
Abstract
Risk of suicide attempt (SA), suicidal ideation (SI) and deliberate self-harm (DSH) is high among young people with annual prevalence rates of DSH reported as being as high as 7.3% and lifetime rates of between 12–13% [1–3]. SI is more common with as many as 60% of adolescents in the USA reporting having experienced SI on at least one occasion [1]. Previous suicidal or self-harming behaviours are not only problematic in their own right but are key risk factors for future suicide [2,3]; however, limited evidence exists regarding interventions to reduce this risk [4], particularly that from randomized controlled trials (RCTs) [5]. Further, interventions that are effective among adults may not necessarily be applicable to young people, and RCTs testing interventions among this group are fewer still.
Research into the efficacy of interventions for young people at risk is hampered by a range of factors, not least small sample sizes, varying definitions of suicidality and DSH, and the fact that in many cases young people at risk are excluded from trials for safety reasons [6]. Hence the aim of this study was to conduct a systematic review and meta-analysis of all RCTs testing interventions for young people who have presented to a clinical setting with a recent history of SI, SA, and/or DSH.
Method
The Cochrane Collaboration systematic review methodology was used as outlined in the Cochrane Handbook for systematic reviews of interventions [7].
Search strategy
Systematic bibliographic searches were performed to find relevant trials from the following databases: the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase and PsycINFO with each database being searched from 1980 to June 2010. The following keywords were used to form the basis of the search strategy: ‘self-injurious behaviour’, ‘attempted suicide’, ‘suicide’, ‘suicidal behaviour’, ‘self-inflicted wounds’, ‘self-mutilation’, ‘self-harm’ (contact authors for full search strategy). We also hand searched conference abstracts from the two major international suicide prevention conferences, namely the International Association for Suicide Prevention World Congress and the European Symposium for Suicide Prevention from the years 2003 to 2009. Further papers were found by hand-searching the references of all retrieved articles and previous reviews.
Study selection
Published and unpublished English language RCTs of any psychological or therapeutic intervention for the management of suicide risk and DSH, where intent was not specified, were considered for inclusion. Studies specifically of non-suicidal self-injury were not included. Study participants had to be between 12 and 25 years old. Alternatively, if the age range for the study included people aged 12 to 25 and the mean age of participants fell within this range the studies were included. Study participants also had to have presented to a clinical service with suicide related behaviours including SI, SA or DSH within the 6 months prior to study entry. We included studies where treatment for suicidality occurred in the context of a primary mental health disorder, but not studies that were primarily examining treatment for a mental health disorder whereby some, but not all, participants had experienced suicidality. Studies where interventions were aimed at the clinicians (rather than the young person) were included when the clinicians were working with young people at risk (e.g. practitioner awareness), but not where they were working with young people in general (e.g. gatekeeper, school counsellor programmes etc.).
The primary outcome was considered to be suicide-related behaviours including suicide, SA, DSH, or SI.
Two reviewers (J.R. and C.M.) independently assessed all potentially relevant articles for inclusion. Any disagreements about inclusion were resolved by discussion with a third review author (S.H.).
Assessment of risk of bias
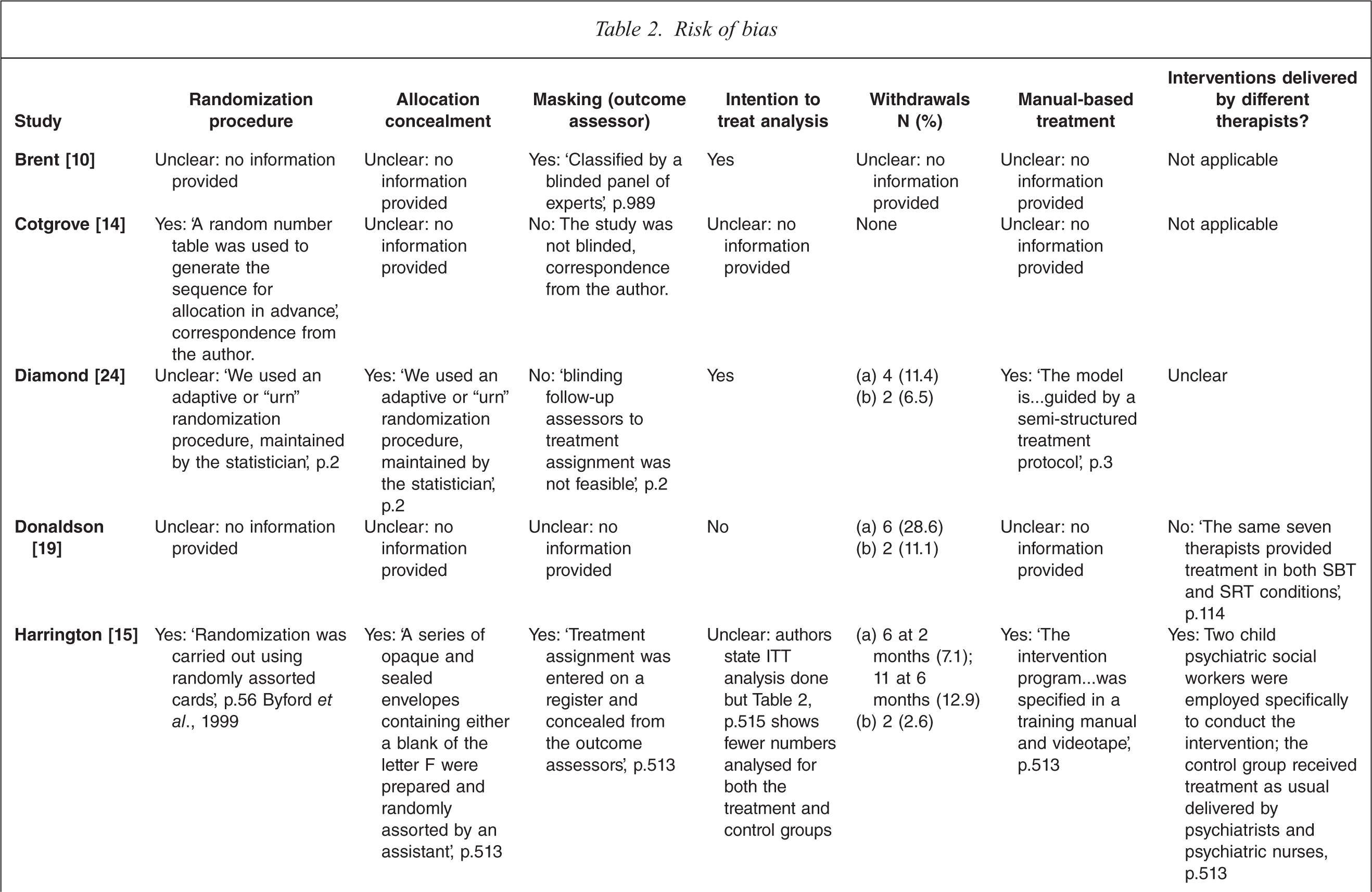
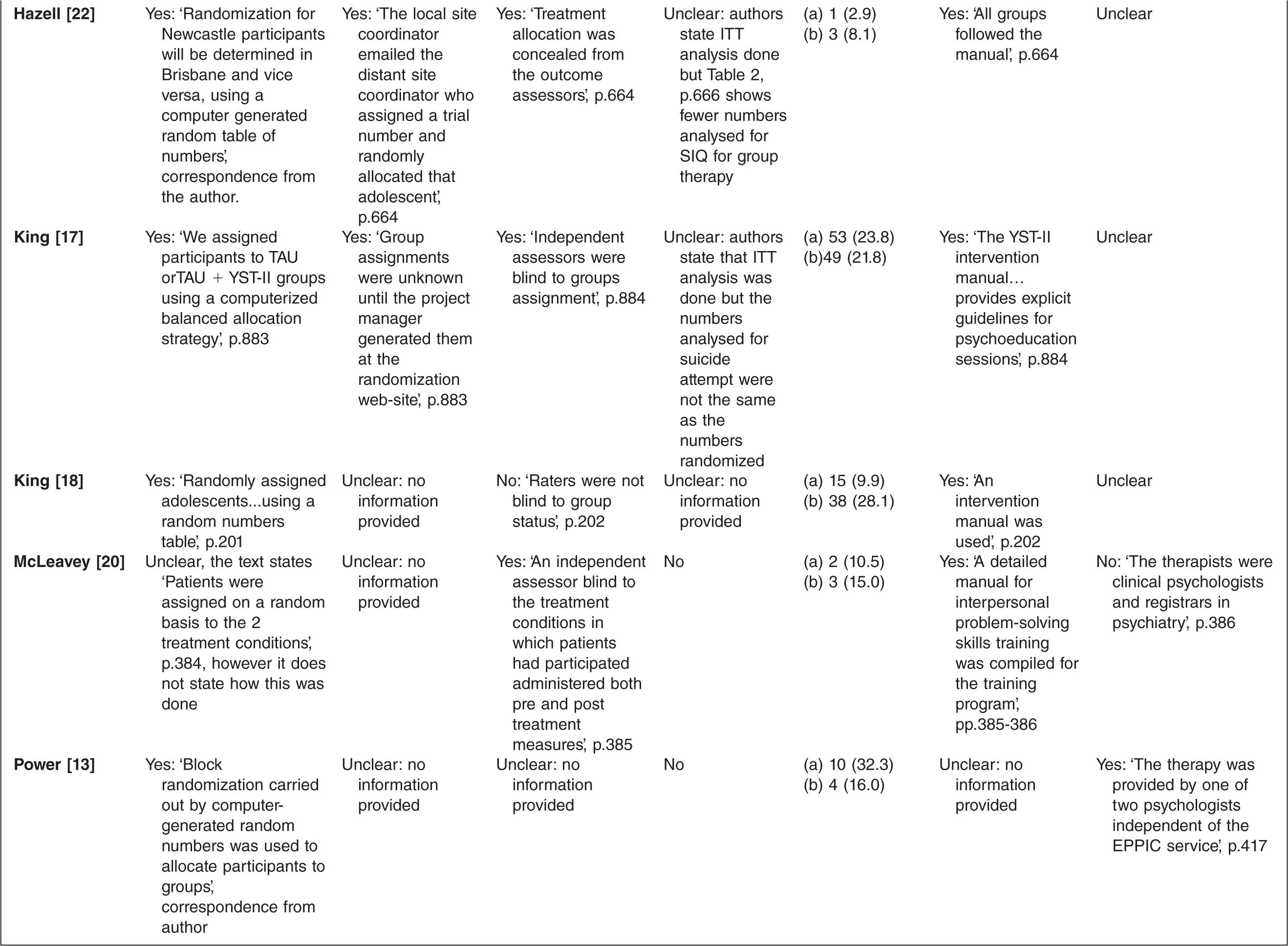
Trials were assessed for risk of bias according to the Cochrane Handbook [7]. Specifically, assessment was made of the conduct of the trial with regard to random sequence generation, allocation concealment, blinded assessment of outcomes, whether the number and reasons for drop out were reported and if intent-to-treat (ITT) analysis was done, and selective reporting bias in terms of whether the results and/or data for review outcomes of relevance were reported. Two review authors (J.R. and S.H.) independently carried out this assessment of the risk of bias, with any disagreement resolved by discussion.
Statistical analysis
When appropriate, meta-analysis was performed and pooled effect estimates obtained, using the meta-analytic standard software used by the Cochrane Collaboration, Review Manager statistical software program [8].
For dichotomous outcomes, such as reduction in the proportion of participants with SAs, the risk ratio (RR) was estimated. For continuous outcomes, such as severity of SI, if absolute values of post-treatment means and standard deviations (SD) were given using the same rating scale across trials, these were used to calculate the mean difference (MD). If different scales were used to measure the same outcomes, the standardized mean difference (SMD) was calculated.
For all meta-analyses we used the random effects model with a 95% confidence interval. Random effects are, in general, more conservative than fixed-effects models because they take heterogeneity among studies into account. With decreasing heterogeneity the random effects approach moves asymptotically towards a fixed-effects model.
Heterogeneity was assessed on the basis of the Cochrane Handbook's recommendations [7] (I2 values of 0–40%: might not be important; 30% to 60%: may represent moderate heterogeneity; 50% to 90%: may represent substantial heterogeneity; 75% to 100%: considerable heterogeneity). Because the importance of the observed I2 depends on (i) magnitude and direction of effects and (ii) strength of evidence for heterogeneity, in addition to the I2 value [9] we have presented the χ2 and its p-value and have considered the direction and magnitude of the treatment effects. Because χ2 test is underpowered to detect heterogeneity in meta-analysis that includes only a few studies, a p-value of 0.01 was used as a threshold of statistical significance. If statistical heterogeneity existed we had planned to examine it by subgroup and sensitivity analyses.
Analysis of subgroups by presentation in terms of presence of primary mental health disorder diagnosis, risk characteristic at entry to the study (SI, SA, DSH), and age (12–18, 18–25) was planned. However, there were too few studies to carry out subgroup analysis on age and risk characteristic.
Sensitivity analyses were performed to assess the robustness of the findings to the exclusion of the lowest quality trials, i.e. trials where allocation concealment was not undertaken or was not clearly stated to have been undertaken, and trials where there was more than a 50% drop out rate.
Results
Description of studies
In total, 4886 articles were retrieved via the search of electronic databases. Of these 4687 were excluded on the basis of title and abstract. A total of 199 full text articles were retrieved for closer examination, of which 187 were excluded. A further seven articles were identified via two of the clinical trials registers (clinicaltrials.gov and the Australian New Zealand Clinical Trials Registry) and four from conference proceedings. Of these 23, we were unable to determine the eligibility for inclusion of two studies despite contact with authors, co-authors or their departments. Of the 21 included studies, 15 have been published and 6 are classed as ongoing.
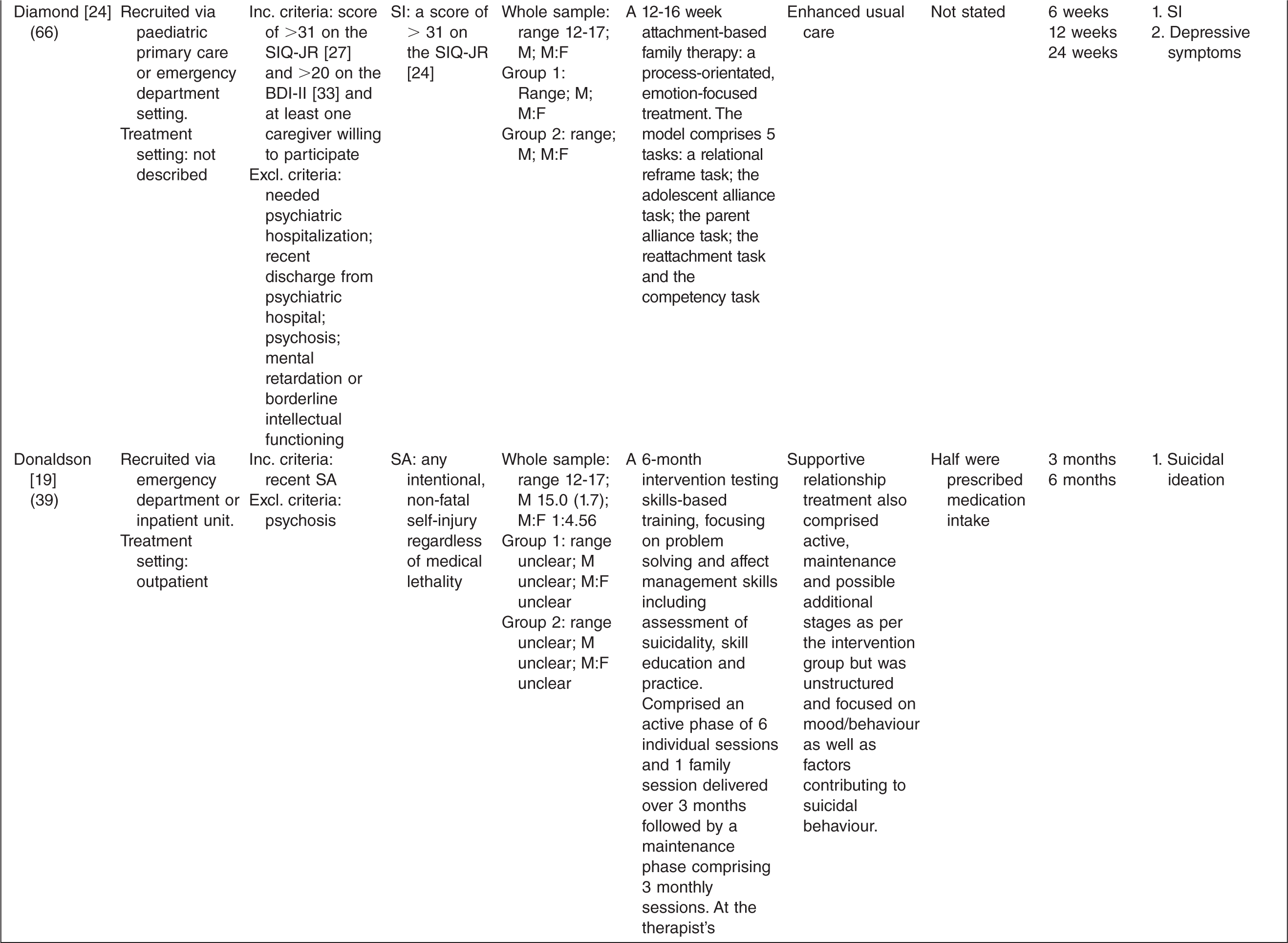
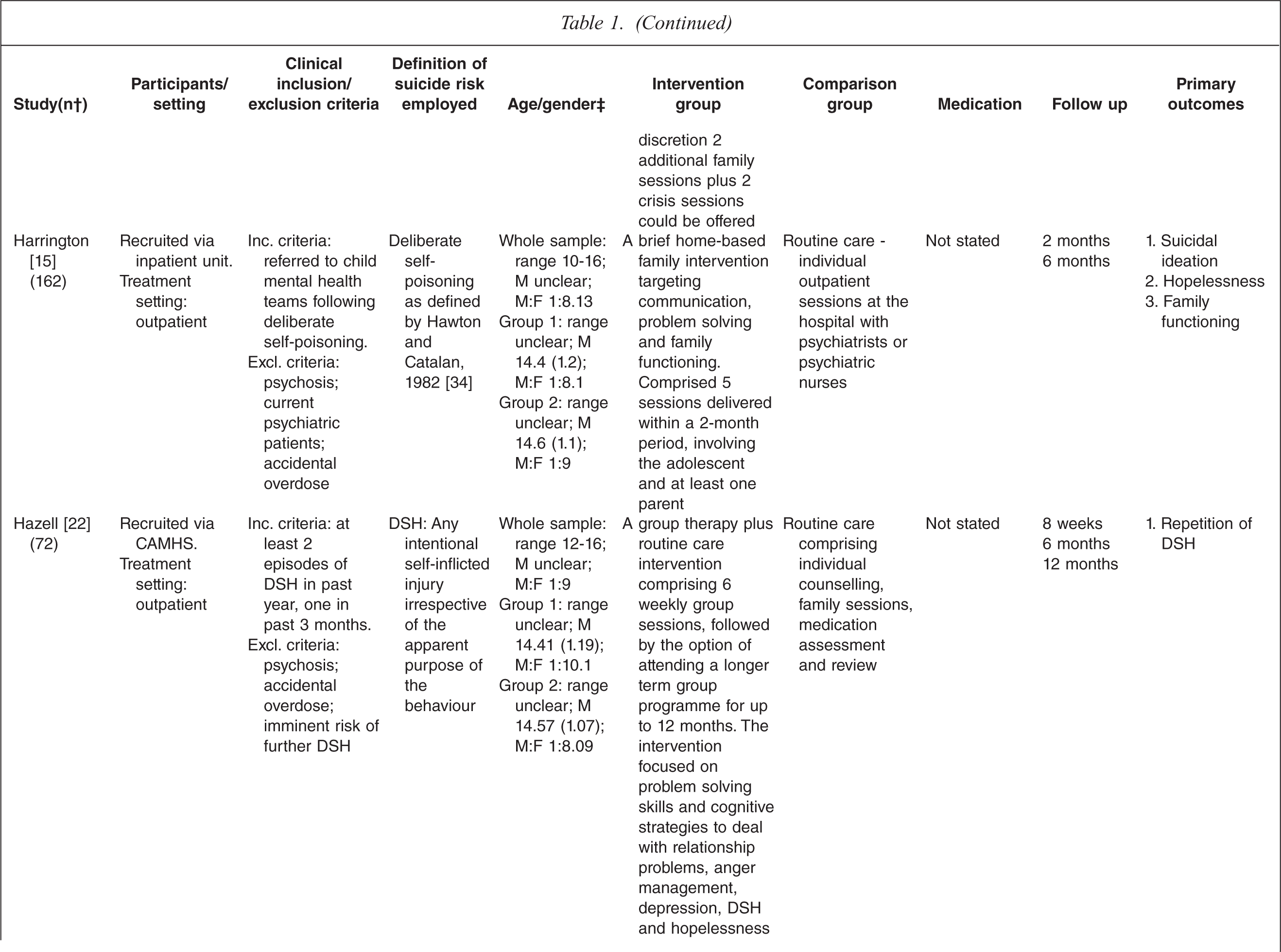
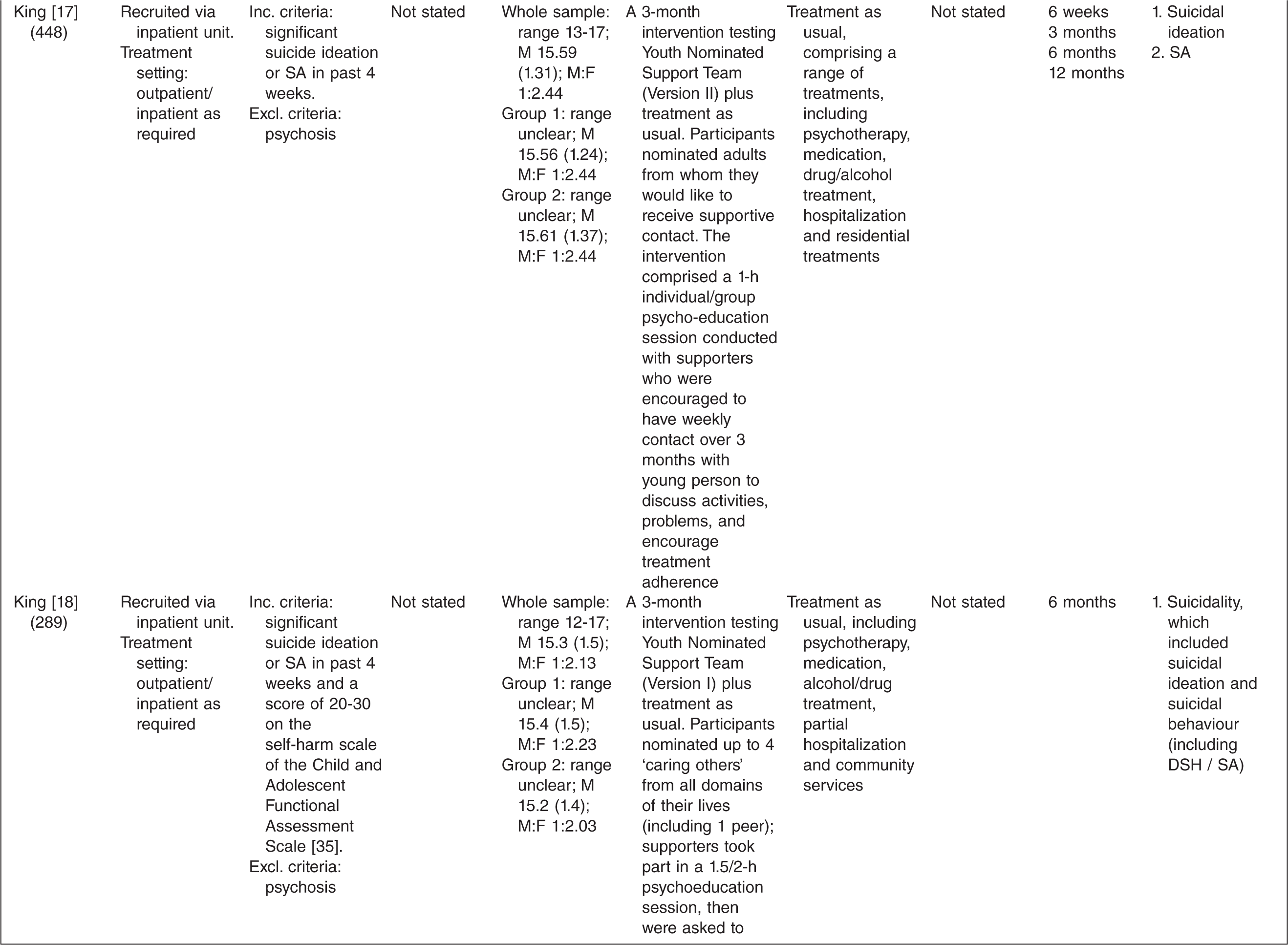
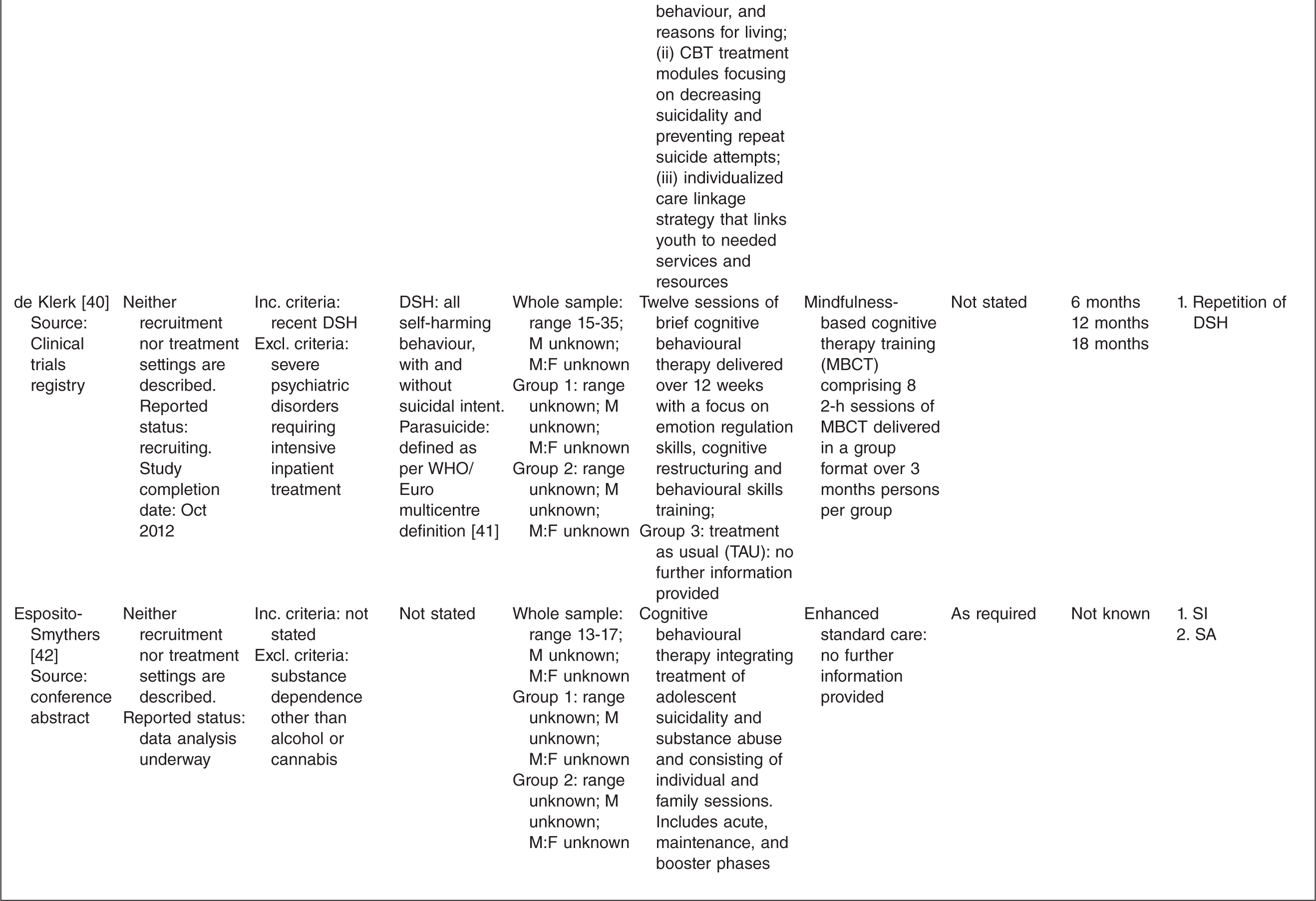
As per our inclusion criteria, all included studies were RCTs targeting adolescents or young adults who had presented to clinical services with suicide risk. The majority of studies recruited young people from inpatient or community mental health services following a SA or presentation for DSH and most interventions were delivered in an outpatient setting. Of the 15 published studies, two specifically targeted young people with mood disorders [10,11], one targeted young people with borderline personality disorder [12] and one study targeted young people with a psychotic disorder [13]. In contrast, many of the studies specifically excluded those with severe psychiatric diagnoses (see Table 1).
Characteristics of randomized controlled trials for suicidality in young people presenting to clinical services
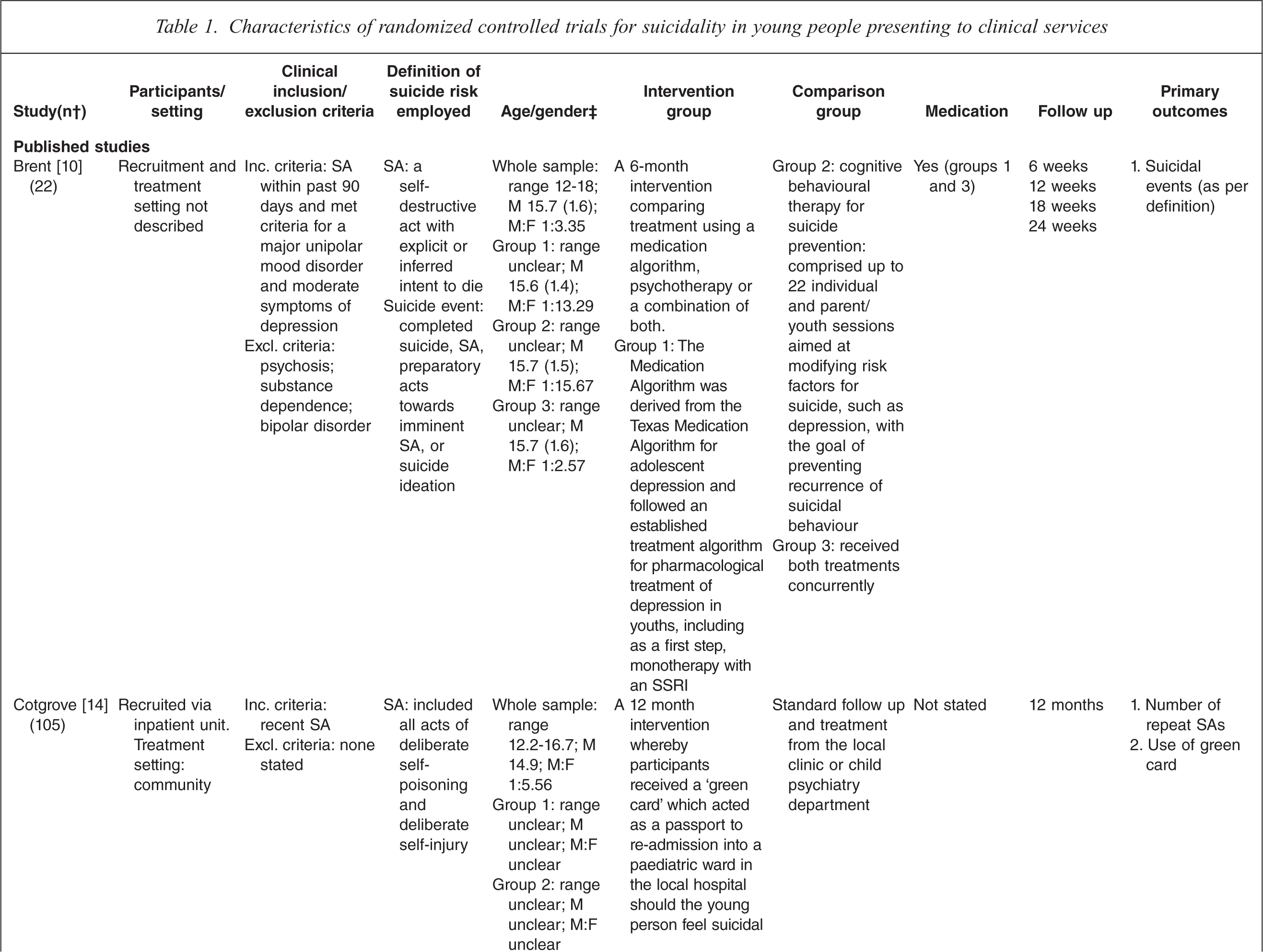
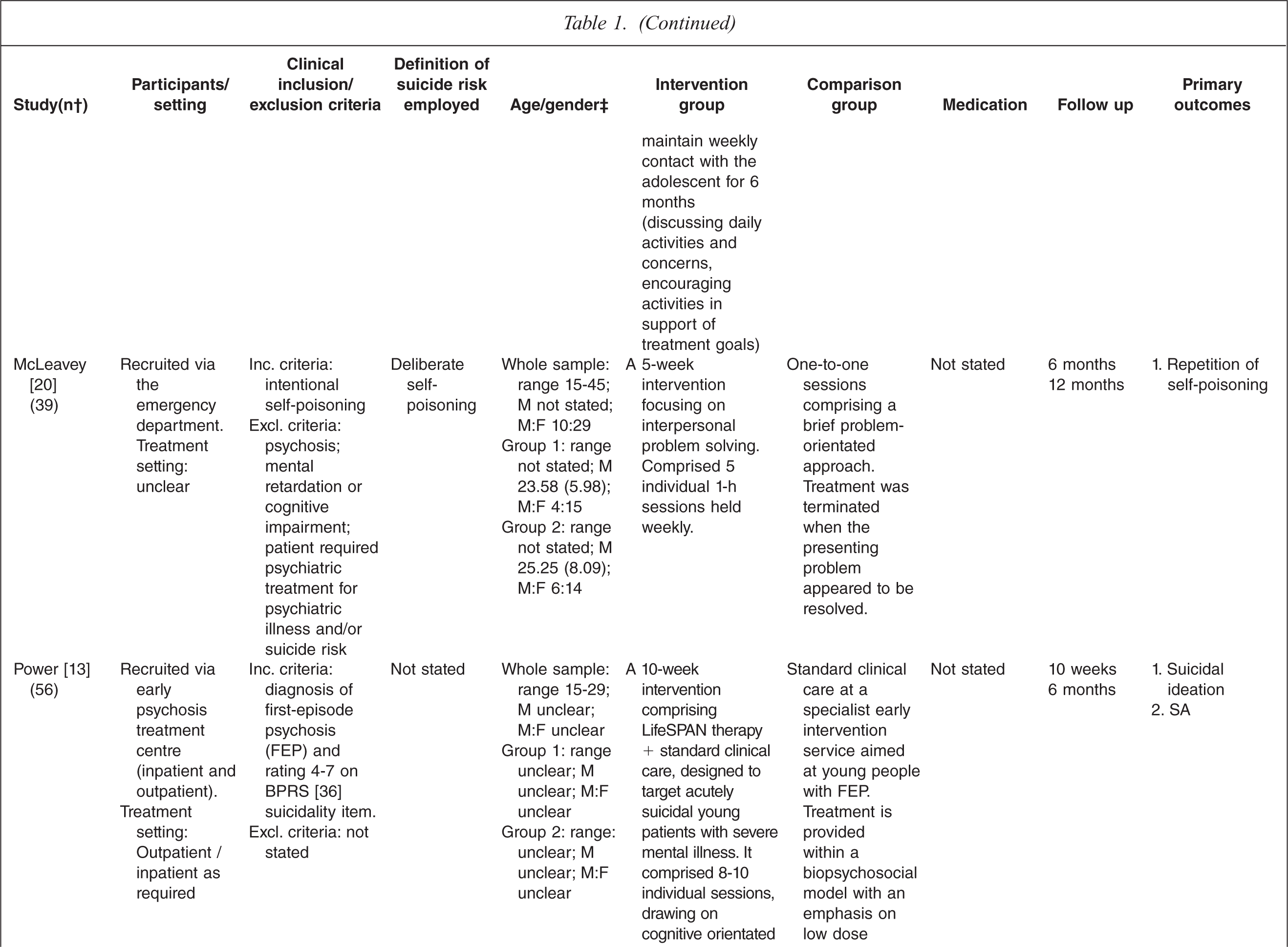
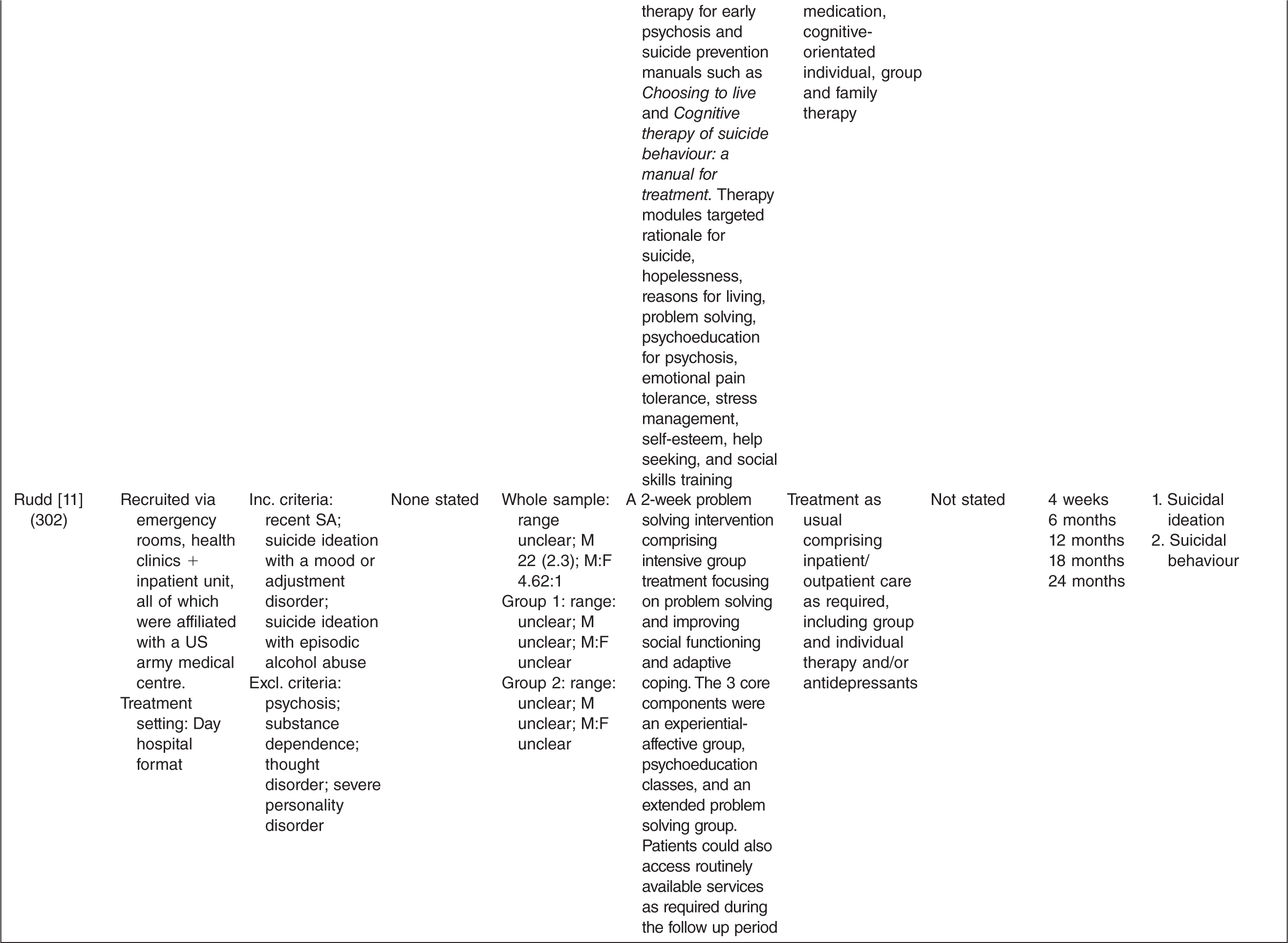
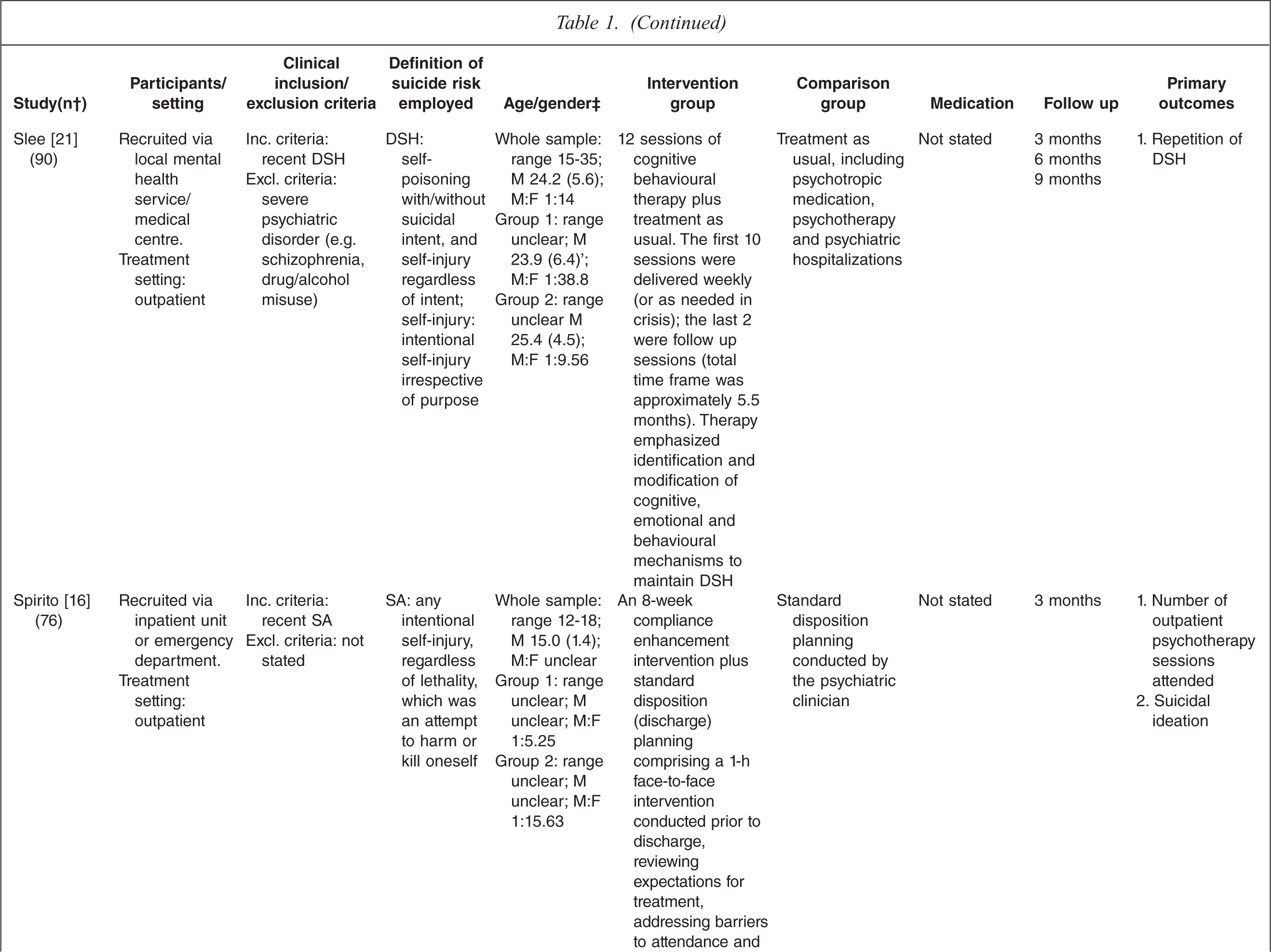
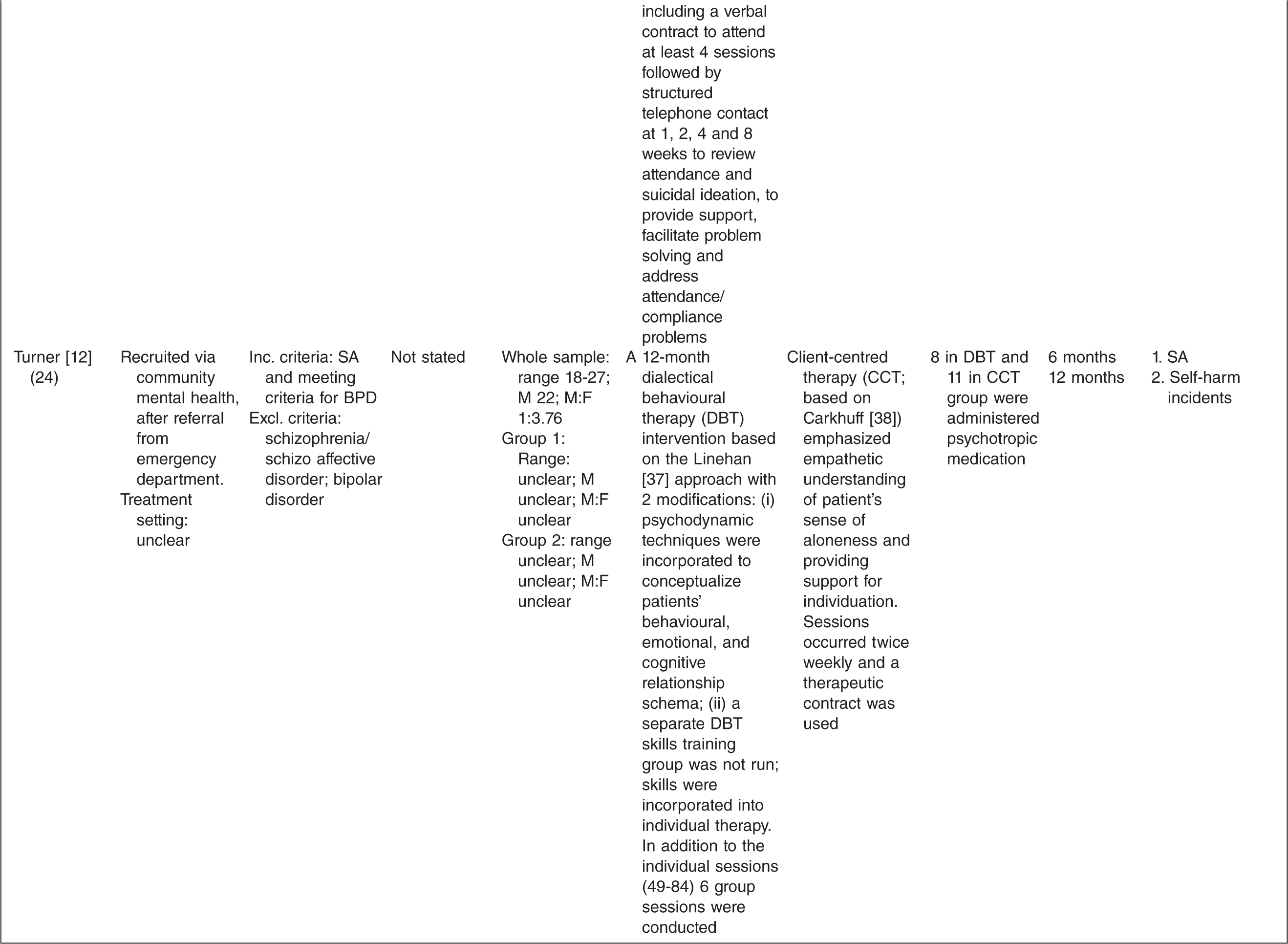
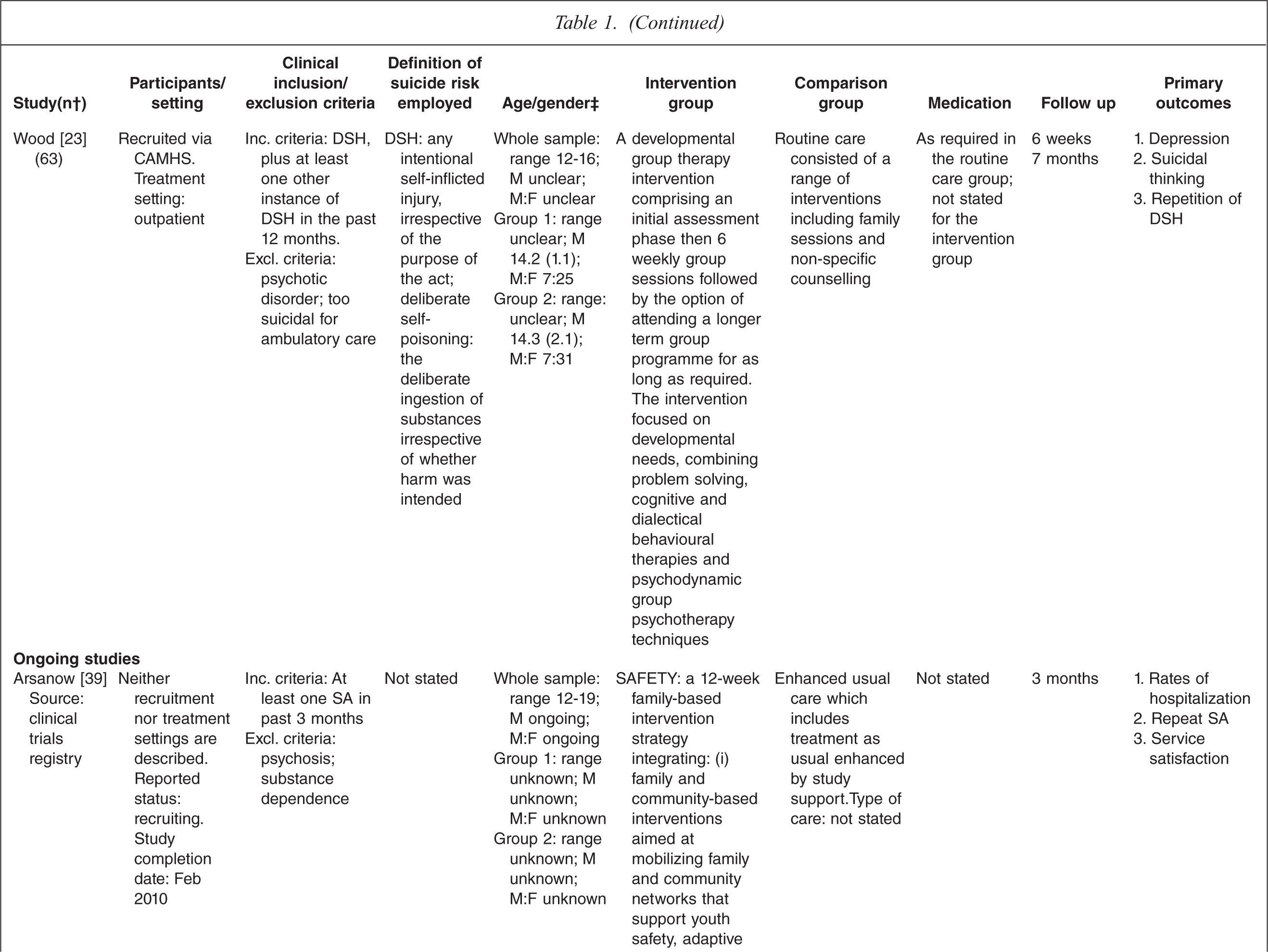
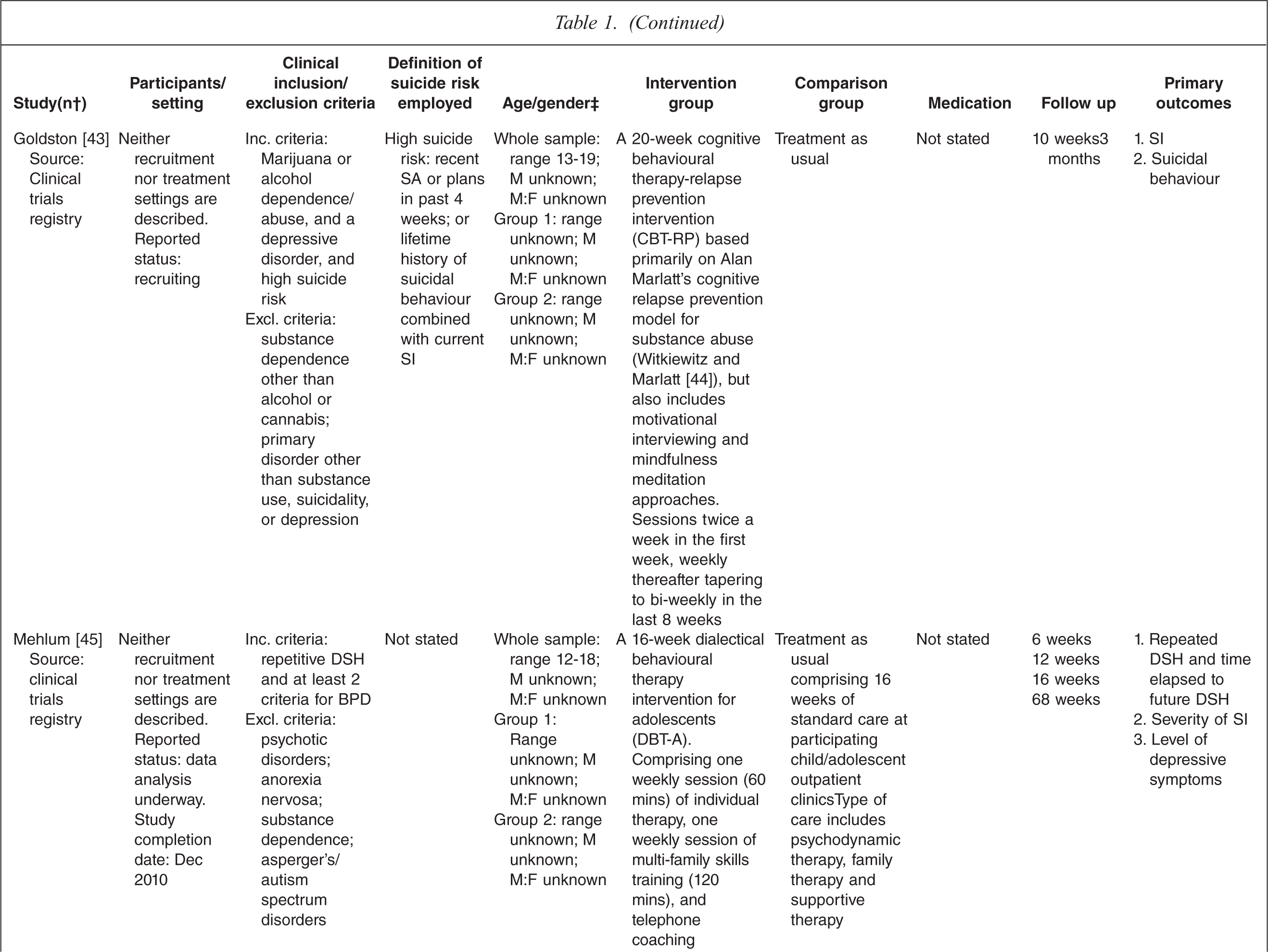
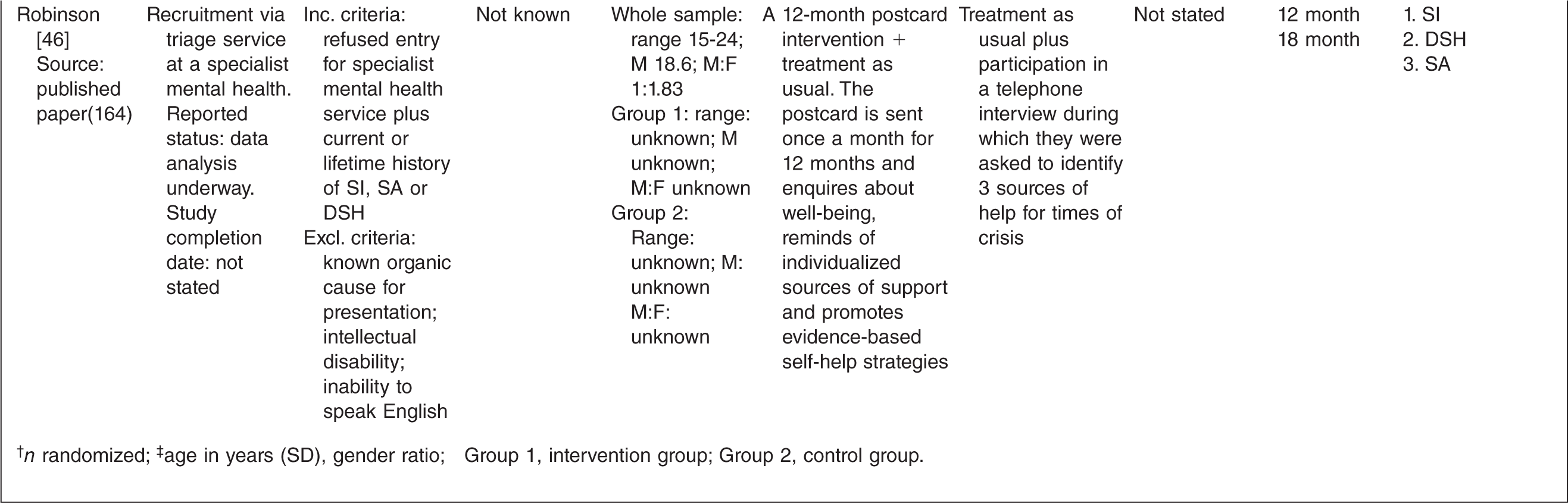
† n randomized;‡ age in years (SD), gender ratio; Group 1, intervention group; Group 2, control group.
One study tested the effects of medication [10] and this study involved comparing three treatment conditions: 1) medication 2) psychotherapy and 3) a combination of medication plus psychotherapy. One study [14] tested an emergency access card, one tested a home-based family intervention [15], one study tested a compliance enhancement intervention [16], two studies tested a youth nominated support team [17,18], five studies tested individual-based psychological therapies, of which one was dialectical behavioural therapy [12] (DBT), two were problem solving interventions [19,20] and the remaining two were cognitive behavioural therapy-based [13,21] (CBT). Three studies tested group-based psychological therapies [11,22,23] and one tested an attachment-based family therapy which uses behavioural, cognitive and psycho-educational interventions [24].
Overall studies were relatively small with sample sizes ranging from 22–448. Interventions lasted between 2 weeks and 12 months with follow-up periods ranging between 4 weeks and 2 years. Further details of each of the included studies are provided in Table 1. In most studies the comparison groups received treatment as usual, which typically included inpatient or outpatient care as required, delivered by local mental health services. In six studies medication was specifically mentioned as a component of treatment as usual.
Methodological quality
Assessment of risk of bias
A description of the conduct of the trials included in the meta-analysis and assessment of the risk of bias is presented in Table 2. The quality of reporting of trial conduct varied. Eight studies gave details of the randomization procedure, which was adequate in all cases [11,13–15,17,18,21,22] and six detailed adequate allocation concealment [15,18,21–24]. Eight studies gave an explicit description of an adequate masking procedure [10,11,13,15,18,20,22,23]. Four studies stated that no masking was used [14,17,21,24], and three did not give a clear description [13,16,19].
Risk of bias
(a) Treatment group; (b) Control group.
The attrition rate for the 15 published trials varied between 0 and 68% in the treatment groups and 0 and 79% in the control groups. Only four trials appeared to include all randomized patients in their analysis [10,12,21,24]. Eight trials were conducted using manual-based interventions [15,17,18,20–24] and in three studies the same therapists appeared to deliver both the treatment and control interventions [12,19,20].
Reporting bias
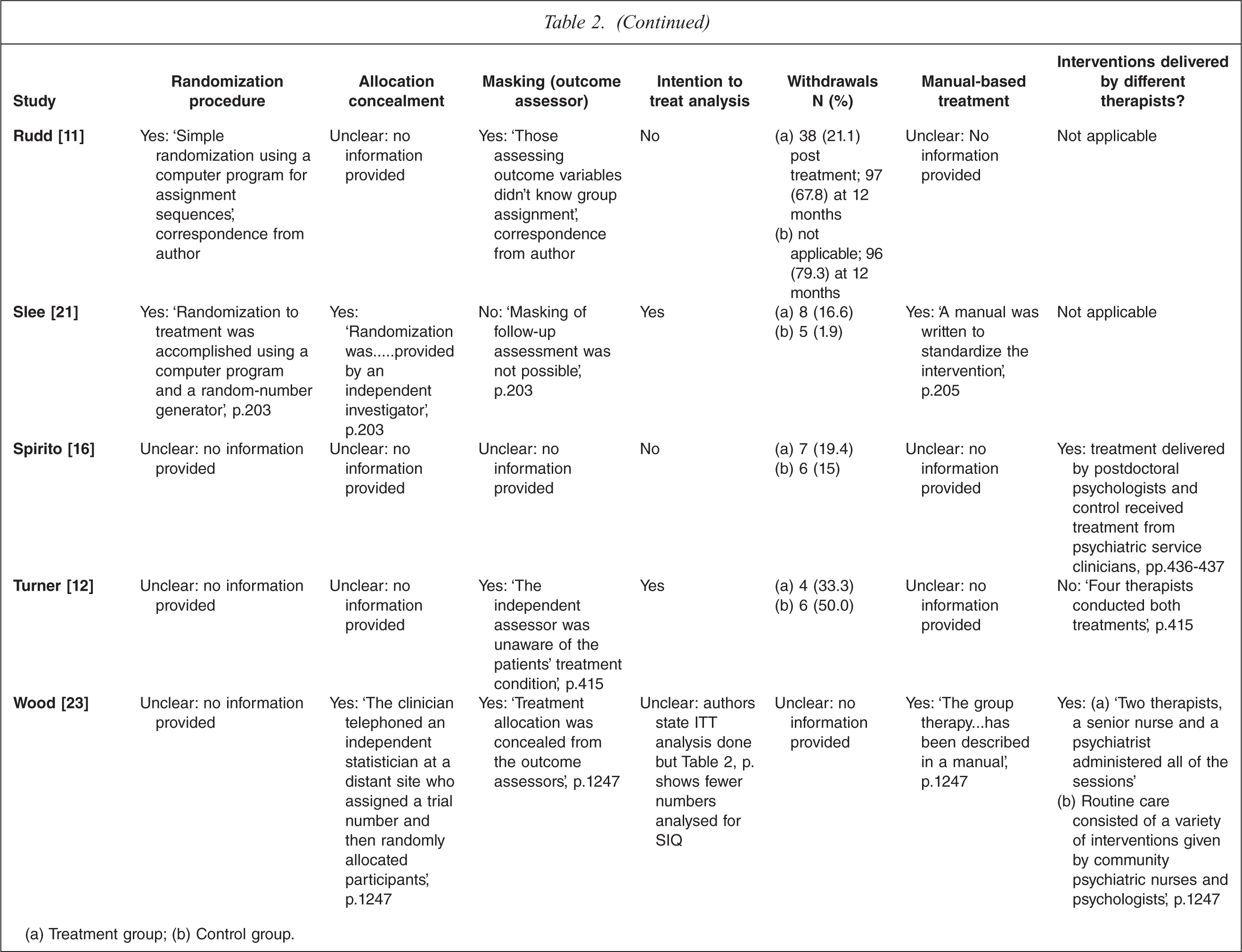
There were three things we looked for in assessing reporting bias in this review (summarized in Table 3). The first was where the authors simply appear not to have measured outcomes that we are collecting (and therefore, there are no results or data reported). The primary outcomes of the review (SI, SA, DSH) are all related and we would expect that they would have been measured in trials that aimed to reduce suicidal behaviours.
Data provided in published trial
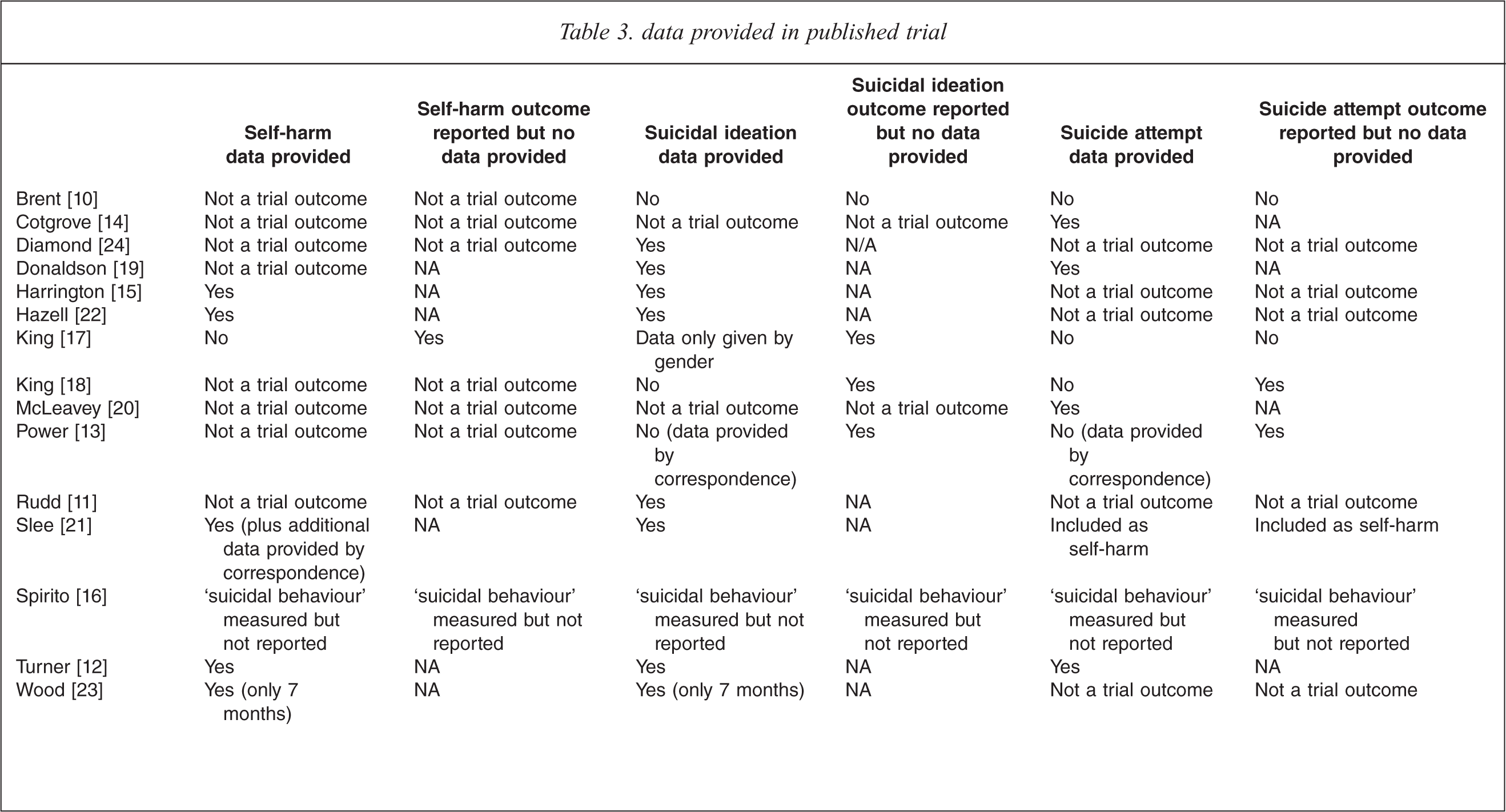
Of the included studies in this review missing data was partly the result of different studies measuring the same outcome in different ways (e.g. number of people with repeat SA versus number of repeat attempts), and partly due to different ways of defining the outcomes of interest. For example, DSH is a term that can include both suicidal and non-suicidal self-injury and often the presence or absence of intent is not clear and not measured. Consequently, SA is often not stated as a trial outcome because it falls under the term DSH, for example in the case of the following studies: Rudd et al. [11]; Wood et al. [23]; Hazell et al. [22] and Harrington et al. [15]. In contrast, Slee et al. [21], specifically state that DSH also includes SA. It is therefore possible that those trials that do not mention SA in fact include it under the term ‘self-harm’. The opposite may be true of Donaldson et al. [19] and Brent et al. [10] who report data for SI and SA but DSH is not stated as a trial outcome.
Secondly, we looked for occasions where an outcome was said to have been measured but no results or data were given. It is assumed that in this case the results were not significant and therefore were not reported. Important data are therefore missing from the meta-analysis. Of the included studies, Brent et al. [10] provides no results and no data for SI or SA. Spirito et al. [16] provides no results or data for ‘suicidal behaviour’ (which, as stated above, may include SI, SA and DSH). Wood et al. [23], although she provides 7-month follow-up data does not provide 7-week data.
Finally, we looked for instances where a result was reported but no data were provided in the trial report (e.g. means and standard deviations for scale score measures and frequency data for dichotomous outcomes). In this case, we could not include relevant data in the meta-analysis, and therefore there are important data missing from our analysis. King et al. [17] provides results for SI, SA and DSH but no data. King et al. [18] provides no data for SI or SA but does provide their own analysis and results. Interestingly, SA is not mentioned as an outcome in their study methods. Power et al. [13] provides results but gives no outcome data for SI or SA [13].
One study (McLeavey et al. [20]) only includes SA as an outcome of interest. Whilst the data are reported, they are presented as percentages only, with no information regarding the denominator. Based on the information provided, we made a ‘best guess’ at a denominator and entered these data into the meta-analysis.
Given the various types of reporting bias noted using these approaches, we then wrote to eleven authors [10,12–14,16–21,23] to obtain missing outcome data; of whom two replied providing the data requested.
Effects of interventions
Cognitive behavioural therapy versus treatment as usual
There were two studies that compared an individual CBT-based psychological therapy with treatment as usual [13,21] (TAU), one of which provided data for some of the outcomes of interest [21].
Number of self-harm incidents
One trial reported on the number of self-harm incidents post intervention, at 6 months and at 9 month follow up [21]. Whilst there were no statistically significant differences between the groups either post intervention or at 6 months, at 9 months there were fewer self-harm incidents reported in the group receiving CBT (MD −3.4 95%CI −6.54 to −0.26).
Number of people with self-harm incidents
One study [21] reported on the number of people who engaged in DSH at 9 month follow up and there was no statistically significant difference between the groups.
Suicidal ideation
One study [21] reported on the severity of SI post intervention at 6 and 9 month follow up. There was a significant reduction in SI (as measured by the Suicide Cognition Scale [25]; scores range from 20–100) in the group receiving CBT post intervention (MD −13.07 95%CI −22.48, −3.66), at six months (MD −13.78 95%CI −23.49, −4.07) and at nine months (MD −18.28 95% CI −26.66, −9.9).
Individual psychological therapy versus control intervention
There were two studies that compared individual psychological therapy to a specific control intervention [19,20], both of which provided some data for some of the outcomes of interest.
Number of people with suicide attempt
One study [19] found no statistically significant differences between individual psychological therapy and a control condition in the number of people who attempted suicide post intervention (RR 4.27 95%CI 0.54, 33.98) or at 6 month follow up (RR 2.13 95%CI 0.46, 9.99), and two studies [19,20] found no differences between groups at 12 months (RR 0.42 95%CI 0.09, 1.92).
Suicidal ideation
One study [19] measured suicidal ideation (using the Suicidal Ideation Questionnaire [26]; SIQ; scores range from 0–180) and found no differences between the groups post intervention (MD −7.50 95%CI −22.94, 7.97), at 6 months follow up (MD −5.11 95%CI −30.18, 19.96) or at 12 months (MD −8.44 95% CI −29.19, 12.31).
Group psychological therapy versus TAU
There were three studies included in this comparison, all of which contributed some data to some meta-analyses. The study by Hazell and colleagues [22] was a replication of an earlier study by Wood et al. [23]. The third study included here [11] had a very high rate of attrition.
Mean number of self-harm incidents (7 months)
One study [23] contributed data to this outcome and showed no statistically significant difference between groups (RR −1.20 95% CI −2.44, 0.44).
Number of people who engaged in multiple self-harm incidents
Two studies [22,23] contributed data to this outcome at the 6–7-month follow-up point and found no statistically significant differences between the groups (RR 0.54 95%CI 0.07, 3.95). We noted considerable heterogeneity (tau2 = 1.79; chi2 = 7.19, df = 1(P = 0.007); I2 = 86%). The study by Wood et al. [23] showed a significant reduction in the number of people who engaged in multiple episodes of DSH at 7 months, whilst Hazell et al. [22], in a replication of Wood et al.'s study, showed no significant differences between groups at 6 month follow up. Follow up from Hazell et al.'s study at 12 months showed that there continued to be no differences between groups (RR 1.37 95%CI 0.96, 1.95).
Number of people with self-harm
Hazell et al. [22] also measured the number of people with self-harm, again finding no differences between the groups either at 6 (RR 1.3 95%CI 1.0, 1.7) or 12 month follow up (RR1.25 95%CI 0.97, 1.6).
Suicidal ideation
Two studies [11,22] found no differences in levels of suicidal ideation between the two groups post intervention (one of the studies measured this using the SIQ [26], range 0180 [22], whilst the other measured it using the Suicide Probability Scale [25](range 30–146) [11] (SMD −0.03 95%CI −0.26, 0.21). All three studies (Wood et al. [23] also employed the SIQ) contributed data to the outcome at 6–7 months follow up and found no differences between the groups (SMD −0.08 95%CI −0.32, 0.17). Two studies [11,22] measured SI at 12 month follow up and again found no differences between the groups (SMD −0.09 95%CI −0.43, 0.25). There is no heterogeneity in these data.
DBT versus control intervention
There was one study [12] included that compared DBT with client-centred therapy and provided data for two outcomes.
Mean number of suicide attempts
There was a statistically significant difference between the groups, with fewer suicide attempts reported in the DBT group compared to the client centred therapy group at both 6 (MD −4.58 95%CI −8.13, −1.03) and 12 month follow up (MD −4.83 95% CI −7.9, −1.76).
Suicidal ideation
Using the Beck Scale for Suicidal Ideation [27] (scores range from range 0–38), there was a statistically significant difference between groups, with the DBT group exhibiting lower levels of SI at both 6 (MD −10.5 95% CI −16.38, −4.62) and 12 months (MD −7.75 95%CI −14.66, −0.84).
Family therapies versus TAU
There were two studies [15,24] that tested a family-based intervention and there were data available for two outcomes.
Number of people with one or more incidents of self-harm
At 6 month follow up there were no differences in the number of people who had experienced one or more incidents of DSH (RR 1.01 95%CI 0.47, 2.19).
Suicidal ideation
Harrington et al. [15] measured suicidal ideation using the Suicidal Ideation Questionnaire [26] (range 0–180; high score indicated greater suicidal ideation) whereas Diamond et al. [24] used the Suicidal Ideation Questionnaire JR [26] (scores range from 0–90, high scores indicating greater suicidal ideation), therefore we used the standardized mean difference to combine the data. There were no differences between groups in levels of SI either post intervention (SMD −0.39 95%CI −1.07, 0.29) or at 6 month follow up (SMD −0.38 95% CI −0.93, 0.17). Heterogeneity was high at post-intervention (tau2 = 0.2; chi2 = 5.31, df = 1(P = 0.02); I2 = 81%) and again at follow up (tau2 = 0.11; chi2 = 3.48, df = 1(P = 0.06); I2 = 71%).
Compliance enhancement intervention versus TAU
There was one study that was included in this outcome [16] but no outcome data were available.
Youth nominated support team versus TAU
There were two studies by the same author [17,18] investigating an intervention called a Youth Nominated Support Team plus TAU compared to TAU alone. Data were only available from one of these studies [17] and only for one outcome.
Number of people with suicide attempt
There was no difference between the groups in the number of people who attempted suicide post intervention (RR 1.55 95%CI 0.83, 2.93).
Emergency access card
One study investigated the use of an emergency ‘green’ card, plus TAU compared to TAU alone [14].
Number of people with suicide attempts
There were only data available for one outcome and this showed that at 12 month follow up there were no differences between groups in the number of people who made a suicide attempt (RR 0.53 95% CI 0.14, 1.93).
Medication versus CBT
There was one study that was included in this outcome [10] but no outcome data were available.
Medication versus CBT plus medication
There was one study that was included in this outcome [10] but no outcome data were available.
CBT versus CBT plus medication
There was one study that was included in this outcome [10] but no outcome data were available.
Whilst completed suicide was not a review outcome, two studies did report this. Power and colleagues [13] reported that 2 suicides had occurred by 6 month follow up, one in the treatment group and 1 in the control group. Slee et al. [21] also reported two suicides, both from the treatment as usual group, one of which had occurred by 6 month follow up and the second of which occurred between 6 and 9 months.
Planned sensitivity analyses
As planned, a sensitivity analysis was conducted whereby studies with either inadequate or unclear allocation concealment or an attrition rate of over 50% were removed from the analysis. Given that only a few studies could be combined in a meta-analysis, sensitivity analysis was only applicable in one instance: group psychological versus TAU. The study by Rudd and colleagues [11] was removed on the basis of unclear allocation concealment and a high dropout rate. Removing this study did not change the results. However, it is also noteworthy that the study by Turner and colleagues [12] also had a relatively high rate of attrition: 33% and 50% in the treatment and control groups respectively, but as this was the only DBT-based study no sensitivity analysis could be undertaken.
Discussion
The current study retrieved 15 published trials and 6 ongoing trials, and only 11 of the 15 published studies reported some data that could contribute to the meta-analysis. However, despite this small number, the meta-analysis did generate some significant findings, providing us with some indication as to what might and might not work when it comes to reducing suicide risk in adolescents and young adults.
Effects of interventions
Psychological therapy demonstrated some effectiveness on some of the outcomes of interest when compared to TAU. However, the same effect was not evident when psychological therapy was compared to a control intervention. The single exception to this was one small study (n = 24) which compared DBT with client-centred therapy in people with borderline personality disorder. This trial demonstrated that there were fewer suicide attempts and less suicidal ideation in the DBT group at both 6 and 12 month follow up [12]. However, caution is required, given this was a small study with an extremely high dropout rate, which could possibly over inflate the treatment effect.
The study conducted by Slee and colleagues [21] (n = 77), which compared individual CBT with TAU, demonstrated clinically significant reductions in terms of suicidal ideation that increased over follow up. While the number of self-harmers remained the same in both groups post intervention, there were significantly fewer incidents of DSH in the CBT group at 9 months follow up. That is, the number of people who engaged in DSH did not change; but the number of incidents of DSH was reduced in the CBT group.
When individual problem solving [20] or skills based therapies [19] were compared to a control intervention as opposed to TAU, there were no treatment effects evident for either the number of people with a suicide attempt (two studies, n = 70) or levels of suicidal ideation (one study, n = 31).
When looking at the results for group-based problem solving therapies versus standard care we saw considerable heterogeneity in the data both across and within outcomes. There were no differences between groups in suicidal ideation post intervention (two studies, n = 282) or at follow up (three studies, n = 258). The study by Hazell et al. [22] was a replication of an earlier study [23] and showed the opposite results, in that the intervention did not reduce the number of people engaging in multiple self-harm incidents at follow up. When combined in meta-analysis, the results show no statistical difference between group therapy and standard care. Hazell et al. [22] suggest that the differences between the results of the earlier study and his study may be due sampling differences such as high rates of self-cutting across both treatment and control groups in the later, Australian study.
Other studies examined the effects of interventions that targeted the family [15] (n = 220), a youth nominated support intervention [18] (n = 236) and an emergency access intervention [14] (n = 105) but none of these studies showed any significant effects with regard to our outcomes of interest, i.e. SI, SA or DSH. We did notice considerable heterogeneity between the two family-based studies, with the study by Harrington and colleagues [15] showing no significant differences between routine care and a 5-session home-based family intervention. In contrast, the study by Diamond and colleagues [24] did show a significant effect. This study compared a 10-session intervention delivered over 12 weeks with usual care. However, we cannot be certain that this difference is not the result of a lack of blinding in the Diamond study and the longer intervention. In fact, overall we cannot be entirely certain that these results are an effect of limitations in study design or ineffective interventions, as opposed to the alternative view whereby the interventions being tested are indeed effective; it is just that they are no more effective than the control condition or treatment as usual.
Limitations of the study
The following limitations need to be borne in mind when interpreting the results of this review.
Firstly, we identified a small number of studies some of which did not measure the outcomes of interest, resulting in only a small amount of data available for each comparison. Further, most studies were not adequately powered to measure suicide as an outcome, only proxy outcomes such as SI, SA and DSH. This is not unusual in suicide research as, despite it being a significant problem, suicide is a low base rate event meaning that in order to conduct research with suicide as an outcome, very large studies with long follow-up periods are required. Whilst proxy indicators of suicide risk are often used as study outcomes, there remains a need for large, adequately powered trials that can examine the effects of interventions on rates of suicide. Related to this was the absence of standardized definitions of the key outcomes of interest and the use of variable outcome measures across the included studies. For example, in some cases trialists did not distinguish between suicide attempt and non-suicidal self-harm which made the pooling of data and the interpretation of the findings problematic.
In general, the reporting of random sequence generation, allocation concealment, the use of intention-to-treat analysis and masking was poor, making the assessment of the potential for biased estimates of treatment effects difficult [9]. Given the relationship between poor reporting and larger treatment effects, findings reported by these trials may have overestimated summary treatment effects [28]. Included in assessment of risk of bias, and of particular concern, was the high rate of drop out in some studies. The study by Rudd and colleagues [11] was of particular concern, but the study conducted by Turner [12] also reported a relatively high rate of attrition.
Strengths of the study
The authors conducted an extensive search not only of the electronic databases cited above, but also of all reference lists of the included studies and conference abstracts. Efforts were also made to search the grey literature; hence the number of articles potentially missed by the study was kept to a minimum. Every effort was made to contact study authors for additional information regarding randomization procedures and for additional outcome data where feasible. The review only includes randomized controlled trials and incorporates a careful assessment of trial conduct and potential risk of bias, including meta-analytic techniques where appropriate. To our knowledge this has not been conducted in previous reviews targeting this population. We also specifically target clinical settings. Finally we have been able to include several trials not previously incorporated into a review.
Hence, this review adds to the previous literature in several important ways. In particular we specifically address a population for whom we know least about effective interventions yet are frequently excluded from clinical trials.
Research and clinical implications
Considering that suicidality and deliberate self-harm among adolescents and young adults continue to be of significant concern, and the reduction of both of these phenomena is a government priority in many countries, this lack of research is disappointing. Recent Australian research has noted the large number of studies that report epidemiological data regarding rates and risk factors for suicide compared to the relatively small number that report the effects of interventions, in particular those tested via RCTs [4]. Previous reviews have found similarly small numbers of published trials undertaken with adolescents [29,30]. A more recent review [31] examining CBT-based interventions in all age groups reported a positive effect among adults but not adolescents. Our review updates this by including recently published RCTs and suggests that this effect may also be true for adolescents and young adults. We also identified a study testing interpersonal therapy among depressed and suicidal school students delivered by school counsellors and intern counselling psychotherapists [32]. This study reported a positive effect and whilst not included in our analysis as it did not meet our criteria (i.e. it was conducted in a school setting) this type of intervention could be equally tested in clinical settings.
Whilst conducting scientifically rigorous research in this field is challenging, in order to achieve a meaningful reduction in these behaviours a greater body of high quality evidence is required. In particular, future research should focus upon the development of large, randomized controlled trials testing a range of interventions which can address the methodological shortfalls that we have identified. Specifically, they should employ standardized definitions of key outcomes of interest and use similar measures, administered at similar follow-up time points. They should ensure trial conduct minimizes the risk of bias. Finally, authors should report the data for all measured outcomes (be they positive or negative). Taken together, this will enable us to pool data from different studies and place us in a better position to develop and test effective interventions designed to reduce SI, SA and DSH in young people.
Limited evidence regarding the effectiveness of interventions to reduce suicide risk in young people has made it difficult to draw firm conclusions regarding what does and does not work in suicide prevention. However, our results suggest that individual CBT-based interventions appear to show promise with this population. Attachment-based family therapy is certainly worth subjecting to further investigation in a high quality randomized controlled trial and there is also room for the development and testing of innovative interventions among young people at risk.
Footnotes
Declaration of interest
Orygen Youth Health receives funds from the Colonial Foundation. Sarah Hetrick is funded via a NHMRC training fellowship. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Author contributions
All authors contributed to the study design, data collection and interpretation of results. J.R. and S.H. drafted the manuscript. All authors participated in critical revision of manuscript drafts and approved the final version.