
Abstract
National and international concern exists about the increase in rates of suicide among young people. Suicide ranks among the top 10 causes of death in most western countries. From 1960 to 2001, the suicide rate for 15–24 years-old Australian males rose three-fold, from 6.8 to 20.3 per 100 000 population, reaching a peak of 30.6 in 1997. Suicide rates for females aged 15–24 rose during the early 1960s but have since stabilized at around 6 per 100 000. In Australia and New Zealand suicide rates in young adult males are higher than in older age groups and over the last 30 years an increase in suicide rates among Australian males aged 25–34 has also been noted [1–3]. Indigenous suicide rates are particularly high [3]. The overall economic costs of suicide and suicidal behaviour are difficult to estimate. In 1996, the medical costs alone of youth suicide and attempted suicide in the USA were estimated at $950 million, and the total costs, including medical, future earnings and quality of life, at $15 639 million [4].
Doubts have been raised about the capacity of service systems to engage and follow-up young people after presentation to services and a re-organization of mental health services for adolescents, to make them more responsive to crises that typically occur after hours is well overdue [5–8]. Available data indicates that adherence rates with follow-up for non-hospitalized adolescents presenting with deliberate self-harm (DSH) range between 20 and 30% of all cases [9], [10]. Similarly, rates of follow-up for adolescents admitted to hospital following self-poisoning have generally been reported at below 50% with high rates of withdrawal from subsequent treatment [10], [11].
In Australia a considerable gap exists between current practice and research findings either supporting or refuting particular strategies employed in the clinical management of suicidal behaviour in young people [12]. Clinical interventions are considered ‘best practice’ despite limited evaluation (e.g. ‘green cards’, ‘suicide contract’). The aim of this review was to examine papers reporting interventions directed to the reduction in the repetition of self-harm, and to increased participation in psychological treatment in young people aged 12–22 years. The proxy variable of reduction in suicidal ideation was also considered.
Method
The foundation document for this paper was a systematic literature review ‘Setting the evidence-based research agenda for Australia’; a joint initiative commissioned by the Strategic Research Development Committee of the National Health and Medical Research Council and the Mental Health Branch of the Commonwealth Department of Health and Aged Care. A broad public health framework was used to identify risk and protective factors for youth suicide with a view to including interventions that targeted these factors (a description of key words can be obtained from the authors).
Studies were included if they described randomised control trials, clinical control trials, or quasi-experimental trials comparing an intervention with standard aftercare directed to adolescents or young adults identified through presentation to hospital with self-harm, or otherwise identified as engaging in self-harm. Outcomes of interest were repetition of self-harm, adherence to treatment, and reduction in suicidal ideation. Papers were identified by searching MEDLINE, PsychINFO, EMBASE, ERIC, CINHAL, Cochrane Database of Systematic Reviews and the Cochrane Controlled Trials Register. In addition to searching electronic databases, we contacted internationally and nationally significant investigators to identify documentation or unpublished manuscripts. Other articles were also identified using the reference lists from published manuscripts. Although it is acknowledged that important research is being conducted in non-English speaking countries, it was not practical to include these studies in this review.
Wherever possible, summary outcomes were expressed as a relative risk (RR) (absolute risk of events in the treatment group divided by the absolute risk of events in the control group) plus the 95% confidence interval (CI) for the RR. A statistically significant benefit of treatment is indicated if the upper limit of the RR 95% CI is less than one, while conversely a statistically significant benefit of control treatment over the experimental treatment is indicated if the lower limit of RR 95% CI is greater than or equal to one.
Results
We identified three RCTs, four clinical control trials and three quasiexperimental studies (see 15], four trials of intense management with outreach [13, 14, Silburn et al., unpublished data, Huey et al., 2004], one trial of readmission on demand (‘green card’) [13], two trials of enhanced family intervention [21], [22], and one trial of group therapy [21]. Rudd's (1996) paper was excluded, as DSH was not measured [22]. Numeric data, including estimates of relative risk for key outcomes, are summarized in Table 1. Owing to the heterogeneity of interventions no meta-analyses have been conducted. Similarly, as data from studies have not been pooled, a systematic assessment of study quality has not been undertaken.
Clinical interventions targeting attempted suicide and deliberate self-harm in adolescent
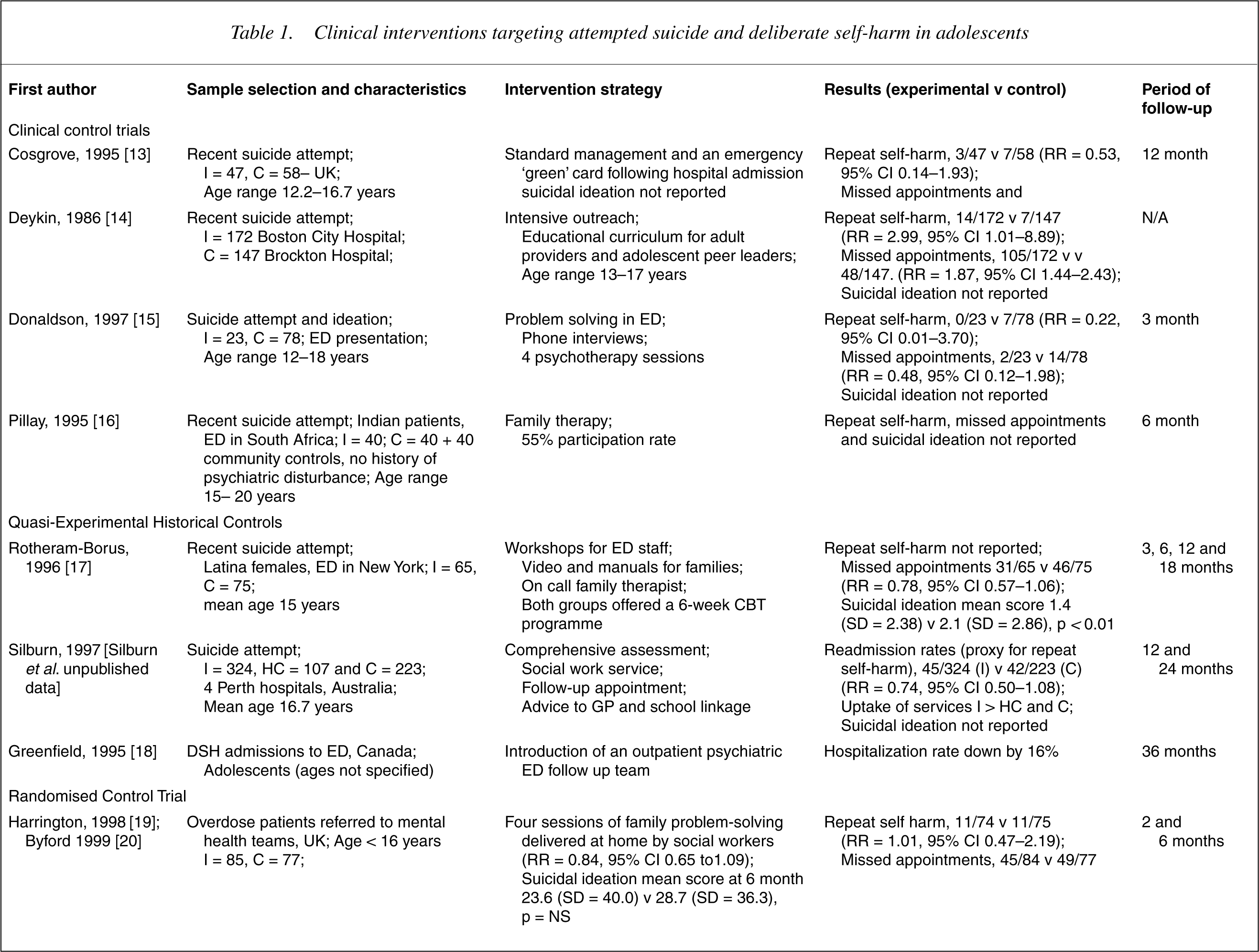
C, control group; CI, confidence interval; ED, emergency department; HC, historical control group; I, intervention group; NS, not statistically significant; RR, relative risk.
Problem solving therapy
Some suicidal adolescents have difficulty generating and evaluating the usefulness of a range of solutions to problems [23]. Problem solving therapy, which is a specific form of cognitive therapy, addresses these deficiencies, and may be especially appropriate for a suicide attempter who is impulsive [24]. An important component of problem solving is the progression though a specific sequence of steps. One such sequence for suicidal adolescents and their families involves problem definition, followed by brainstorming of alternative solutions.
Donaldson et al. reported a clinical control trial of problem solving therapy directed to adolescents presenting to an emergency department with deliberate self-harm and/or suicidal ideation [15]. Twenty-three adolescents received the intervention and their outcome was compared with 78 adolescents who received standard aftercare. The intervention comprised three follow-up phone interviews over an 8-week postdischarge period and a verbal agreement between the adolescent and parent/guardian to attend at least four psychotherapy sessions. At 3-month follow-up there were no significant differences between the treatment group and the group who received standard aftercare in any of the relevant outcome measures. However, there was a non-significant trend for fewer adolescents from the experimental group to self-harm or to fail to attend the minimum number of required psychotherapy sessions.
Intensive intervention plus outreach
Sometimes known as assertive outreach, intensive intervention employs various strategies, such as regular telephone contact and home visiting, to increase engagement and/or reduce self-harm.
One of the earliest prevention studies targeting recent suicide attempts in adolescents was a quasi-experimental trial combining intensive outreach with a community educational curriculum programme for professionals, adult providers and adolescent peer group leaders [14]. One hundred and seventy-two adolescents presenting with suicide attempts received the intervention, and their outcomes were compared with 147 historical controls. This study reported higher subject compliance, greater help-seeking and reduced overall occurrence of emergency admissions for suicidal behaviours in the intervention group. No significant differences were reported on the frequency of repeat suicide attempts. The educational component aided the early identification and referral of young people who were experiencing suicidal thoughts but were not exhibiting self-harming behaviour.
In Canada the impact of an outpatient psychiatric emergency department Follow-up Team was examined. The study employed historical controls comparing the rate of adolescent psychiatric admissions to a general paediatric hospital the year before and after the team's creation. The proportion of patients returning to the emergency department two or more times was also compared for those same years. At 3-year follow-up hospitalization rates were 16% lower in the experimental group without an increase in the proportion of subjects returning to the emergency department [18].
One Australian study assessed the efficacy of improving clinical intervention for patients presenting to emergency departments who have attempted suicide [Silburn et al. unpublished data]. The study used a quasi-experimental design involving three groups: ‘enhanced’ intervention (n = 324), historical controls (n = 107) and contemporary controls (n = 223). The intervention consisted of comprehensive assessment, liaison with community carers and services and a definite follow-up appointment a week after initial contact. Extra funding was provided for social work staff in emergency and psychiatry departments. At 12-month follow-up readmission rates for suicide attempts were significantly lower in the intervention group (14%) compared with historical controls (28%) and contemporary controls (19%). The finding in an Australian context is interesting but the study design hinders interpretation. Controls were drawn from a hospital that had initially refused to participate while the measures of further self-harm were based on hospital readmission, in effect a proxy measure, and it is unclear whether the results might reflect a greater willingness of the intervention group to seek further treatment of any kind, including emergency department consultation for DSH.
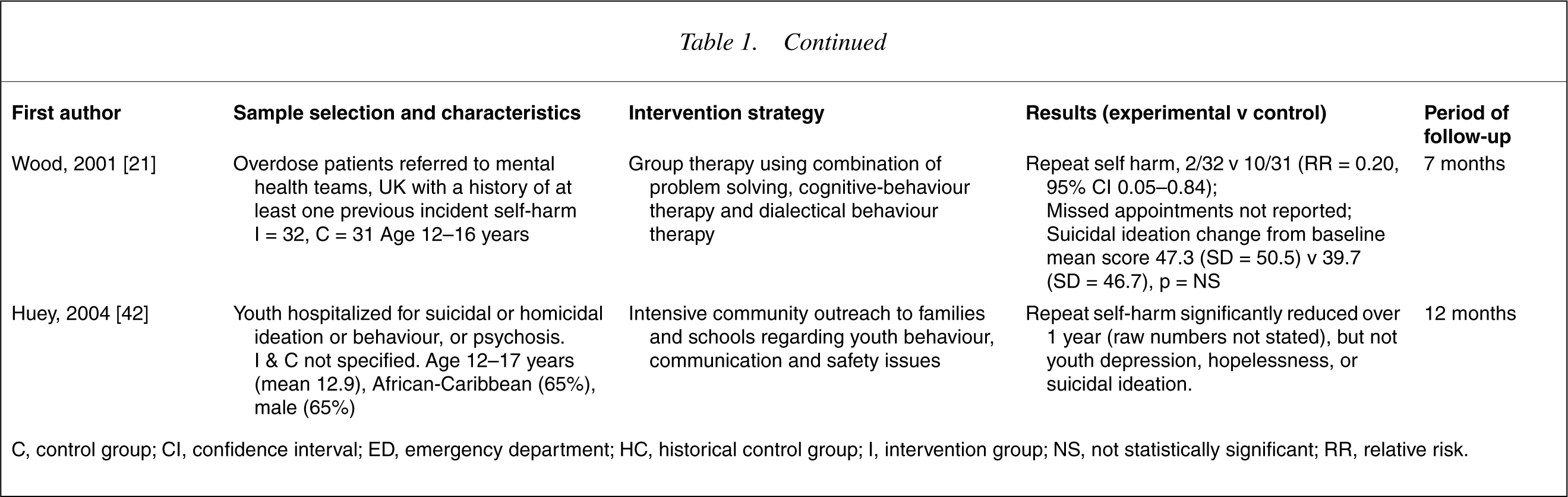
Huey et al. (2004) studied multisystemic therapy (MST) with mainly African–American youths attempting suicide and referred for emergency psychiatric hospitalization. They were randomly assigned to hospitalization or MST, which involved intensive community outreach to families and schools regarding youth behavioural, communication and safety-related issues. Attempted suicide, suicidal and depressive ideation were assessed before treatment, at 4 months and at 1 year. Youth report indicated that MST was significantly more effective than hospitalization at decreasing attempted suicide rates at 1 years, though the results were the same in both groups (4%). This effect was accounted for by the MST group having higher pretreatment levels of attempted suicide (31% vs 19%), and its rate of symptom reduction over time being greater. This raises questions about the success of the randomization process. Questions arose about whether between-group differences represented regression to the mean, and the generalisability of the results, given the specific nature of the sample. The relative lack of effect on depression, hopelessness and suicidal ideation may suggest that these are mediated by other means than those involved with suicide attempts.
Emergency (‘green’) card
The emergency (‘green’) card provides the suicide attempter with guaranteed access to 24-hour clinical follow-up on demand. The rationale for the green card is that the vulnerable individual will contact emergency services for help in preference to engaging in further deliberate self-harm. To measure the effectiveness of ‘green cards’ 47 young people (aged 12.2–16.7) were provided with a token allowing readmission on demand [13], while 58 young people in a comparison group received ‘standard treatment’ from their clinic or child psychiatry department. The card was not used extensively and at 12-month follow-up, no significant differences in readmission rates or suicidal behaviour between the two groups were found. Limited information relating to the study's design was provided and data were only available from hospital records making ascertainment bias a problem.
Family therapy
Clinical experience suggests that family involvement in the aftercare of young people who have attempted suicide can play a major role in facilitating recovery. The effectiveness of family therapy in reducing suicide attempts has been examined in one randomised controlled trial, while two trials have examined the impact of enhanced family participation, one, a clinical control trial, the other involving historical controls.
Harrington et al. report a randomised control trial of home-based social work intervention directed to young people, aged 16 or younger, who had attempted suicide by taking an overdose [19]. The intervention consisted of an assessment session and four home visits by the social workers to conduct family problem-solving sessions. Patients referred to mental health teams with a diagnosis of deliberate selfpoisoning were randomly allocated to either routine care (n = 77) or routine care plus the social work intervention (n = 85). Both groups were assessed at baseline, two and 6 months later. There were no statistically significant differences between the intervention and control groups in repetition of self-harm, adherence to psychotherapy or in suicidal ideation at either of the follow-up assessments.
In South Africa, Pillay and Wassenaar (1995) [16] studied 40 Indian adolescent parasuicides, 40 medical and 40 community controls, the latter two groups having no history of psychiatric illness or suicidal behaviour. Fifty-five per cent of the 40 parasuicides agreed to receive a family orientated psychological intervention. Parasuicide subjects consenting to receive the intervention did not differ from parasuicide subjects who did not consent on measures of hopelessness or psychiatric disturbance, but significant prepost differences in both measures (Wilcoxon two-tailed p = 0.0002) were noted for the intervention group after 6 months. Parasuicide subjects had significantly higher initial levels of hopelessness and psychiatric disturbance than both groups of control subjects (p < 0.01), and the latter groups showed no change in scores on these measures after 6 months. Suicidal behaviour was not included as an outcome measure and the authors acknowledge that other variables between the treated and untreated groups may account for the variance in hopelessness between the two groups at post-test.
Rotheram-Borus 1996 [17] studied a consecutive series of female adolescents (mean age 15) and their families presenting to the emergency department in a New York hospital. Participants had attempted suicide but did not have a psychiatric disorder or medical problem subsequent to the attempt. A quasi-experimental design with historical controls was used. In the first phase of the treatment participants were assigned to standard emergency department care, and in the second phase to the experimental conditions. The intervention included some training of generic emergency staff, provision of manuals and videotapes to set realistic treatment expectations and one family session immediately after the attempt. Both groups were offered a six-session cognitive behavioural therapy programme, which involved both patients and their families. Participation in the programme did not lead to greater attendance at follow-up appointments, but the experimental group had significantly lower levels of suicidal ideation than the control group. Rates of repeat self-harm were not reported.
Group therapy
We identified one randomised control trial comparing group therapy with standard aftercare for young suicide attempters [21]. The therapy drew on techniques from a variety of therapies including problem solving, cognitive-behavioural therapy and dialectical behaviour therapy. Participants were young people aged 12–16 referred to mental health services following an incident of self-harm, who had a history of at least one other incident of self-harm in the previous 12 months. Participants were randomised to standard aftercare or standard aftercare plus group therapy. Compared with the control group, significantly fewer adolescents from the experimental group engaged in two or more episodes of self-harm in the follow-up period. Missed appointments were not reported, but the adolescents from the experimental group attended significantly fewer psychotherapy appointments than adolescents from the control group. There were no statistically significant group differences in suicidal ideation.
Discussion
Given that deliberate self-harm is a relatively common clinical problem in adolescent mental health settings there have been few studies examining the effectiveness of treatments in preventing repetition. Before interpreting the data from these few studies, some comments are warranted concerning methodology. Only three studies employed a randomised control design. Biases may well have been operating in the selection of participants for the other trials. In, addition, there may have been problems in maintaining control groups free of contamination. Subjects and investigators are often not blind to control group status, which raises problems relating to observer bias where interview based measures have been used. Discrepancies between effectiveness judged by self-report and those that are interviewer rated are not uncommon [25]. While directed to young people who had recently engaged in deliberate self-harm, the prevention of repetition was clearly not the primary objective of several of the treatments evaluated.
We found that most novel treatment strategies directed against repetition of suicidal behaviour were compared with ‘standard aftercare’. Such ‘standard’ treatment is usually developed through clinical wisdom and adopted by consensus, but rarely supported by empirical evidence. The term ‘standard aftercare’ is a misnomer, since there is considerable heterogeneity in the aftercare of adolescent suicide attempters, determined by contextual factors such as the availability of treatment resources, financing of medical services, and defence against litigation [5].
The treatments reviewed tended to be multimodal. For example, the group therapy evaluated by Wood et al. (2001) contained elements of problem-solving, cognitive behaviour therapy and dialectical behaviour therapy. The intensive aftercare evaluated by Harrington et al. (1998) comprised brief family therapy and homevisiting. In fact we debated, for the purposes of the present review, whether to classify the intervention as intense aftercare or family therapy. That of Huey et al. (2004), comprised contingency contracting, communication training and behavioural parent training. Had there been more randomised control trials the heterogeneity of the treatments may have caused a problem in determining how to pool the studies for the purpose of meta-analysis. However, the three RCTs we identified concerned markedly different treatments and did not warrant the pooling of data.
Further methodological concerns include low participation rates of young people receiving the intervention in two studies [15], [16]; possible problems with randomization (Huey et al. 2004); problems relating to the delivery or uptake of the intervention [13], [16], [17]; the ascertainment bias inherent in the use of hospital records [13, 18, Silburn et al. unpublished data], and the variability in follow-up intervals across the studies, ranging from 3 months to 18 months. A consequence of relatively brief follow-up intervals is that subsequent self-harm incidents could be missed, and hence give an inflated estimate of the effectiveness of the treatment.
Our review found only one specific treatment, group therapy, to offer any convincing advantage over standard aftercare in reducing repetition. Repetition was defined as two or more incidents of self-harm occurring within the 7 month follow up period. This definition is different from that used in most studies. It would be interesting to know whether the group difference was sustained if the definition of repetition was any episode of self-harm. However, demonstration of a treatment effect in reducing multiple repetition is itself clinically significant. This finding will also provide reassurance to clinicians who may have felt reluctant to offer group treatment to adolescents who engage in deliberate self-harm for fear of fostering contagion. Either there is no contagion effect, or the contagion may work positively against self-harming behaviour [Harrington; personal communication].
None of the studies we reviewed found any benefit of treatment in increasing adherence with follow-up. In several studies there was a problem with the uptake of treatment [13], [16], [17]. New strategies need to be developed that promote adherence with aftercare. However, control trials are not the most suitable research design for evaluating such strategies. Process research that examines patient, therapist and treatment setting factors predictive of adherence to follow up is more likely to be informative. Too few studies reported the impact of treatment on subsequent suicidal ideation for us to draw conclusions. While sometimes used as a proxy variable for suicidality, suicidal ideation is an unsatisfactory outcome measure as it is likely to be highly state dependent.
The apparent lack of effectiveness of most treatments directed to the reduction in repetition of deliberate self-harm in young people needs to be examined in the context of data from research with adult patients. Hawton et al. found few treatments to be effective in reducing the repetition of self-harm in adults, but concluded that owing to methodological weaknesses firm recommendations about the most effective forms of treatment could not be made [26].
Two small trials, one providing depot flupenthixol [27], the other long-term dialectical therapy for female patients with borderline personality disorder [28] have shown a statistically significant reduction in recurrent DSH. The efficacy of other interventions for adults in reducing the repetition of self-harm has not been confirmed [29], although some show promise. Trials of brief problem-solving therapies and the ‘green card’, for example, have shown a statistically non-significant trend towards lower rates of repetition of DSH [30], [31]. Interventions with no established efficacy in adults include intensive intervention plus outreach [32–34], therapist continuity [35], general hospital admission [36], antidepressant therapy [27], [37] and long-term therapy [35].
During the last decade youth suicide prevention has figured prominently on the health agenda of the Australian Government with increasing acknowledgement that evidence-based approaches to the prevention of suicidal behaviour should be adopted [38], [39]. It is increasingly recognized that clinical practice benefits from research evidence of the most effective treatments. The Commonwealth Government's National Youth Suicide Prevention Strategy has aimed to foster a culture of evaluation, and has attempted to identify and disseminate information about good practice, despite the dearth of research about proven effective strategies [40], [41].
The current ‘best’ evidence suggests that multicomponent interventions are no more effective than simple interventions designed to increase patient participation rates. Given the paucity of existing evidence, research efforts should be directed towards understanding and identifying which intervention components result in enhanced outcomes. Consideration should be given to determining what outcome measures indicative of risk and protective factors for suicidal behaviour should be included in original study designs. Careful attention should also be given to process evaluation to determine what hinders or helps the delivery of interventions in clinical settings. Addressing the methodological limitations inherent in the study of interventions designed to prevent suicide in young people will facilitate ‘better practice’ in the delivery of care in clinical settings.
Footnotes
Acknowledgements
We thank Bridget Bassilios for her research assistance and acknowledge support from National Health and Medial research Council (NHMRC) and beyondblue: the national depression initiative.