
Abstract
One consequence of the so-called ‘revolution’ in positive psychology has been a considerable shift in focus from models of ill-health to notions of positive well-being that are distinct from negative well-being states. However, the view that wellness is simply the absence of mental and physical ill-health has long been challenged [1]. More recently, researchers have sought to identify personal characteristics, such as resourcefulness and hardiness, that predispose individuals to better mental ill-health outcomes, with results subsequently informing government population-level health policy [2].
Subjective well-being and mental health
Subjective well-being (SWB) approaches typically focus on individuals’ self-appraisals of affect and judgements of satisfaction [3]. Optimal affective well-being is typically defined in terms of both the presence of positive emotions and absence of negative emotions [4]. Whilst negative affect relates to individuals’ experiences of negative feelings such as sadness, guilt and fear, positive affect is defined in terms of the experience of positive emotions including happiness and energy [5]. The tripartite model of depression and anxiety (TMDA) hypothesizes that low positive affect characterizes depression whilst high negative affect relates to both depression and anxiety [6].
Considerable evidence has supported the TMDA hypothesis relating to the role of positive and negative affect as aetiologies for depression and anxiety [7–9]. Whilst there is consistent evidence for the role of negative affect in both depression and anxiety [10,11], the evidence that low positive affect is a unique etiological component for depression has received mixed support [12,13]. Within a clinical context, the TMDA hypothesis has been supported in a sample of 41 private practice patients who were undergoing cognitive behaviour therapy for depression and anxiety [14]. Over the course of treatment, results were consistent with the tripartite model; reduced negative affect was associated with a reduction in both anxiety and depression, whilst increased positive affect only occurred for those patients who reported a reduction in depression. The importance of this further supports the independent effects of positive and negative affect on depression and anxiety, in particular the notion that positive affect has specific relevance to depression.
Psychological well-being
In contrast to SWB, the psychological well-being (PWB) approach is one that describes wellness in terms of those individual characteristics which are believed to contribute to optimal SWB outcomes (i.e. increased positive affect and decreased negative affect) [3]. PWB constructs typically reflect adaptive cognitive components of self-referent belief systems (e.g. self-concept, control, purpose in life). For example, resilience relates to a network of favourable attitudes and behaviours of self that are associated with adaptive coping strategies to stressful life events and negative life conditions, and resilient people are frequently characterized by an internal locus of control, pro-social behaviour, positive self-image and greater optimism [15–17]. These resilience characteristics are associated with better physical and mental health outcomes [18], and more positive adaptive behaviours to negative life events [19,20]. Mastery is another cognitive component of PWB which reflects a strong self-referent belief in one's capacity to influence the environment and bring about desired outcomes. Considerable evidence links increased mastery to better psychological [21] and physical health outcomes [22,23], and lower mortality risk [24].
Aims
There exists considerable support for the related nature of PWB and SWB components where factorial analytical analyses delineate between affective and cognitive dimensions of well-being whilst demonstrating their interrelatedness [25–27]. The importance of the PWB constructs appears related to their function in promoting better SWB outcomes and positive emotions in particular [26]. However, there is a lack of research concurrently evaluating the relationship between delineated components of PWB and SWB with mental health outcomes such as depression and anxiety.
The aims of the present study were to (i) assess the independence of related PWB (operationalized as resilience and mastery) and SWB (operationalized as positive and negative affect) constructs, (ii) identify the role of PWB in predicting depression and anxiety symptom scores within a TMDA framework, and (iii) demonstrate that current PWB is mostly independent of prior SWB and mental health outcomes. Following prior research into the structure and relationship of PWB and SWB [25,27], we expected factor analysis to identify a measurement model of well-being that discriminated between related PWB and SWB components of well-being. Subsequently, we expected PWB to be a significant predictor of SWB which would in turn predict mental health outcomes. We also expected the association of PWB and mental health to be mediated by positive and negative affect. Our conceptual model is displayed in Figure 1. Furthermore, we expected that current PWB would be largely independent of prior SWB and mental health.
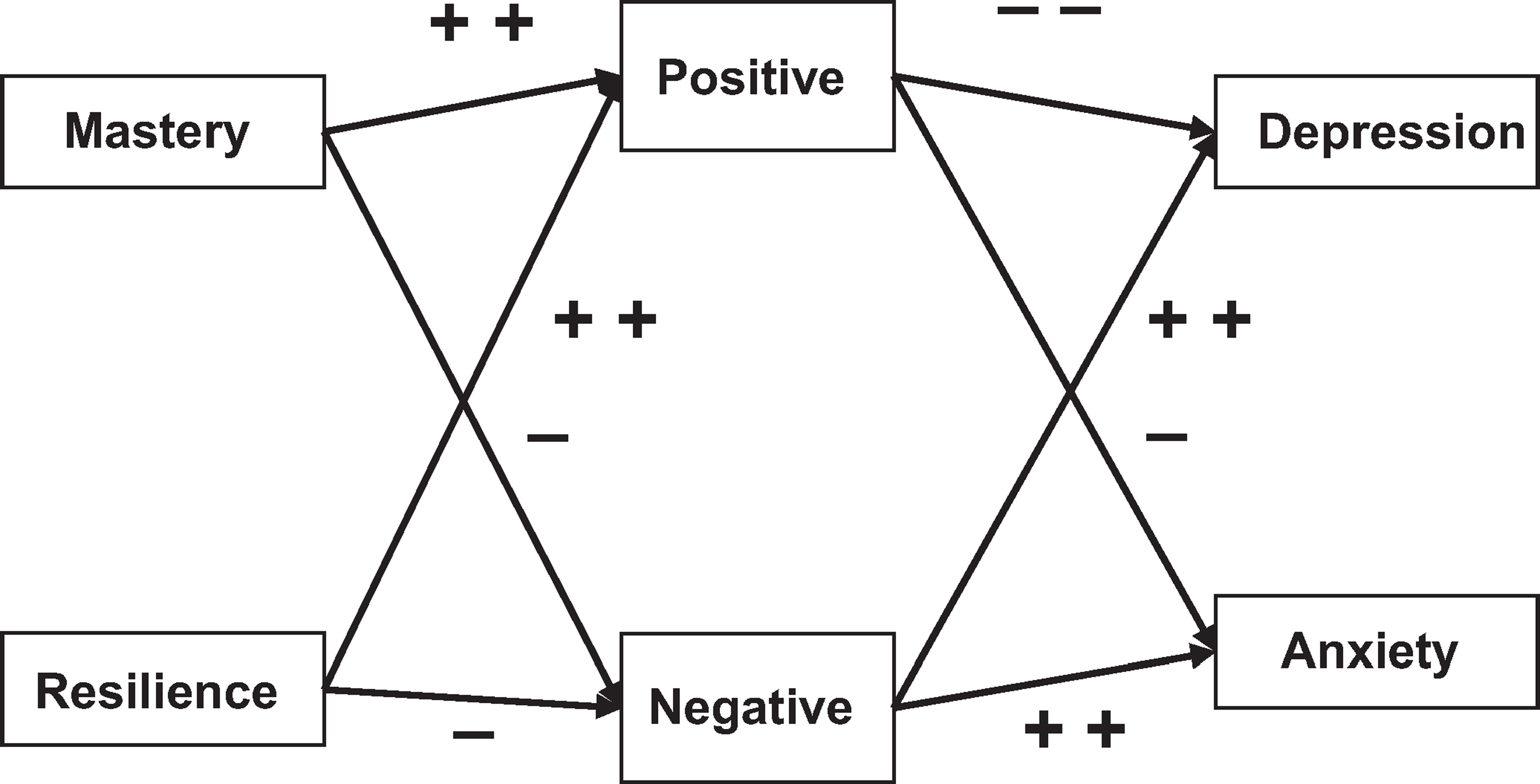
A conceptual model of the role of PWB in a tripartite model of current depression and anxiety (+ weak positive associations; − weak negative associations; ++ strong positive associations; −− strong negative associations).
Materials and methods
Study design and participants
Our sample was drawn from the PATH Through Life Project, a large community survey concerned with the health and well-being of randomly selected individuals from the electoral rolls of Canberra or the neighbouring town of Queanbeyan, Australia [28]. Voting is compulsory in Australia. Results presented here concern the wave 3 data for the youngest and mid-aged cohorts, who were aged 20- to 24- and 40- to 44-years-old at baseline. Although mastery, affect and mental health data were collected at all three waves, a measure of resilience was only introduced at wave 3 and so our analysis focused on this wave. Of the 4934 participants commencing the study in wave 1, 4160 were contactable for assessment eight years later at wave 3 in 2007/2008. Participants (n = 171) were excluded if they were missing 50% or more on items that comprised each scale used in this analysis. Participants (n = 120) missing data on all wave 3 variables, were then imputed using the EM Algorithm in SPSS PASW version 17. Prior (wave 2) affect and mental health were to be used in the analyses as control variables and participants were also excluded if they did not participate or provide affect and mental health data in wave 2. This resulted in a final sample size of N = 3989 participants, 47% of whom were male. In addition, 88% reported their self-rated health as either ‘Good’, ‘Very good’ or ‘Excellent’, 73% were married or ‘defacto’, and 39% reported a university education at bachelor degree level or above. Participants were mostly assessed in their own homes and asked to complete a questionnaire under the supervision of a professional interviewer. Participants received a full description of the study and provided informed consent. The study was approved by the Human Research Ethics Committee at the Australian National University.
Questionnaires
Psychological well-being
Resilience: Connor-Davidson Resilience Scale
The Connor-Davidson Resilience Scale (CD-RISC) [29] (α = 0.918) was used to measure one aspect of PWB. The scale comprises 25 items that measure individuals’ sense of resilience and capacity to change and cope with adversity (e.g. Have a strong sense of purpose, Tend to bounce back after illness or hardship). Respondents indicated agreement with each item on a 5-point Likert scale with higher scores indicating greater resilience.
Mastery: Personal Mastery Scale
The Personal Mastery Scale (PMS) [30] (α = 0.782) was also used to measure PWB. The scale consists of 7 items measuring locus of control (e.g. What happens to me in the future mostly depends on me, I can do just about anything I really set my mind to do). Respondents indicated agreement with each item on a 4-point Likert scale. Internal reliability and construct validity have been reported [31].
Subjective well-being
Positive and negative affect: Positive and Negative Affect Schedule
The Positive and Negative Affect Schedule (PANAS) [32] was used to measure SWB. The scale comprises a 20-item self-report measure of positive (e.g. active, interested; α = 0.917) and negative (e.g. distressed, nervous; α = 0.89) affect with 10 items per construct. Individuals indicated their response on a 5-point Likert scale with higher scores on each scale indicating greater well-being on each dimension. The instrument has proved reliable as a measure of both trait and state measures of affect, depending on the time reference included in the item operative, although correlations between time reference stems are strong [33]. The ‘past month’ reference was used in this study.
Mental health
Depression and anxiety: Goldberg Depression and Anxiety Inventory
The Goldberg Depression and Anxiety Inventory [34] comprises 18 items that list symptoms of depression and anxiety. Participants respond ‘yes’ or ‘no’ to whether they have experienced any of the symptoms. The scale reports high sensitivity and predictive qualities of DSM diagnosis of depression and anxiety [34].
Statistical analysis
To investigate the hypothesis of independence of the SWB and PWB constructs, items from the resilience, mastery, positive and negative affect scales were evaluated using an exploratory factor analysis in PASW version 17. Principal axis factoring with a direct oblimin oblique rotation was used, and factor scores saved using the regression procedure in PASW. To test the second hypothesis, a structural equation model (SEM) was created in SPSS AMOS version 17 to test whether the SWB variables mediated the direct effects of PWB on the mental health outcomes. A second SEM model controlled for prior (wave 2) SWB and mental health outcomes. Standard errors for the SEM were computed from a bootstrap of 200 samples using AMOS version 17. To control for the Goldberg scale distributions that are typically non-Gaussian, the SEM was estimated using both asymptotically distribution-free and maximum likelihood estimation, but results did not differ. A range of goodness of fit indices (GFI) were used to assess model fit and included a test of chi-square distribution, an adjusted goodness of fit index (AGFI), optimal values > 0.9 [35]; a confirmatory fit index (CFI), optimal values > 0.9 [36]; and the root mean square error of approximation (RMSEA), optimal values < 0.06 [37].
Results
Measurement of cognitive and affective components of well-being
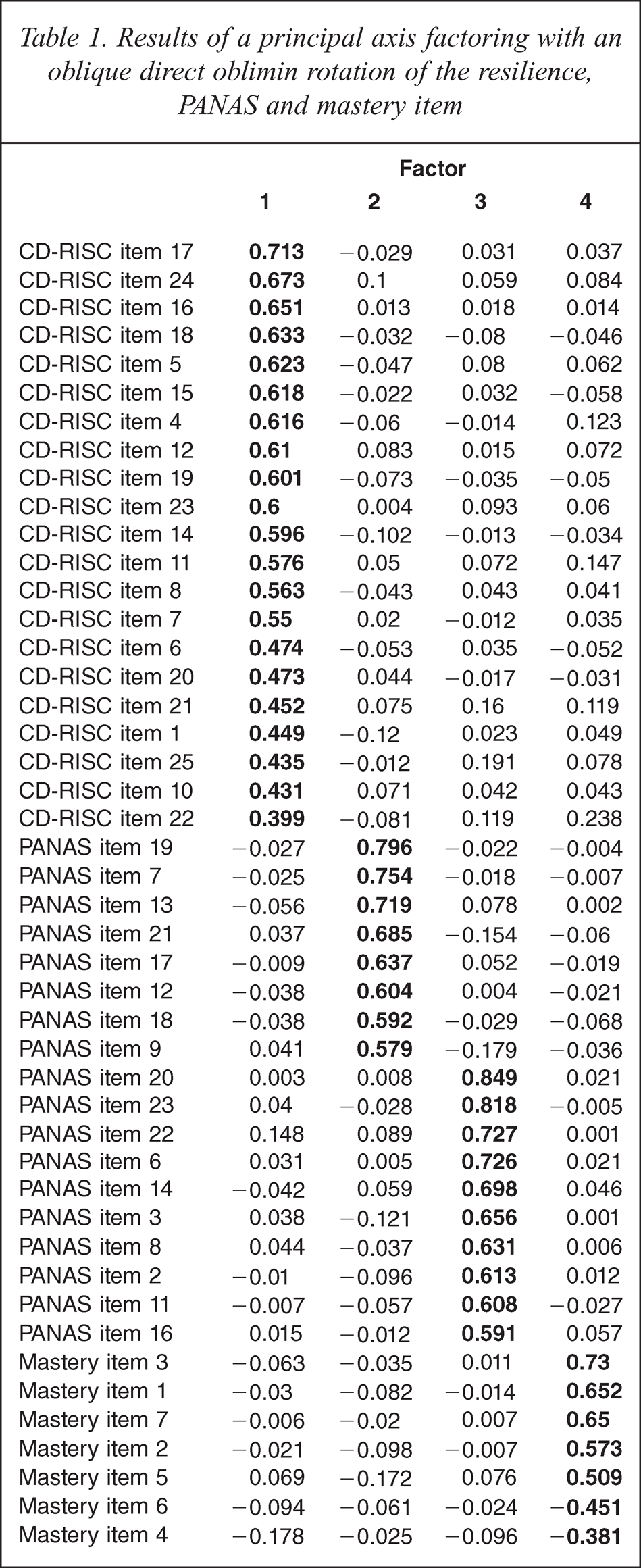
Principal axis factoring (PAF) of the resilience, mastery, and PANAS items revealed a four-factor structure whereby items loaded onto factors that corresponded with the original measures (resilience, mastery, positive affect, negative affect), explaining 51% of item variance (Table 1). Previous factor analysis of the resilience and PANAS items [38] revealed that resilience items 2, 3 and 9 failed to load above 0.32, the level at which a factor explains 10% of the variance in an item, onto a uni-dimensional resilience factor, with this result replicated in the current analysis. All other items loaded onto their respective parent scales, reporting loadings above 0.32. Although discrimination between the four constructs at the item level exists, moderate factor correlations indicate moderate to strong associations with measures of prior and current symptoms of depression and anxiety and prior affect (Table 2). Both Kaiser, Meyer and Olkin's measure of sampling adequacy (KMO = 0.963) and Bartlett's test of sphericity (χ2 = 57235.57, p = 0.000) indicated data appropriate for PAF. For subsequent analyses, factor scores were saved following the factor analysis using the regression method in PASW version 17.
Results of a principal axis factoring with an oblique direct oblimin rotation of the resilience, PANAS and mastery item
Bivariate correlations between the PWB and SWB variables derived from factor analysis with depression and anxiety
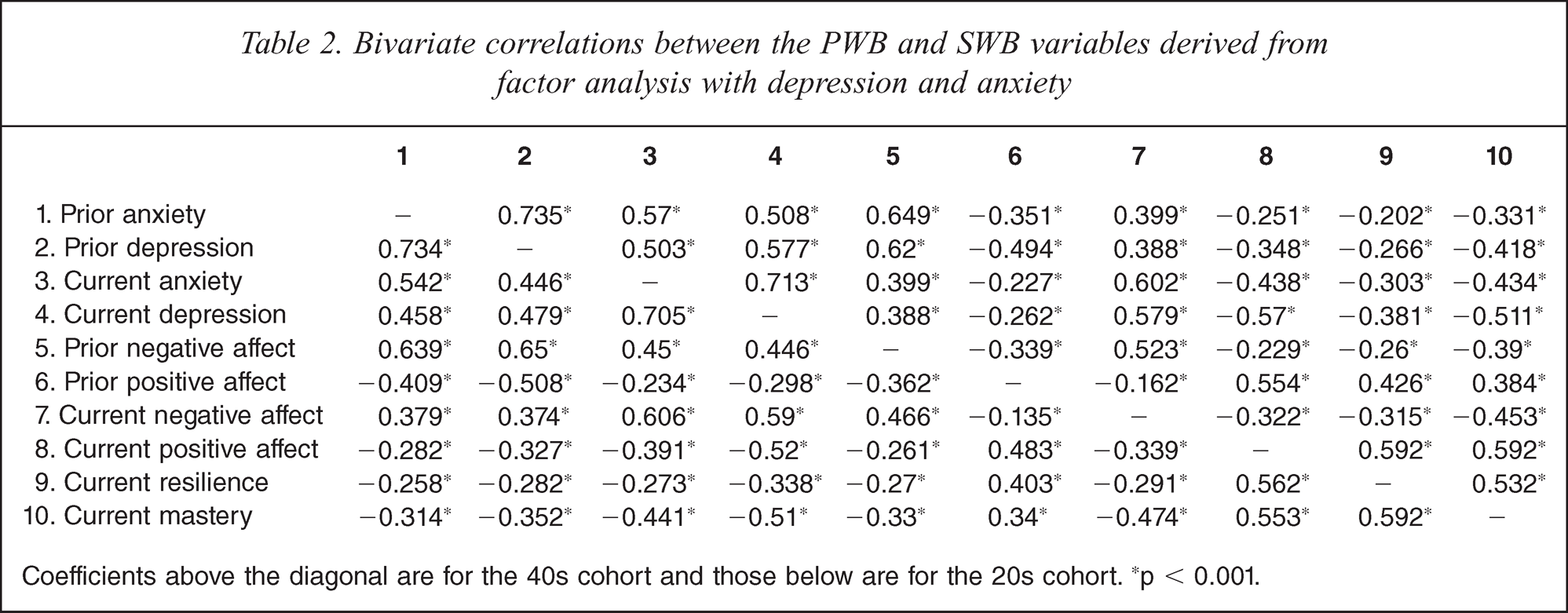
Coefficients above the diagonal are for the 40s cohort and those below are for the 20s cohort. ∗p < 0.001.
Correlations among well-being constructs and depression and anxiety
Correlations between the SWB, PWB and mental health variables are reported in Table 2, by age cohort, with the 40s above the diagonal and the 20s cohort below. The strength of associations appear comparable between age groups. Cross-sectional relationships indicated the co-morbidity of mental health states at both waves, whilst the association across time was moderate for both depression and anxiety. Similar associations were reported for the SWB variables. The association between SWB and mental health variables both within and across waves consistently reported negative associations between positive affect and mental ill-health states, with positive associations between negative affect and mental ill-health. The cross-sectional associations were stronger than the longitudinal associations. Longitudinal associations of prior SWB and prior mental health with the PWB variables were weaker than the corresponding cross-sectional relationships. Prior and current mental ill-health and negative affect were negatively related to PWB, while higher positive affect was related to higher PWB.
Delineating the role of PWB within the tripartite model of depression and anxiety
Following our conceptual model (Figure 1), an SEM was used to test the hypothesis that PWB constructs were significant predictors of SWB and the TMDA hypothesis that SWB components were significant predictors of depression and anxiety. All regression paths were included in the model. A substantial proportion of variance in both the PANAS (positive affect = 42%; negative affect = 20%) and mental health (depression = 49%; anxiety = 43%) variables was explained. Direct and indirect effects of the two cognitive PWB components on depression and anxiety, where positive and negative affect functioned as mediators, were identified (Table 3). Resilience and mastery were both very strong positive predictors of positive affect in particular, but only mastery reported substantial direct associations with depression and anxiety. Whilst results do indicate significant positive effects for resilience on depression (β = 0.047; p < 0.01) and anxiety (β = 0.049; p < 0.001), a review of the standard errors from a bootstrap of 200 samples indicated that these effects are not substantially different from zero and suggests that the significant main effect has limited meaningful contribution to the model (Table 3). Positive and negative affect were clearly the strongest predictors of depression and anxiety.
Comparison of standardized direct and indirect effects on current SWB and mental health
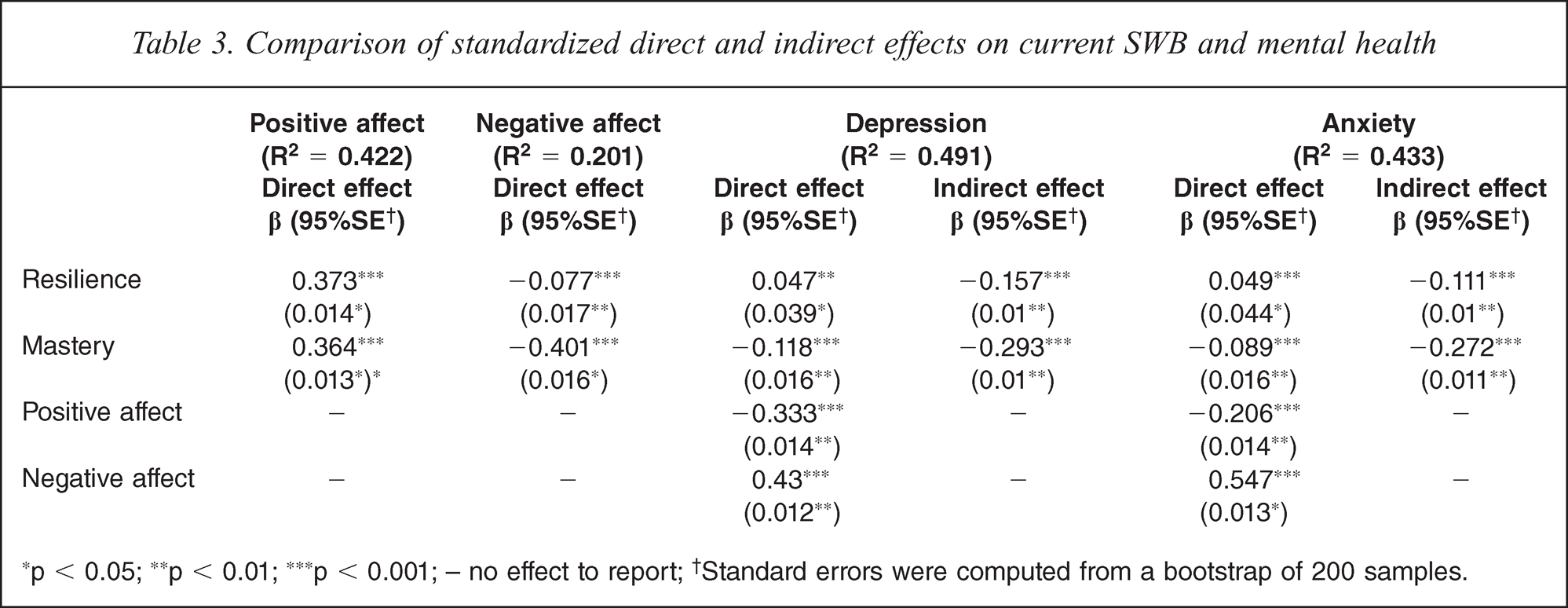
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001; – no effect to report;† Standard errors were computed from a bootstrap of 200 samples.
Following the TMDA hypothesis, lower positive affect was a stronger predictor of higher depressive than anxiety symptoms, whilst negative affect reported comparative associations with both mental health outcomes, although a slightly stronger positive association with anxiety than depression was reported. Several significant mediation effects were identified (Table 3). Positive and negative affect fully mediated the effect of resilience and partially mediated the effects of mastery on both depression and anxiety. Overall GFI revealed strong support for this model (χ2 = 15.557, df = 4, p = 0.004; AGFI = 0.99; CFI = 0.999; RMSEA = 0.027 (90%CI: 0.014–0.042)). A multi-groups analysis revealed no significant differences in the path regression weights between the two age cohorts (Figure 2). Constraining the regression weights to be equal between age groups also reported excellent GFI (χ2 = 36.686, df = 14, p = 0.001; AGFI = 0.991; CFI = 0.998; RMSEA = 0.020 (90% CI: 0.012–0.028)) whilst a comparison between these models (χ2 diff = 21.129; df = 10; p = 0.020), did not indicate superior fit for the unconstrained baseline model. Therefore our findings appear consistent for both young and middle adults.
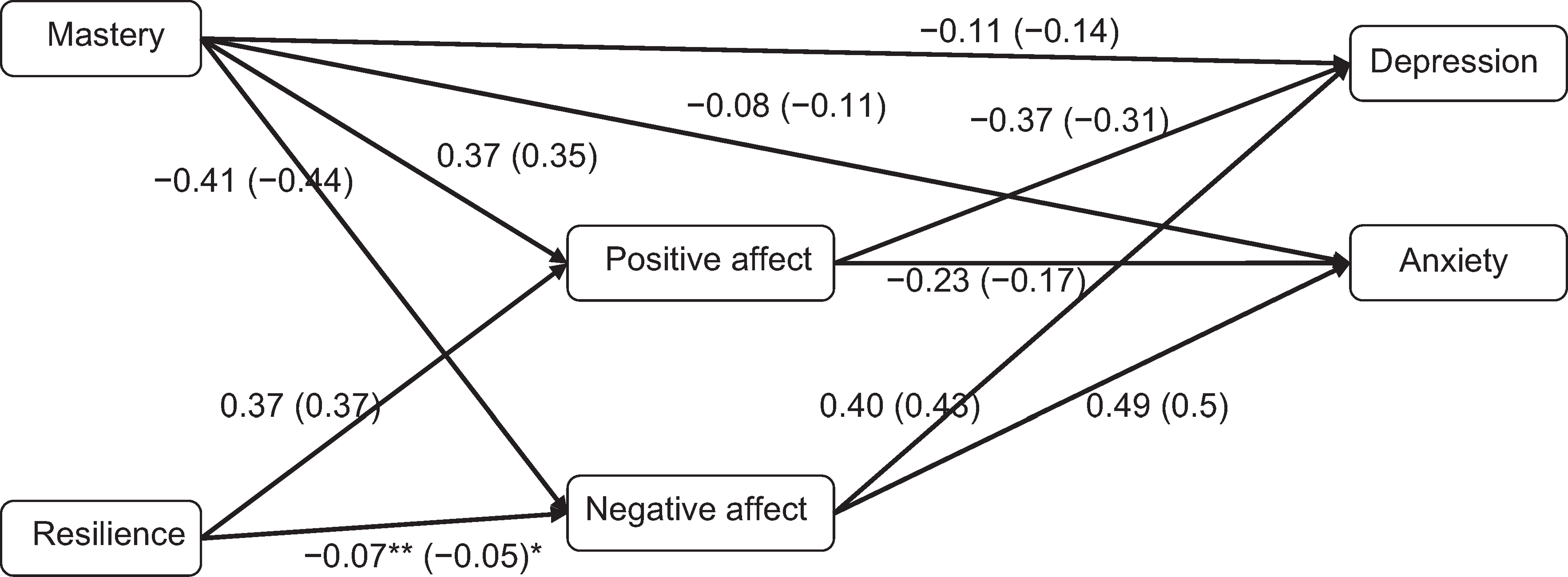
A comparison of regression paths between age cohorts (40s age cohort in parentheses; all coefficients significant at p < 0.001 except for ∗p < 0.05; ∗∗p < 0.01)
Given the longitudinal nature of the PATH study, it was possible to determine the extent to which wave 3 resilience and mastery were associated with prior levels of affect and mental health at wave 2. The degree of variance explained in wave 3 resilience (17%) and mastery (16%) indicate that wave 2 mental health and SWB are mostly unrelated to PWB at wave 3. Instead, prior mental health and affect were most clearly related to their current respective states, and considerably less so with the PWB components (Table 4). The inclusion of prior SWB and mental health variables in our cross-sectional SEM contributed little additional explained variance for either positive affect (2%) or depression (6%), although anxiety (10%) and negative affect (12%) reported slightly larger increases in explained variance. GFI also revealed strong support for this model (χ2 = 34.747, df = 20, p = 0.021; AGFI = 0.987; CFI = 0.998; RMSEA = 0.02 (90%CI: 0.008–0.032)); chi-square analysis did not reveal a significant improvement in model fit in comparison with the previous cross-sectional analysis. For all analyses, a variance inflation factor (VIF) high score of 2.766, and a condition index (CI) high of 6.048, showed that multi-collinearity was not present.
Results of a regression analysis in which prior SWB and mental health predict level of current PWB, SWB and mental health
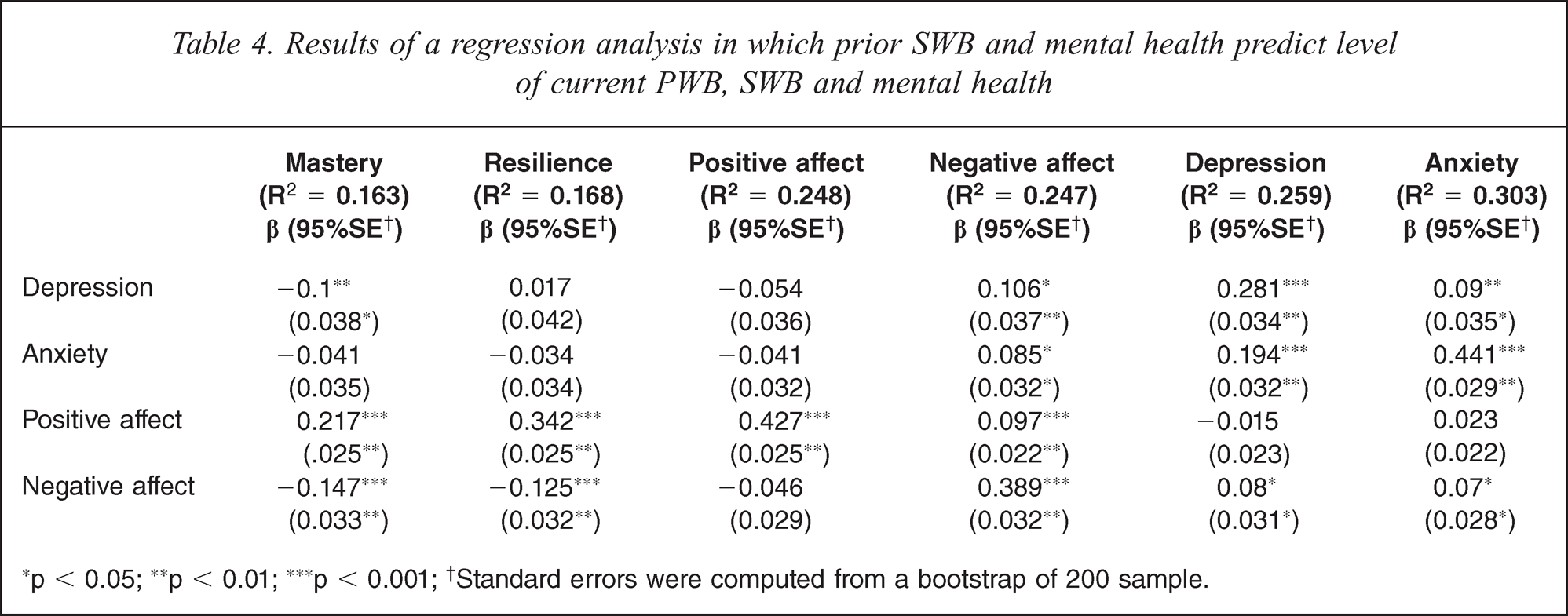
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001;† Standard errors were computed from a bootstrap of 200 sample.
Discussion
In the present study we sought to assess the independence of related PWB and SWB constructs, to identify the role of PWB in mental health outcomes within a TMDA framework and demonstrate that current PWB is mostly independent of prior SWB and mental health outcomes. Construct independence of resilience, mastery and positive and negative affect items indicate that these measures reflect different cognitive and affective components of well-being, whilst moderate correlations between these constructs at a first-order factor level, indicate PWB and SWB as related. Importantly, whilst resilience and mastery were not the most significant predictors of depression and anxiety, they were identified as significant predictors of SWB, in particular explaining half of the variance in positive affect. In addition, the results of an SEM in this study generally support prior findings relating to the TMDA [14,39]. Positive affect was more strongly associated with depression than anxiety, whilst negative affect showed comparable associations with both mental health outcomes. Our findings provide strong support for extending research to investigate positive and negative components of SWB concurrently since they are differentially related to mental health outcomes. Importantly, these findings were consistent across both our young and middle-aged cohorts in our large community sample.
This study identified strong support for the mediating role of positive and negative affect in the relationships between depression and anxiety with resilience and mastery. Support for such a model has been proposed in the literature. The ‘Broaden and Build’ theory of positive emotions [40] describes the reciprocal relationship between positive emotions in developing individual characteristics such as resilience and mastery that further drive current affect states, which following the TMDA hypothesis are significant predictors of mental health outcomes. Our SEM identified resilience and mastery as the strongest predictors of positive affect, whilst prior positive affect was the only variable to report any significant effect on current PWB. Although mastery was a significant predictor of negative affect and reported direct effects on depression and anxiety, its stronger relationship with positive affect support the reciprocal nature of the ‘broaden and build’ hypothesis. Clearly, the strongest associations with the PWB variables were the cross-sectional correlations with current positive affect, but it appears that factors other than prior affect and mental health contribute to explained variance in current resilience and mastery. The importance of PWB should be emphasized since the effects of resilience and mastery on current mental health variables were comparable to the prior mental health and affect variables. In addition, PWB explained considerable variance in current SWB which was itself an important driver of current mental health.
The reported moderate longitudinal associations between the SWB and mental health variables do indicate variability in reported affect and mental health. This possibly supports a set-point theory of affect which proposes that affect states fluctuate around mean levels of affect [41–43]. Interestingly, the longitudinal associations between prior SWB and current PWB and mental health actually support a reversed mediation model to that described by the TMDA, since prior SWB was more strongly related to current PWB than current mental health. However, this is likely the consequence of an epidemiological study design, in which participants were assessed once every four years. Consequently we propose that the TMDA may more accurately describe associations between PWB, SWB and mental health outcomes over shorter temporal contexts and that there are limitations to extending the affect-mental health associations proposed in the TMDA model, which were supported in our cross-sectional analyses, to greater longitudinal contexts. In addition, future research should seek to identify the importance of discerning between stable and reactive natures of SWB which may be related to the likelihood of predicting better mental health outcomes.
There are other limitations to the findings in this study. First, the role of personality was not considered. Although strong associations between extraversion with positive affect and neuroticism with negative affect have been reported, the evidence supporting the relationship between personality and clinically significant mental health outcomes has been less substantial [6]. Whilst several studies have found that neuroticism or emotional instability predicts subsequent onset of depression and anxiety, the relationship with extraversion is less clear [11,44,45]. In particular, it is important to further test the demonstrated relationships between cognitive and affective components of well-being and mental health outcomes after controlling for the personality effects. Whilst, recent analyses [26] controlled for a five-factor personality model and identified PWB as contributing to greater explained variance in positive affect, clearly there will be some conceptual overlap with personality and the well-being constructs not considered in this analysis. Further limitations include a lack of clinical diagnoses of depression and anxiety and the assumption for the causal direction of the influence of current PWB on SWB and mental health variables, due to the lack of prior data on some of the well-being measures at the prior wave. In addition, participants were drawn from two narrow age cohorts and these findings need to be extended to older age groups.
This study has supported recent findings that identify multi-dimensional models of well-being [25,27]. Furthermore, this study has shown that two cognitive PWB components explain a significant proportion of variance in SWB affect states, which are themselves significant drivers of mental health outcomes. In particular, the strong relationship between resilience and mastery with positive affect demonstrates that interventions to reduce depression and anxiety symptomology need to incorporate techniques that broaden and build cognitive PWB components that are more likely to increase levels of, and reduce reactivity in, positive affect. Consequently, we believe that the importance of PWB constructs lies in their capacity to decrease our vulnerability to negative mental health outcomes. Our findings suggest that rather than affecting depression and anxiety directly, PWB exerts an indirect effect on mental health symptoms through its role in reducing negative, and enhancing positive affective experiences.
Footnotes
Acknowledgements
We thank Trish Jacomb, Karen Maxwell, Helen Christensen, Andrew MacKinnon, Peter Butterworth and Simon Easteal and the PATH interviewers.