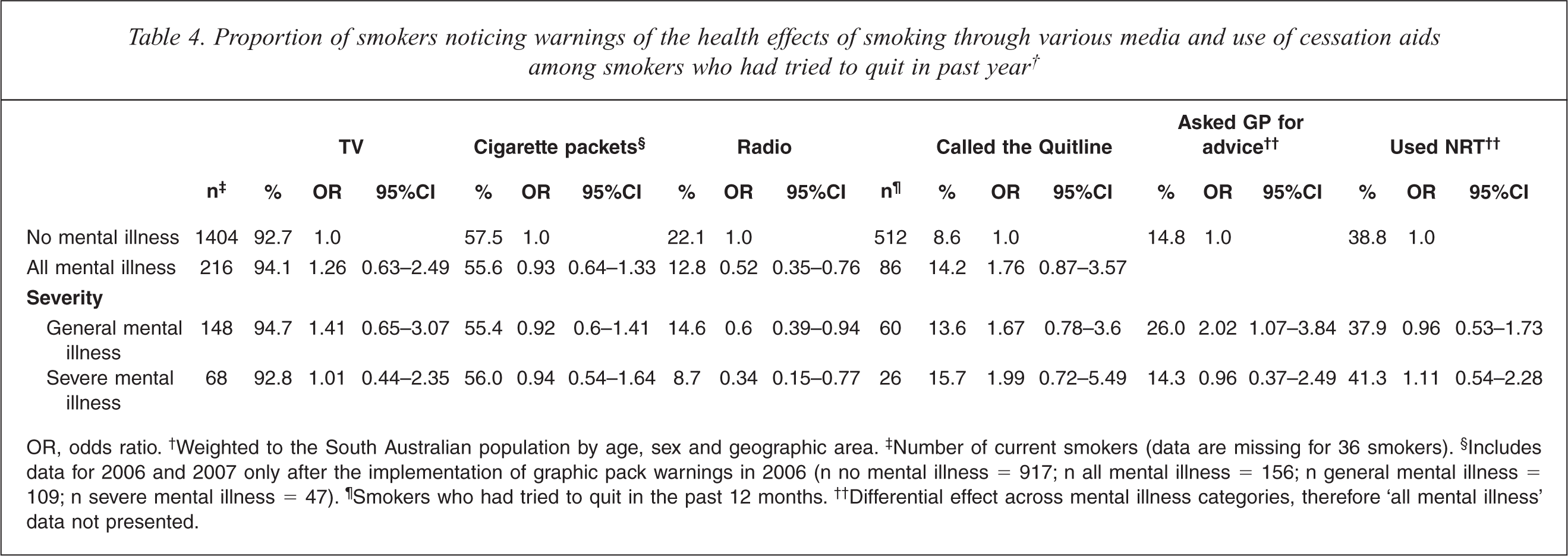
OR, odds ratio.† Weighted to the South Australian population by age, sex and geographic area.‡ Number of current smokers (data are missing for 36 smokers).§ Includes data for 2006 and 2007 only after the implementation of graphic pack warnings in 2006 (n no mental illness = 917; n all mental illness = 156; n general mental illness = 109; n severe mental illness = 47).¶ Smokers who had tried to quit in the past 12 months.†† Differential effect across mental illness categories, therefore ‘all mental illness’ data not presented.
Cessation attempts and use of cessation aids and techniques
Overall, 79% of all current smokers reported that they had attempted to quit smoking at some time in the past (78.1% of those with no mental illness, 85.4% of those with a general mental illness and 82.9% of those with a severe MI). The difference between those with a general mental illness and those with no mental illness was significant (OR = 1.69, 95%CI 1.05–2.73). Overall, 35.7% of smokers with no mental illness, 39.8% of smokers with a general mental illness and 36.6% of those with a severe mental illness had attempted to quit in the past year. Among the population overall, 29.7% were ex-smokers (29.7% of those with no mental illness, 31.4% of those with a general mental illness and 24% of those with a severe mental illness). Logistic regression analysis showed no significant difference in ex-smoking status between those without a mental illness and those with a mental illness (either severe or general).
Respondents who had made a quit attempt in the past year were asked what methods they had used to help them quit. Table 4 shows that there was no significant difference between groups in use of the Quitline or nicotine replacement therapy (NRT). However, smokers with a general mental illness were more likely to report having asked their general practitioner (GP) for advice to help them quit. Respondents were also asked whether there was anything else they had done to help them quit over the past year. There was no difference between the groups on methods e.g. cut down or unassisted (unprompted), however those with a general mental illness were less likely to report quitting without any aids than those without a mental illness (7.7% versus 17.1% respectively).
Discussion
This study revealed that the smoking rate among adults with a general mental illness was one and a half times that of adults without a mental illness (26.4% versus 18.7%). This raised smoking rate is consistent with recent survey findings in New Zealand [8]. Furthermore, the smoking rate among those with a severe mental illness (51.2%) was almost three times that of the community without a mental illness. These figures may be a slight under-representation, as they do not explicitly include those with substance abuse disorders and sampling excluded institutionalized individuals. Consistent with previous studies, those with a mental illness were more dependent on smoking than those with no mental illness [6,7]. Furthermore there was a positive relationship between severity of mental illness and daily tobacco consumption.
Consistent with findings from studies conducted in clinical settings, motivation to quit among those with a mental illness (particularly those with a general mental illness) was high, as exemplified through previous quit attempts in the past year [7,21]. Interestingly, a significantly higher proportion of smokers with a general mental illness (85.4%) and people with severe mental illness (82.9%) had attempted to quit in the past (ever) compared to those without a mental illness (78.1%). However, the proportion of ex-smokers in the population was not significantly different between groups, indicating that whilst the motivation to quit was certainly higher for those with a general mental illness, they may require more cessation attempts and/or additional support to be successful.
This study extends previous research by examining awareness of the health effects of both active and passive smoking and revealed that all groups were well-informed about the effects of active and passive smoking. While there was certainly no evidence of lower levels of awareness about the effects of active smoking among those with mental illness, those with severe mental illness were less likely to be aware of the harms of passive smoking. This may be a contributor to, or exacerbated by, those with a severe mental illness being more likely to be exposed to and/or allow passive smoking in their homes and cars. Tobacco control policies to restrict smoking in public places, and normalizing not smoking in confined spaces may have potential to influence this population disproportionately.
In addition, this study extends previous research by studying awareness of various anti-smoking media. Overall, over 90% of all respondents reported that they had noticed warnings of the health effects of smoking on television. Mass media is an important part of a comprehensive tobacco control strategy and has been associated with increased smoking cessation and declines in smoking prevalence in the general population [22]. However, in recent years some have expressed concern that it may not reach nor be as relevant for priority groups such as people with a mental illness. This study challenges this myth as it demonstrates that people with mental illness are hearing health messages about smoking.
New graphic cigarette packet warnings, designed in part to communicate effectively with disadvantaged groups including those with low-literacy, were reaching smokers with a mental illness equally well as others. In contrast to this, however, radio advertising did not fare well among smokers with either a general mental illness (14.6%) or a severe mental illness (8.7%) compared to the general population (22.1%). Health professionals should consider whether radio is a cost-effective communication strategy for the population overall, especially as it does not seem to influence this significant priority group.
This study did not find a difference in contact with the Quitline by mental illness status; in fact there was a slight but not significant trend toward those with a mental illness being more likely to contact the Quitline for assistance. Cessation help lines have been shown to double abstinence rates in the community [23]. Concerns have been raised about the accessibility and appropriateness of a general cessation helpline for priority groups; however, these data confirm that this service is already being accessed by smokers with a mental illness.
Those with a general mental illness who had attempted to quit in the past year were more likely to have asked their GP for advice. Currently there are no incentives for GPs in Australia to provide cessation advice or to refer individuals to the Quitline. The majority of patients with severe mental illness are in frequent contact with primary care services, and for many this is their only health service contact [24]. Evidence from a recent study in Victoria indicated that GP referrals to a Quitline service resulted in increased cessation compared to standard GP management [25]. In addition, evidence also reveals that individuals who are referred to the Quitline had better cessation outcomes at 6 months, than those who self-select to a Quitline [26]. Thus there is a need for health authorities to develop incentive programmes to encourage practitioner referrals to the Quitlines. Furthermore, practitioners should feel confident in asking patients with a mental illness about their interest in quitting smoking.
Some study limitations need to be considered. Firstly, the data reflect the non-institutionalized population, not including the relatively small population in institutions such as residential facilities, hospitals or prisons. This will result in an under-ascertainment of people with a mental illness who may have a different smoking profile than those captured by the sampling method described. With increasing de-institutionalization, or at least increasing de-hospitalization occurring globally [24] and in South Australia, this effect is likely to be reduced.
Secondly, the survey tool to assess mental illness is a self-report single-item measure based on population items to measure chronic diseases such as asthma and diabetes. Comparison of demographic characteristics (e.g. age, gender and marital status) for the mental illness groups observed in this study with Australian Bureau of Statistics’ data indicate good face validity of both the survey tool and the population surveyed. Furthermore, self-report data of chronic disease status is widely used in health surveillance systems [27]. In addition, comparisons were undertaken with the National Mental Health survey which indicated that 5.5% of the population currently have an anxiety disorder and 3.8% of the population have an affective disorder [28]. It is likely that the method used in this paper will result in a conservative estimate of mental illness, as it is a measure of whether an individual is currently receiving treatment or the disability pension for mental illness rather than a 12-month prevalence. It is likely that this survey will not represent individuals with undiagnosed mental illness or substance abuse disorders; therefore, the results are likely to be conservative. Another limitation of this study was the verification of smoking status, this study relied on self report data to assess smoking which may underestimate smoking when compared to a CO monitor which measures the actual levels of carbon monoxide inhaled from tobacco smoke.
In conclusion, tobacco smoking and mental illness is a growing and significant public health concern in Australia and globally. The results presented here indicate that whilst smokers with a mental illness certainly are more dependent on their smoking, they are in fact interested in quitting. There are a number of mainstream tobacco control strategies that could be further utilized (e.g. mass media; health professional referrals to the Quitline and smoke-free cars legislation) to increase cessation among this group.
Footnotes
Acknowledgements
Sincere thanks to Professor Phil Ryan for his statistical advice, Maxie Ashton for reviewing this paper and to Deb Shaw for editing this paper.