
Abstract
The association between smoking and mental illness in adults has been well established. The smoking rate among people with mental illness is around twice that of the remainder of the population, and around one third of adult smokers are estimated to have mental illness, most commonly anxiety or affective disorders [1,2]. Most adult smokers commence smoking and progress to daily smoking during their teenage years [3]. Anxiety disorders, which are the most common mental disorder among adult Australian smokers [2], often have initial onset during childhood or adolescence [4,5]. Previous studies have suggested that the relationship between mental illness and smoking is observable in adolescents. In a school-based sample of adolescents in Victoria, depressive and anxiety symptoms were found to be associated with higher risk of initiation of smoking and progression to regular smoking [6,7]. Community-based samples of adolescents in the USA have found associations between major depression, disruptive behaviours and smoking [8], attention deficit hyperactivity disorder (ADHD) and early initiation of smoking [9], and anxiety disorders and smoking [10]. Depressive disorders have also been found to be correlated with nicotine dependence in 16 year olds in New Zealand [11].
The child and adolescent component of the National Survey of Mental Health and Wellbeing used two main methods to assess mental health problems: a structured interview was used to assess three mental disorders using DSM-IV criteria, and a standardized checklist was used to assess emotional and behavioural problems. We used these data to investigate the relationship between smoking, mental disorders and emotional and behavioural problems. To our knowledge, this is the first time these relationships have been studied in a national probability-representative sample.
Materials and methods
Data source
Data were taken from the 1998–1999 child and adolescent component of the National Survey of Mental Health and Wellbeing. The survey was a nationally representative sample of children aged 4–17 years and their primary carers, living in private dwellings. Stratified, clustered area-based sampling was employed with census collection districts representing the primary sampling unit. Stratification was by state and then into metropolitan/ex-metropolitan regions. The survey was conducted by personal interview using a panel of trained interviewers. Subjects included in this analysis were 1280 young people aged 13–17 years who completed the Youth Risk Behaviour Questionnaire (YRBQ). Full details of the survey methodology have been published elsewhere [12–14].
Analysis was undertaken on the publicly available confidentialized micro data file. As such, no institutional ethics approval was required for this analysis.
Measures
Mental disorders
Three main mental disorders were assessed using the fourth edition of the Diagnostic Interview Schedule for Children (DISC-IV) [15]. These were conduct disorder, depressive disorder, and ADHD. The DISC-IV assesses the presence of disorder in the 12 months prior to the survey date. The DISC-IV was administered to the primary carer (usually the mother) of the survey child. The DISC-IV generates DSM-IV diagnoses [16], and has acceptable test-retest reliability [15].
Emotional and behavioural problems
The Child Behavior Checklist (CBCL) was completed by parents/caregivers, and the Youth Self Report (YSR) was completed by young people aged 13–17 years [17,18]. The CBCL and YSR assess current emotional and behavioural problems with questions in reference to the six months prior to the survey. T scores for internalizing, externalizing and total problem scales were calculated, with higher scores indicating a higher level of emotional and behavioural problems. Total CBCL and YSR T scores were classified as clinical (60 or above), sub-threshold (54–59), or non-clinical (below 54). Internalizing and externalizing problem scores were classified as clinical (60 or above) or non-clinical (below 60).
Smoking
Smoking was assessed as part of the Youth Risk Behavior Survey Questionnaire (YRBQ) [19] which was administered to young people aged 13–17 years. Questions include whether the young person has ever tried cigarettes, age when they first smoked, how many days they smoked in the last 30, average number of cigarettes smoked per day in last 30 days, usual source of cigarettes, whether they were asked for ID when purchasing cigarettes, whether they smoked on school property, and whether they ever tried to quit smoking.
Demographic characteristics
Demographic factors used in the analysis included age and gender of the young person, family structure, household income and age mother left school.
Analysis methods
Logistic regression analysis was used to assess associations with current smoking status. Each of the measures of mental disorders and emotional and behavioural problems was modelled separately adjusting for age, sex, family structure, household income, and age mother left school. As the three mental disorders were not mutually exclusive, a separate model was fitted for each disorder, with odds relative to the absence of the disorder while controlling for the other disorders. To further explore the shape of the relationship between CBCL and YSR T scores and smoking, these were also examined on a continuous scale using the framework of generalized additive models (GAMs) [20]. As logistic regression models the log of the odds ratio, we did not enter the CBCL T scores as linear variables as this would imply an exponential relationship between T score and probability of smoking. The GAM framework fits non-parametric spline curves to describe the relationship between a continuous variable and an outcome. As the CBCL T scores make an adjustment for the sex of the child, and sex could potentially confound a relationship with smoking status, we also repeated the analyses using the raw scores on both the CBCL and the YSR. As the results were the same using each approach, for brevity only results using T scores are reported.
Kaplan-Meier life table methods were used to assess age first smoked [21]. As the data were taken from a cross-sectional survey including young people of a range of ages, life table methods allow for age censoring in the calculation, as some non-smokers at the time of the survey may have subsequently smoked before age 17 years.
For young people who had smoked in the past 30 days, the distributions of average number of days smoked in the last 30 days, and average number of cigarettes per day were examined by CBCL score. The distributions of days smoked and cigarettes smoked per day for young people with CBCL scores in the sub-threshold and clinical ranges were compared with young people with scores in the normal range using the Kolmogorov-Smirnov test. All analyses were conducted using SAS software, version 9.2 [22].
Results
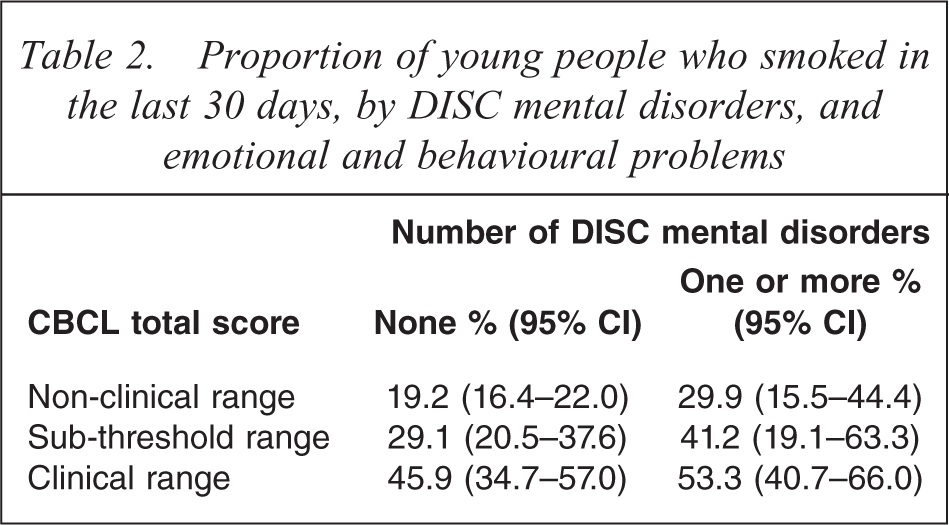
Almost 60% of young people had ever smoked, and 24% smoked in the 30 days before the survey (Table 1). Smoking rates within the last 30 days were higher for young people with specific mental disorders: 72% for young people with conduct disorder, 46% for depressive disorder, and 38% for ADHD. Smoking rates were higher for young people with two or more diagnoses: 58% compared with 38% among young people with one mental disorder. Smoking rates were also elevated among young people scoring in the clinical range on the CBCL: 50% had smoked in the last 30 days among young people scoring in the clinical range on the CBCL externalizing problems scale, and 51% among young people on the YSR externalizing problems scale. Some 41% had smoked in the last 30 days among young people in the clinical range on the CBCL internalizing problems scale, and 42% among young people on the YSR internalizing problems scale. The relationship between CBCL scores, specific mental disorders and smoking is shown in Table 2. Young people not identified with any of the three mental disorders assessed in the survey but with a CBCL score in the clinical range had a higher rate of current smoking than young people scoring in the normal range.
Young people: proportion ever smoked and proportion smoked in last 30 days, by demographic and psychosocial characteristics
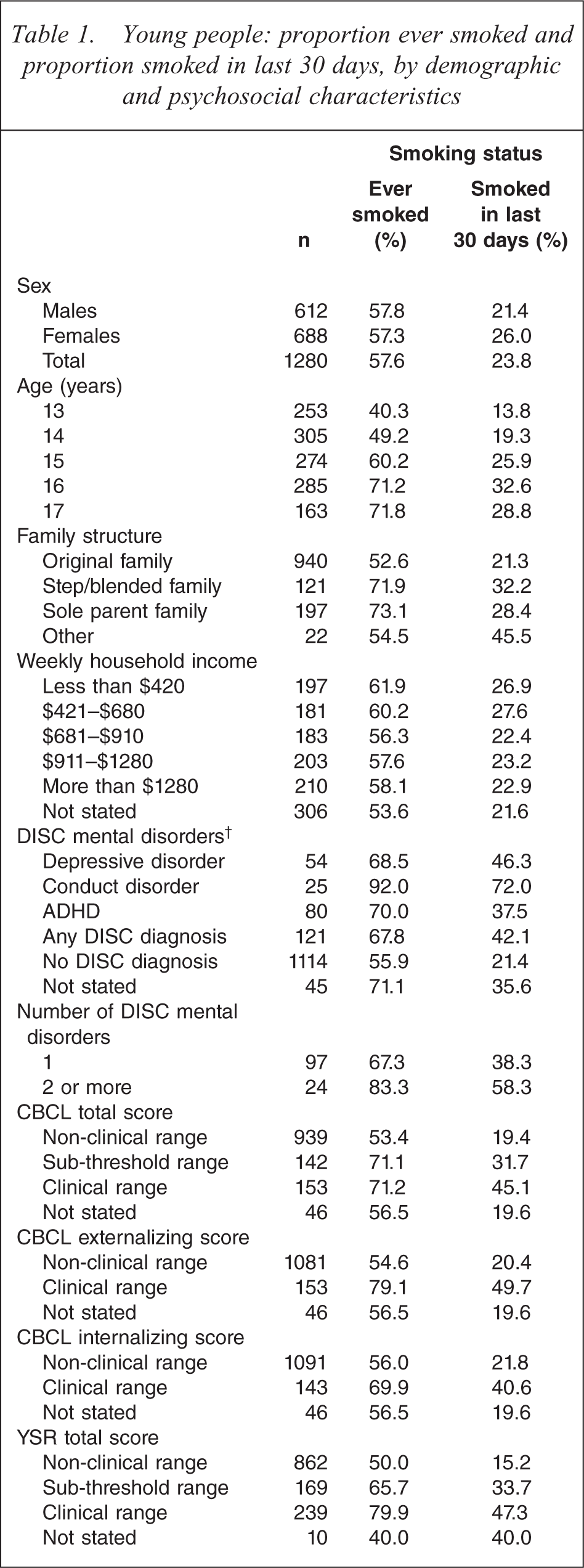
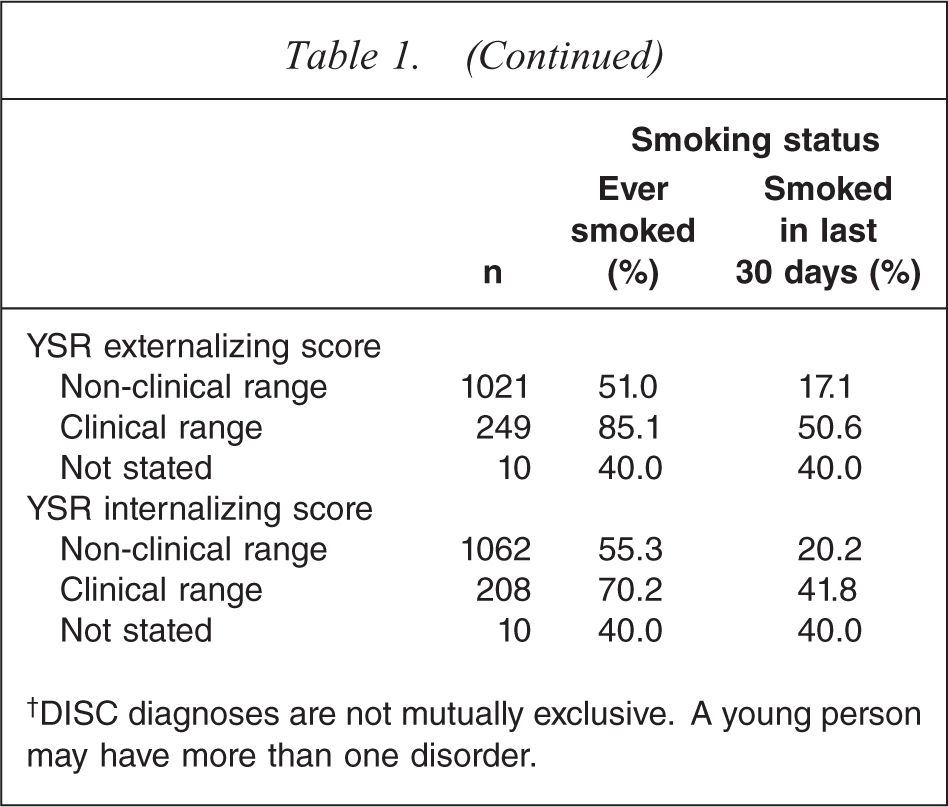
†DISC diagnoses are not mutually exclusive. A young person may have more than one disorder.
Proportion of young people who smoked in the last 30 days, by DISC mental disorders, and emotional and behavioural problems
After adjusting for age, sex, family structure, household income and age mother left school, all measures of mental disorders and emotional and behavioural problems were strongly associated with current smoking status. The full adjusted model for smoking status using CBCL total score is shown in Table 3. Current smoking was higher in females than males, and increased with age. Young people who come from step or blended families or whose mother left school at or before age 15 were also more likely to smoke. After adjusting for other socio-economic variables, the gradient between household income and current smoking was not significant. A CBCL score in the clinical range was more strongly associated with current smoking than any other variable included in the model, after adjusting for all other variables (OR 4.1, 95%CI: 2.7–6.2).
Logistic regression model: factors associated with current smoking
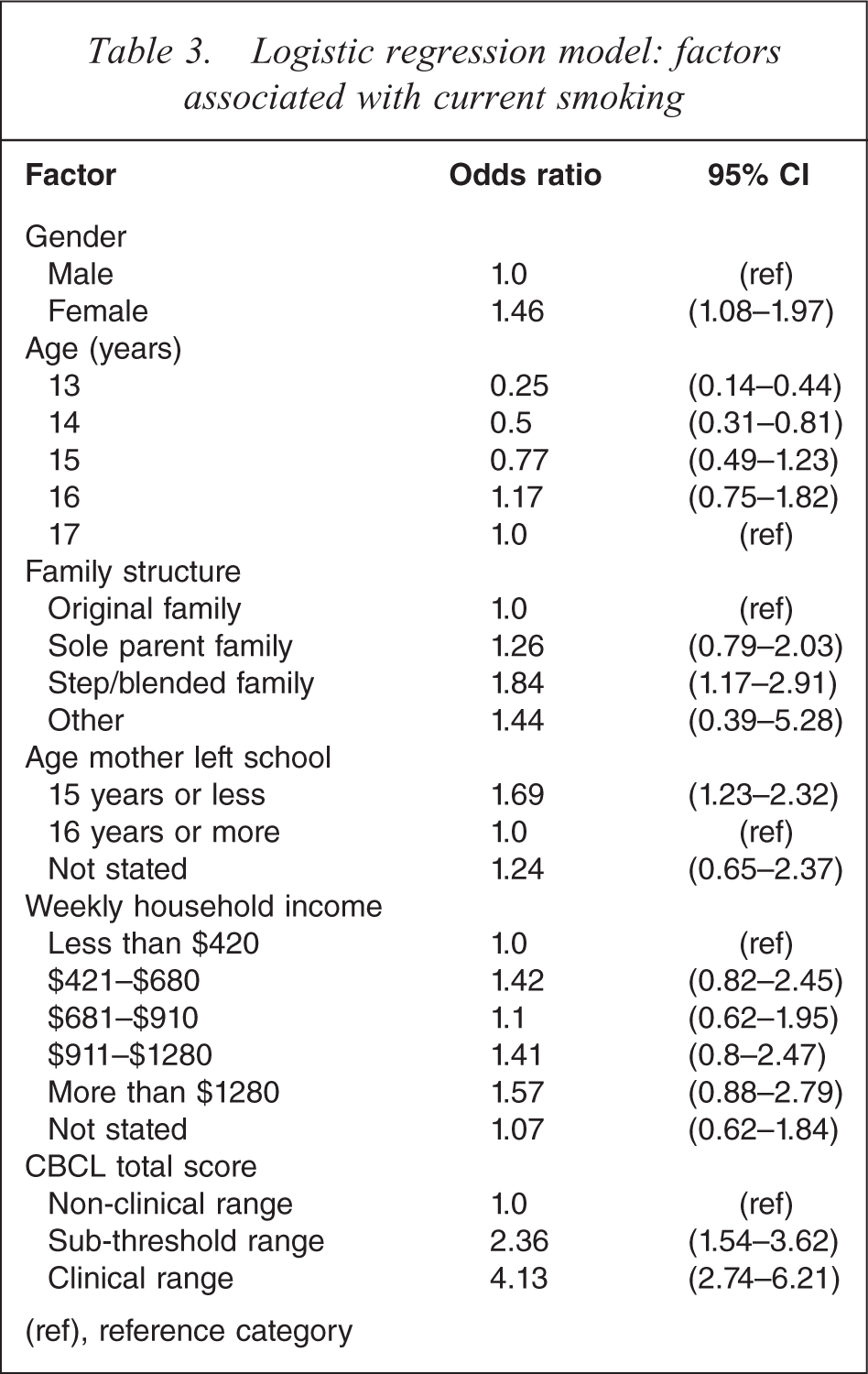
(ref), reference category
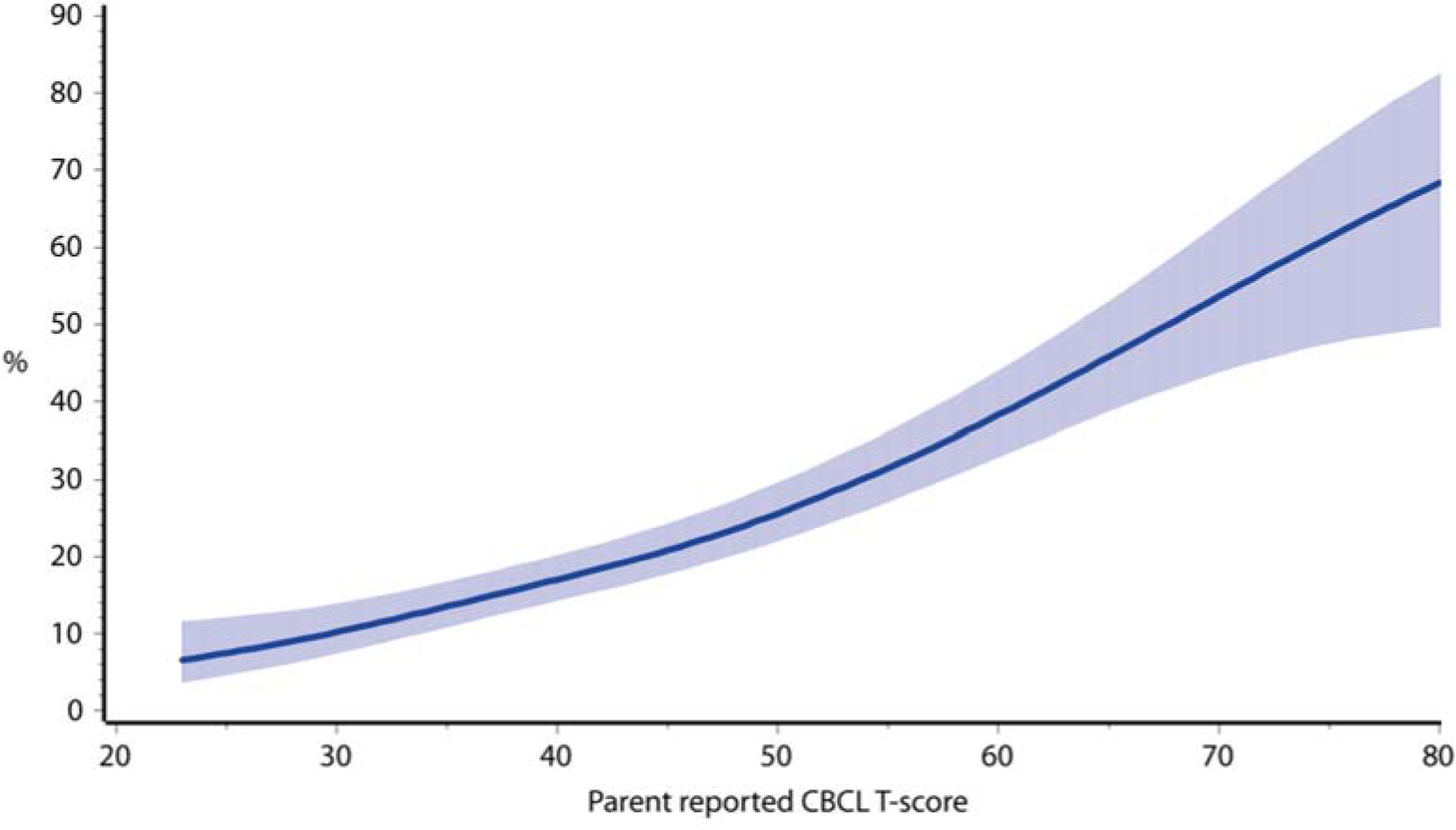
Similar models were fitted for each of the measures of mental disorders and emotional and behavioural problems used in the survey. These are summarized in Table 4. Each model also adjusts for age, sex, family structure, age mother left school and household income. The association between each of these demographic variables and current smoking was very similar in each of these models to that shown in Table 3. Emotional and behavioural problems as measured by the CBCL and YSR were also strongly related to current smoking. Externalizing behaviours were more strongly associated with smoking than internalizing behaviours.
Adjusted logistic regression models: current smoking status†
†All models are adjusted for age, sex, family structure, age mother left school and household income.
‡DISC mental disorders are not mutually exclusive. Each line refers to a separate model, with odds relative to absence of the disorder while controlling for other disorders.
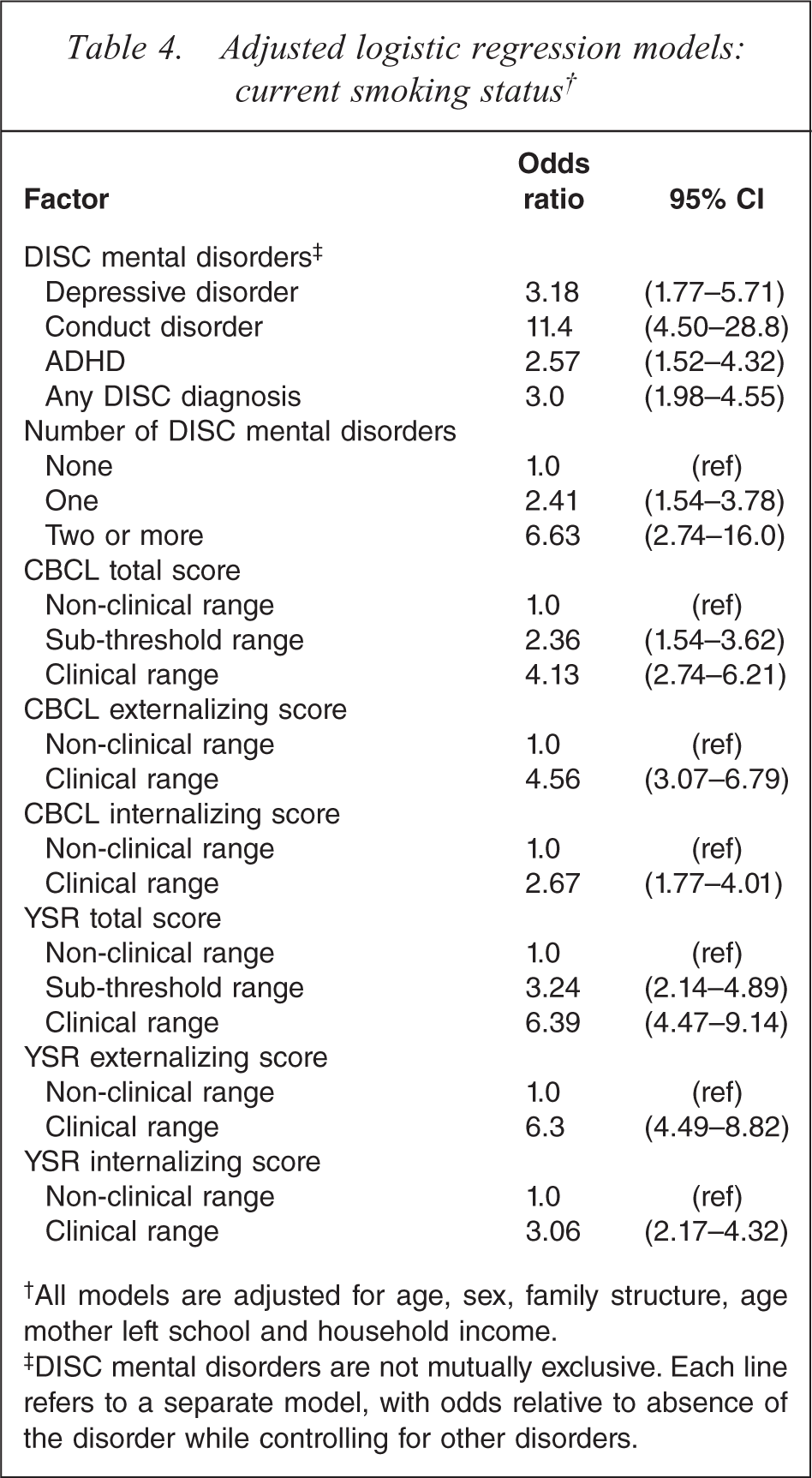
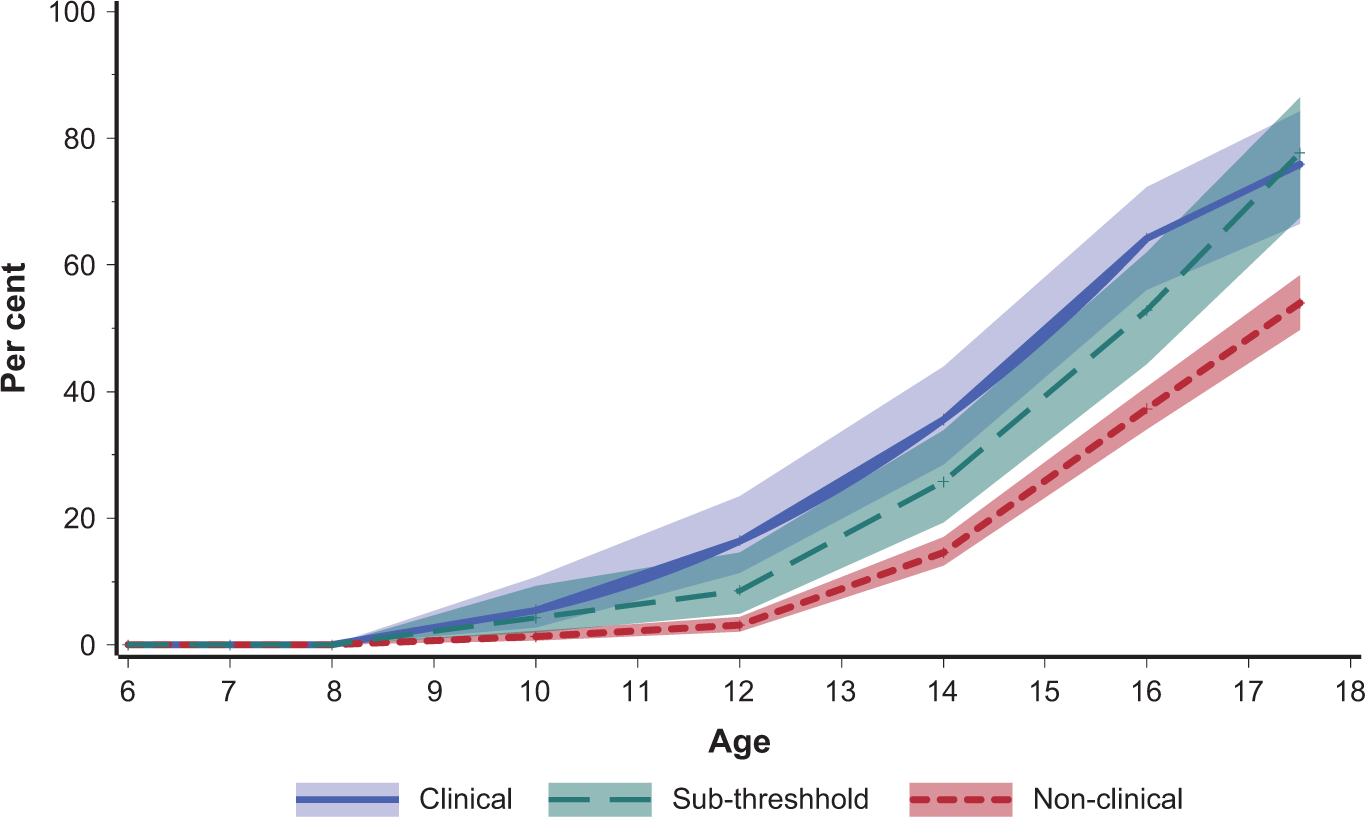
Young people with CBCL scores in the clinical range started smoking at an earlier age on average (Figure 1). The log-rank test for equality of survival curves found a significant difference between age of onset of smoking (χ2 = 14.5, p = 0.0007). Similarly, young people with mental disorders started smoking at an earlier age on average (Figure 2), particularly so for conduct disorder.
Young people: proportion ever smoked by age first smoked and CBCL total score. Shaded bands represent 95% confidence intervals.
Young people: proportion ever smoked by age first smoked and DISC mental disorder. Shaded bands represent 95% confidence intervals; Depression, ADHD and Conduct disorder are not mutually exclusive categories.
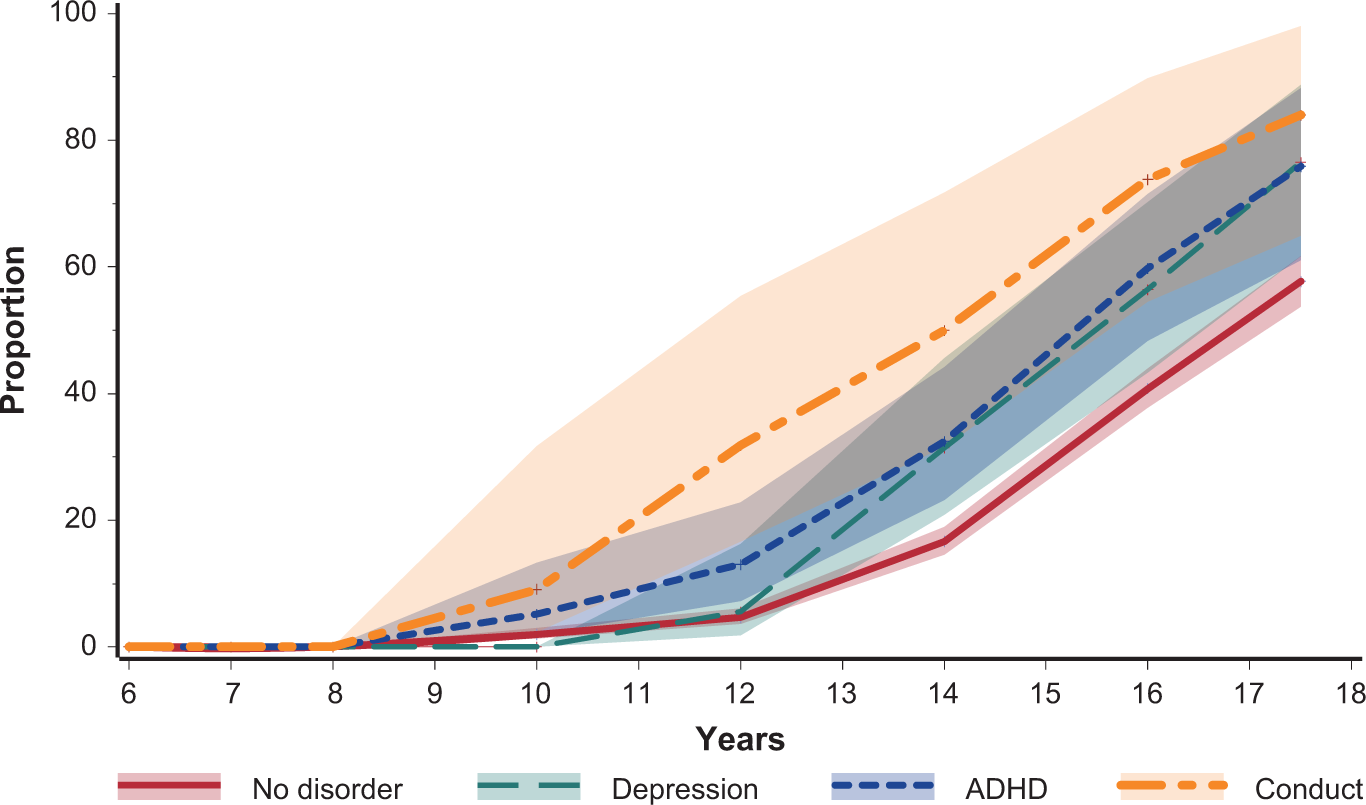
On both CBCL and YSR scores on the continuous scale there was a consistent gradient of increased proportion of smokers with increasing T score. Less than 10% of those with the lowest CBCL T scores smoked, compared with around 70% of those with the highest scores (Figure 3). An almost identical pattern was found for YSR T score (not shown), and an almost identical pattern was found when using the CBCL raw score in place of the T score (not shown). Even within the non-clinical range there was an increasing rate of smoking with increasing T score. At the bottom end of the non-clinical range, less than 10% of young people are current smokers, compared with almost 30% at the upper end of the non-clinical range.
Proportion of young people who are current smokers, by CBCL total T score. Model adjusts for age at time of survey. Shaded band represents 95% confidence interval.
Smokers with CBCL scores in the clinical range consumed on average a larger number of cigarettes per day than those in the non-clinical range and smoked on more days during the past month (Table 5).
Young people who smoked in the last 30 days: proportion by number of days smoked, average number of cigarettes smoked per day, and emotional and behaviouralproblems
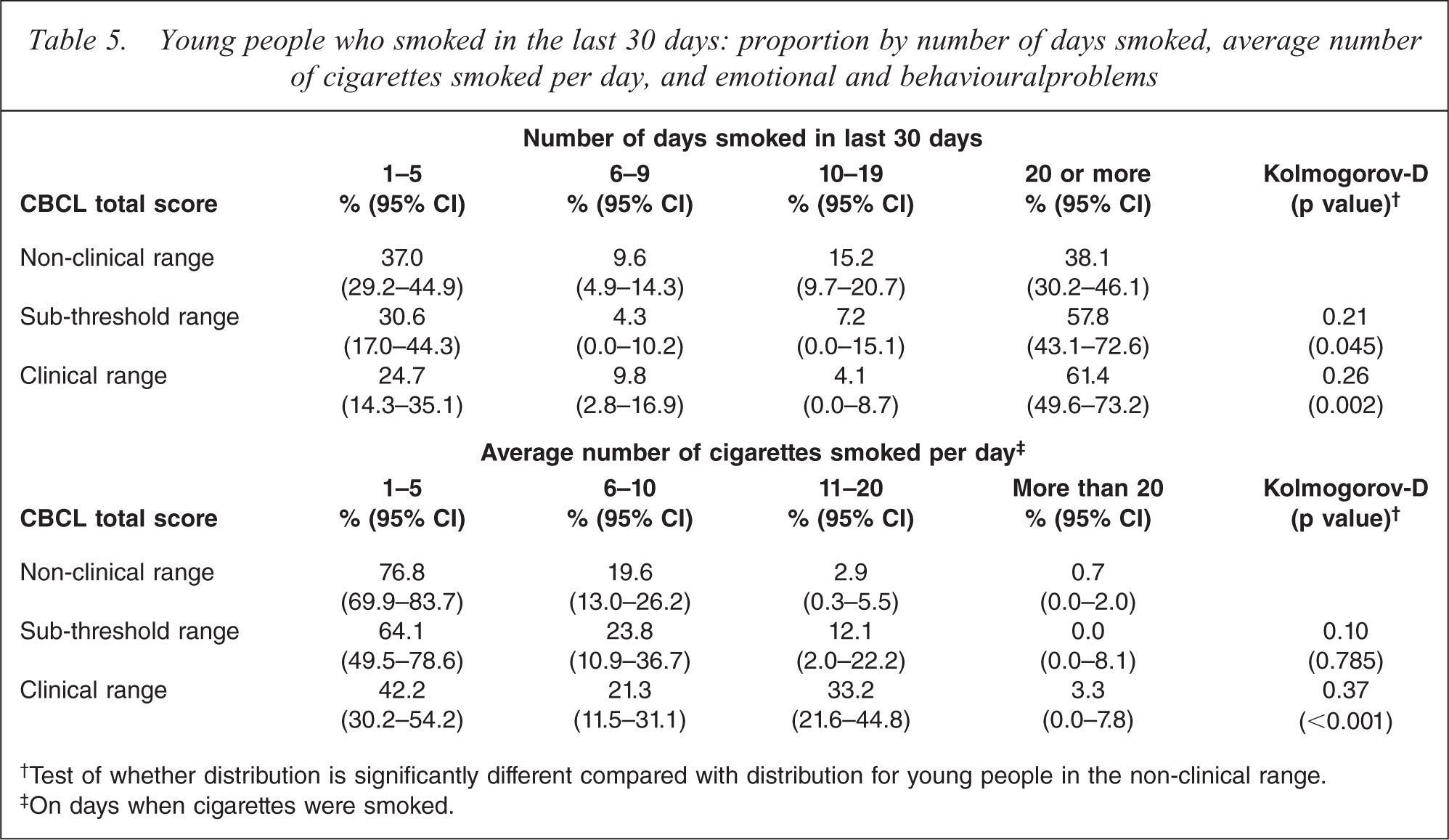
†Test of whether distribution is significantly different compared with distribution for young people in the non-clinical range.
‡On days when cigarettes were smoked.
Discussion
In a large, population-representative sample of young people in Australia, smoking was strongly associated with mental health problems, as measured by both diagnosis of specific mental disorders and using a dimensional measure of emotional and behavioural problems. This is consistent with previous reports [6–11,23]. Young people with conduct disorder or with externalizing problems had the highest rates of smoking. Both parent and youth reports were strongly associated with smoking status, suggesting that assessment of emotional and behavioural problems by either the parent or the youth would be a good indicator of potential smoking risk. We also found that young people with emotional and behavioural problems who smoked started smoking on average at a younger age, were more likely to progress to current smoking, and smoked on average a higher number of cigarettes per day and on more days in the 30 days prior to the survey.
The survey collected information about service use in the six months prior to the survey date. Approximately one third of young people who had one or more specific mental disorders used some type of service in relation to their problems, with school-based counselling services and family doctors the most common reported service providers. Less than one tenth of young people with mental disorders were seen in specialist mental health clinics or by specialist practitioners [13,14]. Nevertheless it is very likely that a high proportion of adolescents attending mental health services are regular smokers. This is a concern as, despite the high rates of smoking amongst their clientele, child and adolescent mental health services rarely provide smoking cessation interventions. The high proportion of smokers among young people with mental disorders would suggest that anti-smoking programmes in mental health services for young people should be developed and evaluated. As young people are more likely to see a school counsellor or family doctor these services may also be important environments for addressing smoking behaviours. Smoking is often not addressed by healthcare providers as it is not viewed as the predominant problem in light of their presenting mental illness. However, the long-term consequences of smoking are significant and smoking should not be ignored during this important developmental period.
There has been considerable speculation in the literature as to whether the relationship between mental illness and smoking is causal, and in which direction it might operate [24,25]. Several theories have been proposed to explain the association. These include the self-medication hypothesis, that people with mental illness choose to smoke to alleviate symptoms or to facilitate coping with their mental illness; that the psychoactive properties of nicotine can precipitate the emergence of symptoms of mental illness in susceptible people; and that both smoking and mental illness may be associated with some unknown, possibly genetic, common prior cause or causes [26,27]. The child and adolescent component of the National Survey of Mental Health and Wellbeing was a cross-sectional survey and the survey does not inform the question of whether the mental illness preceded the initiation of smoking or vice versa. However, the progression from smoking initiation to regular daily smoking typically occurs over a period of one to two years [28]. Similarly, the onset of depressive symptoms or conduct problems is often preceded by a period of sub-threshhold symptomatology [29]. As both smoking and mental health problems are phenomena that can often be viewed as developing over a period of time rather than instantaneously attained risk factors, knowledge of the strong association between mental health problems and smoking behaviour in young people may still prove useful in developing targeted interventions without knowing the exact nature of the causality. It has been suggested that different risk factors are associated with smoking initiation and progression to regular smoking. Smoking initiation may be more associated with opportunity, environment and peer pressure, while progression to daily smoking may be more closely related to emotional and behavioural wellbeing [30,31].
The vast majority of smokers commence smoking in their early to mid teens and progress to daily smoking before age 20 [3]. While the high proportion of adult smokers who have mental illness suggests the need to account for mental illness in smoking cessation strategies [2], there are clear advantages in preventing the uptake of smoking during the teenage years. There is no single conceptual theory of why young people take up smoking. A number of risk factors have been identified including socio-demographic factors and other factors such as family and peer support, and self-esteem [28]. It has been suggested that the association between mental illness and smoking may be partially explained by socio-demographic factors that are associated with both mental illness and smoking, such as low socio-economic status, low parental education, and family break-up [32]. We have included these factors in our models and while these factors are associated with smoking behaviour in young people, the associations are weaker than the association between mental disorders or emotional and behavioural problems and smoking. These associations also remain strongly significant after accounting for socio-demographic variables in our models.
Despite the lack of a single, unified theory on smoking initiation, several potential mechanisms have been postulated [32]. Some young people in making the transition from childhood to independence and wanting to establish their own identities are attracted to risk-taking behaviours as a mechanism for establishing independence from authority figures [33,34]. Young people with lower levels of academic or sporting achievements or who are less popular may be at particular risk of choosing this type of path [35]. Young people with conduct disorders are at particular risk but other mental health problems also affect academic and social attainment. It has been suggested that the fear of long-term health consequences is not a strong motivating factor for some young people [28], although this has been a major part of anti-smoking campaigns for many years.
Strategies to combat smoking have been broadly grouped into individual smoking cessation treatments (including small group-based interventions) and population-based interventions. Broad-based population interventions have been credited with much of the success in reducing smoking rates. These strategies have not generally been targeted at particular population sub-groups, although some population sub-groups have been addressed with targeted programmes, such as pregnant women, prisoners, and Aboriginal people. However, people with mental illness have rarely been the subject of targeted smoking cessation strategies. As the majority of young people with mental disorders are not seen regularly in mental health services, smoking cessation services as part of mental health treatment cannot provide the only response to the high rates of smoking in young people with mental disorders. While some have argued that targeted anti-smoking programmes take resources away from population-wide programmes and that population-wide programmes may represent better value for money [36], people with common mental disorders have lower smoking cessation rates suggesting that population-wide programmes do not work equally in all population groups [37]. A focus only on broad programmes fosters inequality if these programmes do not have the same effectiveness in all sub-groups in the population. Population health-based approaches that can be tailored to people with mental illness should be considered as a means of reaching young people with mental health problems who are not in contact with treatment services.
Among young people, and other segments of the population, strong peer pressure not to smoke has developed, associated with the strategy of stigmatizing smoking. While this stigmatization of smoking has deterred some people from smoking it can have the opposite effect on other vulnerable people [38]. For people who are subjected to social stigma for other reasons, the extra stigma of smoking can form a bond of solidarity among the stigmatized group.
Young people with mental disorders and young people with emotional and behavioural problems started smoking on average at an earlier age. Early age of smoking initiation has been associated with heavier smoking, nicotine dependence, and reduced rates of smoking cessation [39–41]. Because of this it has been suggested that interventions that are able to delay the age of smoking initiation might also contribute to a reduction in smoking-related morbidity by increasing later quit rates [41]. Addressing emotional and behavioural problems in young people would seem to be an important part of such a strategy.
Young people with conduct disorders had extremely high rates of smoking. Conduct disorders are also associated with use of other addictive substances [42]. Addressing smoking in young people with conduct disorders is likely to require a comprehensive strategy including alcohol and other drugs.
Limitations
The data were collected in 1998–1999, and rates of smoking may have declined over that period. However, these data remain the most recent available in Australia. The adult component of the National Survey has recently been repeated, and there was no evidence of any reduction in the contribution of mental illness to adult smoking between 1997 and 2007. As there have been no co-ordinated efforts to reduce smoking initiation or increase smoking cessation in either adults or young people with mental illness, it is quite plausible that the associations between mental illness, emotional and behavioural problems and smoking reported here remain valid.
Because of time limitations in the household, not all DISC modules could be included in the national survey. In particular, anxiety disorders were not assessed. It is known that the prevalence of anxiety disorders is relatively high among young people, but the length of the DISC modules for anxiety disorders precluded them from the survey. As such, the survey does not provide a means for examining the relationship between diagnosis of anxiety disorder and smoking, and some of the young people identified as having no DISC diagnosis in this study may have had an anxiety disorder. This may have led to a slight overstating of the rate of smoking among young people with no DISC diagnosed mental disorder. While the other measures of emotional and behavioural problems used in this study do not generate DSM-based diagnoses, anxiety disorders are reasonably well correlated with high T scores on the CBCL and YSR.
Footnotes
Acknowledgements
The child and adolescent component of the National Survey of Mental Health and Wellbeing was funded by the Commonwealth Department of Health and Ageing. Data were provided by the Australian Social Science Data Archive on behalf of the University of Adelaide who conducted the survey on behalf of the Commonwealth. The organizations that funded and conducted the survey bear no responsibility for the further analysis or interpretation of the data.