
Abstract
When Anthony and Jansen [1] first reported that psychiatric symptomatology and diagnosis were poor predictors of future work performance for the mentally ill, it was inspiring to many in psychiatric rehabilitation. Their findings suggested that the vocational potential of mentally ill individuals should not be prejudged based on these factors. Indeed, it appeared that prior employment history was the best and most reliable predictor of future vocational performance along with work adjustment skills, ability to ‘get along’ or function socially with others, and ego strengths or self-concept. The Anthony and Jansen [1] review article had a significant impact on the development of psychiatric rehabilitation. First, it highlighted the importance of functional outcomes among people with schizophrenia; and, second, its findings had direct effects on the development of vocational interventions to help the mentally ill get and keep their jobs.
In 1984 there was little else that Anthony and Jansen [1] could say about what features of psychiatric illness might be relevant to rehabilitation because the discovery of how mental illness affects vocational functioning had to await developments in the study of psychopathology and functional impairment. Research along these lines continued and was enriched by more sophisticated models of the relationship between psychopathology and function that importantly included the distinction between positive and negative symptoms and the role of neurocognitive and social cognitive impairments. For instance, Bell, Tsang and colleagues [2] studied the relationship between cognitive impairments and rate of symptom improvement in a 26-week work therapy programme from 1998 to 2004. They found that logical memory was a significant predictor of symptom change and work performance. This implied that improvements in cognitive functioning might have an impact on both symptoms and work functioning.
In view of the rapidly growing body of knowledge, we published a review paper that summarized the consistent predictors of vocational performance of psychiatric patients based on 35 relevant studies from 1985 to 1997 [3]. Our review concluded that premorbid occupational functioning, work history, and social skills were consistent predictors. Symptomatology and diagnosis continued to be inconclusive as to their predictive power. Cognitive functioning and family relationships, although largely neglected by researchers, were found to be significant predictors. Since its release in 2000, this article has been frequently cited, in part because vocational rehabilitation has become a legitimate focus for community mental health centres serving individuals with severe mental illnesses [4–7]. A study on perceptions among psychiatric practitioners on remission and recovery in schizophrenia [8] found that more than half (62%) of the respondents endorsed ‘returning to work’ as the core element of recovery. Another study [9] reported that full recovery can only be achieved when a person holds a steady job. More importantly, studies have shown that most individuals with severe mental illness express a strong desire to work [10,11].
The study of predictors of vocational functioning in schizophrenia has also been important as clues to underlying mechanisms of illness that may explain social dysfunction more generally. In addition, the discovery of the predictive power of neurocognitive [12–14,15–18] social cognitive [19] and social skills [12,20–22] deficits has led to the development of interventions that target these deficits in the interest of improving vocational outcomes.
In line with the increasing interest in helping clients improve their employability, the volume of studies that examine predictors of vocational outcomes has continued to expand. There are two characteristic features of recent publications pertaining to vocational outcomes. The first is that cognitive function has received more and more attention. This may be due to the seminal article by Green (1996) [23] which linked neurocognitive abilities to functional outcome for people with schizophrenia which was subsequently supported by empirical studies [24–26]. Another change we observed in the more recent literature is an increase in the sophistication of statistical modelling such as path analysis (PA) and structural equation modelling (SEM) to reveal the direct and indirect contributions of multiple variables in relation to vocational outcomes [27–29]. Despite the availability of this body of new data, there have not been many comprehensive reviews on predictors of vocational outcomes since our own publication in 2000. From 2000, our search revealed six systematic reviews [30–35] on vocational rehabilitation and severe mental illness. However, all of these reviews have limitations and did not give a comprehensive account of vocational predictors for people with schizophrenia based on available information. Our present review thus fills the gap in the literature as we cover studies which were published from 1998 to 2008. Although meta-analysis has been widely used to pool effect sizes of Randomized Clinical Trials (RCTs) and come up with a relevant statistic which summarizes the effectiveness of a particular clinical intervention [36–43], there is to date no attempt to apply similar methods to the study of predictors. In this paper we employed the meta-analytical method using the generic inverse variance [44].
Method
Data searching and initial screening criteria
To collect literature pertaining to the significant predictors of vocational outcomes, a comprehensive electronic search was performed over the period from January 1998 to 2008 with computerized electronic databases (EBSCOhost, InterScience, Journals@Ovid, MEDLINE, MD Consult, PsycINFO, ScienceDirect, Science Citation Index/Social Science Citation Index), using the following keywords ‘schizophrenia’ or ‘mental illness’ or ‘psychiatric disability’ or ‘psychiatric disorder’ and ‘employment’ or ‘vocational outcome’ and ‘prediction’ or ‘predictors’. Studies were further filtered by visual inspection to avoid duplication of articles across different databases. A total of 439 articles (260 from MEDLINE, 120 from Science Citation Index and Social Science Citation Index, 10 from EBSCOhost, 6 from Science Direct, 7 from Journals@Ovid, 18 from MD Consult, 16 from PsycINFO, and 2 from Interscience) were extracted. A study was included in our meta-analysis if: (i) the majority (more than 50%) of the participants were diagnosed as suffering from schizophrenia by certified psychiatrists or by DSM-III, DSM-IIIR, or DSM-IV criteria; (ii) the theme was mainly on identification of predictors of vocational outcome; and (iii) the method was empirical and quantitative in nature. The study was excluded if it was a qualitative study. Following the above screening criteria, 72 articles (31 from MEDLINE, 22 from Science Citation Index and Social Science Citation Index, 9 from PsycINFO, 6 from EBSCOhost, 3 from MD Consult, and 1 from Science Direct) were selected for a detailed review at the second stage.
Second stage screening
At the second stage screening, two qualified reviewers with a Master's degree in clinical psychology or occupational therapy screened through all eligible studies and decided whether each of them should be included for data synthesis in the next stage based on the criteria below. As to methodology, at least one of the objectives was to identify significant predictors of vocational outcomes. The criteria for subject recruitment were clearly defined and the diagnosis of schizophrenia was valid. The assessments for employment status and correlation/predictor variables were validated. Finally, the assessment was performed by independent and qualified assessors. Regarding the criteria for data analysis, only studies using multivariate analysis such as logistic regression, multiple regression, MANOVA, path analysis, structural equation model, etc., on derivation of predictors were included [45]. In addition, we included studies which involved at least five subjects per predictor variable [46], had less than 20% attrition rate [47], and had a priori power analysis on sample size determination [48]. On the other hand, we excluded studies using proportional hazards models with hazard rate estimates quoted. The reason was that method for conversion of hazard rate to odds ratio (OR) was unavailable. If the same research group published more than one paper for the same purpose with the same population, only the most recently published article was included for review [46]. If the same research group published more than one paper with the same population but different purposes, all the papers were included.
After screening by the two raters, 53 articles were selected for extensive review and data synthesis. The concordance rate [49] between the two raters was 80%. After extracting the 53 articles, we found that some papers were missed because they might not be found by the keywords in the databases. Therefore, we supplemented the 53 articles with an additional 9 articles which are also relevant to our current review on predictors of vocational outcome for people with schizophrenia. A similar method was used in McGurk and Mueser's review article [33]. Eventually 62 articles were included in the systematic review. Figure 1 summarizes the screening process leading to the 62 studies for a detailed meta-analysis.
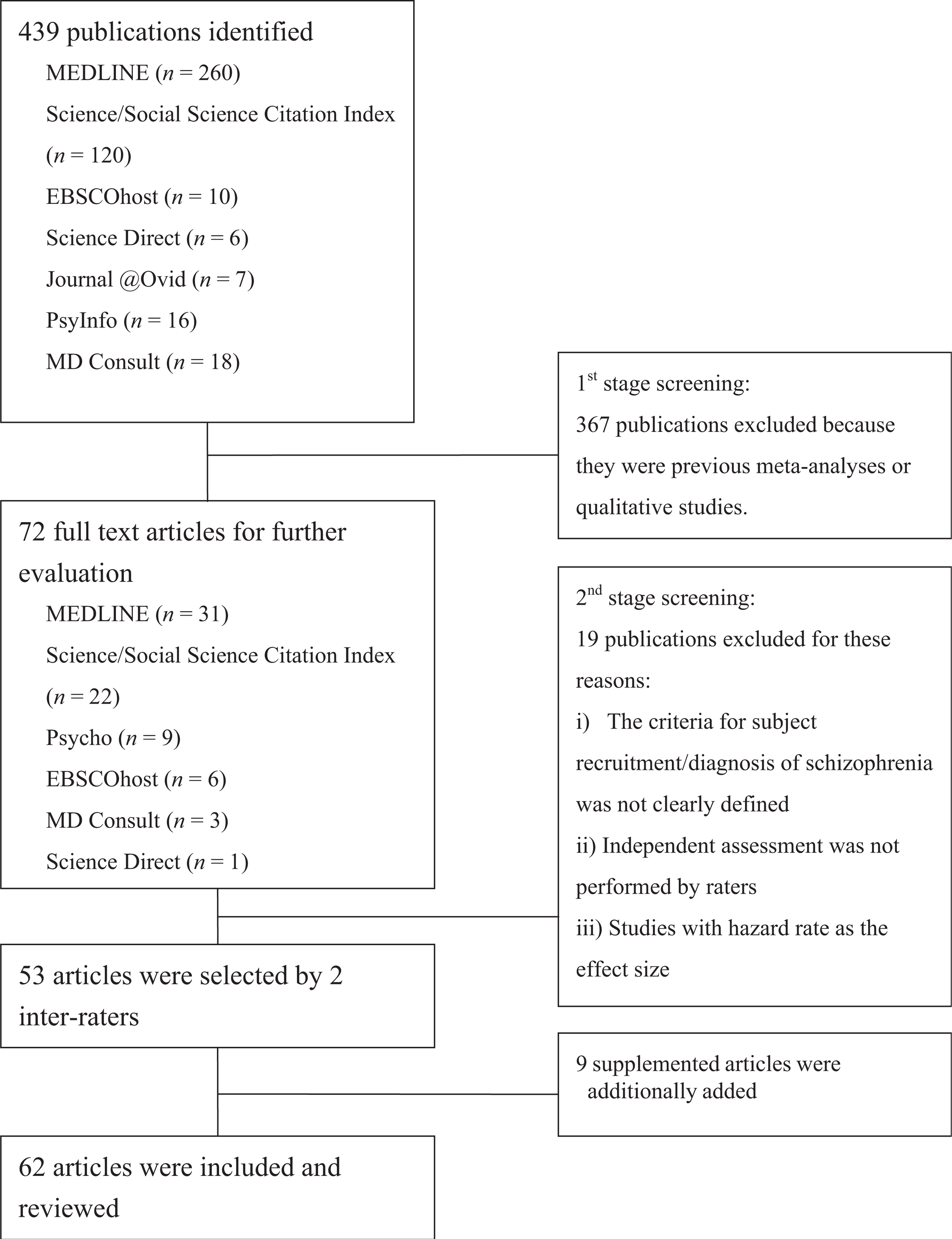
Flowchart of Review Articles Selection Process.
Data analysis
We used two methods for data analysis. First, we replicated the method we used in our earlier review [3] by frequency counts to summarize studies that reported whether an individual predictor was a significant predictor or not. Second, we conducted a meta-analysis on the 62 articles. As to meta-analysis, we aimed to transform the results from the 62 studies into a common metric so that statistical comparisons could be made across the predictors and outcomes [50]. Most studies that we reviewed used regression analysis for either continuous or categorical predictors. In studies involving continuous predictors, standardized regression weights (beta coefficients) were reported. In studies using categorical predictors, the most common effect size was reported as odds ratio. Based on Portney and Watkins [51], odds ratio is a measure of effect size defined as the ratio of the odds of an event occurring in one group to the odds of it occurring in another group. An odds ratio of 1 indicates that the condition or event under study is equally likely in both groups. An odds ratio greater than 1 indicates that the condition or event is more likely in the first group. On the contrary, an odds ratio less than 1 indicates that the condition or event is less likely in the first group. In this meta-analysis, we used odds ratios as the effect estimates for each study because of the ease of interpretation in applied settings and strong mathematical properties [52]. The odds ratio between each predictor variable and each vocational outcome for each study was estimated by cell counts in a 2 × 2 contingency table [53]. In some studies they were extracted directly from the articles without further computation. If odds ratios were not reported in a study, the following three methods were employed to transform the effect size information into a common odds ratio metric, making the results of the studies comparable across different analytical methods [50]. First, we transformed the correlation coefficient into odds ratio using the formula suggested by Digby (1983) [54] if the correlation coefficient estimates were given instead. Second, regression coefficients of predictor variables were converted into Pearson's correlation coefficients. If the results were based on logistic regression models, the regression coefficient of each predictor was converted into odds ratio by exponential transformation. Finally, 41 studies listing only the p-value of each predictor variable without mentioning the magnitudes for any type of effect or not providing results convertible to odds ratio were excluded from the meta-analysis.
Standard errors of the effect size estimates were computed either by conversion of the test statistic or by confidence interval. The test statistic was defined as the natural log odds ratio divided by its standard error [53] and was converted into p-values [51]. By proper transformations, the standard error of natural log odds ratios was obtained. Another way of estimating standard error of the effect estimate was utilization of the width of the individual 95% confidence interval [55]. In addition, the definition of the odds ratio across studies was standardized for directionality. Following these conversions, meta-analytic techniques were used to estimate the overall effect sizes of odds ratio [56]. Regarding the meta-analysis of each predictor on each vocational variable for all eligible studies, the generic inverse variance approach [57] was used to pool all individual effect size estimates for computation of the overall effect size estimates by assuming fixed-effect models with the use of Review Manager 4.2.9 (The Cochrane Collaboration, 2005) [55]. For study with two experimental groups [58], weighted average of correlations was used to obtain a single effect size. Along with this, studies with multiple predictor variables in a single conceptual domain, average across all the variables was computed to obtain the single effect size [59–63]. The pooled effect size estimate of each predictor on each vocational outcome was regarded as statistically significant if its 95% confidence interval did not cover the value of one. Furthermore, cognitive functioning was divided into three aspects (i.e. executive functioning and general intelligence, attention and working memory, and verbal and visual memory) so that cognitive tests could be pulled together for meta-analysis. Odds ratios of the scores of Wisconsin Card Sorting Test (WCST) and Wechsler Adult Intelligence Scale (WAIS) in predicting vocational outcomes were grouped for determining the effect size of executive functioning and general intelligence. Odds ratios of Trail Making Tests, Digit Span, and Repeatable Battery for the Assessment of Neuropsychological Status (RBANS)'s attention index were pooled for attention and working memory. Finally, the California Verbal Learning Test (CVLT), RBAN's immediate memory index, and RBAN's delayed memory index were pooled for verbal and visual memory.
Results
Categorization of predictors
The significant predictors identified from the 62 studies were grouped into 15 categories by the first and second authors (H.W.T.S. and A.Y.L.), with 100% concordance. The 15 categories were further broken down into 41 individual predictors. They were psychiatric symptomatology (positive symptom, negative symptom, general psychopathology), demographic characteristic (age, gender, education, ethnicity, marital status, socio-economic status), cognitive functioning, functional history and attitudes (premorbid functioning, attitude towards work, work adjustment skills, work history), substance abuse, public support/disability income (i.e. publicly funded disability support scheme such as a pension, etc.), rehabilitation services to restore community functioning and well-being by occupational therapists, psychiatrists, psychologists, social workers and mental health professionals, social features (social support and skills, psychosocial stressor), work income, family history, hospitalization history, emotion, intra-psychic functioning, medical features (medical condition or disability which refers to impaired body functions requiring medical attention, diagnosis, atypical antipsychotic medication, first generation antipsychotic medication, medication adherence, length of illness, duration of untreated psychosis, age of onset of illness, course of illness, remission) and others (duration of military service before admission, work quality, work habit, family functioning, family social economic status, therapeutic relationship, self-esteem).
Description of studies
Table 1 shows the number of studies that cited each of the predictors as significant or non-significant. Results show that cognitive functioning was the most intensively studied variable and received overwhelming support (N = 15) as a significant predictor. However, at the same time, seven studies reported it as a non-significant predictor. The next two variables that received much attention from the studies and were mostly cited as significant predictors included education (N = 12) and negative symptoms (N = 10). But these two predictors were simultaneously regarded as non-significant by seven and nine studies respectively. Social support and skills (N = 8), medical condition or disability (N = 8), work history (N = 7) and rehabilitation service (N = 7) were also reported as significant predictors. Five studies unanimously reported public support or disability income as a significant negative predictor. Twelve predictors (socio-economic status, premorbid functioning, work adjustment skills, family history, emotion, intra-psychic functioning, atypical antipsychotic medication, medication non-adherence, length of illness, duration of untreated psychosis, duration of military service before admission, and therapeutic relationship) received support from only one study as being significant.
Frequency counts of studies on significant or non-significant predictors
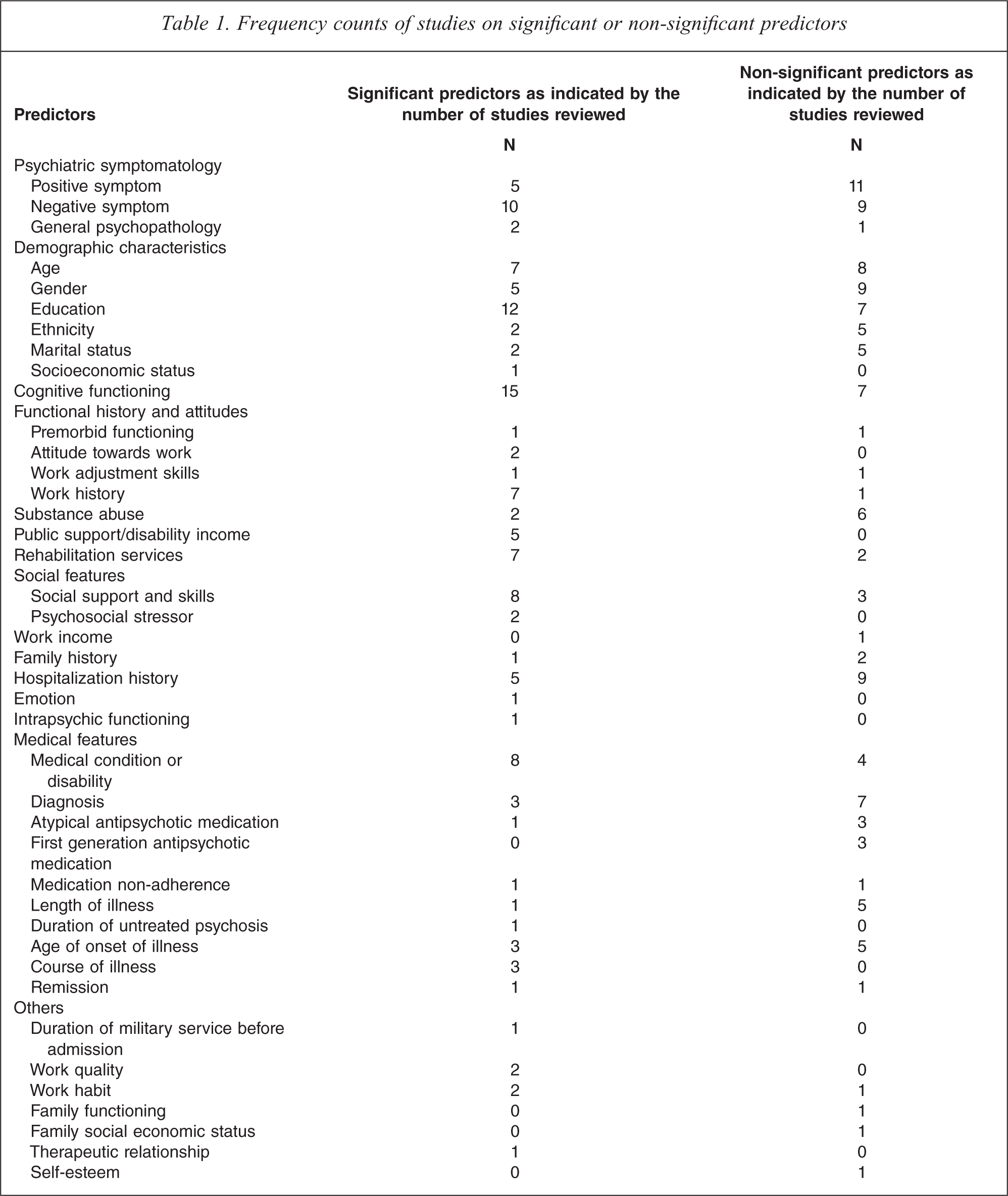
Positive symptoms (N = 11), diagnosis (N = 7) and substance abuse (N = 6) received the most support as non-significant predictors; but positive symptoms were regarded as significant predictors by five studies as well. Similarly, both gender and hospitalization had support from nine studies as non-significant and five as significant. Furthermore, ethnicity, marital status, length of illness, and age of onset all received support as non-significant predictors by five studies.
The most contradictory results were found in negative symptoms and age, they received similar support as significant (N = 10 for negative symptom, and N = 7 for age) and non-significant predictor (N = 9 for negative symptom, and N = 8 for age).
Meta-analysis
Table 2 shows the number of studies used and the results of the pooled effect size of the predictors. The effect sizes of studies with continuous predictors and categorical predictors are pooled separately. There were fewer studies that had the information required for inclusion in this form of analysis: 21 studies were included in the meta-analysis. Negative symptoms of age, education, marital status, work history, public support, diagnosis, and executive functioning and general intelligence were all significant predictors with the highest OR for marital status and diagnosis. Positive symptoms of gender, ethnicity, hospitalization history, attention and working memory, and verbal and visual memory were non-significant predictors.
Results of pooled analysis of outcome parameters
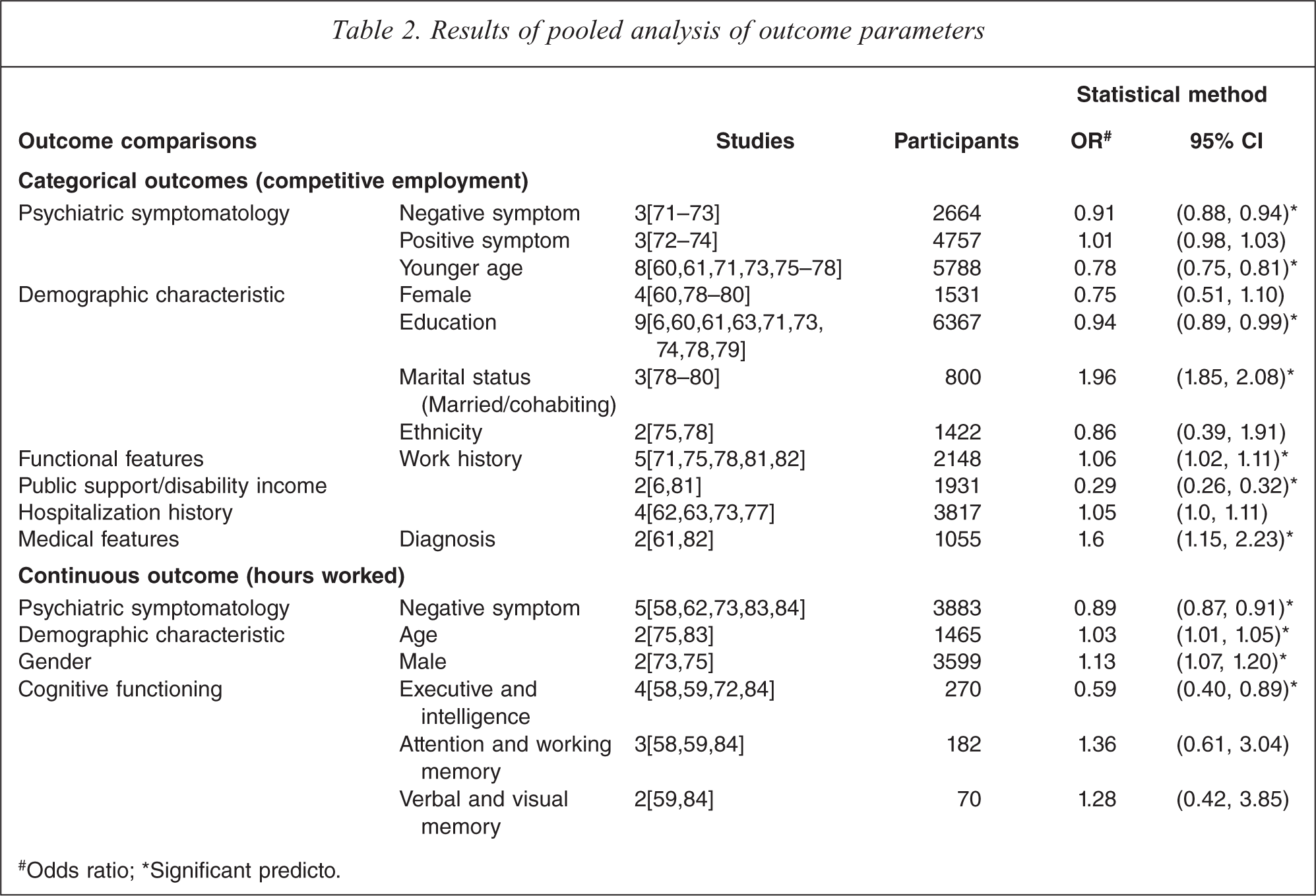
#Odds ratio; ∗Significant predicto.
Discussion
Our review of published research since 1998 has revealed continued refinement and development in the investigation of predictors. In particular there has been a surge of interest in the role of cognitive function. In contrast to our earlier report, results show that cognitive functioning was the most intensively studied variable, and it received overwhelming support (N = 15) as a significant predictor. Although all the predictors in the current review had general representation in the earlier literature, there was greater specificity, particularly in regard to distinguishing between negative symptoms and positive symptoms. Social factors that might be barriers to employment did not receive much attention, but five studies unanimously reported public support or disability income as a significant negative predictor. This reflects that people with mental illness who are on a publicly funded disability support scheme such as a pension scheme may predict poorer employment outcome. Psychological factors such as self-stigmatizing beliefs about their own mental illness, negative cognitions about themselves as workers and the absence of positive psychological factors [64] such as hopefulness and optimism are currently receiving some attention as predictors of social functioning in the context of the recovery movement, but they have yet to find their way into formal studies of predictors of vocational outcome.
This report provided two approaches to reviewing the literature. The frequency count of studies allowed us to include more studies and variables than was the case for the meta-analysis. However, the frequency count method only showed the number of studies of the significant and non-significant predictors instead of counting the number of subjects in a study corresponding to a predictor. The meta-analysis had the advantage of providing odds ratios, which made comparisons possible among variables; for example, marital status emerged as having the highest odds ratio, whereas work history had a significant but much smaller effect. We used both methods so that the readers may cross-check the results of each method. However, as both methods have advantages and limitations, cautions have to be made accordingly.
The meta-analysis for both categorical and continuous variables reported that cognitive functioning (specifically executive function and general intelligence), negative symptom, and age were significant predictors, which agreed with the frequency counts. Similarly, work history, education, and public support/disability income were also found to be statistically significant as categorical variables. Gender and hospitalization history were found to be non-significant predictors, which paralleled the result of the frequency count. Marital status was an exception to the consistency in findings between frequency counts and meta-analysis. Based on meta-analysis, marital status was found to be a significant predictor but the frequency count showed one study supporting it and three studies not supporting it. This contradiction may likely have been because only two of the four studies used in the frequency count could be included in the meta-analysis. Also, the meta-analysis could weigh and combine findings so that the strongly positive finding in one study, when combined with the weak negative finding in the other, still yielded a positive overall effect. Had all four studies been suitable for inclusion, the meta-analytic approach would have been superior to the frequency count in fairly evaluating the predictive value of marital status.
In this review we wanted to weigh the scientific evidence regarding individual predictors because they have potential significance for developing vocational interventions. Some variables such as education may reflect premorbid characteristics such as social class, educational opportunity and the age at which psychiatric illness may have begun to impair social functioning (which may well precede onset of illness). These variables are aspects of the person's past and are not changeable. They are relevant to rehabilitation primarily in terms of appropriate accommodations. Some variables, such as negative symptoms and cognitive functioning represent features of illness that directly affect current functioning and may be changeable. They deserve the attention they are beginning to get as targets for novel medications and remediation strategies. Vocational programs may wish to consider integrating these treatments into their rehabilitation plans in a coordinated effort to improve function through the synergy of new treatments and work opportunity. While medications targeting negative symptoms and cognitive enhancement have yet to be approved, a few experimental studies using cognitive remediation with vocational rehabilitation have been reported with good results [18,65,66]. Such integration of treatment with rehabilitation is consistent with the individual placement and support (IPS) model [67,68], which recognizes the important role that a team approach between clinicians and vocational specialists can play in successful vocational outcomes.
This review also shows that more research is needed into other potentially important predictors that may be changeable and relate to recovery. These include social cognition, social policy, and attitudes related to disability income, and psychological processes such as self-stigmatization, negative beliefs, and social skills deficits for which intervention may be possible [8,20,26,69]. This is particularly true for social cognition which has received more and more attention among researchers because of its relevance to vocational outcomes. For instance, poorer social cognition could lead to social discomfort on the job which in turn could lead to poorer work rehabilitation outcomes [26,70]. By understanding the relationships between individual characteristics and vocational outcomes, the field can gain valuable direction for the development and refinement of interventions that help people overcome their personal barriers to vocational success.
Footnotes
Acknowledgements