
Abstract
Keywords
Generalized anxiety disorder (GAD) and oppositional defiance disorder (ODD) are among the most frequent psychiatric disorders of childhood [1]. GAD has been associated with a wide range of adverse psychosocial contexts, including parental psychopathology [2], disruption of attachment between the child and parents [3], acute life events [4], abuse [5], overprotective parenting [6], loss experiences [7], parental avoidance and modelling of anxious behaviour [8]. Adverse psychosocial contexts associated with ODD include parental psychopathology [9], poor disciplinary practices [10], marital discord [11] and strict and coercive parenting [12].
A limitation of previous work is a focus on single risk factors [13]. Consequently, little is known about interaction between risk settings in the development of GAD and ODD; in particular, the combination of risk settings the uniquely distinguish each developmental trajectory [13]. There is considerable variation in the way psychosocial stressors have been defined and measured in previous work. More consistent approaches to the measurement of psychosocial risk would facilitate cross-study comparison. Furthermore, the majority of previous studies have been of co-morbid samples. Though overlap between disorders is rather common, these samples do not allow for explicit estimation of the environmental factors important for a given disorder.
In an attempt to standardize assessment of abnormal psychosocial settings childhood, the World Health Organization (WHO) developed the Z-codes (Z60-62.9) in the ICD-10 [14]. Z-codes are a method of classifying different kinds of psychosocial situations of relevance to mental disorder. Examples of Z-codes include abnormal intra-familial relationships, parental mental disorder, distorted or inadequate intra-familial communication, and acute life events. However, it remains unclear how Z-codes, alone or in combination, relate to different child and adolescent psychiatric disorders.
Lack of specificity around the factors that distinguish mental health disorders, such as GAD and ODD, means that prevention and treatment approaches to care necessarily include redundancies that increase the cost of intervention. By more clearly separating the unique causes of one outcome from the unique causes of another, greater alignment between intervention strategies and mental health needs could be achieved. Furthermore, improved specificity should translate into improved efficacy, not only in prevention setting but also in treatment settings.
The purpose of this study was to determine whether childhood DSM-IV [15] generalized anxiety disorder (GAD) and oppositional defiant disorder (ODD) could be reliably discriminated from one another and from a non-patient school control group on the basis of ICD-10 psychosocial situations (Z-codes).
Method
Study design and sample
A case-control study design was used in which children with GAD and ODD diagnoses were compared with non-patient control children on ICD-10 classifications of psychosocial stress. Seventy-five children with GAD or ODD were referred from five child and family guidance clinics to the outpatient university clinic in Trondheim, Norway, between 2002 and 2004. Inclusion criteria were primary diagnosis of DSM-IV [15] ODD or GAD, ODD/GAD diagnosis primary reason for referral, age between 8 and 13 years old, and a mother consenting to clinical interview. Exclusion criteria were presence of any other psychiatric disorder including ADHD and somatic diseases or handicaps related to reading or writing disabilities. Twenty-one children were excluded because of co-morbidity or because of sub-threshold symptom levels for GAD and ODD. Eleven children were excluded because the mother refused to participate. The final case sample consisted of 43 children (21 with ODD and 22 with GAD).
The non-patient control group (NC) were classroom-controls with no symptoms of anxiety or behavioural disorders based on a screening prior to inclusion. Fifty children were randomly selected from the same classes as the indexed GAD or ODD patient attended, and then matched on gender. All pupils in the classes were asked to participate as non-patient control and the research collaborator responsible for the screening of the non-patient controls selected the pupils based on a list of names provided from the teachers before the screening interviews commenced. Six families refused to participate and two families moved to another city before the interviews commenced. The final non-patient school control sample consisted of 42 children (84% of those ascertained).
Measures
Assessment of psychiatric status
Childhood mental disorder was assessed in accordance with the DSM-IV criteria for axis I diagnosis. Structured clinical interviews were conducted by the three therapists at the child and family guidance clinics who referred the child to treatment and to the primary investigator. Interviews were validated by an independent assessor who viewed and evaluated videos of all of interviews using a paired-rater design. The kappa values for the presence of ODD, GAD and no disorder were 0.93, 0.84 and 0.88, respectively. Children were also asked about difficulties related to friends, school, family disruption and their general adjustment.
Assessment of psychosocial situation
Retrospective assessment of psychosocial stressors for the six months preceding assessment for GAD and ODD were obtained at the time of the clinical interview from each of the 85 participants and their mothers. Interviews were semi-structured interview specifically designed by the WHO to cover the psychosocial situations included in the ICD-10, Z-codes classification for children and adolescents [14]. The rating of the psychosocial situations was also part of the diagnostic evaluation. The ICD-10 classification of psychosocial situations is as follows:
abnormal intra-familial relationships (e.g. parental hostility or conflict),
parental mental disorder,
distorted or inadequate intra-familial communication (lack of support and empathy),
abnormal qualities of upbringing (abuse, harassment, injurious parenting practices),
abnormal immediate environment (overprotection, inadequate control and parental pressures),
acute life events (loss, physical abuse, experiences carrying threats for the child),
societal stressors (persecution, discrimination, migration),
interpersonal stress associated to school/peers/teacher (conflicts or general unrest at school) and
stressors resulting from the child's disorder (institutional upbringing, removal from home, adverse events resulting in loss of self-esteem).
Three levels of severity were defined: (0) not present, (1) sub-threshold and (2) definitely present [16].
The inter-rater reliability of each of the nine psychosocial codes was based on the scores made by the primary investigator and the independent assessor (range 0–2). The intra-class correlations were 0.64 (distorted intra-familial communication), 0.69 (abnormal immediate environment), 0.74 (abnormal intra-familial relationships), 0.77 (stressful events related to disability/disorder), 0.78 (familial mental disorder), 0.79 (interpersonal stress related to school), 0.8 (societal stressors), 0.81 (abnormal qualities of upbringing) and 0.82 (acute life events).
Ethics
Written informed consent to participate in the study was obtained from one or both of the parents and verbal informed consent was obtained from the children. The National Data Inspectorate and the Regional Committee for Ethics in Medical Research (Norway) approved the protocols for this study.
Statistical analysis
Chi-square tests and Mann-Whitney tests were used to compare GAD, ODD and non-patient control children on demographic characteristics. A between-groups ANOVA was performed for categories of psychosocial situations. Analyses were performed using Statistical Package for the Social Sciences (SPSS, Version 15.0, Chicago: SPSS Inc.)-General Linear Model (GLM); weighting cells by their sample size was done to adjust for unequal sample sizes between the groups.
Multigroup discriminant function analysis (MDA) was performed in SPSS and used to look for unique combinations of psychosocial stressors capable of distinguishing GAD, ODD and non-patient control children. MDA is a suitable method given the multivariate nature of interaction between several risk factors and outcome. This technique combines independent variables that classify groups, and is the most appropriate approach to assess which factors are the best indicators of separation between the groups of children. The multigroup version of discriminant analysis is used when the dependent variable has three or more categories. This statistical technique can identify the most powerful sets of contrasts between clusters of variables on a data-driven basis, and the results can be used to visually represent the position of groups relative to each other in a discriminant space. The MDA analysis is not adversely affected by unequal sample sizes of the groups. The sample size provided adequate power for performing a MDA analysis [17].
Results
The sample comprised 58% boys and 42% girls with a mean age for the total group of 10.2 years old (SD = 1.3). The mean age for the three separate groups was 9.9 years old for the GAD group, 10.1 years old for the ODD group and 10.3 years old for the NC group.
As shown in Table 1 the groups were similar in terms of age, distribution of race, parental marital status (married, divorced, widowed) and level of family income (high, moderate, low), although there was a tendency for lower family income in the ODD group (p < 0.09). There were more boys in the ODD (83%) group compared to the GAD group (48%) (p = 0.02), but little difference in gender distribution between the GAD group and the NC group (p = 0.72).
Demographics of the children in the ODD group, GAD group and the non-patient control group (NC)
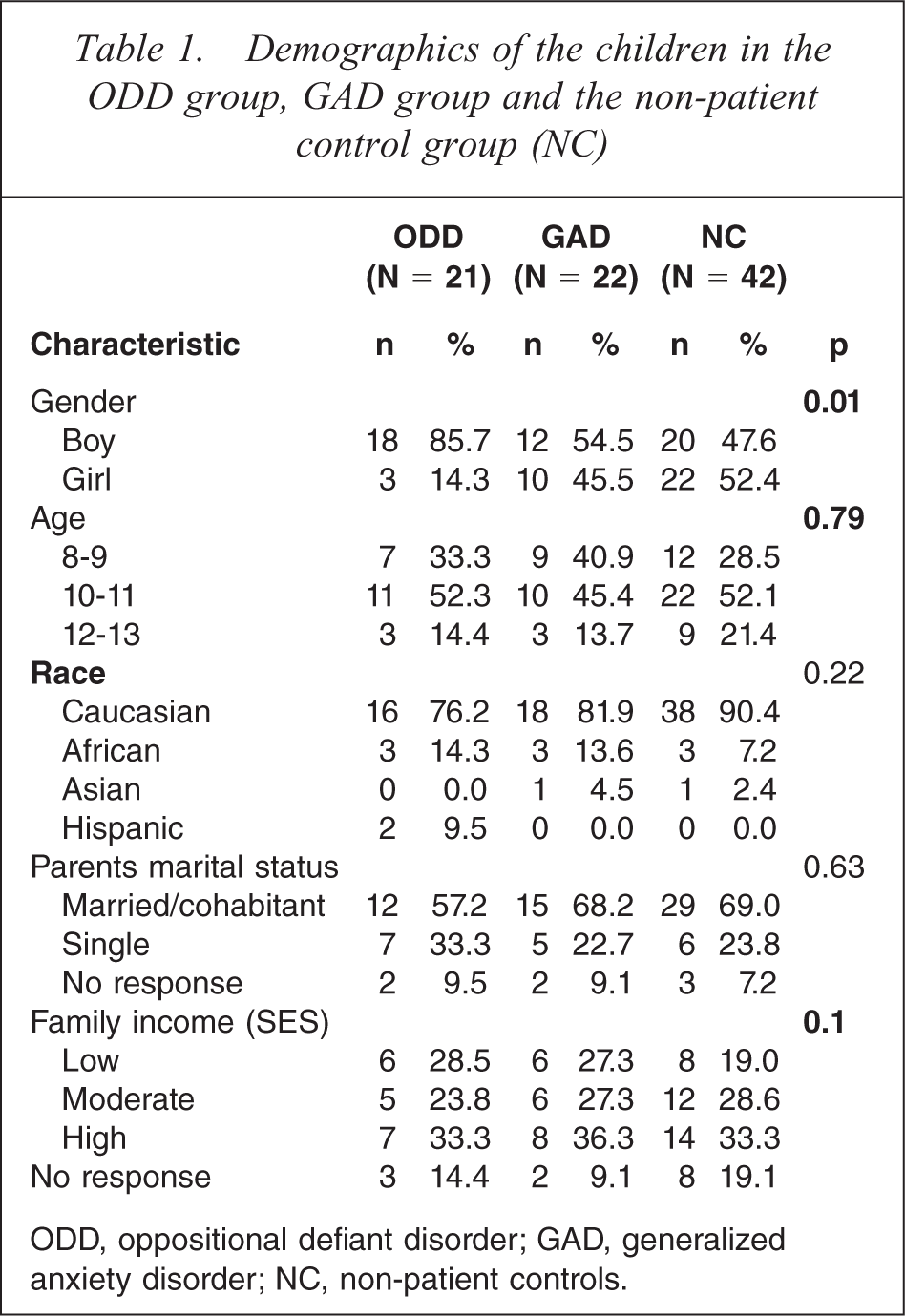
ODD, oppositional defiant disorder; GAD, generalized anxiety disorder; NC, non-patient controls.
Table 2 shows the mean scores for psychosocial situations and standard deviations (SD) in the three groups. For abnormal intra-familial relationships, there was a significant difference between the groups (F(2.82) = 29.68, p = 0.001). This dimension is characterized by lack of warmth in the parent–child relationship, physical child abuse, hostility towards the child and discord among parents. Sheffe post-hoc tests revealed that there were clear differences between the ODD and GAD groups (p < 0.001), but not between GAD and NC groups.
Means and standard deviations of psychosocial stressors for the three subject group
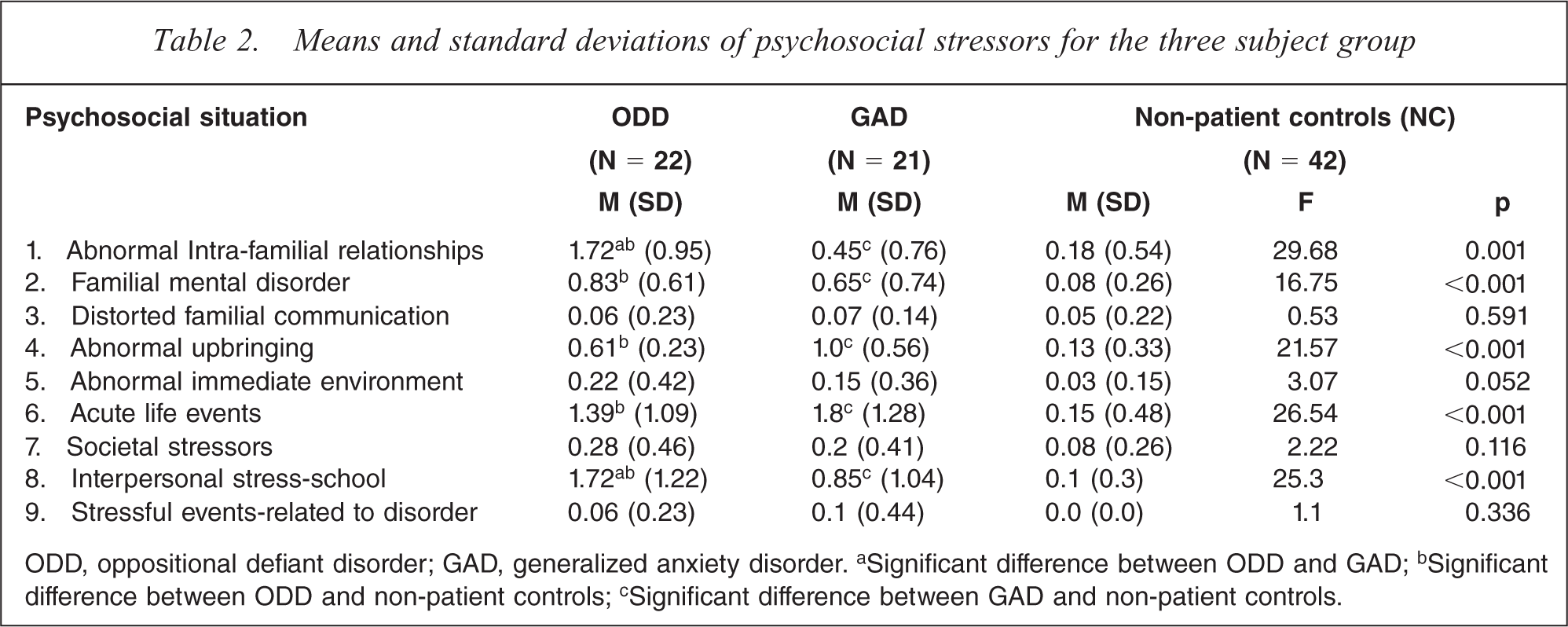
ODD, oppositional defiant disorder; GAD, generalized anxiety disorder. aSignificant difference between ODD and GAD; bSignificant difference between ODD and non-patient controls; cSignificant difference between GAD and non-patient controls.
A main effect of differences between the groups was also found for parental mental disorders (F(2.82) = 16.75, p < 0.001). Sheffe post-hoc tests confirmed this effect in GAD (p < 0.001) and ODD groups (p < 0.001) compared to the NC group, yet found no evidence for differences between GAD and ODD groups.
Abnormal upbringing is an index that includes parental overprotection, inadequate parental supervision or control, and parental pressures. There were large overall differences in this factor across the three groups (F(2.82) = 21.57, p < 0.001). Post-hoc tests revealed that there were no significant differences between ODD and GAD groups and that these groups were clearly different from the NC group (GAD p > 0.001; ODD p < 0.004).
Acute life events, an index measuring altered patterns of relationships, traumatic experiences, abuse, loss and sudden removal from home, differed among the three groups (F(2.82) = 26.54, p = 0.001). Here the GAD and ODD groups differed greatly from the NC group (p < 0.001), whereas little difference between ODD and GAD groups (p = 0.376) were found.
Finally, interpersonal stress related to school also differed between the groups (F(2.82) = 25.3, p < 0.001); post-hoc tests showed that the ODD group experienced highest distress compared to GAD (p< 0.006) and NC (p<0.001), and GAD clearly higher than the NC (p<0.005) group. There were no relevant differences between the groups on the other psychosocial stressors scales.
Next, a MDA was performed to examine whether combinations of the ICD-10 defined psychosocial situations could distinguish GAD, ODD and NC groups. The predictors were the nine categories of ICD-10 psychosocial situations and the dependent variable was group. No cases were identified or defined as multivariate outliers. On the basis of univariate tests, potential discriminating variables were identified. Two significant discriminant functions were derived: function 1 (Wilks’ lambda Λ = 0.162, χ2 (18) = 129.25, p < 0.001), and function 2 (Wilks’ lambda Λ = 0.473, χ2 (8) = 53.2, p < 0.001).
Table 3 shows the correlation matrices between the two discriminant functions and each of the predictors. The canonical correlations for functions 1 and 2 were r = 0.811 and 0.726, respectively.
Correlation between discriminant functions of psychosocial situations and each of the psychosocial situations for the three subject groups
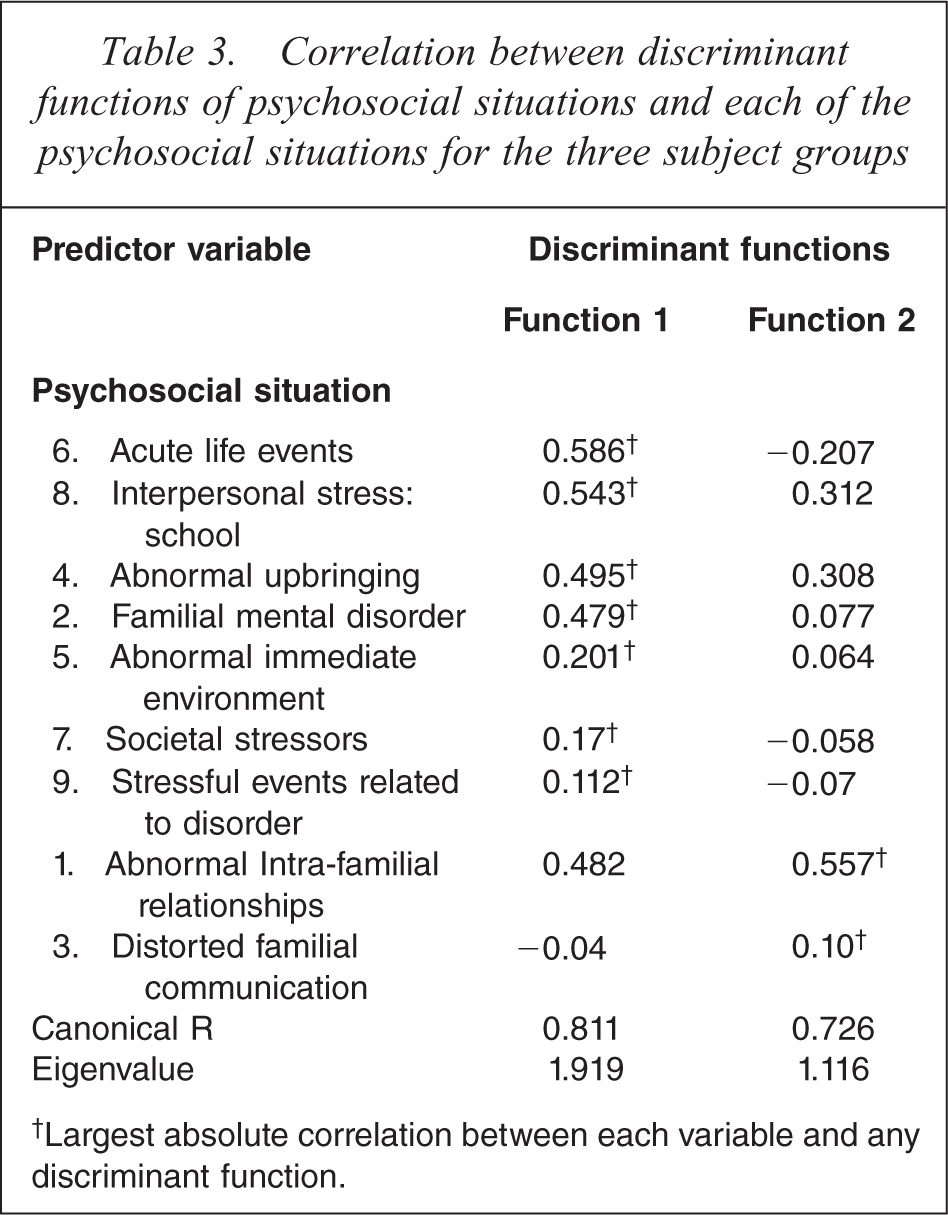
†Largest absolute correlation between each variable and any discriminant function.
The two discriminant functions accounted for 63% (function 1) and 37% (function 2) of the between-group variability. Function 1 contrasted high versus low levels of life adversity and interpersonal stress, while function 2 was more complex; it contrasted parental hostility, abuse and conflict in the high end versus parental overprotection in the low end. The group centroids were plotted as a perceptual map to provide a visual representation of the group differences (Figure 1). As shown in Figure 1, function 1 (high versus low levels of adverse events and interpersonal stress) separated the non-patient controls from the ODD and GAD groups, whereas function 2 (hostility/abuse versus overprotection/control) maximally separated the ODD group from the GAD group. Here the NC group was located in the middle, which is a more healthy position of counterbalancing the positive loadings (abuse/hostility) and the negative loadings (overprotection). Univariate ANOVAs followed by post-hoc tests (Fischer's LSD) showed that GAD and ODD differed from NC on function 1 (p < 0.001) and that GAD and ODD differed from each other on function 2 (p < 0.001).
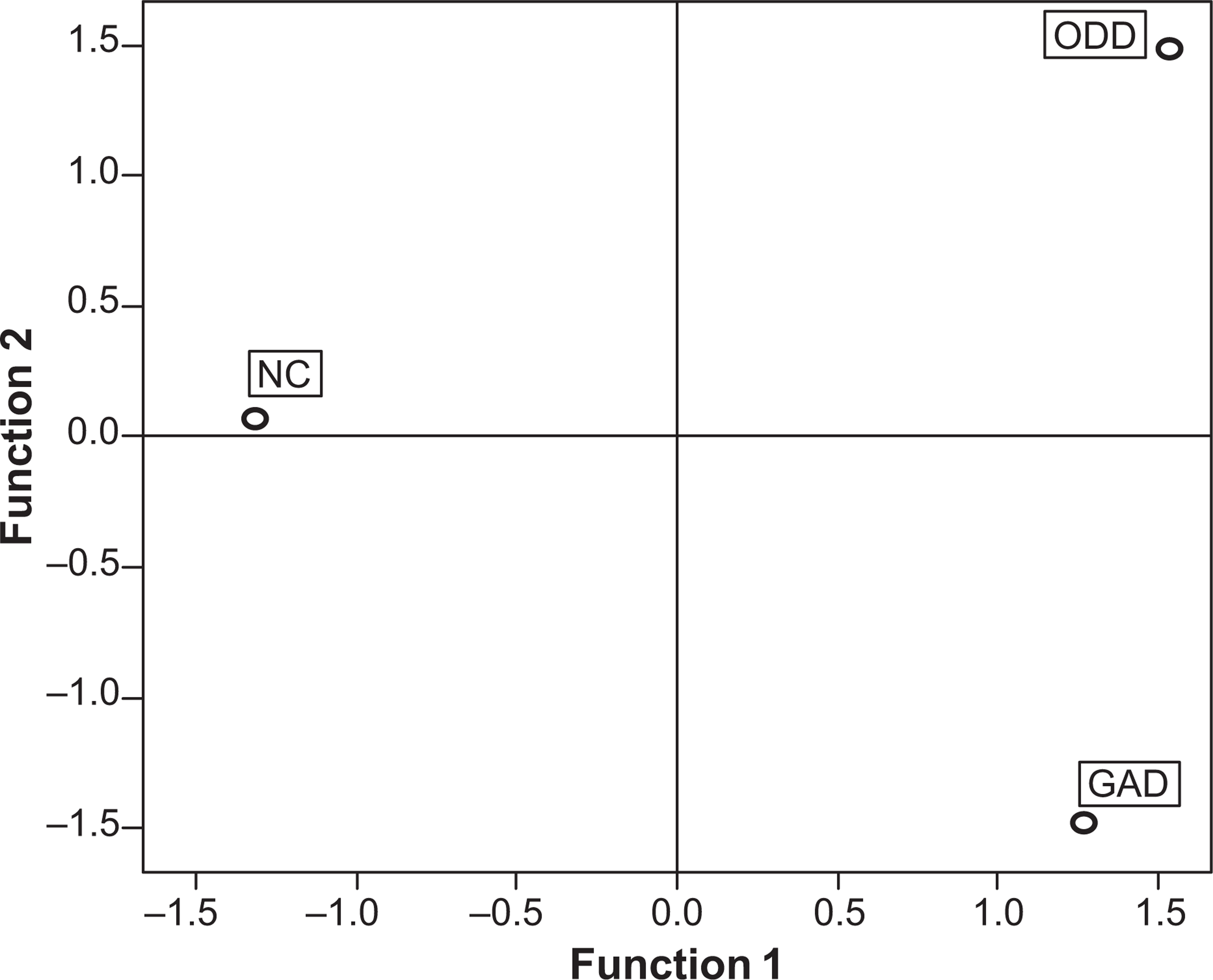
Plots of three group centroids on two discriminant functions derived from clinically rated psychosocial situations. Function 1 represents high vs. low levels of adverse events and interpersonal stress. Function 2 contrasts parental hostility, abuse and conflict in the high end versus parental overprotection in the low end.
Using the classification procedure on the entire sample of 85 children, 89.7% of all grouped cases in the total sample were correctly classified, in contrast to 35.9% correctly classified by chance alone. The relative improvement over chance index (RIOC index) was rather large, and demonstrated that the combination of the two functions of psychosocial situations were powerful discriminators between GAD, ODD and NC.
Discussion
In general, this study shows that childhood GAD and ODD are both characterized by higher levels of psychosocial stressors and life adversity than found in non-patient school controls. More specifically, childhood ODD was associated with abusive child–parent relationships and discordant relationships with teacher/school and/or peers. In contrast, childhood GAD was associated with parental overprotection, parental pressures, inadequate supervision/control and acute threats.
The results of this study have important applied implications. A more refined understanding of the unique risk profile for GAD and ODD allows better targeting of at-risk populations as well as better alignment of resources for prevention of disorder. Greater specificity also has the capacity to focus treatment strategies (where prevention fails) as well as tailoring engagement of patients and families with the most appropriate health services more broadly.
Our results are similar to those from a prospective study of 7-year-old children by Maziade et al. [18] who found that difficult temperament predicted psychiatric status, in particular ODD, but only when stress related to family function was taken into account. The same was found in a large co-morbidity study of 643 youths with ODD [19] where it was reported that the ODD group was found to have significantly greater family and social dysfunction relative to the control group. Both these studies support the present finding that ODD is related to multiple factors, but in particular abnormal parental functioning.
A crucial element is the level of hostility, irritability and abuse in the families of children with ODD. We found that specific factors such as abuse, hostility and intra-familial conflict seem to be highly predictive of psychosocial stressors linked to children with ODD. Irritable and difficult temperamental features of the parents combined with a coercive, irritable/explosive type of parenting may be involved in the maintenance of ODD. It has been suggested that parent–child incompatibility based on behavioural characteristics of both the parents and the child creates the adverse climate in the intra-familial situation [13].
The results of our study indicate that the parental influence on children with GAD may be characterized by being overprotective, controlling and over involved. The same observation has been reported in other studies [6–8]. In addition, we found that children with GAD report higher levels of threatening experiences and acute negative life events, which are adverse psychosocial factors not specifically linked with ODD. Parental influence on children with anxiety disorder was clearly demonstrated in another study showing that parents with anxious children were more supportive and reinforcing of avoidant behaviour than parents of children with ODD or non-patient controls [20].
Similarly, findings were observed in a study of 74 families of children with anxiety disorders by Manassis and Hood [21]. In this study, psychosocial adversity predicted functional impairment in children with GAD but not in children with other anxiety disorders. The finding of greater acute stress associated with GAD is interesting when considering that these children may be sensitized to danger and, in connection with overprotective parenting, may learn the utility of anticipating threat as a means of coping. This would fit with a newer model of GAD [22] in which patients hold erroneous beliefs about the usefulness of worrying, but eventually come to see the worry process as dangerous.
A previous study of this sample [23] showed that parental mental disorder was more common among children presenting with ODD and GAD than children in the non-patient classroom control group. This is consistent with Frick et al. [24] in that in their study of 177 children, antisocial personality disorder and/or substance abuse by one or both of the parents were the strongest predictors of ODD and conduct disorders in children aged 7 to 13. However, the link between parental mental disorder and psychological effects on offspring has been unclear in most cases, with no established relationship between a specific parental disorder and mental disorder in offspring [25]. A possible exception may be anxiety disorders. These disorders tend to aggregate within families, yet even so, there does not seem to be a direct transfer of the same type of anxiety disorder from parents to their offspring [2]. It is important to emphasize that aggregation of any disorder within a family does not necessarily indicate heritability as common genes are confounded with common environment [26].
To our knowledge, this is one of the first studies to examine the specific relationships between dimensions of psychosocial stressors and internalizing (GAD) and externalizing (ODD) childhood psychopathology. The study had a carefully diagnosed sample of children with no or very low level of co-morbidity. The high level of homogeneity in the sample was a crucial aspect in order to assess the context of psychosocial stressors linked to the specific disorder. Further, there was a high inter-rater reliability both in the DSM-IV diagnoses and the psychosocial stressors in the assessment of both children and mothers.
Certain limitations of our study need to be addressed. First, diagnoses and psychosocial situations were assessed by the same assessors, which could contaminate and inflate the association between these two sets of data. Thus, the risk of type 1 error cannot be ruled out. Nevertheless, the ICD-10 psychosocial situations were assessed by a standardized structured interview where the child and the parents were asked the same questions and two independent assessors evaluated the answers. This procedure makes potential contamination between the assessments of diagnoses and psychosocial situations less likely to occur.
Second, psychosocial situations preceding the clinical interview were assessed retrospectively at the time of the clinical interview. Thus, ratings of psychosocial stress could be influenced by memory recall bias. Furthermore, ratings of psychosocial stress may be inflated by the concurrent ratings of symptoms, disorders and psychosocial situation. Lack of temporally separate data therefore precludes strong causal inferences about relationships between psychosocial situations and childhood mental disorders in this study.
Third, the generalizability of the discriminant functions should be cross-validated to test the utility of the coefficients for other samples. This could be done by splitting a sample, then deriving classification in one group and testing them on the other group. Another way to do this is to derive the classification functions from a sample at time 1 and retest them at time 2. However, none of these approaches were feasible for the present study [17].
Fourth, the non-patient classroom controls were not fully assessed on the DSM-IV criteria, but screened on GAD and ODD criteria with an additional interview with the teachers. Thus, there is a possibility that some of the non-patients could have had high levels of symptomatic distress related to other disorders than GAD and ODD.
Finally, there were significant differences in the distribution of gender in the three subject groups, which could have biased the results. A post-hoc analysis was conducted to compare the results of only the boys in the three subject groups: 18 boys in the ODD group, 12 in the GAD group and 20 in the NC group. Although the statistical power was lower by excluding half of the sample, the main findings were upheld and indicated that the distribution of gender did not account for the between-group variability.
Conclusion
Specific dimensions of the ICD-10 psychosocial situations seem to be specifically associated with GAD and ODD in children. This ICD-10 classification scheme could therefore contribute to better understanding of, differentiation between and treatment of some of the most prevalent childhood psychiatric disorders. This is a feasible method of assessment that could help health care workers outside specialist settings plan health care services and prevention at an early stage. This is particularly important in the light of the recent recommendations from the National Institute for Health and Clinical Excellence (NICE, 2005), which state that the first step in primary care should be to detect and act on psychosocial risk in the child's environment.
Footnotes
Acknowledgements
We thank our colleagues at the child guidance clinics for help with the screening and referrals of all the patients.