
Abstract
Objectives:
Anti-police (#EndSARS) protests took place in October 2020 across several Nigerian cities, resulting in deaths, injuries and loss of property, but the psychological sequelae of these protests have not been studied.
Method:
In a cross-sectional online survey, we collected data on psychiatric morbidity and potential risk factors from 426 Nigerian social media users, who self-identified as participants or non-participants in a recent anti-police protest.
Results:
We found elevated rates of psychiatric morbidity, with worse outcomes for protesters compared to non-protesters (psychological distress [44.2% vs 29.8%], depression [26.0% vs 14.9%], anxiety [51.0% vs 29.8%], post-traumatic stress disorder [7.4% vs 1.8%], current substance use [11.2% vs 4.5%] and suicidal ideation [7.1% vs 4.4%], respectively). After adjusting for the effects of COVID-19 pandemic and previous mental health diagnosis, the predictors of poor mental health among non-protesters were being unmarried (odds ratio = 7.4, p = 0.01) and low resilience (odds ratio range = 4.1–5.4, p < 0.03) while for the protesters, the predictors were low resilience (odds ratio range = 2.9–4.7, p < 0.01), being from Northern Nigeria (odds ratio = 4.7, p < 0.01) or residing in Northern Nigeria (odds ratio = 2.8, p = 0.03), being under-/unemployed (odds ratio range = 2.1–2.5, p < 0.04), holding the view that the protest was caused by the state of the economy (odds ratio = 2.0, p = 0.01), belief that the protest had a direct negative impact on the protester (odds ratio = 2.3, p = 0.04) and willingness to participate in future protests (odds ratio = 4.13, p = 0.02).
Conclusion:
We conclude that participating in the #EndSARS protest was associated with significant psychiatric morbidity. There is need to recognise and address the mental health sequelae of collective actions, and invest in programmes that build resilience and address socio-political determinants of mental health, especially with a focus on youth.
Introduction
Protests, riots and revolutions, referred to as collective actions, are ways in which humans show opposition to or express the desire to change the cultural, social or political status quo of society (Ortiz et al., 2013). Collective actions have occurred in almost all human societies (Banks and Wilson, 2017), and there are indications that their frequency is increasing globally in recent times (Ortiz et al., 2013). In a recent review, Ortiz et al. (2013) identified 843 protests occurring in 84 countries between 2006 and 2013. Underlying most of the protests were grievances bothering on issues of economic injustice (e.g. poverty, inequality and poor labour conditions), failure of political systems (e.g. government corruption and failure of the justice system), global injustice (e.g. imperialism and environmental injustice) and rights of people (e.g. women and gay rights).
Most protests are directed at governments and political/economic systems. However, occasionally, they also target the military or the police (Ortiz et al., 2013). This was the case with the #EndSARS protest in Nigeria. The #EndSARS protest took place between 8 October and 22 October 2020, with the main grievance being police and the Special Anti-Robbery Squad (SARS) brutality (Tarila Marclint Ebiede, 2020). The SARS was formed in the 1990s by the Nigerian government in response to the increasing spate of armed robberies and kidnappings in the country at the time. However, over time, this special branch of the police was accused by the public of having derailed in its mission and become notorious for extreme brutality, abuse of power and wanton impunity. Between 2016 and 2020, the human rights group, Amnesty International, reportedly documented at least 82 cases of human rights violations, including armed extortion, rape, kidnapping, torture and extrajudicial executions, with most of the victims being adults below the age of 35 years (Amnesty International Nigeria, 2020).
Following years of public outcry and failure by the Nigerian government to reform the police force generally and the SARS in particular, protests broke out simultaneously in several cities in the Southern Nigeria (most of them in the south), and to a lesser extent among peoples of Nigerian origin across Europe and North America. Arguably, one of the best organised protests in Nigeria in recent history, the #EndSARS protests brought together tens of thousands of Nigerians on the streets and on social media and united them in a powerful social movement. The protest began as a peaceful one, but towards its tail end, it was reportedly hijacked by thugs who were not originally part of the protest, leading to intense and widespread violence that resulted in the death of at least 38 Nigerians, over 200 persons injured and large-scale destruction of property, following the use of live ammunition on protesters by law enforcement agents at protest sites (Sokuma, 2021; Tarila Marclint Ebiede, 2020). Despite the fact that #EndSARS started as a protest against police brutality, it rapidly evolved to encompass other grievances such as demand for better governance, with youths in the south opposing and those in the north supporting the current government (Sokuma, 2021). As a result of the protests, the federal government eventually disbanded the SARS and tasked the 36 states of the federation and the Federal Capital Territory with setting up panels of enquiry into public complaints of police brutality and other unprofessional conducts (Tarila Marclint Ebiede, 2020). However, these exact same measures had been instituted in the past by the federal government with little or nothing to show for them. So, whether they yield any tangible results this time around or not remains to be seen.
There is a growing body of literature on the mental health sequelae of collective actions. A recent systematic review of 52 studies found that mental health outcomes following collective actions in the general population and among victims of violence mirror closely those associated with natural disasters and armed conflicts (Ni et al., 2020a). In a recent cohort study of a probability sample of the general adult population of Hong Kong, it was found that the prevalence of probable major depression had increased from pre-protest levels of 1.5% to 8.5% 6 months after the 2014 Occupy Central/Umbrella Movement, and to 11.2% following the 2019 pro-democracy unrest (Ni et al., 2016, 2020b). Similarly, elevated levels of anxiety and post-traumatic stress disorder (PTSD) have been reported among general populations following collective actions and samples drawn from populations in areas affected by collective actions (Ni et al., 2020a). Important risk factors for poor mental health outcomes reported in the literature in the aftermath of collective actions include female gender, lower socio-economic class, lower resilience, as well as exposure to violence and media coverage, and loss of personal resources and unemployment (Ni et al., 2020a). In rare cases, collective actions have led to better mental health outcomes, possibly due to cathartic experiences (Greenley et al., 1975; Lyons, 1973).
Nigeria has a long history of protests, yet very little is known about the mental health sequelae of collective actions in this setting (Ojeahere et al., 2021). In a systematic review of studies focused on mental health outcomes following collective actions around the world (Ni et al., 2020a), only three studies were identified from Sub-Saharan Africa, one each from Nigeria, Kenya and South Africa. The paucity of research in this field of enquiry in Sub-Saharan Africa translates to a poor understanding of the drivers of collective actions, many of which are also drivers of poor mental health in themselves at the population level. It also translates to a dearth of data on the burden and socio-political determinants of mental health after collective actions, which in turn hampers policy and service response at both individual and population levels (Ni et al., 2020b; Ojeahere et al., 2021). In this study, we set out to determine the burden of mental health morbidity and its determinants in the aftermath of the #EndSARS protest.
Methods
Design
Nigerian social media users were invited to complete a one-off online anonymous survey between 21 February and 1 April 2021. The survey was in English and was displayed to the participants using Google forms. Google forms is an online survey platform that collects data anonymously from respondents and also collects timestamp information of when each response to the survey was submitted. It automatically collates and displays graphical information for each survey question. The data can then be extracted from this platform into a Microsoft Excel sheet for analysis. The collected data were stored anonymously and password-protected in the Google application suit. No personal identifiers were required in responding to the survey.
Setting, sample and sampling
The sample for the study was drawn from users of social media platforms such as Facebook, Telegram, WhatsApp, Instagram and Twitter. The sampling technique was convenience sampling.
Study instruments
The first part of the survey enquired about basic sociodemographic information of the respondents, such as age, gender, employment, place of origin and place of residence. The second part of the survey focused on the respondents’ perception of and attitude to the #EndSARS protest, such as the perceived cause and outcome of the protest. Specifically, in this section, we asked if the respondents participated in the protests in person or online. In-person participation entailed physical presence and participation in the activities at the protest site/sites at least once. Online participation entailed creating, promoting, consuming and engaging with protest-related content online as well as helping to organise resources online for use during the protest. The third part consisted of tools assessing psychiatric morbidity, including substance use and suicidal ideation. The 12-item General Health Questionnaire (GHQ-12) (Goldberg, 1978) was used to assess psychological distress. It has been validated and used extensively among community samples in our setting (Gureje and Obikoya, 1990), including among residents of conflict-affected communities (Okwaraji et al., 2017). We used the 0-0-1-1 scoring system in this study, with a cut off of 3, which is the optimal cut off point for the instrument in this environment (Abiodun, 1993; Gureje and Obikoya, 1990). Anxiety and depression were assessed with the Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983). It is a simple and reliable tool designed for use among both hospital and community samples to assess for anxiety and depressive symptoms. It has been shown to have good psychometric properties when used in this setting (Abiodun, 1994). We used a cut off of 8 for both the HADS anxiety and depression sub-scales, as this is the optimum cut off point for the sub-scales in our setting (Abiodun, 1994). We assessed post-traumatic stress symptoms using a list of items from the PTSD module of the Mini International Neuropsychiatric Interview, version 5.0.0 (MINI) (Sheehan et al., 2010). The MINI has algorithms for making Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnoses as well as built-in skips that allows the screening out of non-cases, without going through the entire module. In this survey, all the items in the module were presented to the respondents without the skips, and the presence of PTSD determined by applying the algorithm to endorsed items.
We assessed suicidal ideation with the first two items of the Columbia Suicide Severity Scale (Posner et al., 2011). The items enquire about the wish to die and thoughts of killing oneself in the previous 2 weeks. An ad hoc questionnaire designed for the study enquired about the trajectory of use of the different categories of psychoactive substances listed in the International Classification of Diseases, 10th edition (ICD-10) in the 3 months since the protest. All respondents who endorsed decreased, same or increased level of use were categorised as current users of any psychoactive substance. This was done because of the very small numbers in the different categories, for ease of analysis.
The fourth segment of the survey assessed resilience and exposure to traumatic events during the protest. The 6-item Brief Resilience Scale (BRS) (Smith et al., 2008) was used to assess resilience. The response to each item is rated on a Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree) for the positively framed statements; responses are reversed for the negatively framed items. All the scores on the six items are added and divided by six to obtain an average score. The total score on the BRS range from 6 to 30. Items from the Harvard Trauma Questionnaire (Mollica et al., 2004) were used to enquire about exposure to traumatic events during the protest. The items on the tool enquired if the respondent had either witnessed or experienced traumatic events ranging from forced separation and torture to death of loved ones. Respondents who endorsed either witnessing or experiencing any of the listed traumatic events on the tool during the protest were adjudged to be exposed to traumatic events.
Additionally, we accounted for confounding by including an item that enquired whether the respondent had had a mental health diagnosis from a medical or mental health practitioner in the past, before the protest. And because data collection for this study was at the peak of the first wave of COVID-19 pandemic in Nigeria, we included four COVID-19-related variables as part of the survey to adjust for the effects of the pandemic on the mental health outcomes of the respondents. The items enquired (1) if the respondent had been worried about contracting COVID-19, if they had tested positive to COVID-19 or if they had been treated in hospital for COVID-19; (2) if they had been affected economically by COVID-19 pandemic or by government response to the pandemic, such as lock down or curfew, (3) if any of their friends or relatives had been diagnosed of, treated for or died from COVID-19, if they were worried that their friends or relatives would contract COVID-19 and (4) if any of their friends or relatives had been affected economically by COVID-19 pandemic or government response to the pandemic, such as lockdown or curfew.
Ethical approval to conduct the study was obtained from the UI/UCH Institutional Review Board.
Procedure
The link to the survey, as well as an introductory message, was disseminated to all the popular social media platforms in Nigeria. The introductory message to the survey explained briefly the purpose of the survey and assured anonymity. Clicking on the link to the survey led to an informed consent form page which each respondent must read and endorse to access the survey proper. Weekly reminders were sent to each of the platforms throughout the study period.
Statistical analyses
Data extraction was performed by authorised data managers and statisticians. Analysis was done using SPSS version 25. Demographic, trauma and protest-related variables, and mental health outcomes were presented with descriptive statistics. Continuous variables with normal distribution such as resilience scores were compared between protesters and non-protesters using T test. Associations of these variables with psychological distress, depression and anxiety were further tested with bivariate statistics. For the purpose of inferential analyses, resilience scores were dichotomised into ‘high’ and ‘low’ scores, with low scorers being those with scores below the mean and high scorers being those scoring mean score and above. Variables that were significantly associated with the mental health outcomes were then entered into regression models for each outcome. As mentioned earlier, previous mental health diagnosis and effects of COVID-19 pandemic were adjusted for in each model. Exposure to trauma was excluded from further analysis for reasons of multi-collinearity. Level of statistical significance was set at p < 0.05 for all analyses.
Results
Demographic characteristics of protesters and non-protesters
A total of 426 subjects completed the online survey. In total, 312 (73.2%) reported participating physically or online in the protests (protesters), while the rest (114, 26.8%) did not participate (non-protesters). There were overlaps in the mode of protest participation among protesters, and this differed by place of residence (not in tables). While almost all the protesters from Southern Nigeria (274, 99.6%) and all the protesters from Northern Nigeria (34, 100%) participated online, 63 (22.9%) of the southern online protesters and 6 of the Northern online protesters (17.6%) also participated physically. The majority of the protesters were younger than 35 years (257, 82.6%), while about half of the non-protesters (59, 52.7%) were older than 35 years (Table 1). Four in five non-protesters had postgraduate degrees while only a quarter of the protesters had postgraduate degrees. About a third of the protesters reported being gainfully employed while the rest were under- or unemployed. These proportions were reversed for the non-protesters. Most of the protesters were single, divorced or separated (229, 73.4%), while about three in five non-protesters were married or cohabiting with a partner (67, 58.8%). The vast majority of the protesters reported being born or resident in the southern part of the country (90.7% and 89.0%, respectively). Among the non-protesters, the corresponding proportions were 67.5% and 71.7%, respectively.
Demographic characteristics of respondents.
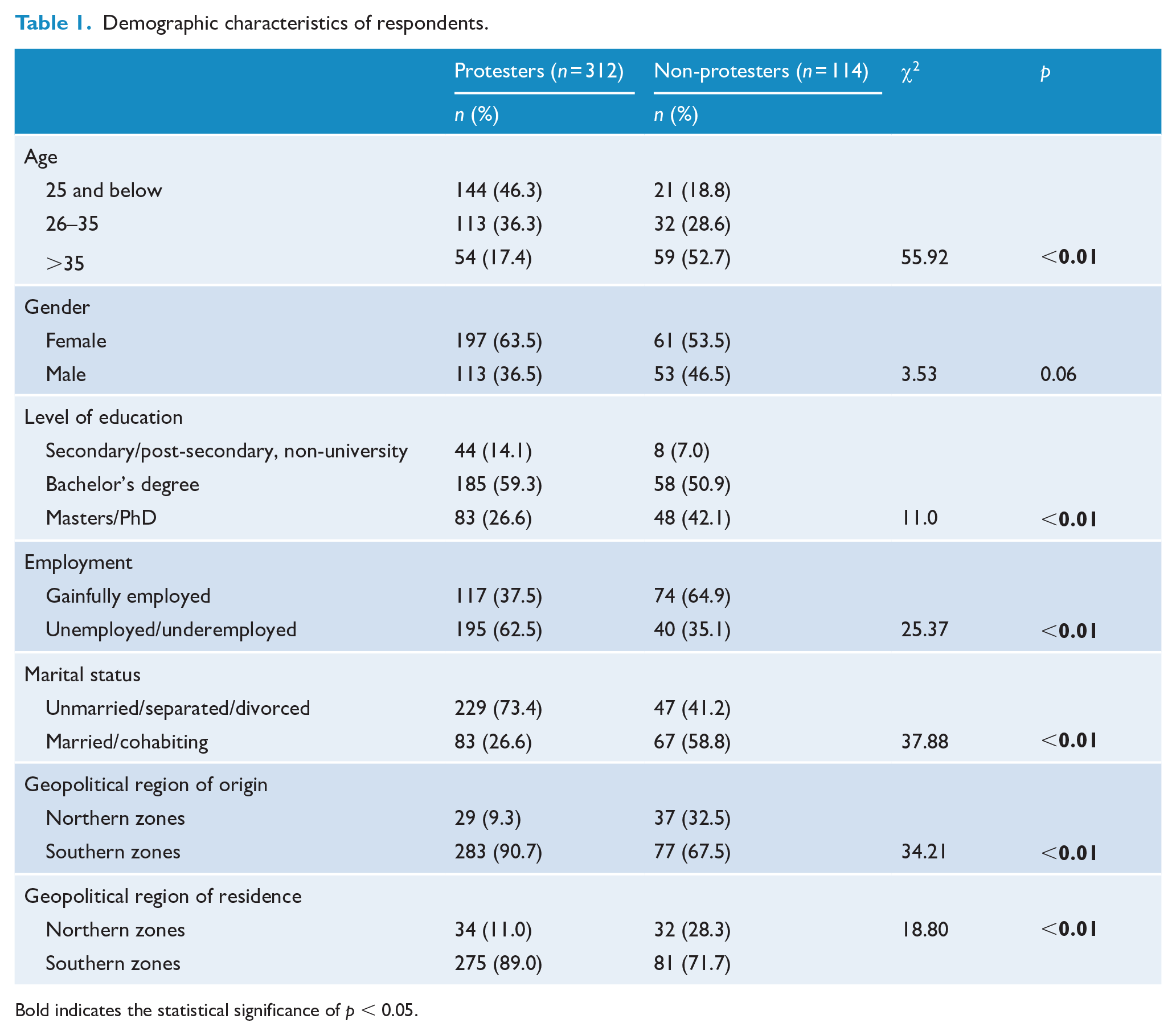
Bold indicates the statistical significance of p < 0.05.
Perception of and attitude to the protest among protesters and non-protesters
Protesters and non-protesters were fairly agreed on the perceived top two causes of the protest, namely police and SARS brutality (90.7% for each of the causes among protesters, and 86.0% and 73.7%, respectively, among non-protesters) (Table 2). The other perceived causes of the protest are shown in Table 2. More than 9 in 10 protesters agree that the protest was justified while two thirds of the non-protesters held this opinion. Majority of the protesters and the non-protesters, respectively, believe that some good came out of the protest (77.9% vs 64.0%), that the protest was justified (92.6% vs 63.2%) and that peaceful protests were desirable (96.2% vs 90.4%). However, only a small proportion of both the protesters and non-protesters believe that the protest achieved its purpose overall (12.5% vs 11.4), or that the protest had a negative impact on them (22.8% vs 21.9%) or their family and friends (27.2% vs 29.8%), respectively. Similarly, only a small proportion of both the protesters and non-protesters would take part in or support violent protests (8.7% vs 7.0%). The majority of the protesters but not the non-protesters believed protests were opportunities to connect with others (77.9% vs 51.8%) and would participate in future protests (71.8% vs 19.3%), respectively.
Perception of and attitude to protest among protesters and non-protesters.
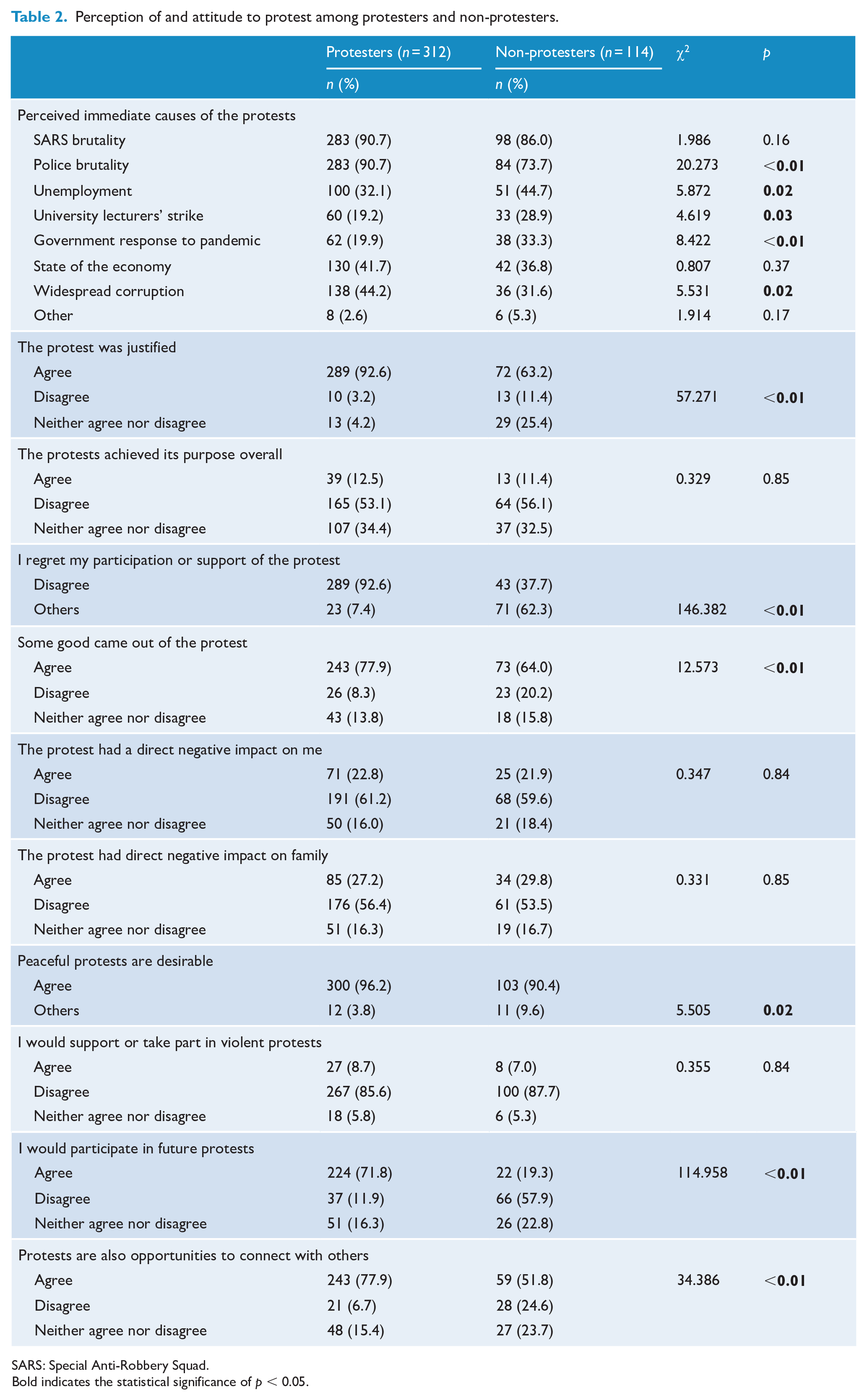
SARS: Special Anti-Robbery Squad.
Bold indicates the statistical significance of p < 0.05.
Exposure to traumatic events during protest
A significantly higher proportion of the protesters, compared to non-protesters, reported witnessing or experiencing at least one traumatic event during the protests (47.8% vs 35.1%, χ2 = 5.4, p = 0.02) (not in any table). The most commonly encountered traumatic experiences among protesters during the protest were murder of strangers (30.8%), ‘other situations that was very frightening’ (26.3%), being close to death (24.4%), serious injury and torture (20.8%). Among non-protesters, the commonest traumatic events encountered included ‘other situations that was very frightening’ (19.3%), murder of strangers (14.0%), lack of food or water (14.0%), sexual abuse or rape (12.3%) and brainwashing (12.3%).
Resilience
Protesters scored significantly lower on the resilience scale compared to non-protesters (mean = 20.4, SD = 4.6 vs mean = 21.4, SD = 4.2, T test = 2.07, p = 0.04).
Mental health outcomes among protesters and non-protesters
The prevalence of mental health outcomes among protesters and non-protesters, respectively, were 44.2% vs 29.8% (χ2 = 7.2, p < 0.01) for psychological distress, 51.0% vs 29.8% (χ2 = 15.1, p < 0.01) for anxiety, 26.0% vs 14.9% (χ2 = 5.8, p = 0.02) for depression, 7.4% vs 1.8% (χ2 = 4.8, p = 0.03) for PTSD, 11.2% vs 4.5% (χ2 = 4.3, p = 0.04) for current substance use and 7.1% vs 4.4% (χ2 = 0.1, p = 0.32) for suicidal ideation.
Predictors of mental health outcomes among protesters and non-protesters
After adjusting for previous mental health diagnosis and the effects of the pandemic, the odds of psychological distress among protesters was increased nearly threefold among respondents with low resilience (odds ratio [OR] = 2.87, p < 0.01) (Table 3), twofold among those who held that the protest was caused by the state of the economy (OR = 1.99, p = 0.01) and twofold among those who believed that the protest had a direct negative impact on them (OR = 2.29, p = 0.04). Only under-/unemployment predicted psychological distress among non-protesters (OR = 4.08, p = 0.03).
Predictors of psychological distress among protesters and non-protesters during the EndSARS protest.
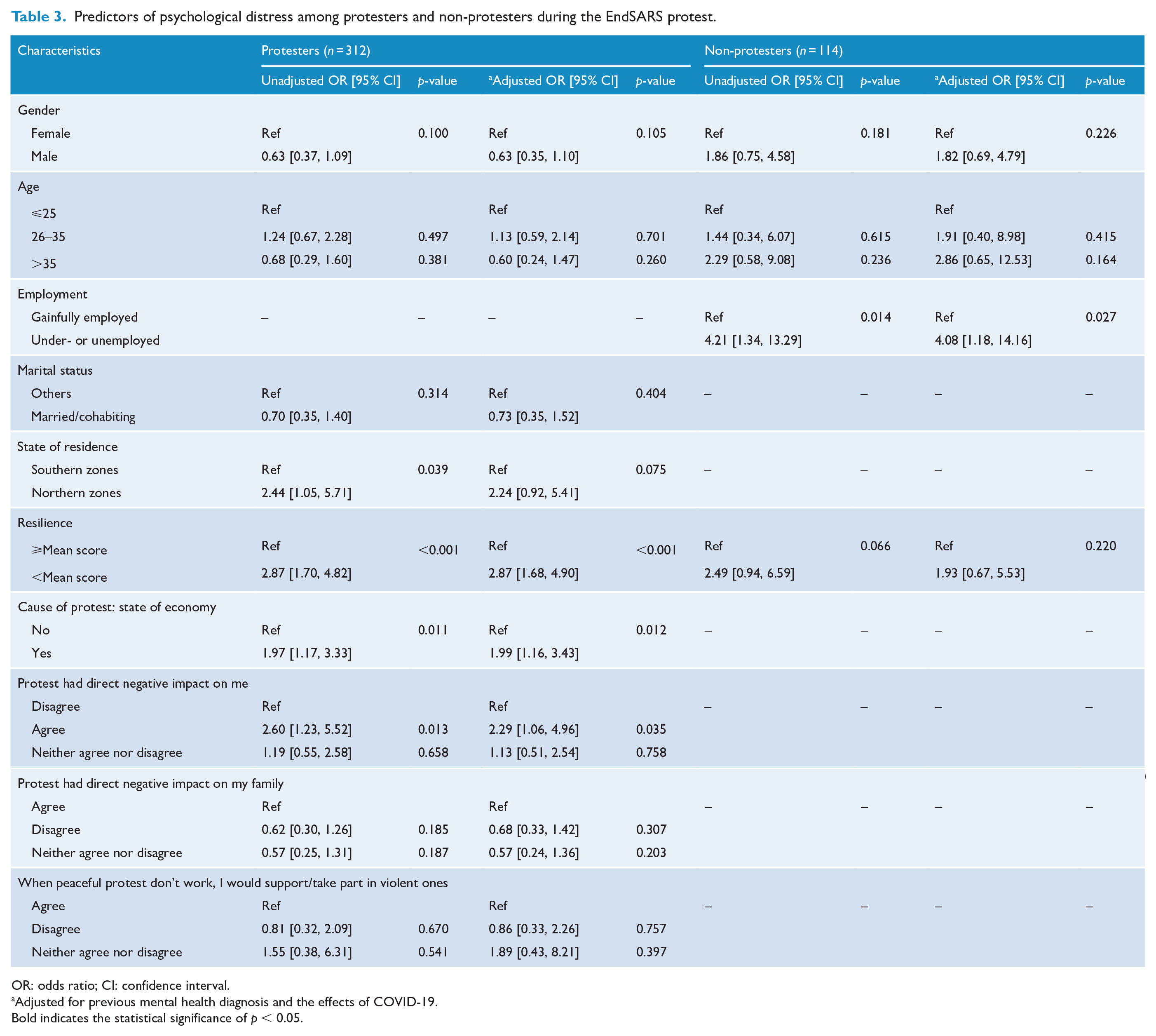
OR: odds ratio; CI: confidence interval.
Adjusted for previous mental health diagnosis and the effects of COVID-19.
Bold indicates the statistical significance of p < 0.05.
The odds of depression was increased among protesters who were under- or unemployed (OR = 2.46, p = 0.03) (Table 4), those who were from Northern Nigeria (OR = 4.64, p < 0.01), among respondents with low resilience (OR = 4.66, p < 0.01) and among respondents who would join future protests (OR = 4.13, p = 0.02). After adjusting for previous mental health diagnosis and the effects of COVID-19, there was no significant predictor of depression among non-protesters.
Predictors of depression among protesters and non-protesters during the EndSARS protest.
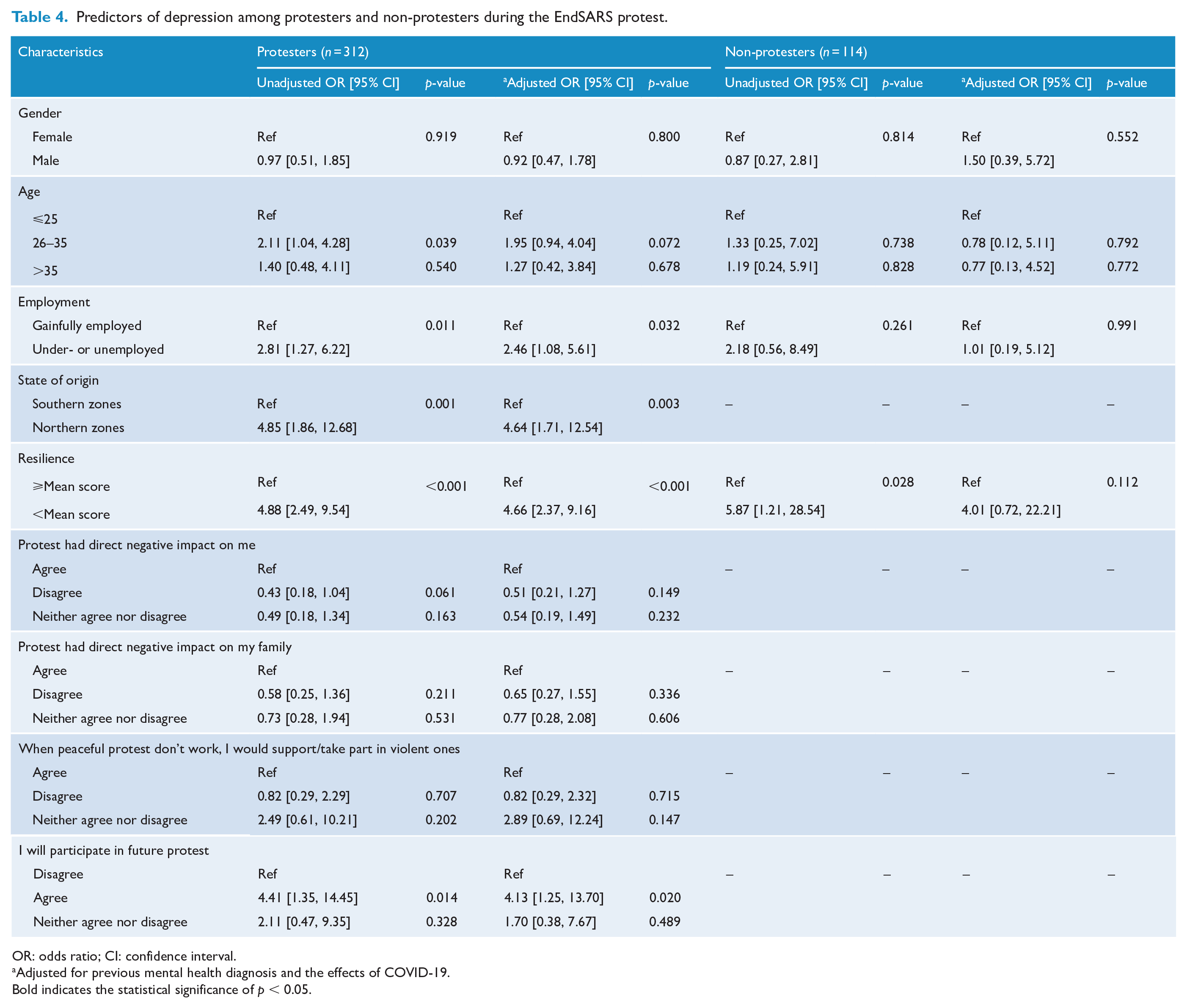
OR: odds ratio; CI: confidence interval.
Adjusted for previous mental health diagnosis and the effects of COVID-19.
Bold indicates the statistical significance of p < 0.05.
The independent predictors of anxiety among protesters were under- or unemployment (OR = 2.09, p = 0.02) (Table 5), being from Northern Nigeria (OR = 2.80, p = 0.03) and scoring low on resilience (OR = 3.13, p < 0.01). Among non-protesters, however, the predictors of anxiety were being unmarried (OR = 7.36, p < 0.01) and low resilience (OR = 5.35, p < 0.01).
Predictors of anxiety among protesters and non-protesters during the EndSARS protest.
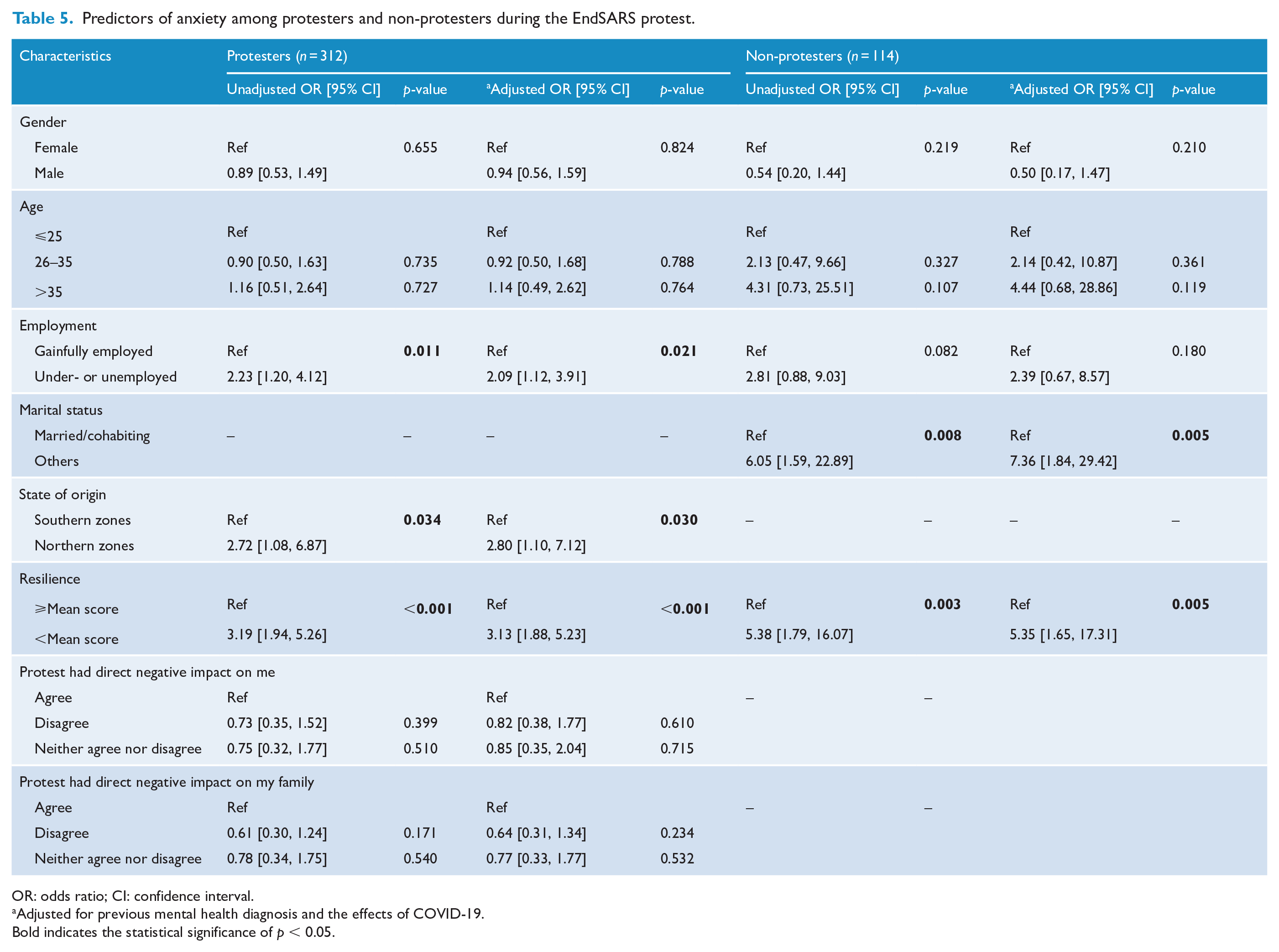
OR: odds ratio; CI: confidence interval.
Adjusted for previous mental health diagnosis and the effects of COVID-19.
Bold indicates the statistical significance of p < 0.05.
Discussion
To our knowledge, this is the first study to assess a wide range of mental health outcomes following a major protest in Nigeria. Although prior to this study, concerns have been raised by the Nigerian mental health community about possible effects of the #EndSARS protests on the mental health of Nigerians (Ojeahere et al., 2021), judging by reports of an increase in the number of helpline calls received by non-governmental organisations during and after the #EndSARS protest (Chika and Mogo, 2020), our study is the first to systematically investigate these concerns. This study is also one of the first few to investigate in depth the effects of perception of and attitude to protests on mental health.
Compared to non-protesters, the respondents who participated in the protests (on site and online) were younger, with a larger proportion of them being unmarried and under-/unemployed. This can be explained by what McAdam (1986) called ‘biographical availability’ in the theory of recruitment into activism. Biographical availability refers to the absence of personal constraints, such as full-time employment, marriage and family responsibilities that may increase the ‘costs’ and ‘risks’ of participating in a social movement such as a protest. McAdam posited that individuals who are more ‘biographically available’ would be more likely to participate in ‘high-risk/cost’ activism such as protest. The costs here refer to time, energy and money, and risks refer to the risks of participation, such as physical harm or social, legal and financial repercussions. This pattern was also observed among protesters in the 2019 Hong Kong prodemocracy protests (Buschmann, 2019).
Another potential explanation for the younger age of the protesters is the public perception and anecdotal accounts that police and SARS brutality had been largely directed at persons below the age of 35 years, making the protest resonate well with this age group (Amnesty International Nigeria, 2020). A study in the United States found that media exposure to police killings of unarmed black Americans had a differential adverse effect on the mental health of Black Americans, but not white Americans, in the general U.S. population. It seems plausible therefore that younger persons participated more in the protests as an avenue to vent the distress stemming from exposure to police brutality to their kind in the media. Considering that Nigeria is a predominantly youthful population and most mental disorders begin around 12–24 years (Patel et al., 2007), a potential strategy for the prevention of incident mental disorders is by addressing police brutality as a risk factor, in addition to other interventions known to be effective in preventing and responding to mental disorders in settings with scarce mental health resources like ours.
We found elevated rates of psychiatric morbidity, with protesters having significantly worse outcomes on almost all measures of psychiatric morbidity. There is compelling evidence that collective actions generally affect mental health adversely (Ni et al., 2020a). Bearing in mind differences in sample population, sampling techniques and study designs, our rates compare well with what have been reported in the literature (Ni et al., 2020a). For example, a 10-year prospective study of a probability sample of the general adult population in Hong Kong found two spikes in the prevalence rates of probable depression following two different protests (6.5% in 2017 and 11.2% in 2019) from the pre-protest levels of 1.9% (Ni et al., 2020b). During the 2007–2008 Kenyan crises, Bamrah et al. (2013) found prevalence rates of depression between 29% and 39% among internally displaced persons and between 27% and 42% among patients with HIV in affected regions. Similar rates were found among community members and law enforcement agents living close to Fergusson, Missouri during the 2014 Ferguson protest (Galovski et al., 2016). In a review of mental health sequelae following collective actions, Ni et al. (2020a) found that the prevalence of anxiety symptoms ranged from 10.5% in a probabilistic general adult sample immediately following the 2014 Hong Kong Occupy Central/Umbrella Movement (which increased to 47.4% 2 months after) through 55% among school children near protest sites in Egypt to 69% among general practice patients during a riot in Northern Ireland. Evidence from previous work suggests that the differences found between protesters and non-protesters in the current study may be due to a number of factors found to be predictive of poor mental health: participation in protests, proximity to the area of protest (Bamrah et al., 2013; Galovski et al., 2016; Obilom and Thacher, 2008), and differential exposure to trauma and violence, both in person and on social media (Ni et al., 2020b; Obilom and Thacher, 2008).
Of note, the prevalence rates of post-traumatic stress disorder (PTSD) in our study were much lower than previously reported rates following collective actions both in Nigeria and elsewhere. Obilom and Thacher (2008) found a prevalence of PTSD symptoms of 41% among inhabitants of areas where the 2001 ethnoreligious riots took place in Jos, Nigeria. There are a number of methodological differences between this study and ours. The study population lived in the areas affected by conflict, the scale of violence was much larger (over 500 killed and 958 injured) and data were collected 7–9 months after the riot. Reported prevalence of PTSD in previous collective actions range from 4.1% to 75% (Ni et al., 2020a, 2020b). Despite these methodological differences, the elevated levels of psychiatric morbidity among protesters, and to a lesser extent, non-protesters is a wake-up call for mental health professionals, policy makers and non-governmental stakeholders in the Nigerian mental health system to invest in mental health during collective actions and at other times (Ojeahere et al., 2021).
Only personal and demographic factors (low resilience and not being in a marital relationship), but not protest-related factors, predicted poor mental health among non-protesters. Unsurprisingly, these are established risk factors expected in the general population. Similarly, consistently, low resilience predicted poor mental well-being among protesters for the different measures of morbidity. Described as ‘the process of withstanding the negative effects of risk exposure, demonstrating positive adjustment in the face of adversity or trauma, and beating the odds associated with risks’ (Bartley, 2006), resilience is a core construct common to mental well-being in the general population, as well as in populations experiencing disasters and collective actions (Goldmann and Galea, 2014; Ni et al., 2020a). Investing in programmes focusing on building resilience is a key mental health promotional activity that can be targeted at individuals across the lifespan, and especially at young persons (Patel et al., 2007), spanning multiple sectors such as education, housing, poverty alleviation and employment (Bartley, 2006). This has the advantage of addressing the grievances leading to collective actions in the first instance, fortifying individuals in times of crises and improving the chances of young persons at contributing meaningfully to society.
Under-/unemployment predicted mental health among both protesters and non-protesters in the current study, consistent with findings in a previous study of collective actions (Ni et al., 2016). There is strong evidence that unemployment is not only associated with mental distress, it also causes it (Paul and Moser, 2009). The detrimental effects of unemployment on mental health is worse in economically less developed countries, in countries with high-income inequalities and in countries with weak unemployment protection (Paul and Moser, 2009), all these factors being ubiquitous in low- and middle-income countries. Holding a view that the protest was caused by ‘the state of the economy’ was also associated with worse mental health in this study. It is plausible that individual affected more by the economic downturn were those who held this view and this may be responsible for the observed association with poor mental health, similar to the effect of unemployment. The case has been made above for investment in social interventions that not only build resilience but also promote mental wellbeing.
We also found that being of Northern Nigerian origin or residing in Northern Nigeria was associated with poor mental health. This finding negates findings from previous collective actions research that had found proximity to the site of protest as a predictor of psychiatric morbidity (Bamrah et al., 2013; Galovski et al., 2016; Obilom and Thacher, 2008). However, most of the protesters in this study who were of Northern Nigerian origin or residing in the north could only participate in the protest online, and possibly spent an inordinate amount of time-consuming protest-related content, compared to their southern counterparts. A large-scale epidemiological study of mental health following a major unrest found an association between social media use and increased depressive symptoms (Ni et al., 2016). This finding in our study can also be explained by the socio-political history and reality of Nigeria. Although Nigeria is made up of more than 500 ethno-linguistic groups (Central Intelligence Agency (CIA), 2021), a rather simplistic north-south geopolitical division has become popular in public discourse, with a long history of mistrust and political tension between the two over perceived inequality in power and resource allocation among the elite, in favour of the north (Sokuma, 2021). The poorer mental health of the northern respondents may therefore be due to psychological reaction to concerns of reprisals from the south.
Protesters who believed that the protest had a direct negative impact on them reported a higher level of psychological distress. There is considerable theoretical support for (Lazarus and Folkman, 1984) and empirical data (Keller et al., 2012) supporting the notion that irrespective of the magnitude of a stressor (protest in this case), the psychological impact of the stressor on an individual is predicted by their appraisal of their susceptibility to as well as their appraisal of the magnitude of the stressor, suggesting that interventions such as cognitive behaviour therapy could be promising in the context of mental health during collective actions. Finally, we found that willingness to participate in future protests predicted depressive symptoms. It is plausible that willingness to participate in future protests is an indication of ongoing distress, or the presence of the psychosocial drivers of such distress. Future research needs to shed light on this association.
Limitations
Our study has a number of limitations within which our results should be interpreted. The study was an online survey, and it is possible that only respondents inclined to participating in online surveys responded to it. Similar to this, the sampling technique was purposive, and was neither representative of protesters nor non-protesters, limiting its generalisability. However, the choice to analyse data separately for protesters and non-protesters afforded us the opportunity to understand the mental health peculiarities of the two sub-populations. Third, because our data were collected at the height of COVID-19 pandemic and government restrictions in Nigeria, the elevated levels of psychiatric morbidity may be due to the additive effects of these to the protest. However, in investigating for predictors, the effects of the pandemic were adjusted for in our models. Fourth, the tools used in this study were self-report measures administered about 100 days after the protest, suggesting the possibility of recall bias. Fifth, the relatively smaller number of the non-protesters may have reduced the power to detect some of the predictors of poor mental health in this sub-group. Sixth, due to the design of the study and the considerable overlap in the mode of protest participation, we were unable to investigate the effects of proximity to the site of protest and exposure to online content as predictors of psychiatric morbidity during the protests. Finally, this was a cross-sectional survey and causal attributions cannot be made.
Conclusion
In conclusion, in this study we found that compared to non-protesters, the vast majority of protesters during the #EndSRS protest were young, unmarried and unemployed, a unique vulnerable group. We also found elevated levels of psychiatric morbidity among protesters and non-protesters, with significantly worse outcomes among protesters than non-protesters. Protesters and non-protesters differed significantly with respect to predictors of poor mental health outcomes, with only personal and demographic characteristics being relevant to non-protesters, while personal, demographic and protest-related variables predicted distress among protesters. This brings to the fore the importance of socio-political predictors of mental health.
Overall, the take-home message from our study include the need for mental health professionals to be aware of the psychological sequelae of protests in our setting, and the need for government and non-governmental actors, and policy makers to invest in the mental health of populations generally and that of young persons specifically, before and especially during collective actions. Our findings also point to the need to invest in programmes that promote resilience as well as in policies that address social and political determinants of mental health. Future research should employ larger sample sizes and adopt longitudinal designs.
Footnotes
Acknowledgements
The authors wishes to thank ASIDO Foundation, Nigeria, for their help in carrying out this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.