
Abstract
Objective:
There is limited Australian information on the prevalence and mental health consequences of bullying and ill-treatment at work. The aims of this study were to use data from an ongoing Australian longitudinal cohort study to (1) compare different measures of workplace bullying, (2) estimate the prevalence of bullying and ill-treatment at work, (3) evaluate whether workplace bullying is distinct from other adverse work characteristics and (4) examine the unique contribution of workplace bullying to common mental disorders in mid-life.
Method:
The sample comprised 1466 participants (52% women) aged 52–58 from wave four of the Personality and Total Health (PATH) through Life study. Workplace bullying was assessed by a single item of self-labelling measure of bullying and a 15-item scale of bullying-related behaviours experienced in the past 6 months. Factor analysis the identified underlying factor structure of the behavioural bullying scale.
Results:
Current bullying was reported by 7.0% of respondents, while 46.4% of respondents reported that they had been bullied at some point in their working life. Person-related and work-related bullying behaviours were more common than violence and intimidation. The multi-dimensional scale of bullying behaviours had greater concordance with a single item of self-labelled bullying (Area Under the Curve = 0.88) than other adverse work characteristics (all Area Under the Curves < 0.67). Self-labelled bullying and scales reflecting person-related and work-related bullying were independent predictors of depression and/or anxiety.
Conclusion:
This study provides unique information on the prevalence and mental health impacts of workplace bullying and ill-treatment in Australia. Workplace bullying is a relatively common experience, and is associated with increased risk of depression and anxiety. Greater attention to identifying and preventing bullying and ill-treatment in the workplace is warranted.
Introduction
Work is a central aspect of most adults’ lives and can have both a positive and negative influence on health and wellbeing. While work can provide identity, time structure and an overall sense of purpose in life, unmanageable work demands and work-related stress can lead to adverse health consequences (Siegrist and Theorell, 2006). Research has investigated a range of adverse psychosocial work characteristics, including job demands (related to the intensity and pace of work), job control (individual autonomy over skill use and decision making) (Karasek, 1979) and perceived job insecurity (D’Souza et al., 2003; Hartley et al., 1991). Other interpersonal aspects of work, such as social support from supervisors and colleagues, have largely been conceptualised as a potential resource which buffers the impact of excessive demands (Karasek et al., 1982). However, adverse interpersonal relationships at work may also undermine mental health. For example, workplace bullying is considered a potent workplace stressor that is associated with poor (mental) health outcomes (Hauge et al., 2010; Law et al., 2011).
Workplace bullying refers to repeated negative behaviour, mistreatment and/or abuse at work from others within the organisation (Einarsen et al., 2009). It is characterised by behaviour that harasses, offends, socially excludes or interferes with the job performance of victims. Definitions of workplace bullying often reference the persistence or duration of the bullying behaviour and the power imbalance (whether structural or social power) between the instigators and recipients (Einarsen et al., 2010; Lahelma et al., 2012). The 2012 Australian House of Representatives inquiry into workplace bullying recommended defining workplace bullying as ‘repeated, unreasonable behaviour directed towards a worker or group of workers, that creates a risk to health and safety’ (House of Representatives Standing Committee on Education and Employment, 2012). Related constructs such as workplace ‘mobbing’ or ‘harassment’ tap into similar behaviours but are less prescriptive about specific definitional elements such as duration and frequency (Hauge et al., 2010; Law et al., 2011; Leymann, 1996). We recognise, therefore, that some may prefer to label our measures as indicators of a broader construct of bullying and ill-treatment at work (Fevre et al., 2012).
Most prevalence studies have been conducted in the Nordic and Western European countries. A meta-analysis of lifetime prevalence estimates from predominantly European countries estimated that 14.6% of workers have experienced workplace bullying at some point (Nielsen et al., 2010). Data from the Australian Workplace Barometer (AWB) project show that 6.8% of Australian workers had experienced workplace bullying during the previous 6 months (Dollard et al., 2012). Workplace bullying is associated with increased sickness absence (Niedhammer et al., 2013) and reduced job satisfaction and job commitment (Askew et al., 2012). Research by Lahelma et al. (2012) found exposure to workplace bullying predicted mental health problems 5 to 7 years later. A recent meta-analytic review of longitudinal studies found that exposure to workplace bullying was significantly related to poor mental health, such that those who experienced bullying had 68% greater odds of subsequent poor mental health than those who had not experienced bullying (Nielsen et al., 2014). Again, the majority of studies included in this review (17 out of 25) were from Nordic countries. The research evidence also shows that workplace bullying is strongly associated with poor mental health, over and above the contribution of other psychosocial workplace stressors (Einarsen and Nielsen, 2015; Hauge et al., 2010; Lahelma et al., 2012), while Wilson (1991) has argued that bullying has greater consequences than all other work-related stressors combined.
Australian context
In recent years, there has been growing recognition in Australia of workplace bullying and its psychological impacts. In 2010, the Productivity Commission’s Review of psychosocial work hazards emphasised the substantial costs of workplace bullying (Productivity Commission, 2010), including both the personal costs to those who are bullied and the financial costs to employers resulting from absenteeism, presenteeism and staff turnover. Due to a lack of local Australian data, the review relied on international prevalence data to estimate the financial costs of workplace bullying in Australia. This amount was estimated to be between $6 and $36 billion annually, but did not include ancillary costs to the economy such as increased welfare and health expenditure. The Productivity Commission’s Report used workers’ compensation data to highlight the psychological impacts of workplace bullying in Australia. Workplace bullying and harassment are among the highest cost categories of mental health claims, and are associated with among the longest median time away from the workplace (Productivity Commission, 2010).
Both the Productivity Commission’s 2010 Report, and the report from the House of Representatives Standing Committee on Education and Employment (2012) on workplace bullying commented on the lack of population-based, Australian studies on workplace bullying. To date, Australian research has focussed largely on workplace bullying within single workplaces, with an emphasis on the medical workforce (e.g. Askew et al., 2012; Hutchinson et al., 2006; Rodwell and Demir, 2012). Despite the limited Australian research at the population-level, analysis of the AWB data show that 8.7% of depression in Australia is attributed to workplace bullying and job strain. This equates to $693 million in preventable lost productivity costs per annum (McTernan et al., 2013). One important limitation of the AWB project findings, acknowledged by McTernan and colleagues, is that a single subjective ‘self-labelling’ item was used to measure workplace bullying.
Measuring workplace bullying
Two methods have been used to assess bullying in the workplace. The self-labelling approach involves presenting a general definition of bullying and asking respondents to report if they have ever experienced such behaviour in the workplace over a specific time frame. This type of item has been used to produce estimates of the prevalence of workplace bullying. The behavioural or operational approach assesses the frequency of specific acts or behaviours, providing more nuanced and multi-dimensional data. It has been suggested that the self-labelling method may underestimate the incidence of bullying compared with a behavioural approach (Dick and Rayner, 2012). Conversely, the behavioural approach can never fully assess the constellation of behaviours and experiences which comprise workplace bullying. Because the self-labelling and behavioural approaches provide different information, some have advocated using both types of measures concurrently in workplace bullying research (Salin, 2001).
Aims
The aims of this study were:
To compare two methods of measuring bullying and ill-treatment at work: a self-labelling approach and a behavioural approach;
To estimate the prevalence of bullying and ill-treatment at work within an Australian context;
To consider the independence of workplace bullying from other aspects of psychosocial work environment (high demands, low job control, job insecurity); and
To evaluate whether bullying experiences at work are associated with increased risk of common mental disorders (depression and anxiety) above the contribution of other risk factors within and outside of the workplace.
Method
Participants and procedure
The Personality and Total Health (PATH) Through Life Project is a prospective community survey assessing the health and wellbeing of residents of Canberra and Queanbeyan (NSW) in Australia (Anstey et al., 2012). Three cohorts of participants (originally aged 20–24, 40–44 and 60–64 years) were randomly selected from the Canberra and Queanbeyan electoral roles in 1999, and have so far been interviewed on four occasions, each approximately 4 years apart. This study draws on data from the mid-aged cohort (40–44). At wave one, a total of 3919 people were selected and invited to participate in the mid-aged cohort, with 2404 (64.6%) agreeing to be interviewed. The current analyses consider data from the wave four interviews conducted in 2012 when cohort members were aged between 52 and 58 years. It was at this wave that measures assessing workplace bullying/ill-treatment at work were introduced. Overall, 2257 respondents remained in-scope for the wave four interview. Those who remained resident in the local region (n = 1615) were invited to participate in a face-to-face interview for the physical, cognitive and clinical assessment and to also complete the survey questionnaire online. Of these, 1570 (97%) participated in the survey. The remaining 626 individuals who had moved from the region were only invited to complete the online survey, with 236 (37%) participating. No baseline differences were evident (e.g. age, sex, education, employment, relationship status, mental health) between those who at wave four remained or had moved from the local area. As the current project draws on data from the online survey, the maximum sample size was 1806 (an overall response rate of 80%). Of these, 1466 respondents reported being ‘currently employed’, were asked the items assessing workplace bullying, and were therefore included in the current analyses.
The Human Research Ethics Committee of The Australian National University approved the PATH study and at each wave respondents provided written informed consent. Further details of the PATH project, including information on procedures to collaborate and access PATH data, are available in Anstey et al. (2012) or from the project website (http://crahw.anu.edu.au/research/projects).
Study measures
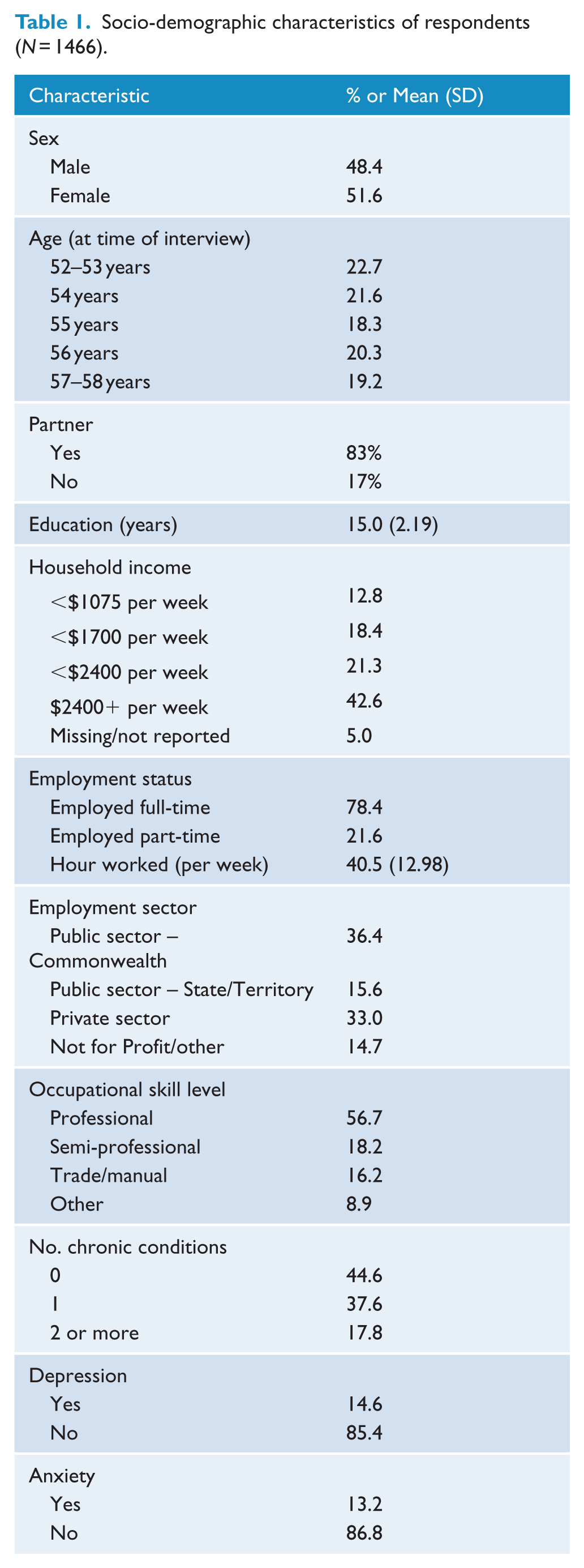
Socio-demographic factors included as covariates were as follows: sex, age, years of education, income, occupational skill level, employment sector (public, private or not-for-profit), employment status and weekly hours worked. Further details of how these covariates were coded are indicated in Table 1. Participants were asked about their experience of a range of chronic physical conditions, including epilepsy, asthma, bronchitis, emphysema, diabetes, thyroid problems, arthritis, Parkinson’s disease, heart problems, stroke, transient ischaemic attack (TIA) or cancer. These were coded into a summary variable representing the experience of none, one or two or more conditions. Negative affect has been previously linked to work stress and self-reported health and was assessed using the seven item Behavioural Inhibition Scale (BIS) (Carver and White, 1994).
Socio-demographic characteristics of respondents (N = 1466).
Bullying and ill-treatment at work was measured using two approaches. The self-labelling item noted ‘Mental violence or workplace bullying refers to isolation of a team member, underestimation of work performance, threatening, talking behind one’s back or other pressurising. Have you experienced such bullying?’ and possible responses were ‘Never’, ‘Yes, currently’, ‘Yes, previously in this workplace’, ‘Yes, previously in another workplace’, or ‘Cannot say’. This item has been used previously to estimate prevalence of workplace bullying (Kivimäki et al., 2000) and a broadly similar self-labelling item was used in the AWB project (Dollard et al., 2012). The behavioural approach presented a series of items and asked ‘How often have any of the following occurred to you in your workplace over the past 6 months? Choose the response closest to your experiences’. A series of 15 items were presented (based on a workplace bullying measure developed by Quine (1999)), each representing a negative behaviour that respondents may have experienced at work such as ‘Persistent attempts to belittle and undermine your work’ and ‘Being ignored or excluded’ (for a full list see Figure 1). Responses categories were as follows: ‘Never’, ‘A few times’, ‘Sometimes’ or ‘Often’. Further details about this scale are available elsewhere (Butterworth et al., 2013).
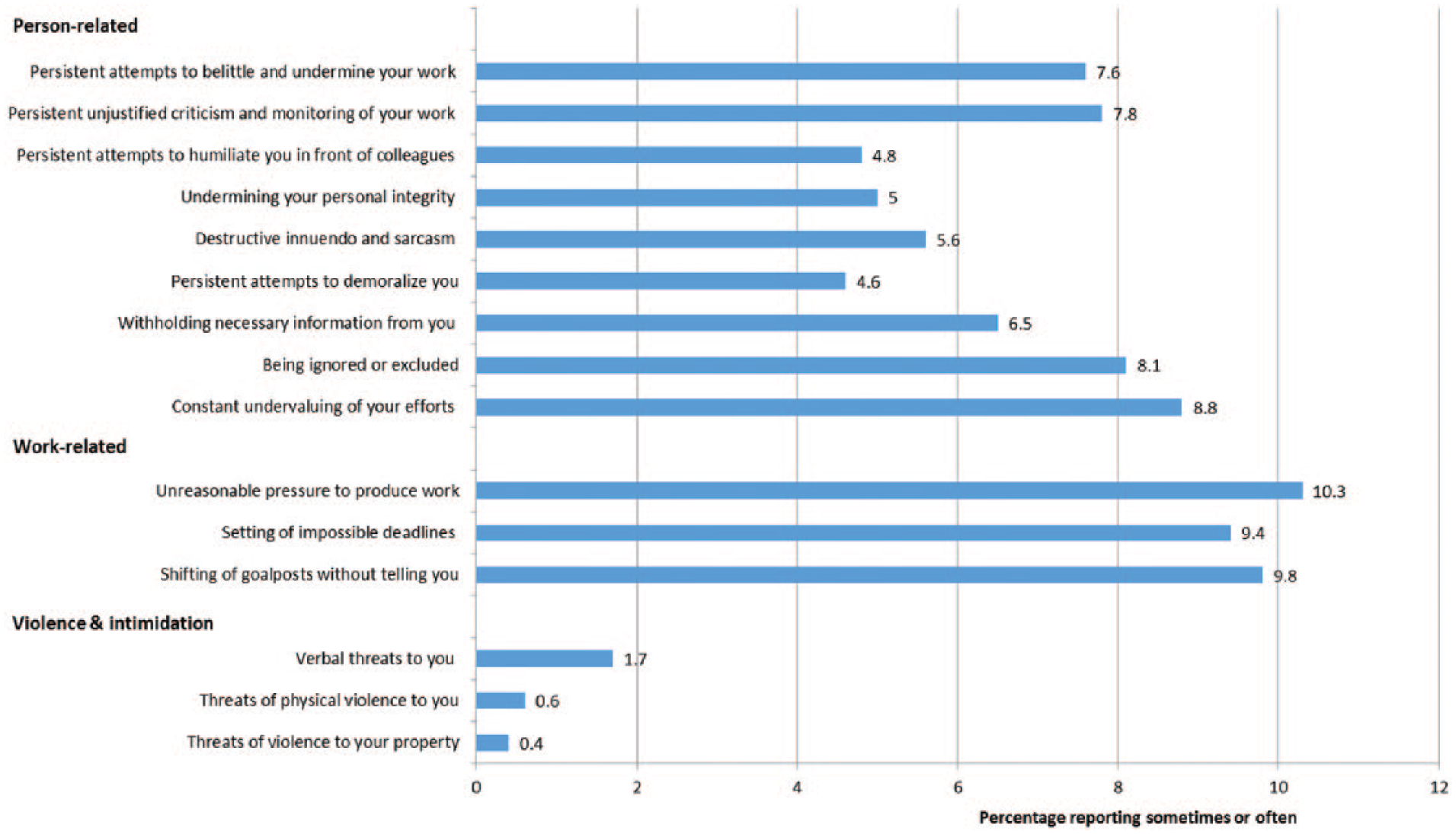
Workplace bullying/ill-treatment at work, factor structure and proportion reporting experiences (sometimes/often) in the past 6 months.
Psychosocial adversity at work was assessed using three well-established measures. Job control and job demands were assessed using 19 items taken from the Whitehall study (Bosma et al., 1997); four items assessed job demands, including ‘Do you have to work very fast?’ and 15 items assessed job control including skill discretion and decision authority such as ‘Others take decisions concerning my work’. Possible responses were as follows: ‘often’, ‘sometimes’, ‘rarely’ and ‘never’. Continuous scale scores for job demands and job control were created by summing the total scores of the relevant items. Following the methodology adopted by Leach et al. (2010) and Broom et al. (2006), these scales were categorised into binary measures with the tertile corresponding with greatest adversity (high job demands, low job control) categorised as high job adversity (‘1’ High and ‘0’ Low). Perceived job insecurity was measured by the question ‘How secure do you feel about your job or career future in your current workplace?’ Possible responses were ‘not at all secure’, ‘moderately secure’, ‘secure’ and ‘extremely secure’. Those who answered either ‘not at all’ or ‘moderately secure’ were categorised as having high job insecurity ‘1’, while the other categories represented low job insecurity ‘0’ (Leach et al., 2010).
Symptoms of generalised anxiety were assessed using the Goldberg Anxiety Scale (Goldberg et al., 1988). This scale comprised nine items assessing the presence of symptoms over the past month, resulting in a scale score of 0–9. A cut point of 7 was used to identify respondents with a probable anxiety disorder (Kiely and Butterworth, 2015). Likely current depressive disorder was identified using the Patient Health Questionnaire depression scale (PHQ) (Spitzer et al., 1999), a self-completion instrument measuring depression symptoms within the past two weeks and approximating the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) classification criteria. Respondents identified with major, minor or sub-syndromal depression according to the scoring protocols of the PHQ were classified with ‘depression’.
Statistical analyses
Descriptive statistics for the analysis sample were initially presented. The prevalence of current workplace bullying (using the self-labelling question) was calculated, in addition to the percentage of individuals exposed to specific bullying behaviours using the behavioural items. Exploratory factor analysis of the behavioural items, using a robust weighted least squares estimator and oblique rotation, was conducted in MPlus 7.3.1 to investigate the underlying factor structure. To evaluate whether the self-labelling item and behaviour items assessed the same underlying construct, and whether this was distinct from other types of adverse work experience, a series of four logistic regression models regressed a binary marker of (self-labelled) current bullying on (1) the three behavioural measures (latent constructs) of bullying, (2) job demands, (3) job control and (4) perceived job insecurity. Receiver Operating Characteristic (ROC) curves and Area Under the Curve (AUC) were used to evaluate and compare the fit of these four models. A series of simple logistic regression models were used to evaluate the socio-demographic profile of respondents who reported current workplace bullying. Finally, logistic regression models were used to assess whether workplace bullying was associated with current depression and anxiety. This included models assessing the univariate association (Model 1); adjusting for socio-demographic and occupational covariates (age, sex, years of education, occupational skill level, employment sector, physical functioning, income, employment status and hours worked; Model 2); adjusting for psychosocial job characteristics (high demands, low control, job insecurity; Model 3); and excluding respondents with either depression or anxiety at wave three (i.e. approximating the onset of depression/anxiety since the last measurement occasion). The final full sample models were repeated for each of the dimensional measures of bullying while sensitivity analyses included negative affect as a covariate to control potential response endogeneity. Cases with missing data were minimal (95.3% of respondents had no missing data on variables in the final model, with a further 3% having only one or two missing values) and excluded on an analysis-by-analysis basis (sequential modelling excluding cases with missing data in the final model).
Results
Sample characteristics
Table 1 presents the relevant socio-demographic characteristics of the sample. The data show that just over half the respondents were female, the majority was married or in a marriage-like relationship and that most respondents worked full-time, with a significant proportion working in the public sector (both Commonwealth and Territory/State Governments). The reported household income of respondents (median between $1700 and $2400 per week) is consistent with the national reported median income for adults aged 45 to 54 years, $1927 (Australian Bureau of Statistics [ABS], 2011–2012: Table 14)). The percentage of wave four respondents classified as depressed was 14.6% and 13.2% were identified with substantial anxiety symptoms.
Self-labelling item of workplace bullying
The prevalence of workplace bullying was estimated using the self-labelling item (see Table 2). Overall, 7.0% of respondents reported that they were currently experiencing bullying in their workplace. A further 16.6% of respondents reported that they had previously experienced bullying in their current workplace. Thus, in total, 23.6% of respondents had experienced workplace bullying at some time in their current workplace. A further 22.8% of respondents reported an experience of bullying in a previous workplace. Therefore, 46.4% of respondents reported some experience of workplace bullying during their working lives.
Reported workplace bullying using self-labelling approach.
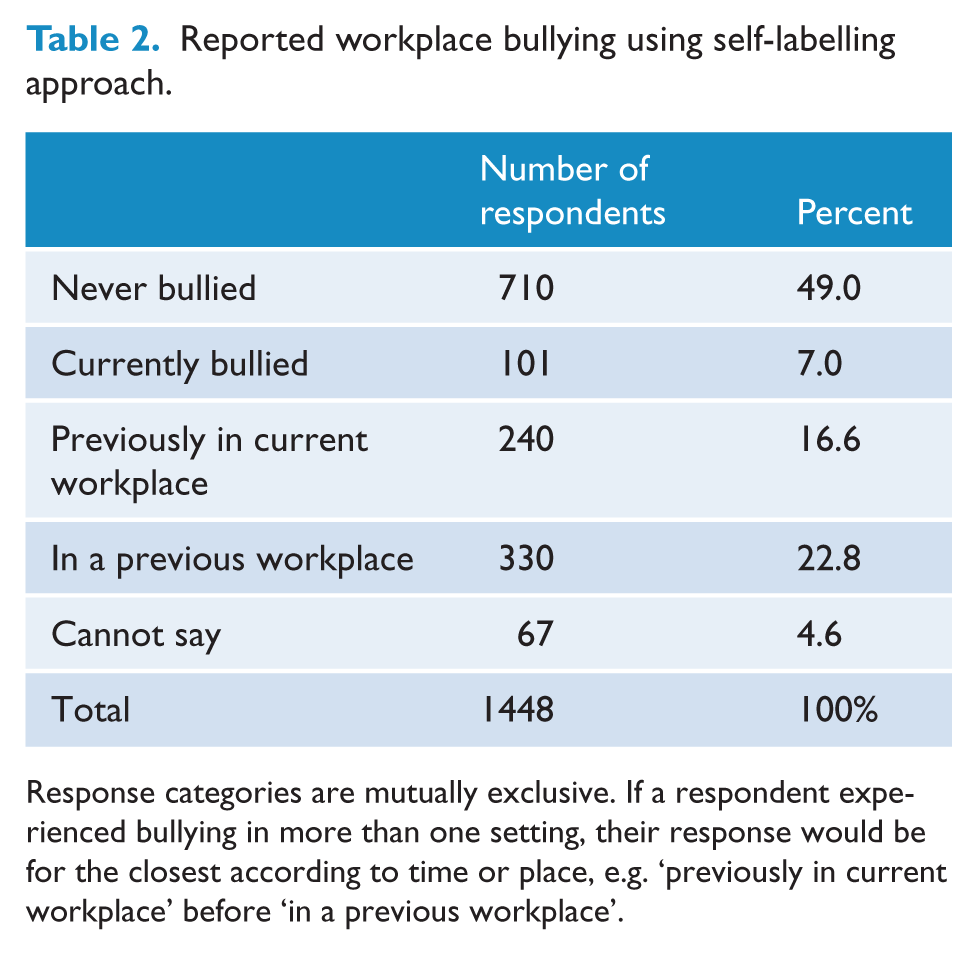
Response categories are mutually exclusive. If a respondent experienced bullying in more than one setting, their response would be for the closest according to time or place, e.g. ‘previously in current workplace’ before ‘in a previous workplace’.
Behavioural items of workplace bullying
Exploratory factor analysis of the set of ‘behavioural’ items supported a three latent factor solution. While the first factor showed a very large eigenvalue (9.9), the first three eigenvalues were each greater than one and substantially larger than the fourth eigenvalue. The three-factor solution was the first to demonstrate consistent adequate model fit (root mean square error of approximation (RMSEA) = 0.047; comparative fit index (CFI) = 0.994; Tucker–Lewis Index (TLI) = 0.990; standardised root mean square residual (SRMR) = 0.041). On the basis of the items loading on each factor, we labelled the three factors as person-related bullying, work-related bullying and violence or intimidating behaviour (See Figure 1). The factors were statistically equivalent to scales constructed by simply summing the relevant items, with Cronbach’s alphas for the three bullying scales being 0.92 (person-related), 0.88 (work-related) and 0.74 (violence and intimidation). Figure 1 shows the prevalence of each of the individual workplace bullying behaviours reported ‘sometimes’ or ‘often’ to reflect the persistent nature of bullying. The figure shows that work-related bullying experiences were more common than other forms of bullying, with physical threats and intimidation the least frequently experienced workplace-bullying behaviours.
Convergence and divergence among measures of adverse work experiences
The next series of analyses assessed whether the different measures of workplace bullying were associated with each other, and distinct from other types of adverse work experiences. There was a strong association between each of the behavioural measures and the (self-labelled) binary indicator of current workplace bullying (Person-related bullying odds ratio [OR] = 6.30, 95% confidence interval [CI] = [4.64, 8.55]; Work-related bullying OR = 2.46, 95% CI = [1.97, 3.08]; Violence and intimidation OR = 3.34, 95% CI = [1.79, 6.23]). While significant, current bullying was less strongly associated with (continuous measures of) the other adverse psychosocial work characteristics (increasing job demands OR = 1.19, 95% CI = [1.09, 1.31]; decreasing job control OR = 1.08, 95% CI = [1.05, 1.11]; and increasing job insecurity OR = 1.61, 95% CI = [1.29, 2.00]). The ROC for the model comprising the three behavioural measures of workplace bullying/ill-treatment showed an AUC of 0.88, indicative of a good/excellent fit (see Figure 2). In contrast, the AUC for each of the other models based on measures of psychosocial work characteristics ranged between 0.60 (demands and insecurity) and 0.67 (job control) (see Figure 2).
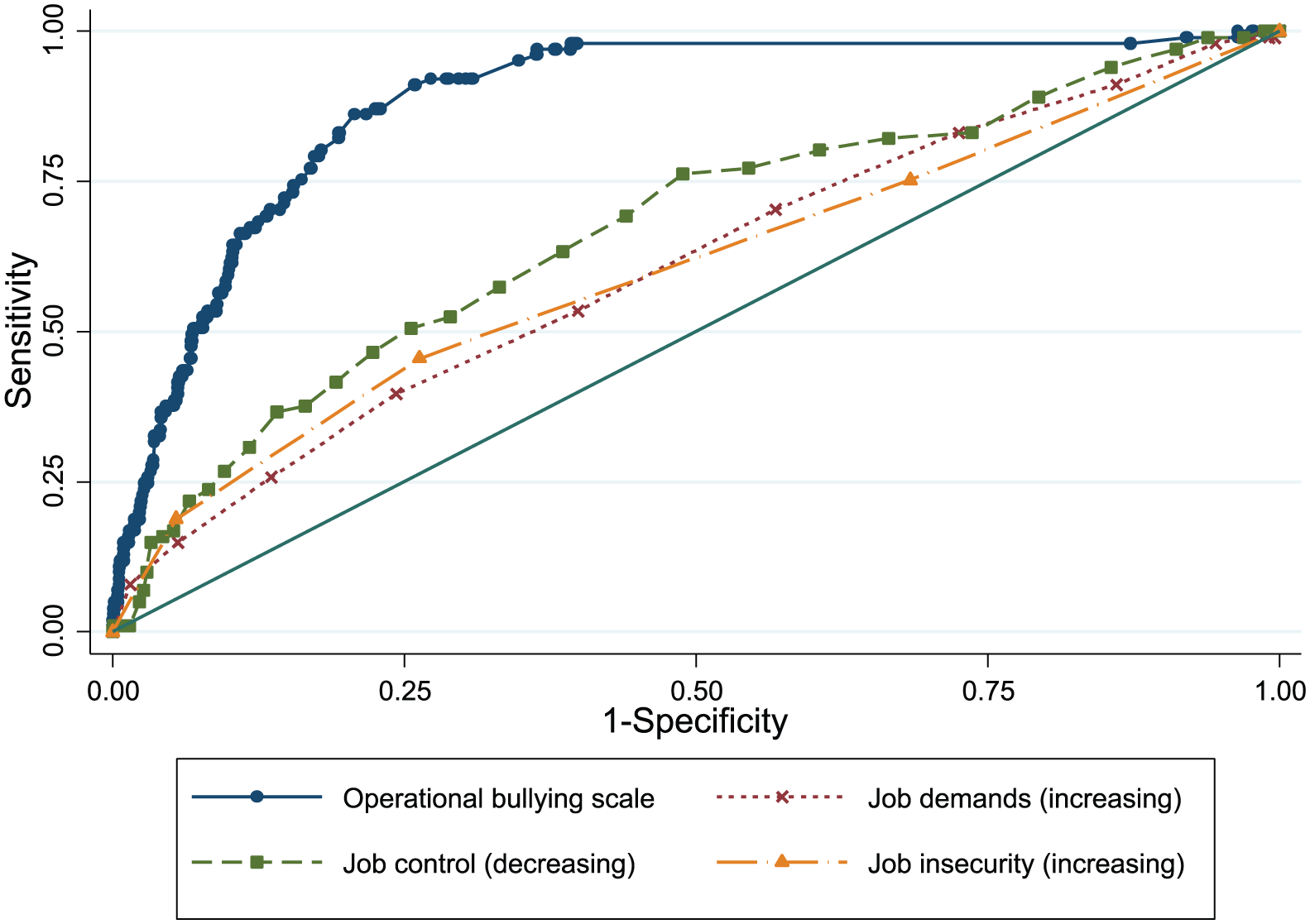
Receiver Operating Characteristic (ROC) curves comparing the measure of overall bullying experiences with other psychosocial job characteristics.
The profile of workplace bullying
A series of simple logistic regression models considered the socio-demographic correlates of bullying in the current organisation. The results showed women reported higher rates of bullying than men (OR = 1.44, 95% CI = [1.13, 1.84]), and that those with a partner reported lower rates of bullying than those without a partner (OR = 0.71, 95% CI = [0.53, 0.98]). Compared with those in the Commonwealth public sector, State/Territory government employees reported higher rates of bullying (OR = 1.45, 95% CI = [1.06, 2.06]). However, Commonwealth government employees reported higher rates of bullying in comparison with private sector employees (OR = 1.97, 95% CI = [1.44, 2.70]) and comparable with respondents employed in the not-for-profit sector (OR = 0.73, 95% CI = [0.50, 1.07]). Compared with those employed in trade or manual occupations, higher rates of bullying were reported by those in professional (OR = 1.76, 95% CI = [1.20, 2.58]) or semi-professional occupations (OR = 1.63, 95% CI = [1.04, 2.56]). There was no difference in reported bullying across levels of income or educational attainment.
Associations between workplace bullying and mental health
Table 3 (top panel) shows the results from the logistic regression models examining the association between workplace bullying and depression. Compared with those who reported no history of bullying, current bullying was associated with significantly increased risk of depression, even after controlling for socio-demographic and other contemporaneous workplace adversities. The full multivariate Model 3 correctly classified 86% of respondents. Using the median or most common category of each covariate as the reference, this model estimated that 15.3% of those who reported current bullying were depressed compared with 6.3% of those with no history of bullying. The final model, restricted to respondents not identified with depression at the previous wave (n = 1268; 10.0% with wave four depression), also demonstrated a consistent pattern of results. The bottom panel of Table 3 shows the association between workplace bullying/ill-treatment and anxiety. Current bullying was associated with increased likelihood of anxiety in all models, including when controlling for socio-demographic and workplace covariates. Model 3 correctly classified 87% of respondents and, for those currently bullied, the estimated prevalence of anxiety was 13.0% compared with 5.3% for those with no history of being bullying. The final model which excluded those identified with anxiety at the previous wave (n = 1231; 7.9% identified with anxiety at wave four) again confirmed the association between current workplace bullying and current anxiety. Analysis of the dimensions of workplace bullying showed that person-related and work-related bullying were each associated with increased odds of depression and anxiety, while the less common ‘violence and intimidation’ measure showed an association in the same direction but did not reach statistical significance (see Table 4). Finally, sensitivity analyses which included a measure of negative affect produced the same pattern of results (results not presented).
Odds of depression and anxiety in association with the ‘self-labelling’ item of workplace bullying.
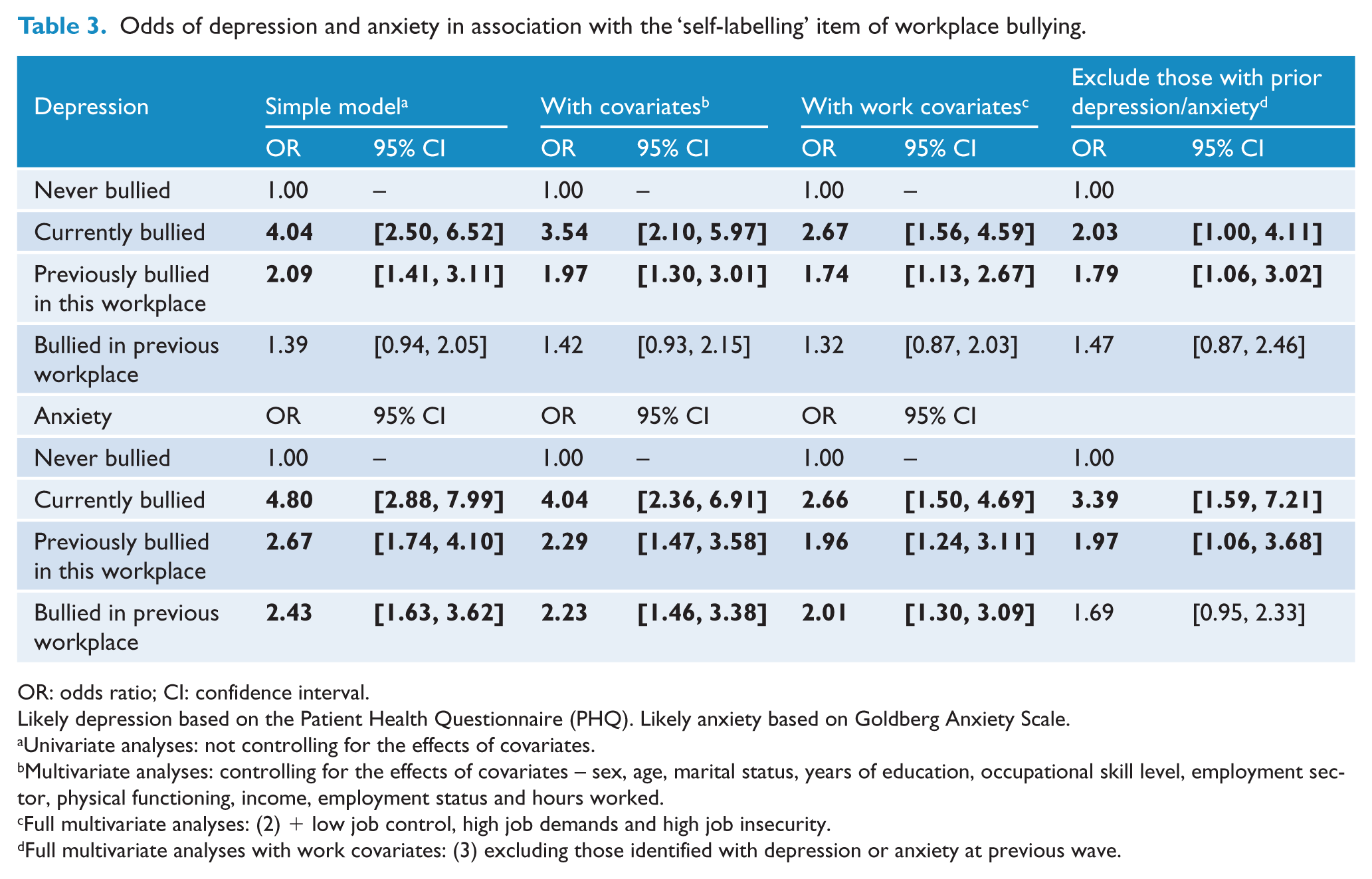
OR: odds ratio; CI: confidence interval.
Likely depression based on the Patient Health Questionnaire (PHQ). Likely anxiety based on Goldberg Anxiety Scale.
Univariate analyses: not controlling for the effects of covariates.
Multivariate analyses: controlling for the effects of covariates – sex, age, marital status, years of education, occupational skill level, employment sector, physical functioning, income, employment status and hours worked.
Full multivariate analyses: (2) + low job control, high job demands and high job insecurity.
Full multivariate analyses with work covariates: (3) excluding those identified with depression or anxiety at previous wave.
Odds of depression and anxiety associated with each dimensional measure of workplace bullying.
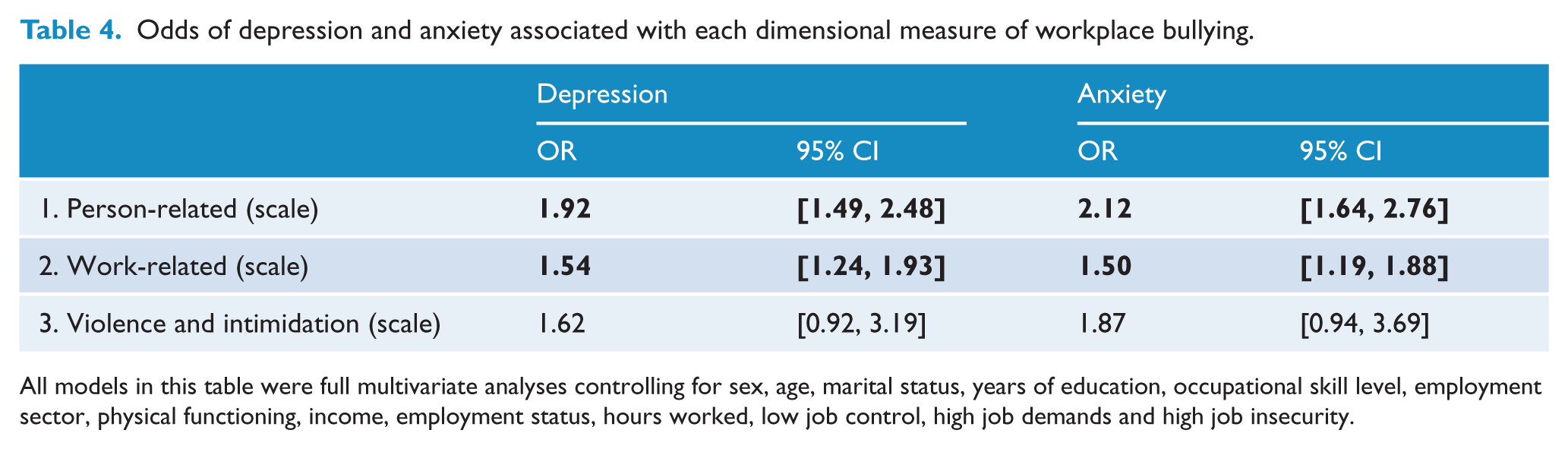
All models in this table were full multivariate analyses controlling for sex, age, marital status, years of education, occupational skill level, employment sector, physical functioning, income, employment status, hours worked, low job control, high job demands and high job insecurity.
Discussion
This study found that workplace bullying and ill-treatment at work was common in Australia, with 7% of respondents reporting they were currently experiencing bullying, and 46% indicating they had been bullied at some point in their working life. The most frequent types of workplace bullying and ill-treatment were personal and work-related experiences, whereas violence and intimidation was less common. The validity of both the self-labelling and the behavioural approach to measuring workplace bullying was confirmed, as the measures representing both approaches were highly correlated and found to be distinct from other adverse work characteristics (high demands, low control, high insecurity). Workplace bullying was significantly associated with 2–3 times greater odds of depression and anxiety for those currently bullied, even after accounting for other risk factors within and outside of the workplace and when analysis was restricted to respondents not identified with mental illness at the previous measurement occasion.
The current findings are consistent with other studies estimating the prevalence of workplace bullying and its association with poor mental health. For example, longitudinal research conducted in Finland with municipal employees aged 40–60 years found that 5% of workers were currently being bullied, and that 5 to 7 years later, these workers were 1.5 to 2 times more likely to have a probable anxiety or depressive disorder than those who had never been bullied (Lahelma et al., 2012). Similarly, a study conducted by Einarsen and Nielsen (2015) in Norway found that 4.6% of respondents reported bullying at baseline, and that this group remained at greater risk of poor mental health 5 years later. Like this study, findings from Northern European research show that while workplace bullying is associated with both depression and anxiety, the strength of the association is greater for anxiety (Einarsen and Nielsen, 2015; Lahelma et al., 2012).
There are two alternative explanations of the association between workplace bullying and poor mental health: (1) that individuals with poor mental health (or a negative personality bias) are more likely to be victimised (reverse-causality) and (2) that other adverse characteristics of work (e.g. a generally stressful work environment), associated with both perceived victimisation and poor mental health, explain the association. The current findings go some way to exclude these alternative hypotheses. The results showed that the association between current workplace bullying and current mental health was evident among those without prior mental health problems, and that the association was not explained by negative affect. Other studies have explicitly tested whether baseline mental health and/or specific personality traits predict subsequent exposure to bullying with mixed findings (Einarsen and Nielsen, 2015; Finne et al., 2011; Nielsen and Knardahl, 2015; Rugulies et al., 2012). The findings from the ROC and AUC analyses in this study (Figure 2) suggest that the self-labelling measure of workplace bullying is strongly associated with behavioural measures of bullying and ill-treatment at work, but more weakly associated and distinct from other adverse job characteristics (job demands, job control, job insecurity). Likewise, the findings from this study and some others (e.g. Einarsen and Nielsen, 2015; Lahelma et al., 2012) show that there is a strong independent association between exposure to bullying and poor mental health after adjusting for other aspects of work. We did not find, as some have claimed (Wilson, 1991), that bullying was as potent a stressor as all other job adversities combined, but bullying and personal- and work-related ill-treatment remained significant independent predictors of both depression and anxiety.
Implications
The current findings highlight the need for further strategies and policies to prevent workplace bullying, and the need to support those who experience bullying. While workplace bullying is now widely recognised as a problem for organisations and communities in Australia, and Australian laws acknowledge workplace bullying as a work health and safety issue, there are many difficulties with enforcing codes of practice (Dollard et al., 2012; Johnstone et al., 2011). There is little incentive to report workplace bullying when there is no clear pathway to resolve disputes and those who report bullying risk further victimisation and loss of career opportunities. Potential interventions to reduce workplace bullying include better training and resources to ensure staff and supervisors understand what constitutes workplace bullying and its likely consequences. Policies outlining how to make complaints about workplace bullying and having a designated person responsible for managing complaints may reduce the incidence of bullying and the negative consequences (Hogh et al., 2010). The final report of the 2012 House of Representatives inquiry into workplace bullying produced a detailed set of recommendations of potential strategies to reduce and better manage the consequences of bullying at work.
The study found greater rates of bullying for respondents employed in the public sector: a finding consistent with workers’ compensation data (Safe Work Australia, 2012). It may be that greater awareness and recognition of workplace bullying may explain this difference, but further research is needed. Evidence that respondents employed by State/Territory governments reported greater rates of bullying than their Commonwealth colleagues is not consistent with other reports (Victorian Public Sector Commission, 2015) and also requires further consideration. While we have focussed our attention on current bullying, it is also important to recognise that the data in Table 2 show that almost two-thirds of bullying or ill-treatment experienced by respondents within their current workplace had resolved (i.e. respondents reported prior but not current bullying). This may be a positive finding illustrating the resolution or addressing of workplace conflicts, or it could reflect the departure of the perpetrator from the workplace. It does illustrate how little we know about the course of bullying over time, the dearth of longitudinal research and the need for further study of patterns of variability and persistence in workplace bullying over time.
Limitations
This study has several limitations which should be acknowledged. First, although the PATH 40s cohort is representative of the population from which it was recruited (Canberra and Queanbeyan, Australia; Anstey et al., 2012), this region is not necessarily representative of the broader Australian population. Canberra residents have higher rates of labour force participation and employment than the national average (ABS, 2008). ABS census data shows that the workforce in Canberra/Queanbeyan has almost 50% more professionals and lower rates of persons employed in sales, machinery operators/driver & labourers than the overall Australian population (ABS, 2006). While previous research suggests workplace bullying may be more prevalent in unskilled occupations (Ortega et al., 2009), the current findings showed bullying and ill-treatment at work were most common among professional and semi-professional occupations. This is consistent with recent workers’ compensation data (Safe Work Australia, 2015). A further limitation is that the sample reports high levels of educational attainment which may influence generalizability to other populations. The measures of workplace bullying and mental health were self-reported, and may not be equivalent to objective measures of workplace bullying/ill-treatment at work or diagnostic measures of mental disorders. As such, response-bias or endogeneity may play a role in the associations observed between workplace bullying and depression/anxiety, though this possibility was minimised by including negative affect as a covariate. The self-report and behavioural measures of bullying did not assess duration of workplace bullying. Some definitions of workplace bullying emphasise the persistent and ongoing nature of the ill-treatment. This is not only a potential operational limitation, but may limit the strength of association between bullying and mental health in this study. Some research suggests that longer duration of exposure to bullying is associated with higher levels of psychological distress (Figueiredo-Ferraz et al., 2015). This study, although drawn from a longitudinal cohort study, considered the contemporaneous association between workplace bullying and mental health as the bullying measures were only included in the most recent measurement occasion. Finally, the small number of respondents indicating that they had experienced violence or intimidation within their workplace may have limited power to detect an association with depression and anxiety.
Despite these limitations, this study has a number of strengths. Research including both self-report and behavioural measures of workplace bullying and ill-treatment is rare, and enabled unique converging evidence. The longitudinal data enabled analysis excluding individuals with prior mental health problems, increasing our confidence that the association evident between workplace bullying and mental health did not reflect reverse causation. Finally, the current paper assessed the association between workplace bullying and both depression and anxiety.
Conclusion
This study is one of the few Australian studies to estimate the prevalence of workplace bullying and investigate the association of bullying and ill-treatment at work with depression and anxiety. The findings show that bullying significantly increases the likelihood of experiencing depression and/or anxiety. The brief measures of bullying included in the PATH study (both the self-labelling and behaviour approach) may have utility in workplace assessment and screening. More needs to be done in the Australian context to identify effective interventions to reduce workplace bullying and the associated negative impacts on mental health. The House of Representatives workplace bullying inquiry noted that most targets of bullying were not necessarily concerned about formal grievance or disciplinary processes, but simply wanted the behaviour to stop (House of Representatives Standing Committee on Education and Employment, 2012). This study provides some insight into the mental health experiences and distress experienced by bullied individuals, and provides population-level data about why it is important to continue efforts to stop workplace bullying.
Footnotes
Acknowledgements
We thank the study participants, PATH Interviewers, Trish Jacomb and Karen Maxwell. We would also like to acknowledge the contribution of other PATH Investigators: K Anstey, H Christensen, A MacKinnon, S Easteal and N Cherbuin.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Health and Medical Research Council project grant #1002160, funding from Safe Work Australia, Australian Research Council (ARC) Future Fellowship #FT13101444, National Health and Medical Research Council (NHMRC) Early Career Fellowship #1035803, and Alzheimer’s Australia Dementia Research Foundation (AADRF) Fellowship #DGP13F00005.