
Abstract
Tobacco use among people with mental illness
The rates of tobacco use among people with mental illness are consistently reported to be much higher than the rates within the general population [1–3].
The 1997 Australian Bureau of Statistics’ Survey of Mental Health and Well-being found 18% of the population over 18 years of age had an affective, anxiety or substance use mental disorder at some time in the 12 months prior to the survey [1]. Of these, 39.5% smoked daily, compared to 23.3% of Australian adults generally (The Australian Bureau of Statistics, personal correspondence, 2005).
Rates of smoking among some subgroups of people with mental illness have been found to be higher again. A national survey of people living with psychotic illness in Australia found that 73% of men and 56% of women smoked tobacco [2]. People with mental illness also tend to smoke more cigarettes per day, with a meta-analysis of over 40 studies over 20 nations finding, in most studies, smokers with schizophrenia and other types of severe mental illness smoked significantly more heavily than smokers within the general population [3].
Not only are smoking rates high among those with mental illness, but people with mental illness make up a substantial proportion of all smokers. The 1997 Australian Bureau of Statistics’ Survey of Mental Health and Well-being revealed 35% of all smokers aged between 18–39 years had suffered an affective, anxiety or substance use mental disorder in the previous 12 months [1,4]. In a study in the USA, 40.6% of current smokers reported having a mental illness in the past month and it was calculated 44% of the cigarettes smoked in the USA are smoked by people with mental illness [5]. A recent study conducted in New Zealand estimated 33% of all cigarettes are consumed by people who had experienced an anxiety, mood or substance use disorder in the 12 months prior to assessment [6]. Access Economics also reported people living with mental illness are now 38.8% of all adult smokers in Australia, and they smoke at least 42% of all cigarettes sold [7].
Many reasons for the high rate of tobacco use by this group have been proposed including biological factors and a range of psychosocial reasons such as a lack of social support, cognitive function, anxiety, side effects of medication and limited coping skills [8].
The high rates of tobacco smoking among people with mental illness and the significant proportion of smokers who have mental illness make this a serious public health concern which needs to be addressed by tobacco control and mental health services.
The impact of tobacco use for people with mental illness
The physical health effects of tobacco smoking within the general population have been well documented [9], with almost two thirds of long-term smokers dying as a result [10]. On average, smokers lose 13–14 years of their life and many spend their last years with significant illness and disability caused by tobacco use [11].
Smoking places a high financial burden on many people with severe mental illness, especially those living on a disability pension or limited income. Many spend a significant percentage of their income on cigarettes and this can make it difficult to afford food, clothing, stable accommodation and other basic necessities [12,13].
Tobacco smoking has become less acceptable in enclosed public spaces, and those who are heavily dependent may find themselves uncomfortable and as a result have more difficulties reintegrating into community life.
Population-wide cessation interventions
Public health campaigns addressing tobacco use within the general Australian population have been very effective. Mass media campaigns, public policy initiatives such as taxation and clean indoor air laws as well as well-delivered cessation services have helped thousands of smokers to quit [14]. Many people with mental illness experience significant and ongoing disability associated with their mental illness including loss of confidence and difficulties with activities of daily living. This can impair their self-efficacy, ability to manage their health and to seek help, making it more difficult to take advantage of population-wide health promotion measures [1,2].
A few interventions provided specifically for this group of smokers have been reported in the literature, and have shown promising results [15–18]. This paper describes the methodology and outcomes of the South Australian Tobacco and Mental Illness Project. This project was provided by mental health services with funding and support from Government tobacco control and Cancer Council South Australia. The project, based within community mental health services, built upon mainstream tobacco cessation materials, and applied them specifically to meet the needs of people with mental illness, and in particular those with ongoing disability.
The aim of this study was to develop a programme for people living with mental illness and associated disability, and to evaluate the intervention provided between November 2002 and October 2005.
Methods
Recruitment
A ten–week group smoking cessation or reduction programme was offered and 226 people with mental illness registered to be involved. The programme was promoted primarily through mental health services, and the Quitline, a state-based telephone counselling service. Information about the programme was also provided to patients by private psychiatrists, general practitioners and community health services.
The programme was open to those who wanted to quit or reduce their tobacco use, and those who expressed interest were interviewed. The interview involved collecting demographic information and baseline data and providing information about the course. Information was then sent to the person's doctor, with their written consent, and a referral was sought to confirm the person's psychiatric diagnosis, medication and the doctor's permission to provide nicotine replacement therapy (NRT) if their patient wanted to use it. This information informed the doctor of their patient's involvement in the course and asked them to provide encouragement, support and to monitor their patient's mental health and medication.
Intervention
The programme was offered across the Adelaide metropolitan area at 10 community mental health sites which were familiar to participants and offered a range of other psychosocial rehabilitation programmes. Participants were required to arrange their own attendance although support was provided where necessary and this included transport, a carer or community worker to attend the course with them or a telephone reminder. Participants who missed a session were contacted to encourage them to attend and if necessary, provide additional support.
A mental health worker and a peer worker provided the programme [19]. The peer worker was someone with a mental illness and personal experience of quitting tobacco. The course ran over 10 weeks, with most involving two sessions per week for the first 5 or 6 weeks and then one session per week. Each session of the course ran for 2 h with a break in the middle.
The course was structured with session plans and the content was similar to most standard cessation interventions, however, it was tailored to the needs of this group by providing additional information about issues of concern including managing mental health, dealing with boredom and stress, building confidence and coping strategies. Course materials, including a step-by-step guide were developed specifically to accommodate the range of abilities within the group including those with difficulties with concentration, literacy and cognitive function.
Healthy refreshments were provided as an added incentive and as an alternative activity to smoking during the break time. Participants who were still smokers were asked to move away from others if smoking during the break time.
A Micro 4 Smokerlyzer (Bedfont) was used to measure breath carbon monoxide levels during the course. It was also used as a visual indicator of smoking reduction or cessation and as a motivator for participants.
At the end of the course, individual telephone counselling was provided to those who requested ongoing support. Participants were encouraged to view quitting as a journey that may involve a number of quit or reduction attempts and some chose to enrol in subsequent courses.
The course was provided to participants at a nominal cost of $40 (Aus) and some paid by instalments. If a participant was unable to pay, the fee was waived. Up to 8 weeks supply of nicotine replacement therapy (NRT) was provided at no additional cost to those who wanted to use it and had written permission from their doctor. Four NRT products were available; transdermal patches, gum, lozenges and inhalers. Participants received one week's supply at a time and this was conditional on regular course attendance. Ongoing NRT was not provided where the participant continued to smoke heavily, no longer wanted to quit or chose to stop using NRT. Combination NRT was not offered within the programme.
Data collection
Ethics approval was granted by the Human Research Ethics Committees of the South Australian Department of Health, the Queen Elizabeth Hospital, Lyell McEwin Hospital, Royal Adelaide Hospital, Flinders Medical Centre, and the Aboriginal Health Council of South Australia. All participants gave written informed consent.
Prior to commencing the course, participants were interviewed to collect demographic and background information about lifestyle and tobacco smoking behaviour. The Fagerström Test for Nicotine Dependence [20] was used to assess nicotine dependency and scores were ranked according to the New South Wales Health Department guidelines for the management of nicotine dependent inpatients [21].
During the course, at week 5 and week 10, participants were asked to complete a written questionnaire about their smoking behaviour, their mental health status and their views of the programme and the group experience. Participants were contacted by telephone at 3, 6 and 12 months after the course to complete a further questionnaire about their smoking status and if smoking, their interest in a quit attempt. In the event that participants attended more than one course, quit rates were generated from the last course attended within the study period.
Participants were asked to use the Micro 4 Smokerlyzer during the course. However, it was not always available and so there were insufficient carbon monoxide readings to validate the reported smoking status. The participant's self report was used and the Smokerlyser data was excluded from analysis.
Analyses
SPSS version 16.02 was used for statistical analyses. Differences between proportions were analysed using chi squares. Differences between means were analysed using 2-tailed t-tests.
Both standard and conservative quit rates were calculated. Standard quit rates use all those who could be contacted as the denominator. Conservative quit rates make the ‘conservative’ assumption that everyone who could not be contacted at follow up had resumed smoking.
Results
Course attendance
A total of 226 smokers with a mental illness registered interest in the programme during the study period and completed an initial interview. Of those, 183 attended at least one session and 105 attended at least 10 sessions of the course.
Forty-three people registered but did not attend at all. When followed up they reported various reasons for not attending including difficulty committing (30.2%), being too unwell at the time the course was offered (27.9%), the location, time or day was no longer suitable due to other commitments (16.3%), they had decided they no longer wanted to address tobacco (9.3%), or they needed more support to get to the group (14%). One person had died. The 43 people who did not attend at all were excluded from the analysis.
Characteristics of course participants
Of the 183 participants who attended at least one session, 51.9% were female and their mean age was 42.4 years (range 19–67 years, SD = 10.2). The majority had secondary schooling as their highest educational qualification (71.6%) and 25.1% had some tertiary education. The majority of participants (80.3%) were diagnosed with a psychotic disorder by their medical officer, i.e. schizophrenia (43.2%), schizo-affective disorder (21.9%), or bipolar disorder (15.3%) (Table 1).
Profile of course participants
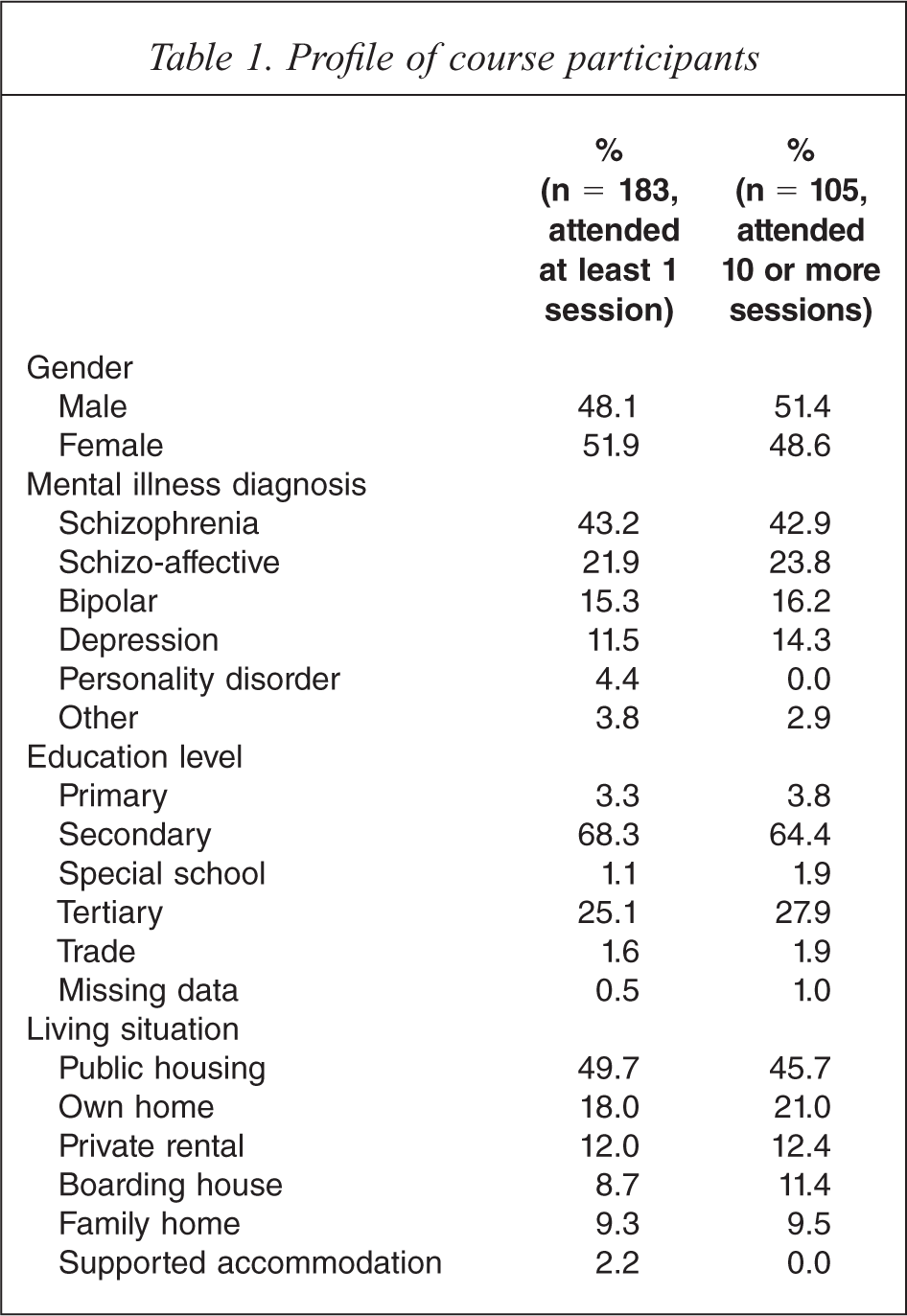
Overall, 49.7% of participants reported they lived in public housing and 55.7% of the participants lived alone. 10.9% of the 183 participants were living in supported housing or boarding houses. Of those who lived with others (n = 81), 53.1% reported they lived with people who smoked. Most participants (93.4%) reported they had stable accommodation.
A series of chi square analyses comparing those who attended 1–9 sessions with those who attended 10 or more sessions showed there were no significant differences between these two groups in gender, diagnosis, education or living situation. Table 1 presents data separately for those who attended at least one session and the subset who attended 10 or more sessions.
Smoking history at baseline
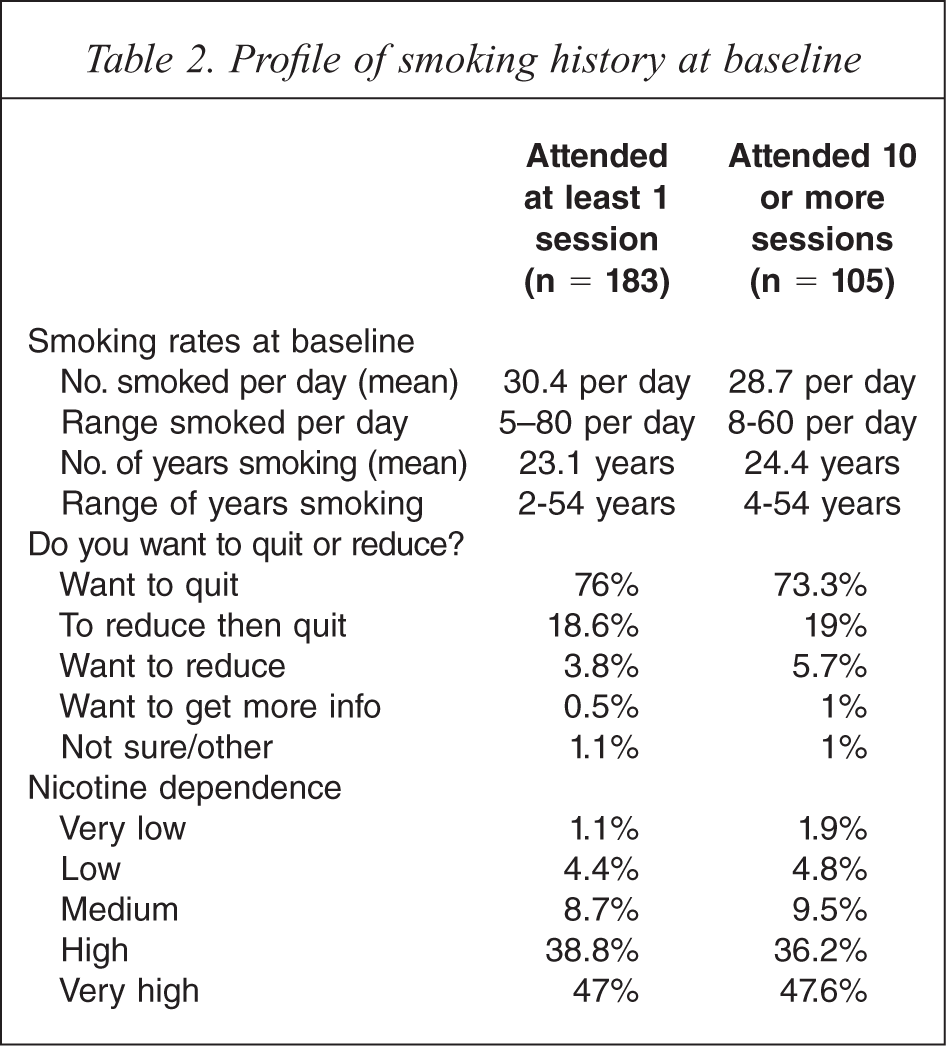
At baseline, 76% of the participants who had attended at least one session reported they wanted to quit smoking, 18.6% wanted to reduce and then quit, and 3.8% wanted only to reduce their consumption. Overall, 86.9% of these participants reported they had tried to quit in the past. At baseline, the majority (85.8%) being highly dependent, 38.8% ranked as high dependence and 47% very high dependence, as assessed by the Fagerström Test for Nicotine Dependence [18,19]. At baseline, the mean number of cigarettes smoked per day was 30.4 with a range of 5 to 80 cigarettes and the mean number of years smoking was 23.1 years (SD = 10.7), range of 2 to 54 years.
A series of chi square analyses comparing those who attended 1–9 sessions and those who attended 10 or more sessions also confirmed no significant differences related to baseline smoking history. Table 2 shows smoking history at baseline and dependence for those who attended 1 or more session and the subset who attended 10 or more sessions.
Profile of smoking history at baseline
NRT use
At the end of the 10 week course, 72.1% of those who had attended at least one session reported they had used NRT. Of these, 60.6% had used the nicotine patch, 6.1% the gum, 13.6% the lozenge, and 19.7% had used the inhaler.
Smoking cessation rates
Of the 183 participants who managed to attend at least once, 79.8% reported not smoking at all for at least 24 h, with 72.1% doing so during the course and 29% doing so after the course completion (multiple quit attempts were made). A substantial proportion of participants (58.5%) reported that they managed to not smoke for at least 7 days and 30.6% did not smoke for at least 30 days during the 12 months. At the 12 month follow up, 16.6% (13.7% as a conservative estimate) reported they were abstinent. Table 3 shows self-reported smoking cessation rates at different evaluation points for those who attended at least one session.
Smoking cessation rates for those who attended at least one session
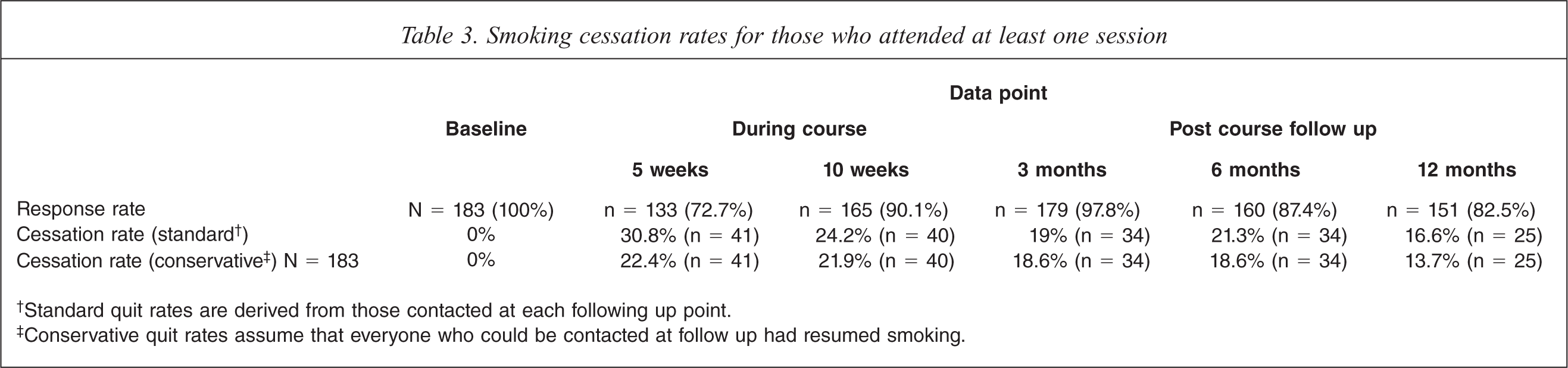
†Standard quit rates are derived from those contacted at each following up point.
‡Conservative quit rates assume that everyone who could be contacted at follow up had resumed smoking.
Of the 105 participants who attended 10 or more sessions, 85.7% reported they did not smoke for at least 24 h, with 81% not smoking during the course and 31.4% not smoking after the course completion (multiple quit attempts were made). Of these participants 62.9% reported they did not have a smoke for at least 7 days and 37.1% did not smoke for at least 30 days during the 12 months. At the 12 month follow up, 21.3% (19% as a conservative estimate) reported they were abstinent. Table 4 shows self-reported smoking cessation rates at different evaluation points for those who attended at least ten sessions.
Smoking cessation rates for those who attended at least ten sessions
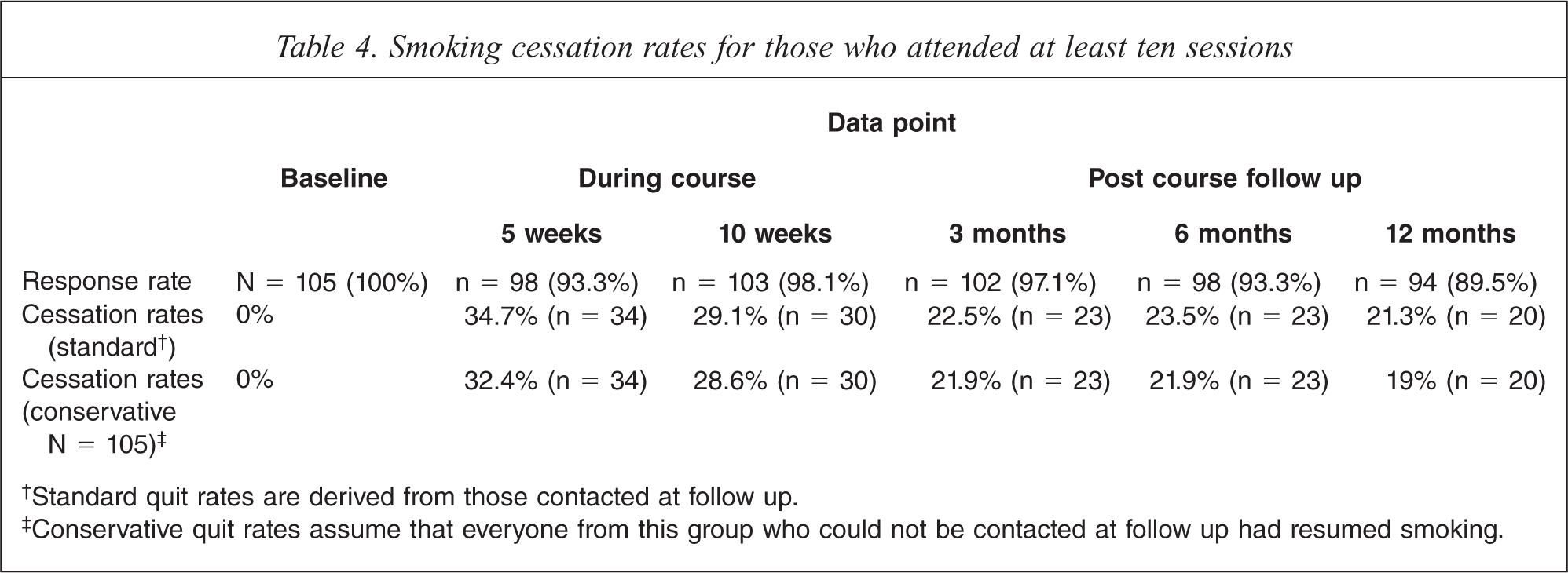
†Standard quit rates are derived from those contacted at follow up.
‡Conservative quit rates assume that everyone from this group who could not be contacted at follow up had resumed smoking.
Smoking consumption amongst those who had not quit at all
Among the participants who had attended at least once and who were smoking at all of the follow up surveys, overall consumption declined significantly from baseline to the first 5 weeks of the course (t = 6.3, df = 57, p = 0.000) and then remained significantly lower at 12 months compared to baseline (t = 3.1, df = 56, p = 0.003) (Table 5).
Smoking consumption amongst those who had not quit at all, n= 58

Motivation to continue to address tobacco use
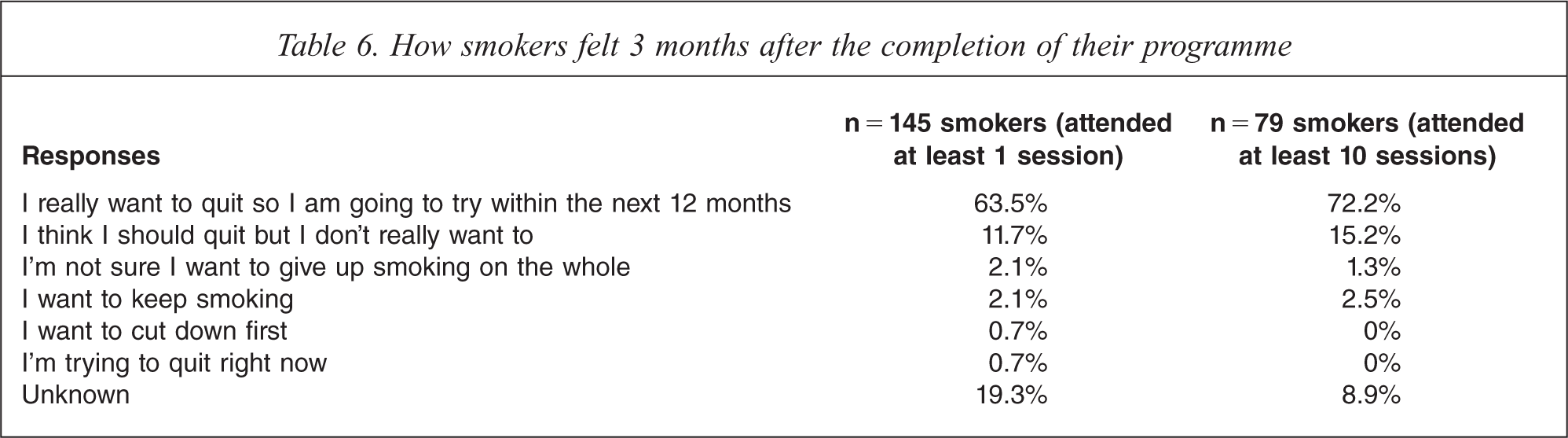
Most participants remained committed to addressing their tobacco use. As shown by Table 6. Of those who could be contacted at 12 months, and reported they were smoking, 83.9% said that they wanted to try to quit again.
How smokers felt 3 months after the completion of their programme
Discussion
The smoking cessation and reduction intervention provided specifically for people living with mental illness was effective in assisting many to quit or reduce their tobacco use. Of the 183 people who attended at least one session of the programme (79.8%) reported not smoking for at least 24 hours, demonstrating they were motivated and able to make a quit attempt and go without cigarettes. Over 30% of participants quit for at least 30 days and at 12 months 16.6% were not smoking (13.7% conservative estimate).
Of the 105 people who attended at least 10 sessions, at 12 months 21.3% were not smoking (19.0% conservative estimate). These 12 months quit rates are comparable with rates achieved in group programmes provided to the general community and challenge the notion that this group is not interested or able to quit tobacco [22].
Participants who remained smoking at all follow up points were able to reduce the number of cigarettes smoked indicating they were developing some control over the amount they were smoking and were continuing to smoke less.
At 12 months after completion of the programme most of the smokers said they still wanted to address their tobacco use. These results indicate these participants remained motivated and are important as most smokers need to make more than one quit attempt [23].
Given that all participants in the programme had a mental illness, and most lived with significant disability, and had been heavy smokers for many years, these results are very encouraging.
Those participants who were able to attend more often achieved a better long-term cessation result. This suggests that offering motivated participants the opportunity to access programmes, and where necessary increased support to assist them to attend more regularly can increase cessation results.
The course content was similar to that provided by interventions offered to the general population. However, there were a number of specific features of this programme which seemed, from the feedback received from participants, to be important. The time spent each week and the length of the programme provided participants with more opportunity to make the decision, prepare and then to make a quit attempt. The time spent on topics which were especially relevant to this group was appreciated and the additional supports appeared to be vital in helping some to attend.
Participants found the group support helpful and most valued working with others who were in a similar position to themselves. The employment of a peer worker as a co-leader seemed to be especially valued as many participants said it enabled them to feel more confident as the peer workers were living proof that having mental illness is not a barrier to quitting tobacco and they were able to offer suggestions from their personal experience.
The programme was offered to those who wanted to quit and also to those who wanted to reduce their tobacco use. Some participants who wanted only to reduce said they lacked confidence to quit completely and the opportunity to attend the group and learn from other participants and peer workers seemed to be useful in building their confidence.
Limitations
One limitation of this study was the verification of smoking status. The study relied on self-reported smoking status and not biochemical validation as carbon monoxide readings were not always available; however, the close working relationship with participants and the carbon monoxide readings that were recorded indicated a high degree of accuracy.
When individuals had attended more than one course throughout the study period, their most recent course outcomes were included in the analysis. This was done to enable comparison with evaluations of other interventions (such as telephone counselling) which do not control in their analysis for the number of prior occasions on which a participant has called.
The project aimed to develop and provide a sustainable smoking cessation and reduction programme within mental health services and did not involve randomizing to a control group and therefore no comparison can be made with a group involved in other forms of support.
Conclusion
The high rate of tobacco use among people with mental illness and the fact that they are also a significant percentage of smokers makes this a serious public health issue. Both mental health services and the tobacco control services which are funded to reduce the rate of tobacco use across the community need to ensure they recognize and address the specific needs of this group of smokers. Mental health services need to ensure assisting people with mental illness to address tobacco is included within clinical care, rehabilitation and recovery programmes. Patients need to be asked by health care providers about their smoking status and encouraged to tackle their tobacco use. Combining motivational and behavioural approaches with opportunities to access subsidised pharmacological treatments is an incentive, in particular for those on a low income. Given that people with mental illness are a significant percentage of the smokers, population-wide approaches need to reach out specifically to this group. Tobacco control and mental health services have a shared responsibility and can work together to ensure effective support is provided. This programme was developed for people with mental illness, in particular those with significant associated disability. It demonstrates that many people with mental illness are motivated to address tobacco and, when provided with specifically tailored support, many can quit tobacco.
Footnotes
Acknowledgements
Acknowledgements are due to Mark Weston, Sheryl Mulconray, Sue Condon for co-facilitating the group programmes, other group co-leaders and to all course participants. Sincere thanks to Deb Shaw, Carol Weston and Cherrie Galletly, University of Adelaide for reviewing this article prior to submission.