
Abstract
Numerous studies have shown a disproportionately high prevalence of depression in cardiac patients compared with the general community, and depression is now recognized as an independent risk factor for both onset and poor prognosis of cardiovascular disease [1–11]. This risk is directly related to the severity of depression, with risk increased up to twofold for mild depression and three to five times for major depression [12]. This is manifest as increased mortality rates [4], increased morbidity (rehospitalization, medical service utilization) [13] and poorer self-reported quality of life [14]. The mechanisms proposed for the association between depression and heart disease include behavioural factors (poor compliance with recommended treatments to address cardiac risk factors), and biological mechanisms (autonomic nervous system dysfunction and serotonin mediated changes in platelet aggregation) [1]. Such mechanisms could also explain the prolonged duration of effect on health and wellbeing if depression persists. Depression is known to be under-recognized and under-treated in patients with cardiac disease [15, 16], in part because many clinicians believe that comorbid depression is ‘understandable’ hence adopt a ‘watch and wait’ approach rather than initiating treatment. Better targeted interventions could be implemented if cardiac patients at risk of more persistent and severe forms of depression could be identified.
The Identifying Depression as a Comorbid Condition (IDACC) study prospectively examined depressive symptoms in a cohort of patients admitted to hospital for a range of cardiac conditions or procedures, and included a nested intervention trial for depressed patients [2]. The cohort analysis, reported here, relates to those patients not depressed during cardiac hospitalization and the depressed ‘control’ group subjects. Using the Center for Epidemiological Studies Depression Scale (CES-D), 44% of inpatients reported depressive symptomatology at baseline (20% moderate to severe, 24% mild depression). A similar prevalence of depression was found 3 months after discharge, although more than one-third of patients had experienced a change in depression level over the 3 months [17]. Five clinically accessible characteristics were found to predict depression 3 months after cardiac hospitalization: depressive symptoms during the hospitalization; past history of emotional health problems (self-reported depression, anxiety or stress); previous diagnosis of a cardiac condition; current smoking and younger age. This paper extends these findings and examines baseline characteristics which predict depressive symptomatology 12 months after cardiac hospitalization. We also explore the course of depression from hospitalization to 3 and 12 months post discharge.
Method
Subjects
Details of this prospective study of 1444 cardiac inpatients have previously been described [2]. In summary, patients aged 18–84 years (68% male) and admitted to one of four large public hospitals in Adelaide, South Australia from August 2000 to December 2001, with admission reasons of either myocardial infarction, unstable angina, arrhythmia, congestive heart failure, angioplasty or coronary artery bypass surgery, were approached to participate in the study. Depressive symptoms were assessed using the CES-D [18], a 20-item self-report questionnaire. Depression severity was categorized according to standard threshold scores [19, 20] as not depressed (CES-D < 16), mild depression (CES-D = 16–26) and moderate to severe depression (CESD < 26). The CES-D has been used in a number of studies of depression in cardiac disease and these CES-D categories have been associated with increased risks of cardiac mortality [11, 21]. Questionnaires reported here were completed during the hospital admission and by postal follow-up at 3 and 12 months post discharge. Sixty-eight patients had died within 12 months of the index hospitalization (4.7% overall mortality rate, 3.6% not depressed, 5.1% mild depression, 7.4% moderate to severe depression at baseline). Complete baseline data were available for 1226 patients and of these, 81.2% returned a follow-up postal questionnaire at 12 months. The 231 patients who were still alive but did not return the 12-month questionnaire were significantly more likely to be moderate to severely depressed (χ2= 23.480, df = 2, n = 1223, p < 0.001), aged less than 55 years (χ2= 40.700, df = 3, n = 1223, p < 0.001), divorced, separated or never married (χ2= 24.185, df = 4, n = 1223, p < 0.001), current smokers (χ2= 40.394, df = 3, n = 1223, p < 0.001), and have a history of emotional problems (χ2= 20.947, df = 2, n = 1223, p < 0.001).
The 205 depressed patients randomized to the intervention arm of the trial were excluded from the following analyses to avoid the influence of intervention treatment effects. Probability weights were assigned to the ‘not depressed’ and ‘depressed’ control groups to account for removal of depressed patients randomized to the intervention group. Five further subjects with multiple fields of missing values were excluded, resulting in a dataset of 785 subjects who had completed baseline and 12-month questionnaires, and did not receive the trial intervention. The natural history of depression was examined in the subset of 739 participants who completed baseline, 3- and 12month questionnaires.
Statistical analyses
The statistical methodology used in our previous report [17] was followed for these analyses, using STATA version 8.0 (Stata Corporation, College Station, TX, US) [22] and SPSS for Windows version 11.0 (SPSS Inc., Chicago, IL, US) [23]. All statistical tests were twotailed with significance defined as p < 0.05. Chi-squared analysis identified associations between the outcome of depression at 12 months and potential predictor variables. Regression models were then developed with depression at 12 months as the dependent variable, to determine the odds ratio (OR) and 95% confidence interval (CI) of predictor variables. All variables were categorical and entered into the model. Missing responses were combined into a ‘not sure/not stated’ category, to avoid list-wise deletion of cases in the regression. Multinomial logistic regression was conducted after exploratory logistic regression analyses showed that different variables contributed to the prediction of mild depression and moderate to severe depression. Stepwise backward elimination was used to determine the association between the CES-D depression category at 12 months and a set of 20 baseline variables: depression level during the cardiac admission, demographic (e.g. age, gender, occupation), self-reported past history of cardiac or emotional health problems or risk factors, and hospital admission details (e.g. current cardiac diagnosis and length of stay, number of admissions during the past 2 years). Variables with largest p-values were individually removed and the model assessed at each step using the Log Likelihood Test. Significance at p < 0.1 was the initial criteria for removal, then p < 0.05 was used when no further variables could be removed at the higher level. As age was a predictor of depression at 3 months after cardiac hospitalization [17], and gender had been found to be associated with depression by other researchers [8, 11], these variables were retained in the model to adjust for differences between the depression severity categories. Regression diagnostics according to the method of Hosmer and Lemeshow [24] were subsequently undertaken to determine the fit of the multinomial model.
Results
Twenty baseline variables were originally tested as predictors of mild or moderate to severe depression at 12 months after the index hospitalization. Baseline variables significantly associated with depression at 12 months in the univariate analysis were: baseline level of depression (p < 0.001), previous diagnosis of self-reported depression, anxiety or stress (p < 0.001), gender (p < 0.01), length of hospital stay (p < 0.01), number of overnight admissions in 2 years before index admission (p < 0.01), marital status (p < 0.05), smoking status (p < 0.05), occupation for most of life (p < 0.05), source of household income (p < 0.05) and education level (p < 0.05).
In the multivariate analysis, moderate to severe depression at 12 months was associated with baseline depression level (moderate to severe OR = 19.5, mild OR = 6.4), past experience of emotional health problems (self-reported depression, anxiety or stress, OR = 2.8) and current smoking (OR = 2.3) (see Table 1). Mild depression at 12 months was associated with baseline depression level (moderate to severe OR = 2.4, mild OR = 1.75) and past experience of emotional health problems (OR = 2.2), while longer duration of hospital admission (≥5 days) was associated with a reduction (OR = 0.5) in risk of mild depression at 12 months.
Depression at 12 months predicted by baseline characteristics (Weighted multivariate results, adjusted for age and gender)
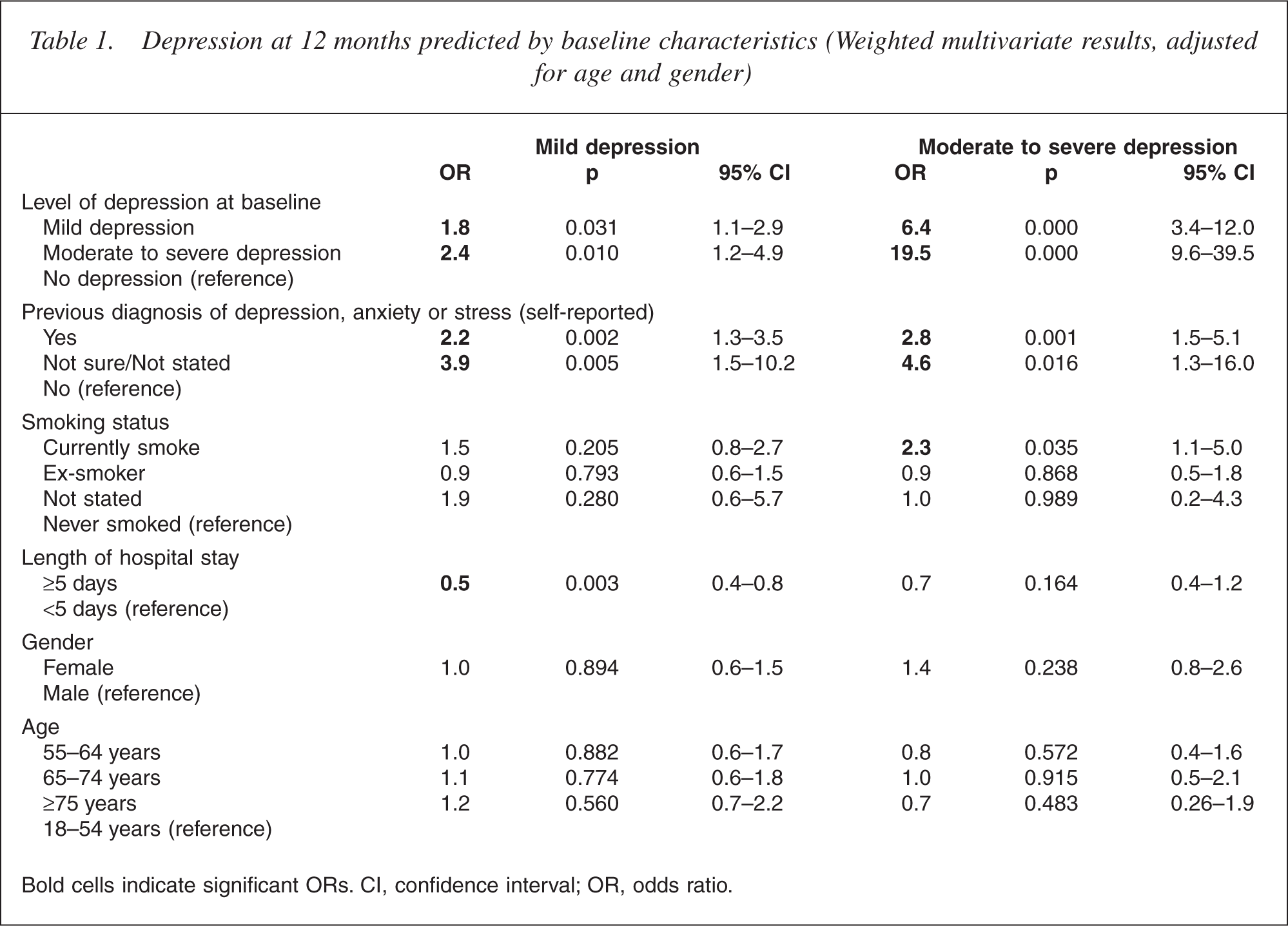
Bold cells indicate significant ORs. CI, confidence interval; OR, odds ratio.
The ability of the model to correctly predict level of depression at 12 months was good at 64% overall. The model was able to correctly predict 91% of people with no depression, 47% of those with moderate to severe depression and 7% with mild depression. Diagnostic tests indicated that the model was a good fit.
Tracking the natural history of depression over 12 months showed that the proportions in each depression category were similar at baseline, 3 and 12 months with 23% having mild depression and 16–17% having moderate to severe depression at each of the three assessments. However, considerable fluctuation in depressive symptoms took place at an individual level during this time, as illustrated by Fig. 1.
Natural history of depressive symptoms at baseline, 3 and 12 months after cardiac hospitalization (weighted cohort).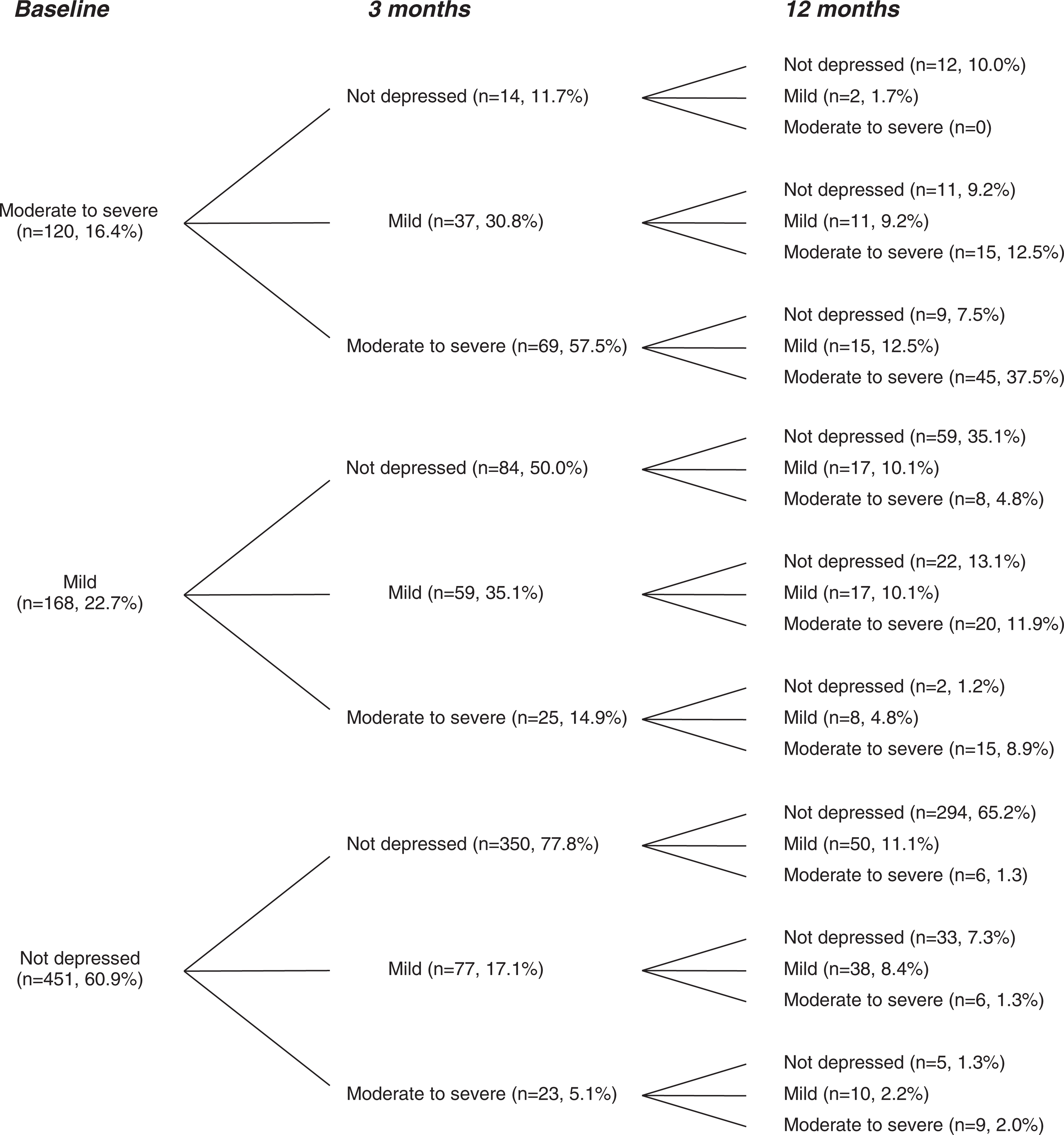
Overall, 66% (190/288) of patients with depressive symptoms (either mild or moderate to severe) at hospitalization had depressive symptoms at 3 months. By 12 months, 51% (146/288) remained depressed. However, there were differences between the baseline mild and the moderate to severe depression groups. Of patients with moderate to severe depression at hospitalization, 88% (106/120) reported depressive symptoms at 3 months. By 12 months, 72% (86/120) continued to report depressive symptoms. Only 10% (12/120) showed a ‘transient depressive response’ which had resolved by 3 months and did not recur at 12 months. At 3 months, 50% (84/168) of patients with mild depression at hospitalization continued to report depressive symptoms. By 12 months, 36% (60/168) remained depressed, with over half (35/60) of these progressing to moderate to severe depression. Only 35% (59/ 168) of patients with mild depression at hospitalization scored as not depressed at both 3 and 12 months. It is of note that 65% (294/451) of those ‘not depressed’ at baseline remained ‘not depressed’ at both 3 and 12 months. whereas only 5% (21/451) of those ‘not depressed’ at baseline had become moderate to severely depressed by 12 months.
Discussion
We found that baseline depression, a past history of emotional health problems and ‘current smoker’ status were powerful predictors of moderate to severe depression 12 months after hospitalization in cardiac patients. This finding is consistent with previous research. For example, Lesperance et al. found that a significant proportion of post myocardial infarction patients experiencing their first episode of major depression had a relatively rapid remission [25]. Lesperance and Frasure-Smith therefore recommended that patients with no history of depression should be allowed some time to recover without treatment, whereas rapid and aggressive treatment for those with previous depressive episodes is warranted [7]. In our study, mild depression at 12 months was predicted by depression severity at hospitalization, history of emotional problems and interestingly a shorter length of stay. However, the association with length of stay cannot be intuitively explained and may be related to the lower specificity the mild CES-D category has for depression.
While our results illustrate some fluidity of depressive symptoms at the individual level, depression persisted in 51% of patients, particularly in those who were moderate to severely depressed at baseline, where 72% remained depressed at both 3 and 12 months. Interestingly, we found that depression was as likely to persist as to remit in those with mild depression. Similar findings were reported by Hance et al. in a study of 200 patients after angiogram [26]. They found that minor depression was as likely to progress to major depression as to remit, especially among younger patients. Whether mild depression poses a risk of adverse outcomes by itself, or only if it worsens, is unclear from the literature, because many patients with minor depression go on to develop major depression [27]. The multivariate analysis in the present study shows that mild depression is a risk factor for continuing mild depression, as well as a risk factor for moderate to severe depression. Of note, the IDACC study included a nested randomized controlled trial of a general practitioner intervention for depression. This trial found that providing general practitioners with patientspecific information about depressive symptoms and advice regarding management reduced the proportion of patients with moderate to severe depression at 12 months, apparently because of averting progression from mild to more severe depression [28]. Importantly, this finding suggests that a simple intervention can modify the natural history of depression in cardiac patients.
High rates of transient depression in cardiac patients, indicative of an adjustment reaction rather than a depressive syndrome, are often cited as a reason why a ‘wait and watch’ approach is often adopted. It is understandable that clinicians are reluctant to initiate depression treatment unnecessarily. However, we found that only 10% of those classified as moderate to severely depressed at baseline were not depressed thereafter (at 3 and 12 months). While transience was more common after mild depression, with 35% of cases ‘not depressed’ at 3 and 12 months, substantial proportions of patients remained mildly depressed or progressed to moderate to severe depression. Clearly, depressive symptoms in some cardiac patients may fluctuate over time, and one assessment may not be sufficient to adequately assess the persistence of symptoms, particularly in patients with milder depressive symptoms. Results of our study may assist identification of cardiac patients in whom depression is more likely to persist and require treatment. Our findings suggest that patients with mild depression during cardiac hospitalization should perhaps be reassessed 3 months after discharge before commencing treatment.
Our study was unable to include non-English speaking patients and used self-reported depressive symptoms as an indicator of depression. Importantly, while the CESD categories of mild and moderately severe depression do not directly correlate with minor and major depression, these CES-D categories have been reported to be associated with increased risk of cardiac mortality [11, 21]. Nonetheless, we achieved high rates of initial consent and follow-up at 12 months, and the prevalence of depression in the IDACC cohort was similar to that previously reported among hospitalized cardiac patients [4–6,21]. Patients with moderate to severe depression at baseline were underrepresented in the 12-month analysis, as they were less likely to return the final questionnaire. This suggests that our findings might underestimate the persistence of depression at 12 months. We also included patients with a range of cardiovascular conditions on the basis of increasing evidence that depression is associated with a range of cardiac diagnoses [4, 5, 8, 10]. Furthermore, in our study neither admission reason nor discharge diagnosis was associated with prediction of depression at 12 months. In the multinomial regression, the ‘not sure/ not stated’ category for the variable ‘self-reported previous diagnosis of depression, anxiety or stress’ was associated with a significant OR. This finding was also reported in our previous analyses [17] and is difficult to interpret because of the small number of cases.
It has been argued that the identification of cardiac patients with persistent depression is an important direction for research [29]. The IDACC cohort study confirms that depression associated with cardiac disease often persists over a 12-month period. Furthermore, our findings identify clinically accessible predictors of persistent depression, namely baseline severity of depression, past history of emotional problems and ‘current smoker’ status. These findings strengthen the case for screening for depression in cardiac patients. They provide evidence for initiating treatment for patients with moderate to severe depression and for careful monitoring of cardiac patients with milder forms of depression.
Acknowledgements
The authors gratefully acknowledge the cooperation and support of the Heads of Cardiology and Psychiatry at each of the sites, and the many people involved in implementing the trial, including psychiatric registrars, medical and cardiac nursing staff, the IDACC project officers, and especially each of the patient and general practitioner participants.