
Abstract
Objective:
Few studies have investigated the parental risk of major psychiatric disorders among patients with comorbid autism spectrum disorder and attention deficit hyperactivity disorder. This study examined the differences in such risk among patients with autism spectrum disorder–only, with attention deficit hyperactivity disorder–only and both conditions.
Methods:
Between 2001 and 2011, we enrolled 132,624 patients with autism spectrum disorder or attention deficit hyperactivity disorder and 1:10 matched controls for age, sex and demographics from the National Health Insurance Database of Taiwan. Poisson regression models were used to examine the risk of five major psychiatric disorders in the patients’ parents compared with those of the controls, including schizophrenia, bipolar disorder, major depressive disorder, alcohol use disorder, and substance use disorder. Patients were classified into the autism spectrum disorder–only, attention deficit hyperactivity disorder–only and dual-diagnosis groups.
Results:
The parents of attention deficit hyperactivity disorder–only and dual-diagnosis groups had a higher likelihood to be diagnosed with (odds ratios [95% confidence intervals]) schizophrenia (attention deficit hyperactivity disorder: 1.48 [1.39, 1.57]; dual: 1.79 [1.45, 1.20]), bipolar disorder (attention deficit hyperactivity disorder: 1.91 [1.82, 2.01]; dual: 1.81 [1.51, 2.17]), major depressive disorder (attention deficit hyperactivity disorder: 1.94 [1.89, 2.00]; dual: 1.99 [1.81, 2.20]), alcohol use disorder (attention deficit hyperactivity disorder: 1.39 [1.33, 1.45]; dual: 1.20 [1.01, 1.42]) and substance use disorder (attention deficit hyperactivity disorder: 1.66 [1.59, 1.73]; dual: 1.34 [1.13, 1.58]) than the controls. In contrast, the parents of autism spectrum disorder–only group had a higher likelihood to be diagnosed with schizophrenia (1.77 [1.46, 2.15]) and major depressive disorder (1.45 [1.32, 1.61]) and a lower likelihood to be diagnosed with alcohol use disorder (0.68 [0.55, 0.84]) than the controls.
Conclusion:
The autism spectrum disorder–only group had a different parental incidence of major psychiatric disorders than the attention deficit hyperactivity disorder–only and dual-diagnosis groups. Our findings have implications for clinical practice and future genetic research.
Keywords
Introduction
Attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) are common and highly heritable neurodevelopmental disorders with early childhood onset (Bai et al., 2019; Faraone et al., 2005). Previous studies suggest that heritability is 80% and 76% for ASD and ADHD, respectively (Bai et al., 2019; Faraone et al., 2005). In clinical practice, comorbidity of ADHD with ASD is common and vice versa. A previous study reported that 30–80% of children with ASD fulfilled the criteria for ADHD and 20–50% of children with ADHD fulfilled the criteria for ASD (Leitner, 2014). Several studies on twins have suggested that shared genetic risk factors contribute to the co-occurrence of ASD and ADHD (Polderman et al., 2014; Ronald et al., 2008; Taylor et al., 2015). Genetic research using large rare copy number variant data has indicated that these two disorders share several biological underpinnings, including the nicotinic acetylcholine receptor signaling pathway, cell division and response to drugs (Lionel et al., 2014; Martin et al., 2014).
Recent studies have shown a hereditary association among ADHD, ASD and other major psychiatric disorders (MPDs), such as schizophrenia, bipolar disorder (BD), major depressive disorder (MDD), alcohol use disorder (AUD) and substance use disorder (SUD) (Jokiranta-Olkoniemi et al., 2016; Larsson et al., 2013; Parvaresh et al., 2016; Rasic et al., 2014; Sundquist et al., 2014). A Finnish nationwide cohort study reported increased risks (reported as adjusted relative risk with 95% confidence intervals [CIs]) of ASD (11.8 [9.4, 14.7]), ADHD (3.7 [2.9, 4.7]), schizophrenia (2.0 [1.3, 2.9]) and affective disorder (1.8 [1.5, 2.1]) in the siblings of ASD probands than in the controls (Jokiranta-Olkoniemi et al., 2016). Another Swedish population-based study revealed that parents of probands with ADHD had an approximately two-fold higher risk for bipolar disorder and schizophrenia than the controls (Larsson et al., 2013). Two Taiwanese nationwide cohort studies also reported higher risks of schizophrenia, BD, MDD, ADHD, and ASD in the first-degree relatives of probands with ADHD (Chen et al., 2019b) or ASD (Wang et al., 2020) than in the controls. These MPDs may share genetic factors that underlie a substantial proportion of cross-disorder psychopathology overlap, including executive dysfunction, reward dysregulation, mood disturbance, cognitive impairment and social dysfunction (Gandal et al., 2018). A large-scale European genome-wide association study (GWAS) reported common genetic variants among ADHD, ASD, schizophrenia, BD and MDD (Cross-Disorder Group of the Psychiatric Genomics Consortium et al., 2013), and significant genetic correlations were found between schizophrenia and BD, schizophrenia and MDD, BD and MDD, ADHD and MDD and schizophrenia and ASD (Cross-Disorder Group of the Psychiatric Genomics Consortium et al., 2013).
Despite the high comorbidity between ASD and ADHD, there is a lack of population-based studies examining the risk of MPDs in parents of probands with comorbid ASD and ADHD. Using a nationwide dataset, we examined the differences in the parental risk of MPDs among probands with ASD-only, with ADHD-only and both comorbid disorders. We hypothesized that there were differences in parental risk of MPDs among these three groups, including schizophrenia, BD, MDD, SUD and AUD. Our results might provide implications for future epidemiology and biology studies to investigate the heredity and pathophysiology of these psychiatric disorders.
Methods
Data acquisition
Taiwan’s National Health Insurance, a mandatory universal health insurance program, offers comprehensive medical care coverage, including preventive medicine, inpatient, outpatient, and dental services to all residents in Taiwan (more than 23 million people). At the end of 2010, approximately 99.6% of the nation’s population received medical coverage through this program. The Taiwan National Health Research Institute audited and released the Taiwan National Health Insurance Research Database (NHIRD) for scientific study purposes (Huang et al., 2021; Liang et al., 2020). Comprehensive information on insured individuals, such as demographic data, clinical visit dates, disease diagnoses and prescriptions, was included in the NHIRD. The insurance claims information of the individual is anonymized to maintain privacy. The NHIRD uses the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) for diagnoses. The NHIRD has been extensively used in several epidemiological studies in Taiwan (Chen et al., 2016, 2018a, 2018b; Zhang et al., 2021). The study protocol was reviewed and approved by the institutional review board of Taipei Veterans General Hospital.
Study population
Between 2001 and 2011, we identified children (aged 3–11 years) and adolescents (aged 12–19 years) with a diagnosis of ASD (ICD-9-CM: 299), ADHD (ICD-9-CM: 314) or with a dual diagnosis of ADHD and ASD as the study cohort. For each proband, we randomly selected 1:10 matched controls based on age, sex, birth time, income and residence after eliminating individuals with any major psychiatric disorder (ICD-9-CM: 291, 292, 295, 296, 300.3, 300.4, 303, 304, 305 except 305.1, 311, and 314) at any time in the database as a reference group. Family kinships in the NHIRD were identified for genealogy reconstruction using the methods described in previous studies (Chen et al., 2019a; Kuo et al., 2015). Only blood relatives were qualified to be dependents of the insured individuals covered by Taiwan’s National Health Insurance.
Disease classification
The current study focused on five MPDs, including schizophrenia (ICD-9-CM: 295), BD (ICD-9-CM: 296, except 296.2, 296.3, 296.9, and 296.82), MDD (ICD-9-CM: 296.2 and 296.3), AUD (ICD-9-CM: 291, 303, and 305.00-305.03) and SUD (ICD-9-CM:292, 303, 305, except 305.00-305.03 and 305.1). Diagnoses of the five MPDs were assessed in the parents of probands with ASD-only, ADHD-only, or a dual diagnosis and the parents of matched controls. The diagnoses of the five MPDs were required to be given at least twice by board-certified psychiatrists between 1 January 2001 and 31 December 2011 to ensure diagnostic validity.
Assessment of covariates
Demographic data, including age, sex, place of residence and income status, were collected. The monthly income level was divided into three levels (level 1: ⩽19,100 New Taiwanese dollars [NTD], level 2: 19,001–42,000 NTD and level 3: >42,000 NTD), which was the government-designated cut-off for the minimum income of full-time employment in Taiwan during the research period. The urbanization level of residence (levels 1–5, most to least urbanized) was assessed as a proxy for healthcare availability in Taiwan (Liu et al., 2006). All the ICD-9-CM codes used in this study were provided in the supplement.
Statistical methods
Chi-square statistics and F-tests were used to compare categorical and continuous variables, respectively, among the four groups (ASD-only, ADHD-only, dual-diagnosis and control groups). Some offspring were from the same family, resulting in a clustered study sample (Zou, 2004). After adjusting for demographic data (age, sex, residence and income), we used Poisson regression models with a robust error variance to estimate the odds ratios (ORs) and 95% CIs to examine the likelihood of parental MPDs. Sub-analyses stratified by sex of probands, age at diagnosis of ASD or ADHD (<12 years or ⩾12 years) and paternal and maternal risk of MPDs were performed. SAS 9.2 (SAS Institute, Cary, NC, USA) was used for all statistical analyses. All tests were two-tailed and statistical significance was set at p < 0.05.
Data availability
As the participants did not provide consent for their data to be publicly shared, even anonymized data will be made available only to potential collaborators with ethical approval after submitting a research proposal to the Bureau of the National Health Insurance (https://nhird.nhri.org.tw/).
Results
We included 8532 probands with ASD-only, 116,063 probands with ADHD-only, 8029 probands with a dual diagnosis and 1,326,240 matched controls (Table 1). The four groups had different incidences of schizophrenia, BD, MDD, AUD and SUD (all p < 0.001). The dual-diagnosis and ADHD-only groups had the highest incidence of MDD, followed by SUD and AUD in their parents. In contrast, the ASD-only group had the highest incidence of MDD, followed by SUD and schizophrenia.
Demographic characteristics and prevalence of parental mental disorders between probands and controls.
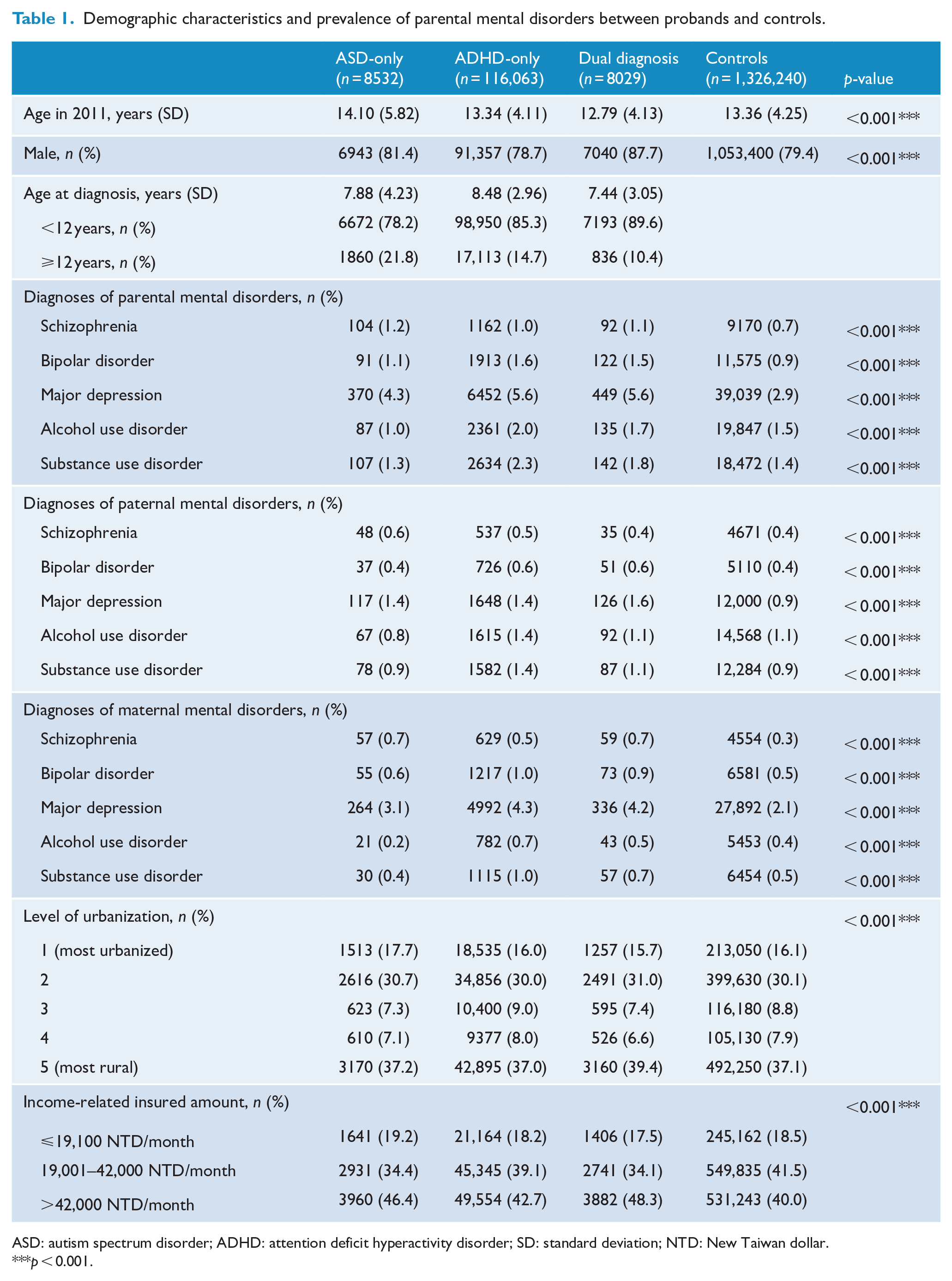
ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder; SD: standard deviation; NTD: New Taiwan dollar.
p < 0.001.
Table 2 shows the risks (shown as ORs with 95% CIs) of MPDs in parents of probands in the ASD-only, ADHD-only or dual-diagnosis groups compared with the control group, with adjustment for demographic characteristics. The parents of the ASD-only group members had a higher likelihood to be diagnosed with schizophrenia (1.77 [1.46, 2.15]) and MDD (1.45 [1.32, 1.61]) and a lower likelihood to be diagnosed with AUD (0.68 [0.55, 0.84]) than the controls. The parents of the ADHD-only and dual-diagnosis group members had a higher likelihood to be diagnosed with schizophrenia (ADHD: 1.48 [1.39, 1.57]; dual: 1.79 [1.45, 1.20]), BD (ADHD: 1.91 [1.82, 2.01]; dual: 1.81 [1.51, 2.17]), MDD (ADHD: 1.94 [1.89, 2.00]; dual: 1.99 [1.81, 2.20]), AUD (ADHD: 1.39 [1.33, 1.45]; dual: 1.20 [1.01, 1.42]) and SUD (ADHD: 1.66 [1.59, 1.73]; dual: 1.34 [1.13, 1.58]) than the controls.
Risks of parental mental disorders among probands with ASD-only, ADHD-only or dual-diagnosis groups a .
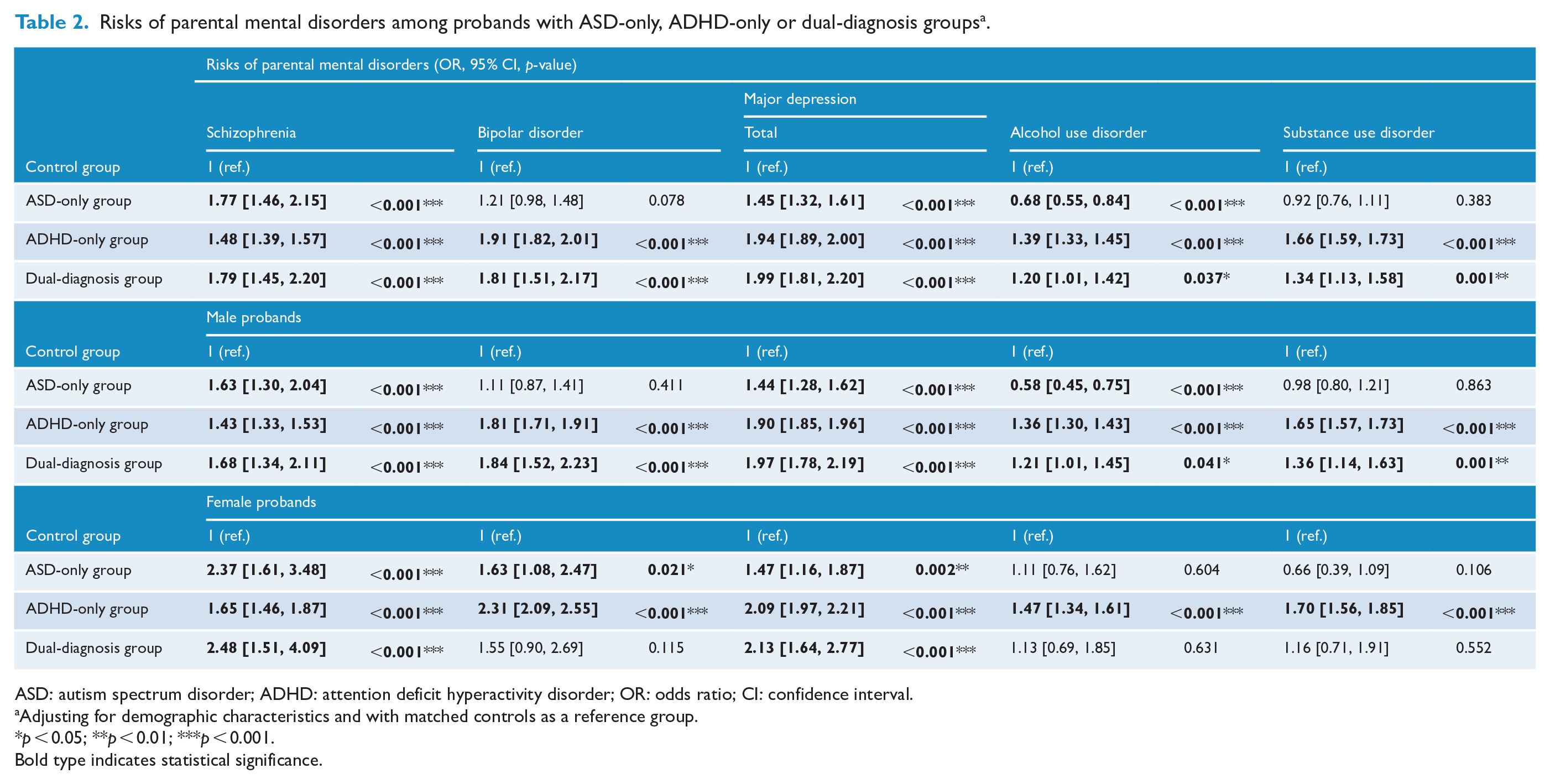
ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder; OR: odds ratio; CI: confidence interval.
Adjusting for demographic characteristics and with matched controls as a reference group.
p < 0.05; **p < 0.01; ***p < 0.001.
Bold type indicates statistical significance.
Figure 1 illustrates the risk of parental MPDs between male and female probands. The highest likelihood to be diagnosed with schizophrenia was observed in the parents of female probands with a dual diagnosis, while the highest likelihood to be diagnosed with BD was observed in the parents of female probands with ADHD-only. The parents of female probands with a dual diagnosis had highest likelihood to be diagnosed with MDD, while the parents of female probands with ADHD-only had the highest likelihood to be diagnosed with both AUD and SUD. The parents of male probands with ASD-only had the lowest likelihood to be diagnosed with AUD.
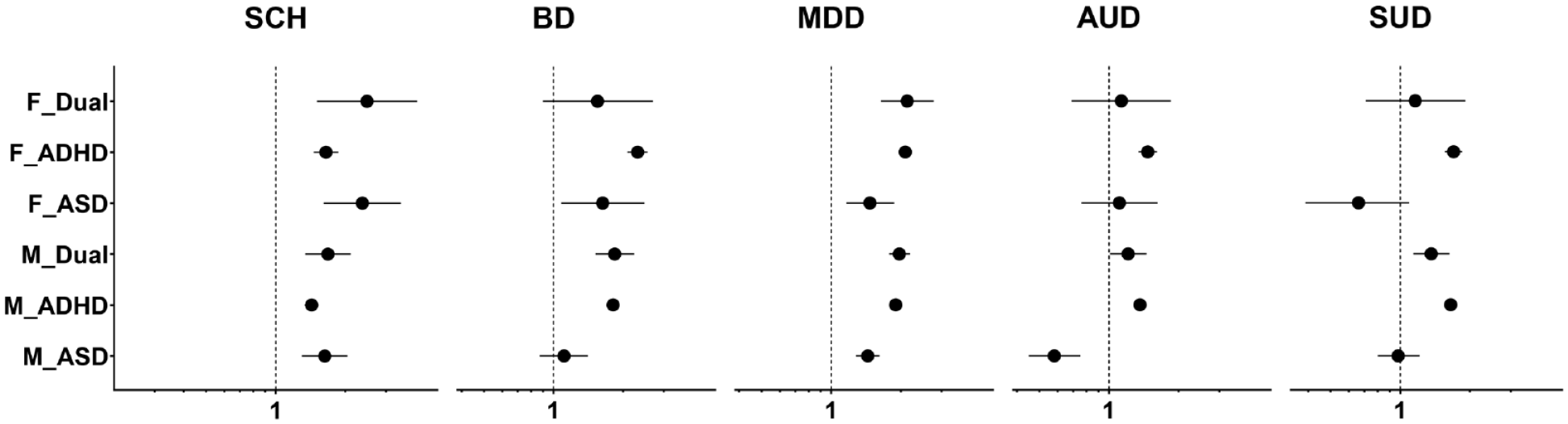
Risk of parental major psychiatric disorders between male and female probands.
In the sub-analysis of sex, the parents of male probands with ASD-only had similar patterns of incidence for the five MPDs as the parents of all probands with ASD-only (Table 2). Likewise, the parents of male probands with ADHD-only and the parents of male probands with a dual diagnosis had similar patterns of incidence for the five MPDs as their corresponding parent groups. However, the parents of female probands with ASD-only had a higher likelihood to be diagnosed with schizophrenia (2.37 [1.61, 3.48]), BD (1.63 [1.08, 2.47]) and MDD (1.47 [1.16, 1.87]) than the controls, whereas the parents of female probands with a dual diagnosis had a higher likelihood to be diagnosed with schizophrenia (2.48 [1.51, 4.09]) and MDD (2.13 [1.46, 2.77]) than the controls. Similar to the parents of male probands with ADHD-only, the parents of female probands with ADHD-only had a higher likelihood to be diagnosed with these five MPDs than the controls (OR range = 1.47–2.31) (Table 2).
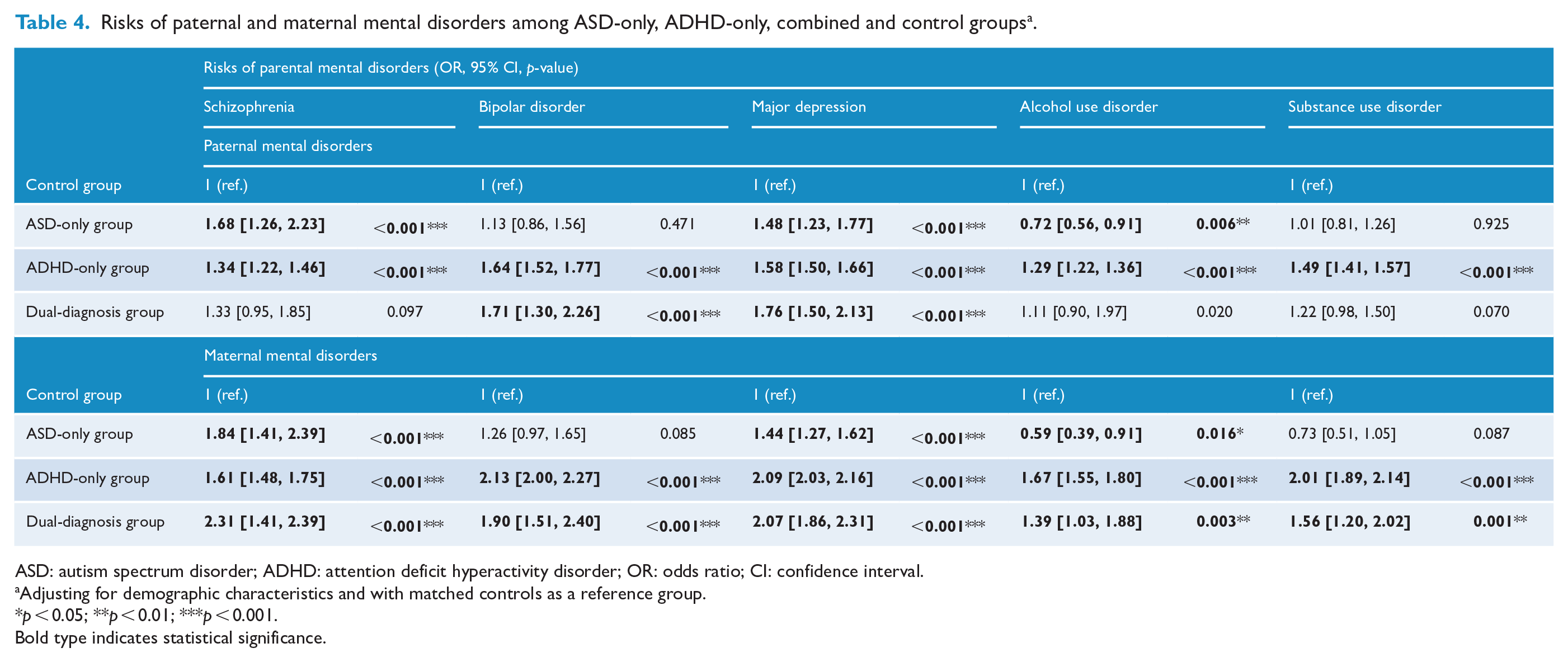
In the sub-analysis of age at diagnosis <12 years (Table 3), the parents of the ADHD-only and dual-diagnosis group members had a higher likelihood to be diagnosed with these five MPDs than the controls (OR range = 1.24–2.04). The parents of the ASD-only group had a higher likelihood to be diagnosed with schizophrenia (1.75 [1.39, 2.20]), BD (1.27 [1.00, 1.60]) and MDD (1.43 [1.26, 1.61]) and a lower likelihood to be diagnosed with AUD (0.62 [0.48, 0.80]) than the controls. In the sub-analysis of age at diagnosis ⩾12 years, the parents of the ASD-only group members had a higher likelihood to be diagnosed with schizophrenia (1.84 [1.27, 2.67]) and MDD (1.52 [1.24, 1.86]) than the controls, while parents of the ADHD-only group members had a higher likelihood to be diagnosed with all five MPDs than the controls (OR range = 1.25–1.86). The parents of the dual-diagnosis group members had a higher likelihood to be diagnosed with BD (2.06 [1.25, 3.38]) and MDD (1.66 [1.23, 2.25]) than the controls (Table 3). Finally, Table 4 shows the risks of paternal and maternal mental disorders among the three groups. The risks were similar with those of parental mental disorders in Table 2.
Risks of parental mental disorders among ASD-only, ADHD-only, combined and control groups, stratified by age of diagnosis a .
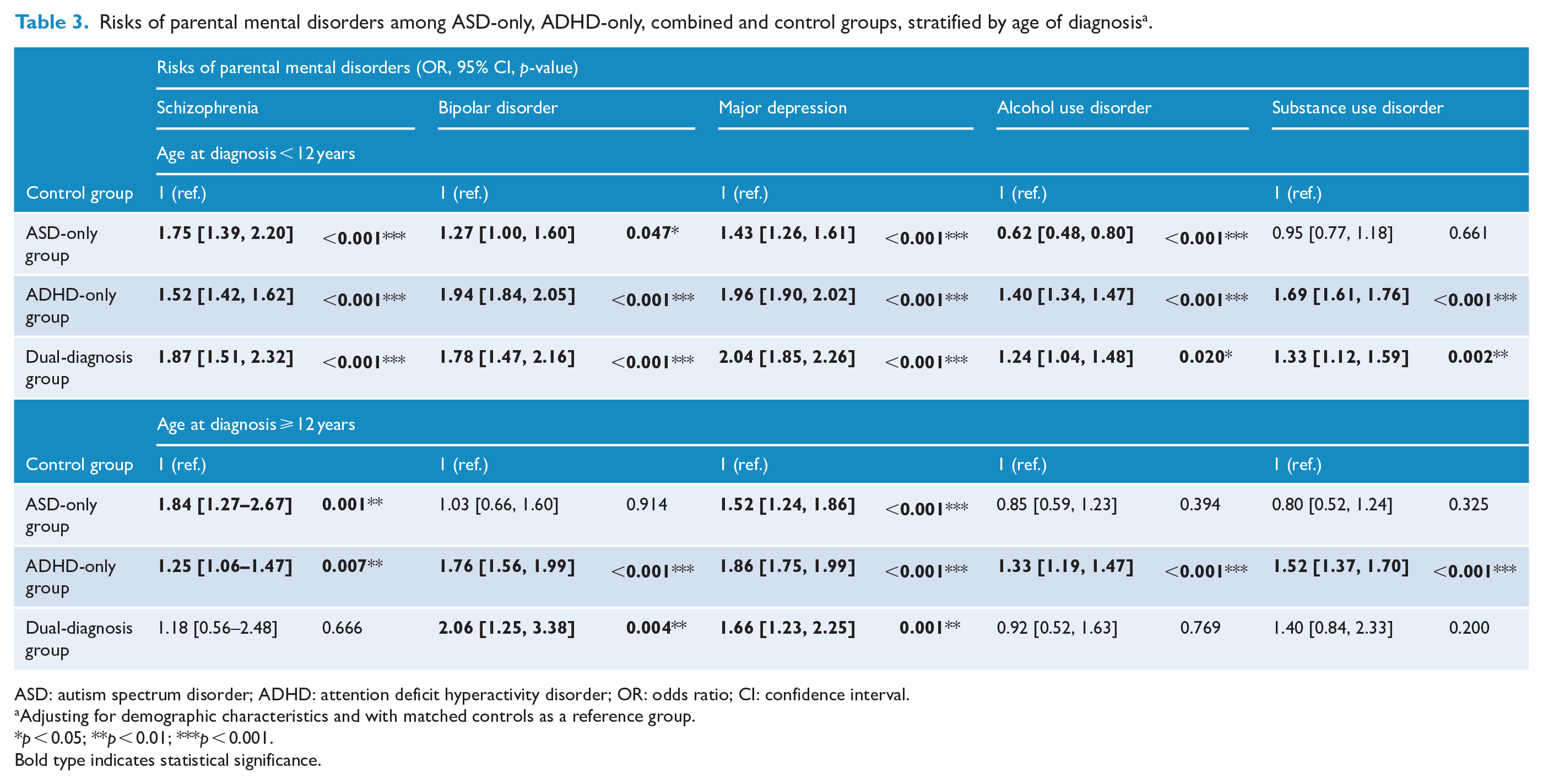
ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder; OR: odds ratio; CI: confidence interval.
Adjusting for demographic characteristics and with matched controls as a reference group.
p < 0.05; **p < 0.01; ***p < 0.001.
Bold type indicates statistical significance.
Risks of paternal and maternal mental disorders among ASD-only, ADHD-only, combined and control groups a .
ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder; OR: odds ratio; CI: confidence interval.
Adjusting for demographic characteristics and with matched controls as a reference group.
p < 0.05; **p < 0.01; ***p < 0.001.
Bold type indicates statistical significance.
Discussion
To the best of our knowledge, this nationwide study is the largest one to assess the parental risk of MPDs in probands with ASD-only, ADHD-only or a dual diagnosis. We found that the parents of probands with ADHD-only or a dual diagnosis had a higher likelihood to be diagnosed with schizophrenia, BD, MDD, SUD and AUD compared with the controls. However, the parents of probands with ASD-only had a higher likelihood to be diagnosed with schizophrenia and MDD and a lower likelihood to be diagnosed with AUD compared with the controls. When assessing the differences between male and female probands, parents of male probands with a dual diagnosis had a higher likelihood to be diagnosed with the five MPDs compared with the controls; however, parents of female probands with a dual diagnosis had a higher likelihood to be diagnosed with schizophrenia and MDD compared with the controls.
We found that the parents of probands with a dual diagnosis had a higher likelihood to be diagnosed with the five MPDs than those of the controls. Genetic factors may play an important role in the heredity association. Our findings were consistent with those of a previous study showing that a latent shared genetic factor accounted for up to 45% of co-variance across childhood externalizing (e.g. AUD and SUD) and internalizing (e.g. BD and MDD) symptoms and 31% of co-variance in childhood neurodevelopmental symptoms (e.g. ASD) (Faraone and Larsson, 2019). Another large-scale GWAS (18,381 ASD cases and 27,969 controls) reported that ASD, schizophrenia and MDD have significantly overlapping genetic architectures (Grove et al., 2019). On the other hand, psychological and environmental stresses may also contribute to the risk of parental MDD. A previous study reported that patients with comorbid ASD and ADHD would have greater impairment in cognitive, interpersonal, school, family and psychosocial domains than individuals with a single diagnosis (Leitner, 2014). Another birth cohort study assessed the risk of depression onset in parents of probands with ASD or ADHD and the authors reported that the risk of depression in the parents was higher than that in the controls at any offspring stage, including pre-pregnancy, perinatal period, infancy and childhood (Chen et al., 2020). The findings of the aforementioned studies are consistent with ours. Moreover, our study showed that either of the three groups (i.e. ASD-only, ADHD-only or a dual diagnosis) had a higher likelihood to be diagnosed with MDD. Notably, the highest likelihood of parental MDD was found in the dual-diagnosis group than the other two groups, which might be associated with the greater impairment and care burden in this group.
A previous study reported higher incidences of autism and ADHD among individuals with a parental biological history of AUD (Sundquist et al., 2014). Alcohol exposure might alter the methylation status, which could lead to epigenetic modifications of specific genes in sperm cells and further influence the neurodevelopment (Govorko et al., 2012). However, in this study, the increased risks of parental AUD were only found in ADHD-only group and dual-diagnosis group, but not in ASD-only group. The decreased risk of AUD in the parents of probands in the ASD-only group was opposed to the results of previous cohort studies (Miles et al., 2003; Sundquist et al., 2014). However, there were also negative results showing that maternal alcohol consumption posed no risk for autism (Eliasen et al., 2010; Gallagher et al., 2018). Although some overlap of candidate genes has been identified through genome-wide screenings of ASD and AUD (Reich et al., 1998; Risch et al., 1999), the hereditary association between ASD and AUD remains uncertain. Further studies are warranted to address this issue. Taken together, our study suggests that probands with ADHD-only had a similar pattern of parental risks of the five MPDs as probands with a dual diagnosis.
Our study showed that schizophrenia and ASD appeared to cluster together more than schizophrenia and ADHD, and that BD and ADHD appeared to cluster together more than BD and ASD. In previous meta-analytic studies, 11.8% (95% CI = [7.7, 17.6]) of the 22,176 participants with ASD had schizophrenia spectrum disorders (Zheng et al., 2018), while the prevalence rate of BD was 5.0% (95% CI = [3.0, 6.0]) among 153,192 participants with ASD (Lai et al., 2019). Regarding ADHD, the meta-analytic studies reported that the prevalence rate of BD was 8.0% (95% CI = [5.3, 11.1]) in people with ADHD (Schiweck et al., 2021), while the prevalence of schizophrenia spectrum disorders after ADHD ranged from 0.4% to 6.4% (Nourredine et al., 2021). A large-scale GWAS reported that schizophrenia had stronger genetic correlation with ASD than ADHD, and BD had stronger genetic correlation with ADHD than ASD (Solberg et al., 2019). As a consequence, the etiologies of ASD and schizophrenia might overlap more than ASD and BD, and the etiologies of ADHD and BD might overlap more than ADHD and schizophrenia.
Considering the differences between male and female probands, we found that parents of female probands with ASD-only were associated with the highest likelihood to be diagnosed with schizophrenia. Furthermore, parents of female probands with ADHD-only were associated with the highest likelihood to be diagnosed with BD. An epidemiologic study has reported that the prevalence rate of schizophrenia was higher in women with ASD than in men with ASD (Solberg et al., 2019). Biological studies reported that genetic mutations of schizophrenia (such as 15q33 and 8p12) were associated with female patients with ASD (Chen et al., 2017; Fernandez et al., 2019). On the contrary, a nationwide cohort study reported that female patients with ADHD were associated with a higher risk of progression to BD than male patients with ADHD (Chu et al., 2021). Taken together, sex differences in probands with ASD-only, ADHD-only or a dual diagnosis might contribute to different pattern of family coaggregation of schizophrenia and BD.
This study has several limitations. First, the sample sizes of some of the subgroups were small. For example, only 12.3% and 10.4% of probands in the dual-diagnosis group were classified into subgroups of females and diagnoses ⩾ 12 years of age. This underpower may have been limited to our study findings. Second, the mean age at the first diagnosis of ASD/ADHD was relatively old. If a patient had been diagnosed with ADHD before the study period (1 January 2001), the age at diagnosis recorded in our study would have been the first visit to a medical institution after 1 January 2001. Third, we followed this cohort for only 11 years. Therefore, late-onset MPDs in parents might not have been assessed. Finally, certain confounding factors such as medication exposure, substance/alcohol/cigarette exposure, education level and environmental information were unavailable in the NHIRD. Without this information, we could not have assessed their influence.
Conclusion
To the best of our knowledge, this is the first cohort study to assess the risks of major parental psychiatric disorders in probands with comorbid ADHD and ASD. We found that the parents of probands with a dual diagnosis or ADHD-only had a higher likelihood to be diagnosed with schizophrenia, BD, MDD, AUD, and SUD, while the parents of probands with ASD-only had a higher likelihood to be diagnosed with schizophrenia and MDD. Psychiatrists should consider these findings and offer information, social support and prevention strategies to patients with these five MPDs who want to have children. Parents of children with ASD or ADHD need to have access to programs for preventing psychiatric disorders. Prevention strategies and social support for such parents and children should be implemented early. Future genetic and population-based studies assessing genetic and environmental factors in the clinical manifestations of ASD, ADHD, and MPDs are needed.
Supplemental Material
sj-doc-1-anp-10.1177_00048674221108897 – Supplemental material for Risk of parental major psychiatric disorders in patients with comorbid autism spectrum disorder and attention deficit hyperactivity disorder: A population-based family-link study
Supplemental material, sj-doc-1-anp-10.1177_00048674221108897 for Risk of parental major psychiatric disorders in patients with comorbid autism spectrum disorder and attention deficit hyperactivity disorder: A population-based family-link study by Tien-Wei Hsu, Ya-Mei Bai, Shih-Jen Tsai, Tzeng-Ji Chen, Chih-Sung Liang and Mu-Hong Chen in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors thank Mr. I-Fan Hu, MA (Courtauld Institute of Art, University of London; National Taiwan University) for his friendship and support. Mr. Hu declares no conflicts of interest.
Author Contributions
M.-H.C. and C.-S.L. designed the study and wrote the protocol. T.-W.H. drafted the manuscript. M.-H.C. analyzed the data. C.-S.L and S.-J.T. assisted with the preparation and proof reading of the manuscript. Y.-M.B. and T.-J.C. provided the advices on statistical analysis. All authors agreed the submission and publication of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was supported by grant from Taipei Veterans General Hospital (V106B-020, V107B-010, V107C-181, V108B-012, V110C-025, V110B-002), Yen Tjing Ling Medical Foundation (CI-109-21, CI-109-22, CI-110-30) and Ministry of Science and Technology, Taiwan (107-2314-B-075-063-MY3). The funding source had no role in any process of our study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.