
Abstract
There is increasing focus on the impact of psychosocial variables such as anxiety, depression and social support on the outcome of people with coronary heart disease (CHD). Even minimal symptoms of depression are a reliable indicator of prognosis in CHD populations [1,2], with risk for cardiac mortality increasing with higher severity of depression symptoms [2]. Symptoms of anxiety and anxiety disorders have similarly been associated with poor outcome in CHD patients [3], although this relationship is less clear [4]. It has been suggested that high levels of social support can be cardio-protective [5] and are associated with improved depression outcome [6].
Research groups and national bodies [7–9] have encouraged cardiology services to routinely screen for depression and anxiety symptoms with the intention of informing individual care. The collection and auditing of these data also have the potential to reveal important clinical information about the group for whom the service provides care, as well as the impact of these variables on patient outcomes including survival, further cardiac events and admissions.
In our centre, cardiac rehabilitation patients are routinely screened for symptoms of anxiety and depression approximately six weeks post cardiac event. Screening at this point allows time for the psychological benefits of cardiac rehabilitation to accrue [10], and means that self-reported emotional distress is less likely to be a transient reaction to a significant health event [11]. Scores indicating distress are used to inform nurses about the need to prompt for further information and to make referrals. The opportunity arose to examine the prognostic value of screening among the group by linking these data with another local database holding medical and admissions data.
The present study reports data from this linkage in order to investigate psychological and social characteristics related to outcome of cardiac rehabilitation participants in Newcastle, New South Wales, Australia. Specifically, the data were analysed in order to determine whether cardiac rehabilitation attendees with depressive and/or anxiety symptoms and/or low levels of social support have higher mortality, hospital readmission rates, and longer length of stay in hospital independent of other clinical and demographic risk factors. The extent to which depression, anxiety and social support have interrelated prognostic impacts in cardiac patients was also investigated and it was expected that high levels of social support will reduce the impact of depressive and/or anxiety symptoms on mortality, readmission rates and length of stay in hospital. Moreover, this study aimed to provide evidence for the utility of analysing existing databases to obtain clinically relevant information pertaining to outcomes of cardiac patients with and without symptoms of depression and anxiety and social support.
Methods and materials
Design
Cardiac rehabilitation participants at the John Hunter Hospital, Newcastle, Australia [13], were screened with the Hospital Anxiety and Depression Scale (HADS) in week 4 of their programme as part of routine clinical practice (approximately 6 weeks post event). Ethics approval was obtained in order to link HADS scores collected between July 2003 and January 2006 to data held on a separate register (the Hunter Heart and Stroke Register [12]), which records information about consenting patients admitted to public hospitals in the Newcastle region following a cardiovascular event. Variables pertain to demographic, lifestyle and medical risk factors, cardiac rehabilitation participation and subsequent admissions. The follow-up period was calculated from the HADS completion date to their date of death or the study end date (April 2007).
A central database was established with the variables of interest:
HADS Anxiety (HADS-A) and Depression (HADS-D) scores.
Proxy measures of social support (Married: Yes/No; Lives alone: Yes/No).
Demographic variables (gender, age, employment status, cultural background).
CHD risk factors and medical variables (physical activity (inactivity: <30 minutes of moderate activity most days); smoking status (current smoker, ex-smoker, non-smoker); hazardous alcohol intake (men: >4 standard drinks/day, women:, > standard drinks/day); Body Mass Index (BMI) (underweight (BMI <20), normal weight (BMI = 20–25), overweight (BMI = 26–30), obese (BMI > 30); family history of CHD; comorbid conditions (hypertension, diabetes, high cholesterol, previous acute myocardial infarction (AMI), previous heart failure, previous left ventricular hypertrophy (LVH)); primary cardiac diagnosis/es and major cardiac procedure).
Outcome variables: (i) total number of recorded admissions to hospital (ii) length of stay in hospital of all recorded admissions (LOS), and (iii) mortality.
Participant group
A total of 426 cardiac rehabilitation participants (310 males) completed the HADS in the study period. Of these, 389 (91%; 279 males; mean age = 64.7 years, SD = 10.9) voluntarily provided information for the Heart and Stroke Register.
Measures
HADS is a 14-item scale that measures anxiety and depression symptoms, designed for use among medical outpatients [13]. It is well validated and easy to complete, with suggested cut-offs to describe severity of symptoms.
Statistical analysis
The Statistical Package for Social Sciences (SPSS) version 15.0 for Windows (SPSS, Chicago, IL) was used for all statistical analyses. Statistical significance was assessed at the p ≤ 0.05 level.
The association of baseline depression, anxiety, social support, and other potential covariates (e.g. age, obesity, primary cardiac diagnosis) with the outcome variables of admissions, LOS and mortality was explored in univariate analyses. Group differences were evaluated with chi-square statistics and logistic regression for the categorical outcome variables, and independent t-tests, correlations and ANOVA for the continuous outcome variables. Non-parametric tests were used for positively skewed data (admissions, LOS, HADS-D, HADS-A), specifically Spearman's correlations (Spearman r), Mann-Whitney U tests (z) and Kruskal-Wallis tests (H). The significant predictors from the univariate analyses were assessed in multiple variable generalized linear models (GLM) using the gamma error distribution and log link function to determine predictors of admissions and LOS, with backward elimination used to simplify the models. Logistic regression was used for the mortality variable. Depression, anxiety and social support were then added to determine whether they improved the simplified model, even if not significant at univariate analysis, as a final check to ascertain whether these variables were associated with the outcome variables. Furthermore, anxiety and depression were added as interaction terms with marital status and whether participants were living alone to determine whether levels of social support reduced the impact of depressive and anxiety symptoms on admissions, LOS and mortality.
Results
Sample characteristics
Of the 389 linked records, 32 participants (8%) had incomplete HADS data (range 7–13 items completed, mean = 12 items). Non-completers were significantly older (M = 70.0 years, SD = 9.6) compared with completers (M = 64.2 years, SD = 10.9; t (387) = −2.9, p < 0.01). These cases were excluded, resulting in a sample of 357 participants aged between 24 years and 87 years (see Table 1 for sample characteristics).
Characteristics of outpatient cardiac rehabilitation participants in the Newcastle region
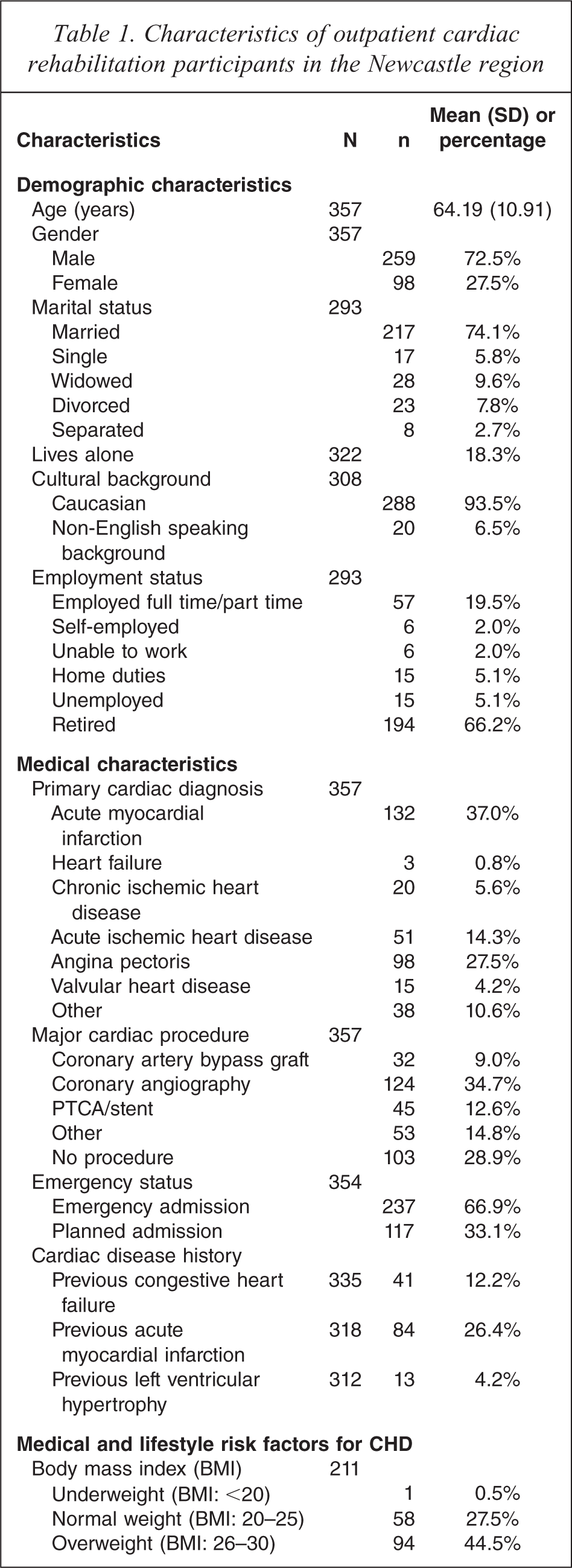
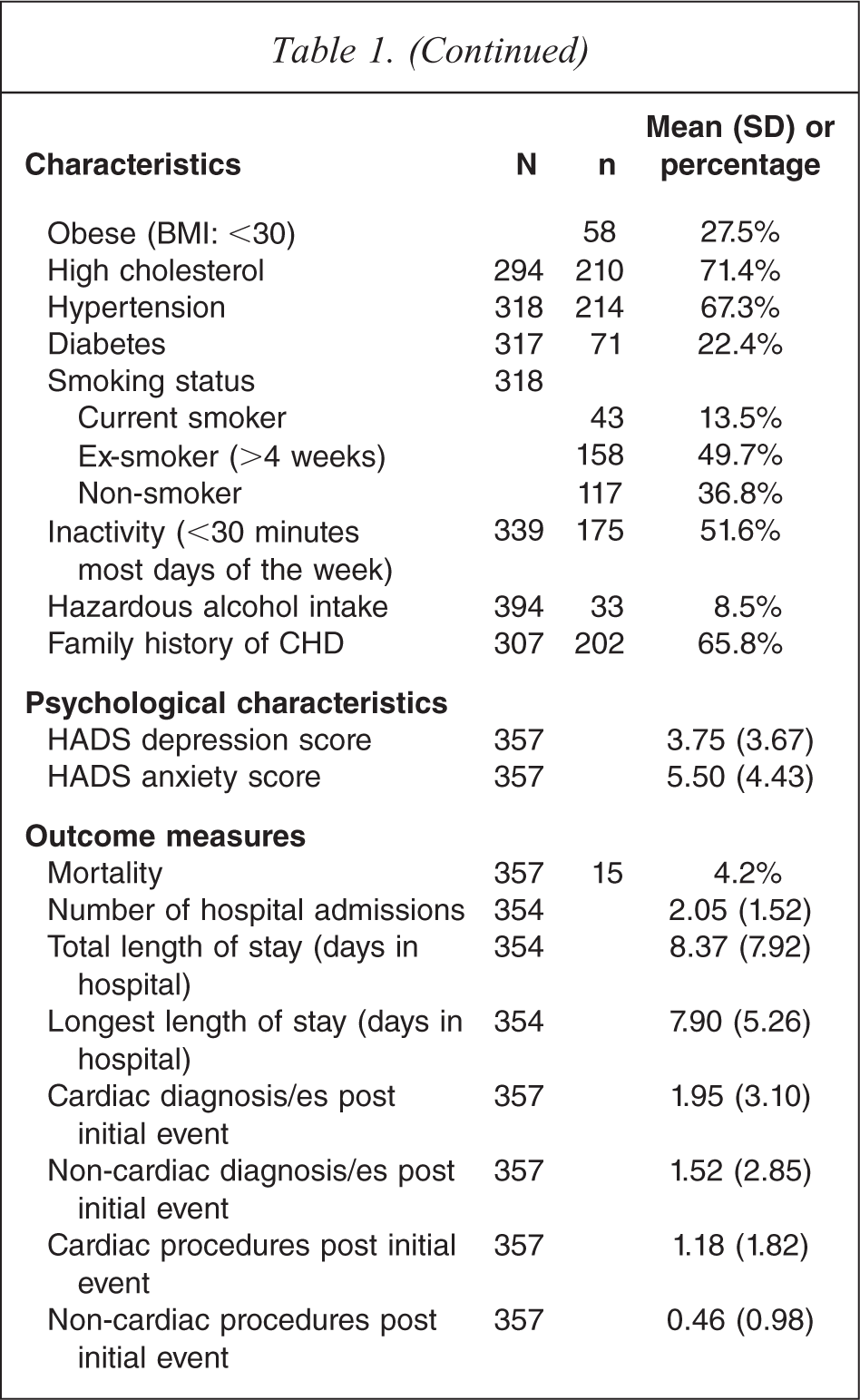
Participants’ scores ranged from 0 to 19 on the HADS-D and 0 to 21 on the HADS-A. Using the subscale cut-off of ≥ 8, 16.5% and 26.6% of the sample reported elevated depression and anxiety symptoms respectively. More specifically for depression, 38 (10.6%) participants reported mild symptoms (HADS-D score 8–10), 16 (4.5%) participants reported moderate symptoms (HADS-D score 11–15) and 5 (1.4%) participants reported severe depressive symptoms (HADS-D score ≥ 16). With regard to anxiety, 40 (11.2%) participants reported mild levels, 41 (11.5%) participants reported moderate levels and 14 (3.9%) participants reported severe levels of anxiety symptoms.
The average LOS was approximately 8 days, and the mean number of admissions was approximately 2. Fifteen deaths were recorded during the time period of the study. Duration of follow up ranged from 39 days to 3.8 years (M = 2.6 years, SD = 0.9).
Relationship between depression, anxiety, social support and baseline characteristics
Levels of depressive and anxiety symptoms at baseline were strongly and positively associated with each other (r = 0.66, p < 0.001). There was no association between whether participants lived alone and depressive (z = 1.34, p = 0.18) or anxiety (z = 1.85, p = 0.06) symptoms; nor between marital status and depressive (z = 1.32, p = 0.19) or anxiety symptoms (z = 0.94, p = 0.35).
Participants from a non-English speaking background (NESB) reported significantly higher levels of depressive symptoms (M = 5.45, SD = 4.98) compared with participants from an English speaking background (M = 3.39, SD = 3.47; z = 2.1, p = 0.03). Current smokers reported significantly higher levels of depressive symptoms (M = 5.49, SD = 3.64) compared with ex-smokers (M = 3.42, SD = 3.74) and non-smokers (M = 3.37, SD = 3.44; Hχ2(2) = 15.2, p < 0.001).
Age and gender were significantly associated with anxiety symptoms. Anxiety levels decreased as age increased (r = 0.21, p < 0.001), while female participants reported significantly higher levels of anxiety symptoms (M = 6.4, SD = 4.4) compared with male participants (M = 5.2, SD = 4.4, z = 2.5, p = 0.013). Participants who were employed full time or part time (M = 6.37, SD = 4.25), in home duties (M = 6.73, SD = 5.37), unable to work (M = 6.83, SD = 7.44), or unemployed (M = 7.20, SD = 4.87) reported significantly higher levels of anxiety symptoms compared with retired (M = 4.69, SD = 3.96) and self-employed participants (M = 4.83, SD = 3.97; Hχ2(5) = 12.0, p = 0.035). Current smokers reported significantly higher levels of anxiety symptoms (M = 7.79, SD = 5.26) compared with ex-smokers (M = 5.18, SD = 4.23) and non-smokers (M = 5.11, SD = 4.29; Hχ2(2) = 9.9, p = 0.007).
With regard to social support, male participants were more likely to report that they were married (78.4%) compared with female participants (63.5%; χ2 = 6.9, p = 0.009).
Predictors of number of hospital admissions
Univariate analysis revealed that a greater number of admissions was associated with more severe depressive (but not anxiety) symptoms (Spearman r = 0.10, p = 0.05, r = 0.06, p = 0.29 respectively). No relationship was found between number of admissions and anxiety or depression severity categories (Hχ2(3) = 4.95, p = 0.18, Hχ2(3) = 3.33, p = 0.34 respectively), marital status or whether or not the person lived alone. With regard to medical factors, high cholesterol (z = 2.11, p < 0.05), previous AMI (z = 4.19, p < 0.001), type of primary cardiac diagnosis (Hχ2(6) = 29.9, p < 0.001) and type of major cardiac procedure (Hχ2(4) = 28.38, p < 0.001) were associated with an increased number of admissions. GLM analysis using these significant variables revealed that a higher number of admissions was predicted by a previous AMI (Wald χ2(1) = 17.61, p < 0.001), a primary cardiac diagnosis of AMI, angina or heart failure (Wald χ2(6) = 46.48, p < 0.001) and a major cardiac procedure of stenting, angiography or coronary artery bypass grafting (Wald χ2(4) = 41.29, p < 0.001) (overall model: χ2(11) = 99.71, p < 0.001).
Social support indices, anxiety (continuous scores and symptom severity categories) and depression (continuous and symptom severity categories), and the interaction terms, were then added to this base model, one variable at a time, to see whether each variable independently improved the model's predictive value. Depression severity scores and category (Wald χ2(1) = 6.43, p = 0.01 and χ2(3) = 10.99, p = 0.01 respectively), continuous anxiety scores (Wald χ2(1) = 5.45, p = 0.01) and anxiety symptom severity categories (Wald χ2(3) = 12.75, p = 0.004) were all now individually significant predictors in the overall model. This was not the case for the univariate analysis and is attributed to adjusting for the cardiac-related factors. These and the significant variables from the base model were entered into a further regression analysis (final model: χ2(14) = 113.14, p < 0.001). The final model included anxiety symptom severity categories (Wald χ2(3) = 12.75, p = 0.004), previous AMI (Wald χ2(1) = 17.71, p < 0.001), primary cardiac diagnosis (Wald χ2(6) = 45.57, p < 0.001) and major cardiac procedure (Wald χ2(4) = 39.31, p < 0.001). In relation to anxiety, participants experiencing moderate to severe levels of symptoms reported a higher number of admissions compared to participants experiencing normal to mild anxiety symptoms. Depression no longer remained a significant predictor after controlling for anxiety symptoms, previous AMI, primary cardiac diagnosis and major cardiac procedure. This is likely due to a high correlation between anxiety and depression (for continuous scores Spearman r = 0.64, p < 0.001) but anxiety severity category remained in the final model due to having a slightly stronger relationship with number of admissions than depression.
Predictors of length of stay
Univariate analysis revealed that increased LOS was associated with increased depression symptom severity category (Hχ2(3) = 9.06, p = 0.03) but not anxiety symptom severity categories (H χ2(3) = 2.15, p = 0.54) nor continuous depressive and anxiety symptom scores (r = 0.07, p = 0.18 and r = 0.06, p = 0.25 respectively). In relation to social support, decreased LOS was associated with being married (z = 2.27, p = 0.02), but there was no association with whether the patient was living alone. Increased age (Spearman r = 0.11, p = 0.05), previous AMI (z = 3.38, p = 0.001) and type of major cardiac procedure (Hχ2(4) = 21.19, p < 0.001) were also significantly associated with increased LOS. GLM analysis using these significant variables (χ2(5) = 29.59, p < 0.001), revealed that increased LOS was predicted by having had a previous AMI, (Wald χ2(1) = 11.36, p = 0.001) and a major cardiac procedure other than stenting (Wald χ2(4) = 15.37, p = 0.004).
Using the above as a base model to control for cardiac-related effects the following variables were tested again one at a time to see if any were related: social support indices, anxiety continuous score (Wald χ2(1) = 1.29, p = 0.26), symptom severity categories (Wald χ2(3) = 2.94, p = 0.40) and depression (Wald χ2(1) = 5.69, p = 0.02, symptom severity categories Wald χ2(3) = 7.66, p = 0.05)) were added to the model. Both continuous and symptom severity depression measures were now significant, whereas the continuous form was not previously significant. Both anxiety measures being not significant it suggested that depression was more likely to be related to LOS than anxiety. The significant predictors in the final model (χ2(6) = 35.58, p < 0.001) were continuous depression scores (Wald χ2(1) = 5.69, p = 0.02), previous AMI (Wald χ2(1) = 12.95, p < 0.001), and major cardiac procedure (Wald χ2(4) = 15.78, p = 0.003).
Effect size of condition/surgery factors compared to psychological factors
Table 2 contains a summary of the effects from the final GLM models for number of admissions and LOS as marginal means and their 95% confidence intervals. This allows comparison of the relative impact of the psychological factors depression and anxiety with the condition and treatment effects. For number of admissions the difference between non-clinical (normal or mild) compared to severe anxiety is about 1 extra stay. This is comparable to the range displayed for previous AMI (0.6) and major cardiac procedure (1.3) and half the range for primary cardiac diagnosis (2.0). For LOS the impact of a change in depression score from 6 to 11 is about 1.5 days compared to 3.4 days for a previous AMI and a range of 6.1 days among the major cardiac procedures.
Summary of effects from GLM models
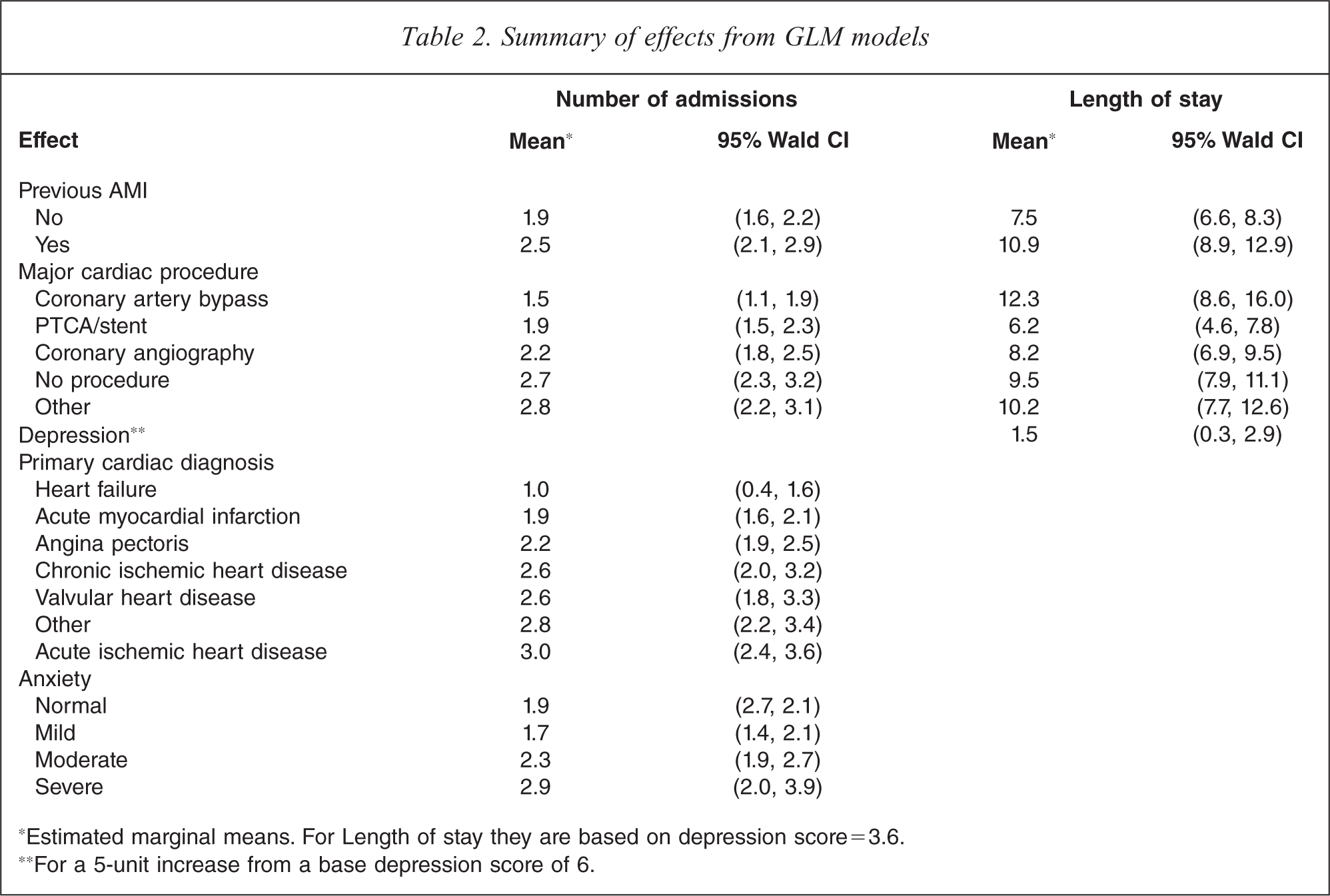
∗Estimated marginal means. For Length of stay they are based on depression score=3.6.
∗∗For a 5-unit increase from a base depression score of 6.
Predictors of mortality
The only variables significantly associated with mortality were gender (no female deaths; χ2(1) = 5.93, p = 0.015) and physical inactivity (χ2(3) = 7.97, p = 0.047). As 16 variables were analysed for possible associations with mortality, the Bonferroni adjustment was applied to rule out chance of Type I error from multiple comparisons, (α = 0.05/16 = 0.003) so the gender and physical inactivity were no longer considered likely to be significant.
Discussion
The present study examined medical records of cardiac rehabilitation participants to determine whether depressive and anxiety symptoms and social support were related to a higher number of hospital admissions, longer LOS and higher rates of mortality independent of other prognostic risk factors. When taking into account other risk factors, higher anxiety scores predicted a higher number of admissions and higher depression scores predicted a longer LOS in hospital. While social support (marital status) was associated with LOS, this did not remain significant after taking into account other risk factors. Social support was not associated with anxiety or depression scores and did not play a moderating role between depression or anxiety and admissions or LOS. No variables were associated with mortality, although mortality rates were low. Univariate analysis revealed higher levels of anxiety symptoms were associated with younger age, female gender, those who worked outside the home (versus retired or self-employed), and current smokers; while higher levels of depression were associated with current smoking and NESB status.
These findings provide further support for a prognostic role of depressive and anxiety symptoms, but not social support, with regard to morbidity in CHD. Clinical levels of anxiety symptoms were associated with one extra admission, while clinical levels of depression symptoms were associated with 1.5 extra days’ stay. In addition to depression being linked with poorer treatment adherence [14,15] and greater likelihood of engaging in behaviours that increase CHD risk (e.g. smoking and inactivity), there is evidence of direct pathophysiological effects which promote atherosclerotic growth (e.g. activation of the ANS and HPA axis, serotonergic dysfunction, secretion of proinflammatory cytokines and platelet activation [16,17]). Prior studies regarding the relationship between anxiety and outcome for CHD patients have reported mixed findings. High levels of anxiety or presence of anxiety disorders have been found to be associated with increased risk of subsequent cardiac complications or mortality [3,18,19]; however, not all studies have found such an association [20–22], with one study finding that anxiety was associated with lower mortality [23]. In the present study, while there is an apparent superiority of anxiety over depression with regard to number of admissions there is evidence anxiety and depression were similarly related. As such the finding could be due to random variability and depression could well be an equivalent predictor, suggesting that the interpretation that anxiety was more important than depression for length of stay should be resisted.
Previous findings have indicated that low level of social support is a strong risk factor for poor prognosis in cardiac patients [24,25]. The negative findings in this study may be due to the proxy measures used to assess social support (marital status and living alone). In the absence of more comprehensive assessments of, for example, perceived availability and satisfaction with support [26–29], relationship quality is unknown, as is the size and input of the person's available support network.
The finding that no variables were associated with mortality is at odds with previous research demonstrating increased risk of mortality in depressed cardiac patients compared to their non-depressed counterparts [30,31]. Some studies failing to demonstrate an association between depression and increased risk of morbidity and death have reported low rates of mortality [23] or relatively low rates of clinically relevant depressive symptoms [32], as occurred in this study. The low population prevalence of mortality does not allow for detailed examination of the correlates associated with this outcome variable, and the interrelationships between depression, anxiety and social support in relation to mortality could not be assessed.
Associations between anxiety symptoms and age and gender support previous findings in CHD [3,4] and community samples [33–36]. Females generally score higher on self-report measures, and anxiety and depression disorders are more common in females [33]. From the 40s onwards, prevalence of mental disorders and severity of anxiety and depression symptoms in the general community have been found to decrease as age increases [34–36]. While findings of increased anxiety amongst employed workers may result from increased stress on non-retirees who are faced with the possibility of being unable to work either temporarily or permanently, this finding may have also been influenced by age and/or gender effects, particularly as the other employment categories contained small numbers. Higher levels of anxiety and depression symptoms have been found in men that retire prematurely compared to those retiring at the usual retirement age [34,37]. Smoking was associated with higher levels of both baseline depression and anxiety, supporting existing literature [38], highlighting the importance of providing psychological interventions that target both smoking cessation and depressive and anxiety symptoms. With regard to cultural background, previous work has implicated NESB status as a predictor of persistent depression in women following an acute cardiac event [39]. In our study there was a trend for participants from a NESB to be living alone, therefore social isolation may be one factor contributing to increased levels of depression symptoms, particularly in regional areas with small NESB populations and limited services.
Demographic, medical and risk factor profiles of the participants were comparable to participant samples previously reported (e.g. [22,27,40]). This suggests that the small number of demographic and medical characteristics and conventional CHD risk factors implicated in prognosis in the current study cannot be attributed to differences in sample characteristics or lower prevalence of these risk factors. Rates of depressive symptoms among the group were lower than has been found in prevalence studies, with only 16.5% of participants experiencing pathological levels of depressive symptoms compared with prevalence rates of 27% to 46% found elsewhere [41,42]. However, a similar prevalence rate of 17.7% was found in a sample of 1052 cardiac rehabilitation patients, using the HADS-D at 3 weeks post event [18], suggesting that lower rates of clinical levels of depression symptoms may be expected amongst rehabilitation participants. Similarly, above threshold anxiety rates (using the HADS-A ≥8) were comparable to that sample (24.4% versus 26.6% in the present study) compared with rates of between 30 to 35% found one week post AMI [43]. Anxiety and depression scores were highly correlated in this study. There is increasing focus on the impact of comorbidity in CHD populations [3,44], with suggestions of a need to further explore the shared general distress underlying anxiety, depression and anger [3,38,45,46].
Study limitations
Results should be interpreted with caution due to several limitations. Excluded from analysis were 16% of participants due to incomplete items on the HADS. These participants were older on average that the remaining sample and it is unknown whether they may have had poorer outcomes. Secondly, the study examined cardiac rehabilitation patients, as no other CHD group are routinely screened for depression and anxiety symptoms within the Newcastle region. Cardiac rehabilitation programmes have been found to improve survival and emotional well-being [47] and rehabilitation attendees differ from non-attendees and non-completers with regard to age, gender, cardiac procedure/event and rates of emotional distress [48,49]. This selection bias may have resulted in a floor effect in the current study and be responsible for the low population prevalence of mortality, limiting power to detect associations between mortality and depression, anxiety and social support. As depression and anxiety were only assessed at one time point, longer term outcome and the impact of changes in depression, anxiety and social support impact on prognosis are unknown. Finally, data on severity of illness and types of subsequent procedures and diagnoses were not available.
Other limitations of the present study, including use of proxy measures (particularly with regard to social support) and missing data, also point to the importance of the quality of the information kept on databases, and the impact of missing data on the power to draw out clinically relevant information. Absence of gold standard measures limits generalizability and ability to draw conclusions. In the case of psychological measures, this highlights the importance of mental health and cardiology professionals liaising with regard to the measures utilized to assess psychological symptoms/diagnoses and relevant variables in hospital settings (e.g. adequate measures of social support).
Conclusion
The present study utilized existing clinical databases to determine the relative importance of depression, anxiety and social support in predicting prognosis in cardiac rehabilitation participants after controlling for demographic, medical and risk factor variables. A diverse range of cardiac diagnoses was included in the sample, and there was the ability to control for a large number of confounding CHD risk factors. Findings provide support for a prognostic role of depressive symptoms in relation to the LOS in hospital, and suggest that anxiety is associated with poorer outcomes in terms of an increased number of hospital admissions. This study has also provided a comprehensive summary of the characteristics of outpatient cardiac rehabilitation patients in the Newcastle region of NSW, and identified factors associated with emotional distress in these patients (younger, female, employed, smoking, or from a NESB), information that should be considered when creating or providing psychosocial or rehabilitation services. Overall, these results underscore the need for services to take into account patient characteristics, assess for psychological pathology and levels of social support, and develop and evaluate safe and efficacious psychological and/or pharmacological interventions to ameliorate their symptomatology, improve social support and improve clinical outcomes.
Footnotes
Acknowledgements
The authors wish to thank Rhonda Walker (Manager, Heart & Stroke Register) and Colleen Grace and the cardiac rehabilitation nurses at the John Hunter Hospital, Newcastle, Australia at the time of the evaluation.