
Abstract
Keywords
There is considerable evidence showing that disruptive disorders are more common among dysfunctional families and in environments with high levels of chronic adversity [1–7]. However, less is known about differences in family environment according to specific diagnosis within the disruptive group: attention deficit hyperactivity disorder (ADHD), oppositional defiant disorder and conduct disorder. This requires clarification because of the implications for our understanding of the nature of these common and troubling conditions and for their treatment.
Most of the available data about the association of the disruptive disorders with family environment pertain to patients with oppositional or conduct disorder. These data are difficult to interpret because reports rarely separate the two disorders. Oppositional defiant disorder and conduct disorder are conceptualised in most studies as being part of a single dimension of behaviour [2]. By and large, patients with these disorders grow up in disorganised, deprived, conflictive families more often than those without these conditions [2–6].
The potential contributory effect of psychosocial factors in the aetiology of ADHD has been largely ignored by researchers [7] while our personal experience suggests that, by and large, practitioners in child and adolescent psychiatry believe that family disfunction contributes to the causation and/or exacerbation of ADHD behaviours. The scarce data available for ADHD suggest that hyperkinetic patients come from families who are no different from those without this disorder. Nevertheless, young people with ADHD are less responsive to parental commands and parents tend to relate to them in a more controlling and critical fashion than to those without this condition [8,9]. It has been argued that these interactions may increase the likelihood of hyperkinetic children developing oppositional defiant disorder or conduct disorder during adolescence [10]. Family adversity has been associated with persistence of ADHD symptoms [11] and with increased comorbidity and impairment in these children [12].
This report presents further evidence on the differences in family environment between adolescents with ADHD, oppositional defiant disorder and conduct disorder in a group of clinic-referred patients. It was hypothesised that: (i) adolescents with ADHD would have a poorer family environment than those without; (ii) patients with oppositional defiant disorder and conduct disorder would have a worse family environment than those with ADHD only; and (iii) youth with ADHD exposed to a poorer family environment would show higher rates of conduct disorder. Because most of the research in this area is based on male subjects, we specifically sought to include a similar number of females. It was expected there would be no differences in family environment according to gender.
Method
Subjects
Patients for the study were randomly selected from a large group of children and adolescents assessed at the Rivendell Unit, Sydney, Australia, between 1983 and 1997. Because the main aspect of the study was to examine the influence of family environment on adolescents with ADHD, a balanced group of patients of both sexes with and without ADHD symptoms was identified. The basic criterion for selection was a high score (> 12, and therefore a high probability of ADHD) on a hyperactivity scale extracted from the Child Behaviour Checklist (CBCL) [13–15]. Each case was matched with another of the same gender and age but with low scores (< 6) on this scale and therefore a low probability of ADHD. Of the 247 cases thus selected, three were excluded because of inadequate information in the file and a further 14 because they were younger than 12 years.
Diagnosis
Diagnosis, which followed DSM-IV criteria, was made by three experienced clinicians (JMR, GW and JMP) using all the information in the clinical file. Clinicians were blind to group membership and CBCL scores. Information in the file was comprehensive and included a variety of self-report measures, information from other agencies and schools, and a detailed report of the assessment interview [16]. Each clinician rated about one-third of the cases. Reliability estimates from a random 20 files rated by the three clinicians were acceptable (kappa for ADHD, conduct disorder and oppositional defiant disorder was 0.77, 0.64 and 0.78 respectively).
Measures
Quality of the family environment was estimated using the Global Family Environment Scale (GFES) [17]. The GFES seeks to measure the adequacy of the environment in which a child was reared. This encompasses the family's ability to provide physical and emotional care, secure attachment relationships, consistency and appropriate, non-punitive limit setting. Ratings reflect the lowest quality of the family environment for a period of at least 12 months prior to the age of 12 years. The GFES ratings have good test–retest and interrater reliability [17]. Following review of the file, clinicians made GFES ratings of each patient. Average agreement among raters, based on the 20 files mentioned, was adequate (r = 0.91).
Other measures included the following: the narrowband syndromes obtained from the CBCL and Youth Self-Report (YSR) [13]; ratings of socioeconomic status (SES) according to Australian norms [18]; and Global Assessment of Functioning (GAF) ratings [19]. Follow-up data were also available for 142 (61%) patients. These included involvement in delinquent activities, alcohol or drug abuse, admission to a psychiatric facility, residential treatment in a non-psychiatric institution, and response to stimulant medication in the cases in which it had been prescribed.
Statistical analysis
When possible, parallel analyses were performed using clinicians' DSM-IV diagnosis and scores on CBCL syndromes. This was done because: (i) there is no definite evidence to show that categorical diagnosis is better than dimensional classification, particularly in the disorders of interest [7,20]; and (ii) DSM-IV criteria for conduct disorder excludes a comorbid oppositional defiant disorder diagnosis, although many patients have symptoms of both disorders. Using CBCL-derived syndromes allowed us to take into account the presence of both syndromes. There is evidence that the CBCL ‘attention problems’ scale has good convergence with DSM-III-R ADHD [14,21], and the ‘aggressive’ and ‘delinquent’ syndromes with oppositional defiant disorder and conduct disorder, respectively [15,22].
Categorical variables were analysed using a chi-squared test, dimensional data were analysed using a t-test (two-tailed) and Pearson's correlation. Hierarchical logistic regression and ANOVA were used to statistically control for comorbidity and other confounding factors (age, gender, SES). Alpha was set at 0.05. Reported percentages are rounded to the nearest unit.
Results
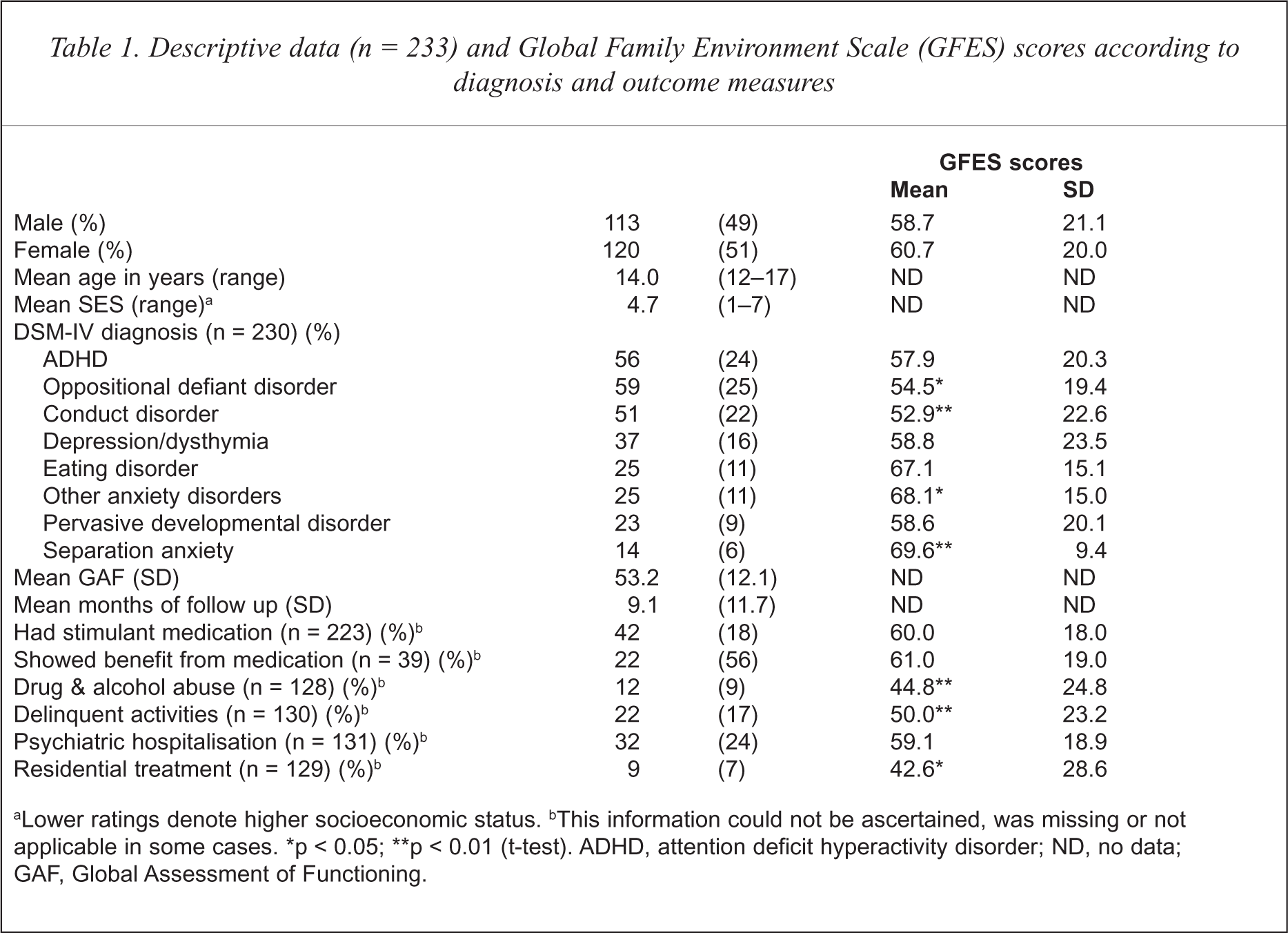
The number of patients included in the study was 233. Although the group was balanced according to sex, only 15 (27%) of the 56 adolescents diagnosed with ADHD were female. Age, gender, diagnosis and other descriptive data are presented in Table 1. Results can be summarised as follows: (i) ratings of family environment did not vary according to gender; (ii) adolescents with a DSM-IV diagnosis of oppositional defiant disorder or conduct disorder had a poorer family environment (lower GFES ratings) than those without; (iii) patients with diagnoses of separation anxiety and other anxiety disorders had better family environments (higher GFES ratings) than those with other disorders; (iii) among the follow-up data, family environment was worse in individuals who abused alcohol or drugs, were involved in delinquent activities or who had been admitted to a non-psychiatric facility. Multivariate analysis (hierarchical logistic regression) replicated the finding that GFES ratings did not vary according to gender, after controlling for the effect of age, SES and diagnosis.
Descriptive data (n = 233) and Global Family Environment Scale (GFES) scores according to diagnosis and outcome measures
Lower ratings denote higher socioeconomic status.
This information could not be ascertained, was missing or not applicable in some cases.
p < 0.05;
p < 0.01 (t-test). ADHD, attention deficit hyperactivity disorder; ND, no data; GAF, Global Assessment of Functioning.
Disruptive disorders and family environment
There were significant negative correlations between GFES scores and parent ratings in the aggressive (r = −0.31), delinquent (r = −0.33) and attention problems (r = −0.26) scales of the CBCL. Correlations were also significant with youth ratings (r = −0.21, −0.29 and −0.22 respectively). This showed that the poorer the family environment, the higher the scores on these behavioural dimensions. However, only the correlation between GFES scores and parent- or adolescent-reported delinquent scale remained significant when the confounding associations between the aggressive, delinquent and attention problems scales were statistically controlled (partial r = −0.15, p <0.05, for parent report; partial r = −0.18, p < 0.05, for adolescent report).
When using DSM-IV diagnoses, hierarchical logistic regression analyses showed that GFES scores made a significant contribution to the predictability of conduct disorder after taking into account the effect of age, sex, SES and other diagnoses (chi-squared = 7.8, df = 1, p < 0.01). The interaction between ADHD and GFES scores did not increase the probability of conduct disorder. A similar result was obtained in relation to oppositional defiant disorder (chi-squared = 4.0, df = 1, p < 0.05). However, GFES scores did not contribute to the predictability of ADHD. In summary, multivariate analyses showed an association between poor family environment, conduct disorder and oppositional defiant disorder, but not ADHD.
Family environment, psychosocial functioning and outcome
Global Family Environment Scale scores were associated with psychosocial functioning, as measured by the GAF (r = 0.36). This persisted after taking into account the associations between GAF scores and CBCL scale scores (partial r = 0.24, p < 0.01). That is, subjects rated as having a better family environment were also likely to be given higher ratings of psychosocial functioning.
Multivariate analyses (
Discussion
Caution must be exercised in the interpretation and generalisation of these results because of several methodological shortcomings. First, patients were clinically referred, and thus the sample was potentially biased in a number of unknown ways. Second, this is a cross-sectional study, although some longitudinal data were available in a proportion of the cases. Third, diagnoses were not made using a structured interview. On the other hand, test–retest reliability and diagnostic agreement obtained by other researchers with various structured interviews [23,24] were no better than those in this study. It is important to keep in mind also that GFES ratings do not necessarily reflect the family environment at the time of assesment, but the lowest quality of the family environment for a period of at least 12 months prior to the age of 12 years.
There was no difference in family environment, as measured by the GFES, between patients with and without ADHD. By contrast, family environment was poorer among referred adolescents with conduct and oppositional disorders. This is irrespective of whether conduct disorder was diagnosed according to DSM-IV criteria or based on parent or youth questionnaires. A poorer family environment in patients with ADHD did not result in a higher likelihood of conduct problems. This is inconsistent with the results of Biederman
Quality of the family environment was associated with later psychosocial functioning. Lower GFES ratings, reflecting a poorer environment, were associated with an increased likelihood of admission to a non-psychiatric institution and drug and alcohol abuse, after taking into account the effect of age, gender, SES and diagnosis. This reinforces the belief that a poor family environment has lasting effects in a variety of domains, not just mental disorder.
Conclusions
Poor family environment, as determined by the GFES, is not associated with ADHD in this group of patients. Rather, a worse family environment is specifically associated with conduct disorder, oppositional defiant disorder and poorer functioning. The findings lend support to the view that interventions that target parenting in the early years of life and support families at risk may prevent the development of conduct disorder problems and improve psychosocial functioning.