
Abstract
Objective:
This study examined whether the diminished treatment response previously reported for children with conduct problems and high levels of callous-unemotional (CU) traits is evident when these traits are indexed using multi-informant data collected from mothers, fathers, and teachers. It also tested whether treatment outcomes associated with CU traits are independent of overlap between CU traits and autism spectrum disorder (ASD) symptoms.
Method:
Diagnostic data on oppositional defiant disorder (ODD) severity were collected pre-treatment (time 1) and at 6-month follow-up (time 2) in a sample of children (N = 95; 67 boys, 28 girls) aged 3–9 years with clinic-referred conduct problems and comorbid symptoms in a range of diagnostic domains. Time 1 measures of CU traits and ASD symptoms were tested as predictors of time 2 ODD severity using structural equation modeling, with multi-informant ratings of CU traits modeled as a single latent variable.
Results:
Compared to children with low levels of CU traits, those with high levels exhibited more severe ODD symptoms at follow-up (β = 0.33, SE = 0.08, p < 0.05), after controlling for pre-treatment severity, socio-economic status, other demographics (age, gender), and parameters of treatment (number of treatment sessions, medication status). Although CU traits and ASD symptoms were positively correlated, ASD symptoms showed no association with change in ODD severity from pre-treatment to follow-up. Likewise, the association between CU traits and ODD outcomes held when controlling for covariation between CU traits and ASD symptoms.
Conclusions:
Our findings replicate previous evidence that CU traits are uniquely associated with poor clinical outcomes among children treated for conduct problems, and show for the first time that this association is not accounted for by symptoms of ASD.
Introduction
There is growing support for the subtyping of childhood conduct problems based on high versus low levels of callous-unemotional (CU) traits (i.e. a lack of guilt and empathy). This is seen in the proposed introduction of a specifier for CU traits to the diagnosis of conduct disorder (CD) in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) (Frick and Moffitt, 2010). The proposed revision is based in part on evidence that the conduct problems of children with high levels of CU traits are more severe than those of children without CU traits, and are less responsive to established interventions (Hawes and Dadds, 2005; Waschbusch et al., 2007). Although proposed for the diagnosis of CD, this effect has, however, been reported primarily in children diagnosed with oppositional defiant disorder (ODD) (Hawes and Dadds, 2005) and attention deficit hyperactivity disorder (ADHD) (Waschbusch et al., 2007). Given the implications of this issue for clinical practice, the impact of CU traits on treatment response was identified as a priority focus in the research agenda outlined by the DSM-5 advisory committee for disruptive behavior disorders (DBDs) (Moffitt et al., 2008). Research into the treatment outcomes associated with CU traits has since grown and has indicated that parent training interventions may contribute to reductions in the CU traits of young children (Hawes and Dadds, 2007; McDonald et al., 2011). However, research regarding the effects of such interventions on the conduct problems of children with CU traits remains limited and has produced mixed findings (Haas et al., 2011; Kolko and Pardini, 2010; White et al., 2012).
The first study to directly examine the association between CU traits and the treatment outcomes of children with DBDs was reported by Hawes and Dadds (2005). In a sample of boys diagnosed with ODD (n = 56; aged 4–8 years) who completed a 10-week parent training program, those with the highest baseline levels of mother-reported CU traits were the most likely to retain diagnoses of ODD at a 6-month follow-up. The association between CU traits and poor behavioral outcomes was independent of baseline ODD severity and parents’ adherence to the intervention, according to observational data collected in the home setting. Waschbusch and colleagues (2007) reported a similar effect in a sample of children (aged 7–12 years) diagnosed with ADHD plus either ODD or CD. High levels of multi-informant-rated (parent and teacher) CU traits were associated with poor response to behavioral therapy during an intensive 8-week day camp program. In a follow-up study that incorporated this earlier sample, Haas and colleagues (2011) showed that CU traits uniquely predicted poor response to social skills and problem-solving components of this program, and negative behaviors during time-out.
Somewhat contradictory findings were reported by Kolko and Pardini (2010) in a study of children aged 6–11 years treated for ODD/CD. The authors of this study found that the most robust predictor of long-term diagnostic outcomes and youth-reported delinquency was the ODD dimension of hurtfulness. This is one of three dimensions of ODD symptoms (along with irritability and headstrong) that have been shown to differentially relate to broader profiles of psychopathology in population-based child research (Stringaris and Goodman, 2009a, b). Longitudinal data indicate that this dimension specifically – indexed by the single ODD symptom often spiteful or vindictive – may be a marker for proactive aggression and callousness (Stringaris and Goodman, 2009a). Seemingly at odds with this, CU traits per se were not found by Kolko and Pardini (2010) to be associated with poor treatment outcomes.
Such mixed findings highlight the need for further research in this area. Importantly also, while intervention research has demonstrated that effects associated with CU traits are not accounted for by comorbid ADHD (Hawes and Dadds, 2005; Waschbusch et al., 2007), the possibility that these effects may be explained by comorbid symptoms of autism spectrum disorders (ASD) – which share phenotypic overlap with CU traits (Rogers et al., 2006) – has not been tested. In recent years, growing research has focused on the relationship between CU traits and ASD, both of which have been conceptualized as empathy disorders (Jones et al., 2010). While research indicates that the specific behavioral profiles and cognitive/affective deficits associated with CU traits and ASD may be quite distinct, some overlap between these disorders is apparent in relation to social dysfunction and emotion processing (e.g. Blair, 2008). Not only is comorbidity between ASD and DBDs often seen in clinic-referred populations, it has also been shown that CU traits may co-occur with ASD in some individuals in a so-called double hit (Rogers et al., 2006). As all treatment outcome studies examining CU traits have excluded children with pervasive developmental disorders (including autistic disorder and Asperger’s syndrome), none of these studies have reported data on the overlap between CU traits and the symptoms of ASD in treatment-seeking families. An important next step for research into the effects of CU traits on treatment outcomes is to examine whether such effects are distinct from those that may be attributable to ASD.
The primary aim of the current study was to examine the effects of CU traits on diagnostic treatment outcomes in children referred for conduct problems. Behavioral parent training programs based on social learning theory meet the criteria for a well-established treatment for children with oppositional behavior (Ollendick and King, 2007). A range of such programs have been manualized and disseminated, including that used in the current study (Dadds and Hawes, 2006). Of the studies that have examined treatment response among children with conduct problems and high levels of CU traits, only two have examined follow-up diagnostic outcomes (Hawes and Dadds, 2005; Kolko and Pardini, 2010). These studies both share potentially important limitations related to the measurement of CU traits and the examination of these traits in relation to other dimensions of child psychopathology. First, both of these studies were limited by single-informant measurement of CU traits, relying on either parent (Hawes and Dadds, 2005) or teacher reports (Kolko and Pardini, 2010). This approach is at odds with assessment guidelines that suggest that multi-informant data may be particularly important to the reliable measurement of CU traits (Frick and Moffitt, 2010). In the current study, CU traits were indexed using multi-informant data provided by mothers, fathers, and teachers.
It is important to note that studies of childhood CU traits have varied considerably with respect to the measurement of the construct. The most commonly used measure of CU traits has been the Antisocial Process Screening Device (APSD) (Frick and Hare, 2002), as used in the studies by Haas et al. (2011), Kolko and Pardini (2010), and Waschbusch et al., (2007). Although there is not yet definitive evidence regarding the most effective method for measuring CU traits (see Kotler and McMahon, 2010), various adaptations of the APSD reported in measurement research have been found to improve on the psychometric properties of the original measure. One such adaptation is that described by Dadds et al. (2005), which was the measure used to collect mother reports of CU traits in the treatment study by Hawes and Dadds (2005). This measure was also used in the current study to collect the multi-informant data on CU traits.
A further aim was to examine whether treatment outcomes associated with CU traits are independent of overlap between CU traits and ASD symptoms. To investigate this, we examined the response to parent training within a real-world clinical sample of children referred for conduct problems and comorbid symptoms in a range of diagnostic domains. First, we hypothesized that CU traits would predict the diagnostic severity of ODD symptoms 6 months following the completion of treatment, while controlling for pre-treatment severity, socio-economic status, and parameters of treatment (medication status, number of sessions). Second, we hypothesized that the relationship between CU traits and diagnostic treatment outcomes would be independent of effects associated with the comorbid features of ASD.
Method
Participants
Participants were referrals to a mental health clinic that specializes in the treatment of child and family problems in Sydney, Australia. Inclusion criteria included child age (from 3 to 9 years) and a primary diagnosis of ODD symptoms. Comorbid DSM, fourth edition (DSM-IV) diagnoses were admitted. A total of N = 95 children (67 boys, 28 girls) were included in the sample (age M = 5.4, SD = 1.9). This gender distribution is comparable to that of previous studies in this research area (Haas et al., 2011; Kolko and Pardini, 2010). Clinically significant symptoms of ASD, as indexed by the Diagnostic Interview Schedule for Children, Adolescents and Parents (DISCAP) (Holland and Dadds, 1997) were evident in 7.5% of cases. Clinically significant symptoms of two disorders were diagnosed in 42% of the sample, while 7% were diagnosed with clinically significant symptoms of three disorders. The highest rates of comorbidity were seen in the diagnostic categories of anxiety disorders (20%) and ADHD (18.9%). Participants in receipt of stimulant medication for behavioral problems (at either pre-treatment or follow-up) represented 10.5% of the overall sample. Participants in receipt of other forms of medication comprised 2.4% of the sample, with the most common of these being antihypertensive and corticosteroid medications. The sample was drawn from a larger project investigating developmental/biological correlates of childhood conduct problems and overlaps with the sample previously reported on by Dadds and colleagues (2011); however, no treatment outcome data have previously been reported for this sample.
Measures
Child diagnoses and symptom severity
The DISCAP (Holland and Dadds, 1997) was used to formulate DSM-IV (American Psychiatric Association, 1994) diagnoses at pre-treatment and 6-month follow-up. This semistructured interview both assigns diagnostic status and quantifies the severity of diagnostic features, thereby providing both categorical (i.e. diagnosis/no diagnosis) and continuous (i.e. symptom severity, 0–6) data. Diagnostic reliability was evaluated for approximately 30% of interviews by having a team of psychologists/psychiatrists make an independent diagnosis while blind to the primary clinician’s formulation. Kappa agreement on primary and secondary diagnoses was 0.77 and 0.70 respectively.
Callous-unemotional traits
CU traits were measured using the scale developed by Dadds and colleagues (2005), comprising joint items from the APSD (Frick and Hare, 2002) and the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997). This joint APSD–SDQ scale has been extensively described and validated in previous research into CU traits (Dadds et al., 2005, 2006, 2009). The scale showed strong internal consistency across the multiple informants in the current sample, as demonstrated by Cronbach’s alphas for mother (α = 0.80), father (α = 0.79), and teacher (α = 0.88) ratings. The availability of CU traits ratings by the respective informants was as follows: mothers 96%, fathers 74%, teachers 80%.
Autism spectrum disorder symptoms
The Social Responsiveness Scale (SRS) (Constantino et al., 2003) is a well-validated 65-item measure of ASD symptoms in the domains of social impairment, social awareness, social information processing, capacity for reciprocal social communication, social anxiety/avoidance, and autistic preoccupations and traits. The validity of the SRS has been supported in genetic linkage studies of ASD (Duvall et al., 2007), and strong convergence between parent and teacher reports on the measure has been demonstrated (Constantino et al., 2007). Mother reports on the SRS were used in the current study.
Procedure
Permission to conduct this research was obtained from the University of New South Wales Human Research Ethics Committee, and informed consent was provided by parents and youth at the time of recruitment. Parents and children completed all measures at time 1 as part of pre-treatment clinical assessment and provided permission for teacher reports to be collected from schools at this time. The diagnostic severity of ODD was reassessed 6 months following the completion of treatment (time 2), by a clinician who was blind to time 1 data.
Parent training intervention
Treatment consisted of the fully manualized parent training program published by Dadds and Hawes (2006), in which parents are trained in social learning-based strategies for effectively reinforcing positive child behavior (e.g. descriptive praise) and setting limits on antisocial behavior (e.g. time-out). These foundation strategies are supplemented with components that target parent/systemic problems (e.g. couples discord, parental anger/depression), and consultation processes designed to maximize therapeutic engagement with families distressed by conduct problems. This widely disseminated program has a long evidence base, with response rates shown to be generally consistent with those reported for well- established parent training interventions for conduct problems (Dadds et al., 1987; Hawes and Dadds, 2005). The intervention commenced with a 1.5-h assessment session with the parents, followed by a child observation session and nine weekly 1-h sessions. Interventions were delivered on an individual basis with families, by psychologists with at least a 1-year experience in the treatment of children and families. Where indicated, medication was prescribed and monitored by a consulting psychiatrist. Cases were discussed in weekly supervision meetings attended by therapists on the project to ensure that treatment integrity was maintained. The average number of sessions attended by the parents was 5.22 (SD = 1.71), with those who dropped out retained in an intention-to- treat design. As reported in Table 1, the number of treatment sessions attended was not associated with any other study variables.
Descriptive statistics and correlations among key study variables.
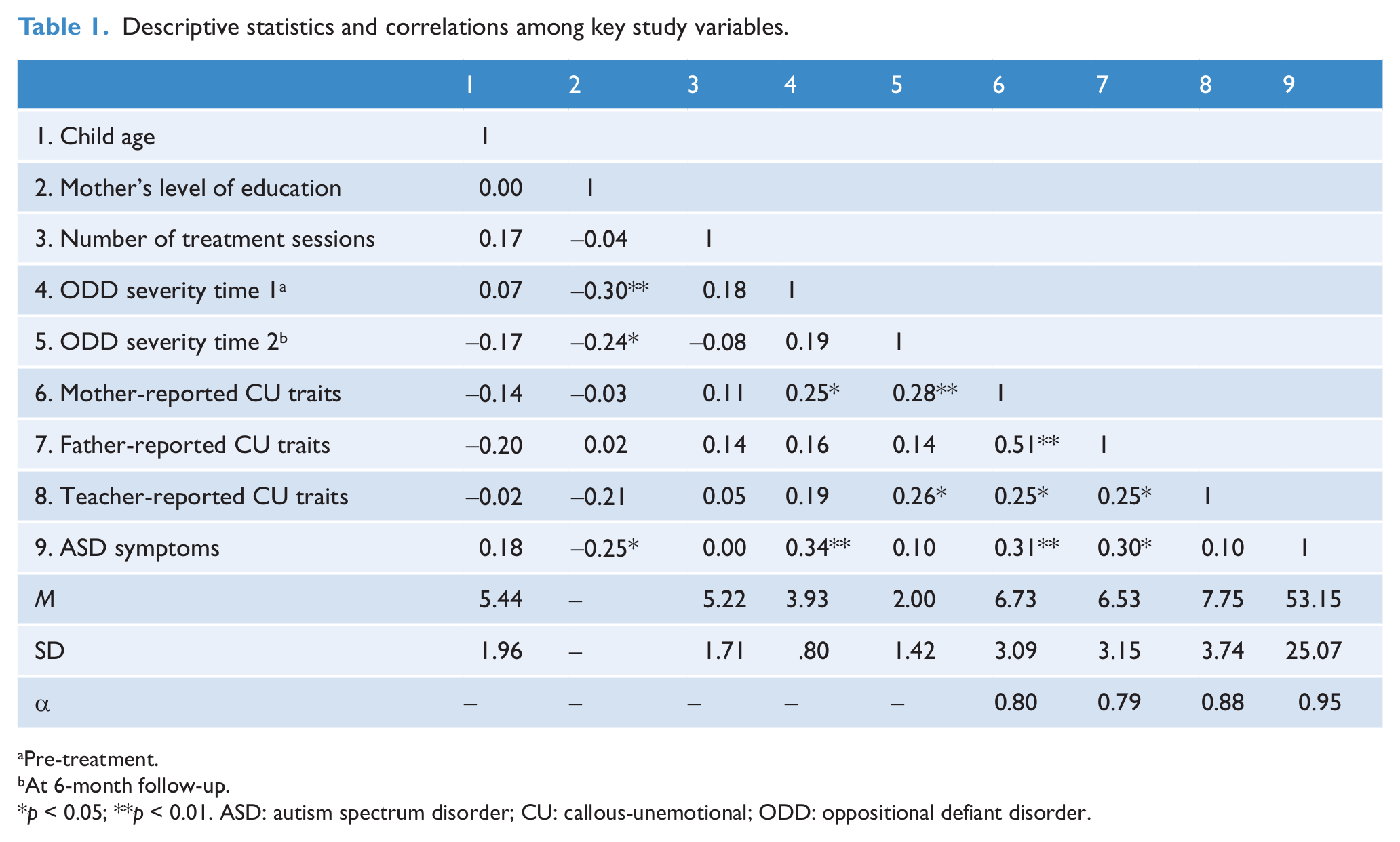
Pre-treatment.
At 6-month follow-up.
p < 0.05; **p < 0.01. ASD: autism spectrum disorder; CU: callous-unemotional; ODD: oppositional defiant disorder.
Results
The ratings of child CU traits provided by mothers, fathers, and teachers at pre-treatment indicated moderate to strong agreement across informants. Correlations between multi-informant ratings ranged from r = 0.26 (p < 0.05) for father and teacher ratings, to r = 0.51 (p < 0.01) for mother and father ratings. Time 1 severity of ODD symptoms was correlated significantly with mother-reported CU traits (r = 0.25, p < 0.05) and severity of ASD symptoms (r = 0.34, p < 0.01). Severity of ODD symptoms at time 2 was correlated with presenting levels of CU traits as rated by mothers (r = 0.28, p < 0.05) and teachers (r = 0.26, p < 0.05). Severity of ASD symptoms was correlated significantly with child CU traits as rated by mothers (r = 0.31, p < 0.01) and fathers (r = 0.30, p < 0.05). Neither mother, father, nor teacher ratings of CU traits differed significantly between participants with and without clinically significant ASD symptoms (p > 0.05 for all t-tests). The mother’s level of education – used to operationalize socio-economic status – was found to be associated with ODD symptom severity at both time 1 (r = -0.30, p < 0.01) and time 2 (r = -0.24, p < 0.05), and was therefore included as a covariate in all analyses.
Prediction of treatment outcomes
The association between CU traits and time 2 severity of ODD symptoms was examined with maximum likelihood estimation using SPSS Amos for Windows, version 20 (IBM Corporation, Armonk, New York, USA). This allowed us to model multi-informant data on CU traits as a single latent variable representing the variance shared by the reports of each informant (mother, father, teacher). The data provided by each informant contributed significantly to this latent variable, with standardized beta weights ranging from β = 0.33 (p < 0.05) for teacher reports, to β = 0.81 (p < 0.01) for mother reports.
To examine the prediction of change in ODD symptom severity between time 1 and time 2, the unique association between multi-informant CU traits and time 2 ODD was tested while controlling for time 1 ODD symptom severity. An initial model was tested in which paths to time 2 ODD severity were drawn from multi-informant CU traits, time 1 ODD symptom severity, ASD symptoms, number of treatment sessions, child age, gender, and medication status, and mother’s level of education. All predictor variables were allowed to covary. The path between mother’s level of education and time 2 ODD severity was statistically significant (β = -0.23, SE = 0.18, p < 0.05), as was the path between multi-informant CU traits and time 2 ODD severity (β = 0.39, SE = 0.10, p < 0.05). Paths for ASD symptoms, number of treatment sessions, medication status, child age, and gender, were all non-significant, and therefore removed to improve model parsimony. The reduced model, shown in Figure 1, was found to fit the data well [root mean square error of approximation = 0.01; 90% confidence interval (CI): 0.00, 0.13; comparative fit index = 0.99; Tucker–Lewis index = 0.99]. The path between mother’s level of education and time 2 ODD severity in this model was statistically significant (β = -0.21, SE = 0.17, p < 0.05), as was the path between multi-informant CU traits and time 2 ODD severity (β = 0.33, SE = 0.08, p < 0.05). Beta coefficients for these paths and the variables comprising the latent CU traits variable are reported in Figure 1. Post-hoc tests showed that the path from CU traits to time 2 ODD severity remained significant when the multi-informant index of CU traits was replaced by mother reports of CU traits (β = 0.26, SE = 0.05, p < 0.05) and teacher reports of CU traits (β = 0.22, SE = 0.04, p < 0.05), but not father reports of CU traits (β = 0.15, SE = 0.05, non-significant).
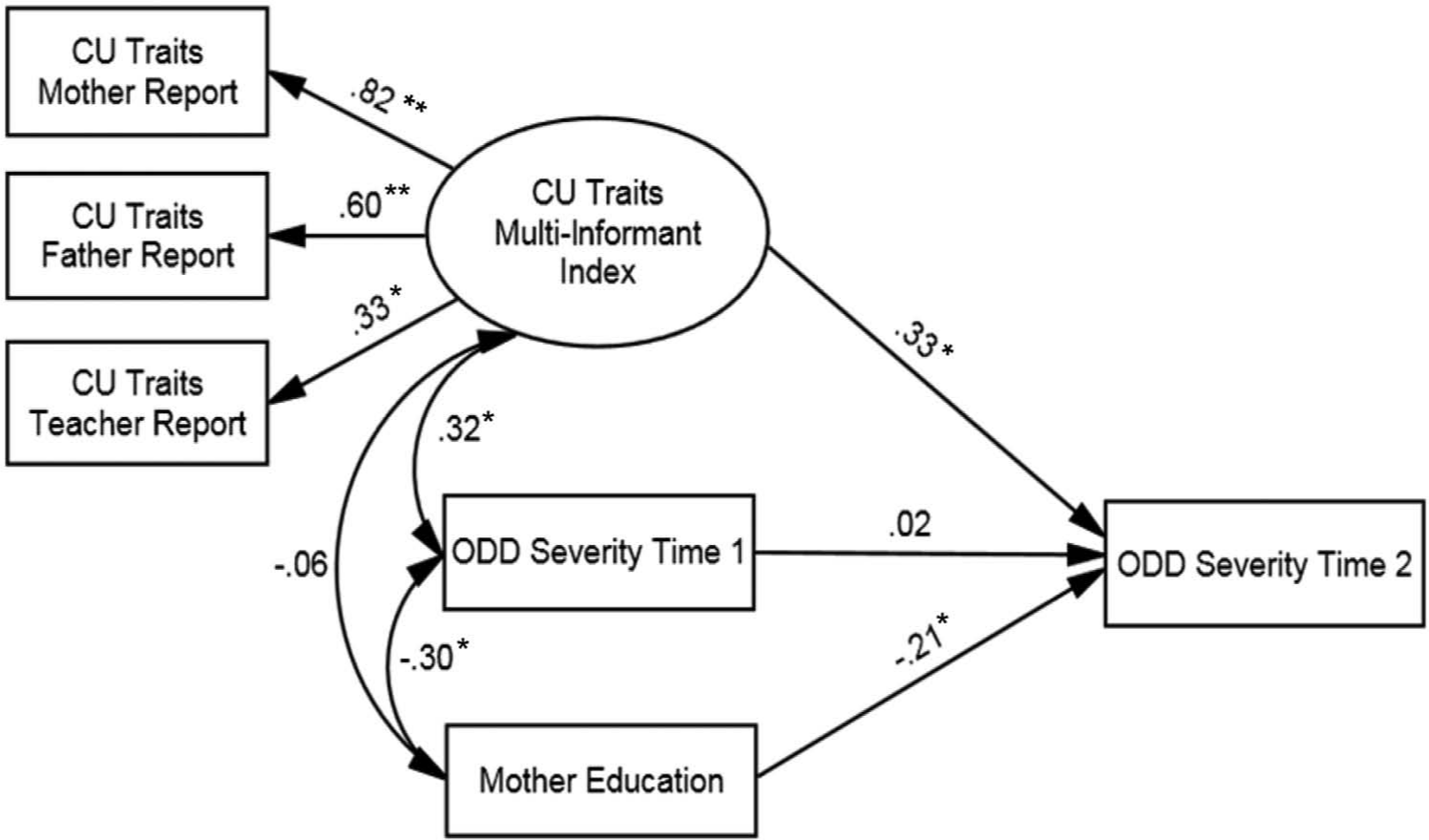
Final model displaying the standardized regression coefficients for paths between time 1 (pre-treatment) and 2 (at 6-month follow-up) variables. *p < 0.05; **p < 0.01.
Previous treatment studies have indicated that neither comorbid symptoms of ADHD nor anxiety disorders account for the poor treatment outcomes that have been associated with CU traits (Hawes and Dadds, 2005; Washchbusch et al., 2007). To check this in the current sample, post-hoc analyses were conducted in which diagnostic symptoms in these respective domains were added to the final structural equation model. The significant path from time 1 CU traits to time 2 ODD was unchanged when the model was run controlling for time 1 ADHD severity and time 1 anxiety severity. The path from time 1 ADHD to time 2 ODD was non-significant. However, a significant negative effect was found for the path from time 1 anxiety to time 2 ODD (β = -0.20, SE = 0.10, p < 0.05). As such, higher levels of anxiety at time 1 were significantly associated with lower levels of ODD at time 2, independent of the significant association between time 1 CU traits and time 2 ODD. This result is consistent with the previously reported finding that children with conduct problems and comorbid internalising problems benefit more from parent training than those without this comorbidity (Beauchaine et al., 2000).
Following examination of CU traits as a continuous dimension, descriptive statistics based on the grouping of participants according to high-/low-CU traits were examined to allow for interpretations related to clinically meaningful criteria. Based on evidence to suggest that approximately 35% of children referred for DBDs demonstrate what can be considered high levels of CU traits (Christian et al., 1997), participants scoring in the top 35% for CU traits in the current sample were categorized as high CU, and the remaining cases categorized as low CU. Following the recommendations of Frick and colleagues (2003) for combining multi-informant data on CU traits, the top 35% were identified by ranking cases based on the highest score they received across informants. The majority of participants with clinically significant ASD symptoms (71%) were classified as low CU. The examination of ODD (DISCAP) severity ratings according to these groupings indicated that among the low-CU group, 12% of the cases who exhibited diagnosable levels of ODD at time 1 maintained this full diagnostic status at time 2. In contrast, within the high-CU group approximately 27% of those children with diagnosable levels of ODD at pre-treatment continued to exhibit diagnosable levels of ODD at time 2.
Discussion
This study examined the association between childhood CU traits and diagnostic treatment outcomes following a parent training intervention for conduct problems. As predicted, children who presented with higher levels of CU traits exhibited more severe ODD symptoms 6 months following treatment than did those with lower levels of CU traits. This association between CU traits and diagnostic treatment outcomes was independent of pre-treatment symptom severity, socio-economic status, other demographics (age, gender), and parameters of treatment (number of treatment sessions, medication status). 1 Importantly, our demonstration of this effect using a multi-informant measurement strategy indicates that associations between CU traits and treatment outcomes are unlikely to be accounted for simply by other family risk factors that may covary with CU traits reporting error (e.g. negative maternal attributions about the child). Our results also provide initial evidence that this effect is unrelated to symptoms of ASD, which may be comorbid in children with CU traits. Although CU traits and ASD symptoms were significantly correlated in our sample, ASD symptoms showed no association with change in ODD symptom severity from pre-treatment to follow-up. Likewise, the association between CU traits and ODD outcomes at 6 months held when controlling for covariation between CU traits and ASD symptoms.
There may be numerous explanations as to why the current study – like that of Hawes and Dadds (2005) – found this effect, while other research has not (Kolko and Pardini, 2010). Although Kolko and Pardini (2010) and the current study both assessed CU traits using the APSD, the latter used an empirically derived revision of the measure (Dadds et al., 2005) more similar to that used in previous research into the heritability of CU traits (Viding et al., 2005). This measure of CU traits may perhaps be more closely related to the dimension of hurtfulness, which Kolko and Pardini (2010) did find to be a robust predictor of long-term treatment outcomes. Importantly, this hurtfulness dimension – indexed by the single ODD symptom often spiteful or vindictive – has previously been conceptualized as a marker for callousness (Stringaris et al., 2009a). Additionally, compared to the parent-focused intervention examined in the current study, that examined by Kolko and Pardini (2010) included both parent-focused and child-focused formats. Given that CU traits have been shown to moderate the association between negative parenting practices and conduct problem severity (Oxford et al., 2003; Wootton et al., 1997; Yeh et al., 2011), CU traits may serve to reduce the extent to which parenting targets translate into child behavior change; conversely, involving children more directly in treatment may in part serve to overcome this effect.
Our findings present two noteworthy implications for the proposed introduction of a CU traits specifier to the diagnosis of CD in the DSM-5. First, by replicating our previous finding that children with conduct problems and high levels of CU traits benefit less from standard parent training intervention than those who are free from these traits, the current data add considerable weight to the notion that CU traits may inform prognostic formulation in the treatment of children referred for conduct problems. The inclusion of a CU traits specifier in the DSM-5 may be indicated on such a basis. Second, however, our findings add to the growing evidence that the predictive value of CU traits is by no means specific to children/adolescents with CD. There is now considerable evidence from research into the developmental course and correlates of CU traits to indicate that these traits are a marker for specific risk processes (including neurocognitive deficits) across a range of clinical populations (ADHD, ASD, CD, ODD), as well as in the absence of externalizing psychopathology (Viding and McCrory, 2012a). On this basis, calls have been made to consider CU traits a transdiagnostic marker (Rutter, 2012; Viding and McCrory, 2012b). The proposal to include CU traits only within the specific diagnosis of CD in the DSM-5 (Frick and Moffitt, 2010) is therefore at odds with this perspective. In any case, the findings of our intervention research to date suggest that the ODD diagnosis should not be excluded from DSM-5 revisions concerning prognostic indicators associated with CU traits.
A growing number of studies have reported evidence to indicate that the negative parenting practices targeted in parent training interventions are more proximal to the conduct problems of children with low levels of CU traits – the majority of referred children – than those with high levels of CU traits (Oxford et al., 2003; Pasalich et al., 2011; Wootton et al., 1997; Yeh et al., 2011). The findings from this study are consistent with the thesis that among children with high levels of CU traits, change in these parenting practices is less likely to translate into child behavior change than it is among low-CU children. Although very little is currently known regarding the precise treatment targets that may be most indicated in children with CU traits, there is some emerging evidence to suggest that among boys with conduct problems, those with CU traits benefit more from the addition of an emotion recognition empathy training component to standard parent training than those without CU traits (Dadds et al., 2012). The findings reported here highlight the need to prioritize research into such novel interventions that may better suit the unique needs of this high-risk subgroup.
It is important to note that while the conduct problems of children with high levels of CU traits may be less responsive than those of low-CU children to existing parent training interventions, the potential benefits of these interventions to children with CU traits should not be dismissed. Among the children with high levels of CU traits in the current study, the majority diagnosed with ODD at pre-treatment no longer met full diagnostic criteria at follow-up. Furthermore, aside from targeting conduct problems, previous studies indicate that parent training may be an effective means of reducing the expression of CU traits in young children (Hawes and Dadds, 2007; McDonald et al., 2011).
A number of limitations should be considered when interpreting the findings of this study. First, the research design used to assess the effects of the intervention did not include a control group. As such, it is difficult to differentiate individual differences in treatment response that are associated with CU traits from those that may be accounted for by other factors, such as maturation. Future research is needed in which control group designs are used to test the effects of CU traits on treatment response. Second, although the study examined child CU traits using mother, father, and teacher report data, other child variables were indexed using fewer informants. The SRS was completed by mothers only, while the DISCAP was conducted jointly with mothers and fathers, but not teachers. Third, it should be noted that relatively little is currently known about the developmental equivalence of the questionnaire items used to index CU traits in the current study. Future research testing invariance across age groups would be beneficial to determine whether the behaviors that reflect CU traits in middle childhood (e.g. breaks promises) do so to the same extent in early childhood. Finally, although the size of the current sample is significantly larger than some previous studies in the area (Haas et al., 2011; Hawes and Dadds, 2005), a larger sample may be needed to detect treatment effects related to some of the variables investigated here.
In conclusion, this study represents the first to use multi-informant data on child CU traits to examine their association with diagnostic outcomes following parent training for conduct problems. Our findings replicate previous evidence that CU traits are uniquely associated with poor clinical outcomes among children treated for conduct problems (Hawes and Dadds, 2005), and show for the first time that this association is not accounted for by symptoms of ASD. Our findings also add to the growing evidence that despite the relatively poor clinical outcomes among children with high levels of CU traits, the conduct problems of these children are far from untreatable.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.