
Abstract
Introduction
Major depressive disorder (MDD) is common in those with heart disease, affecting approximately 20% of subjects, a threefold increase in incidence compared to the general population (Goldston and Baillie, 2008; Rutledge et al., 2006; Thombs et al., 2008). The presence of MDD in heart disease is associated with a wide range of adverse outcomes, including poorer survival, with up to a doubling of mortality at 6 months (Frasure-Smith et al., 1993; Glassman and Shapiro, 1998; Nicholson et al., 2006), worse quality of life (Ruo et al., 2003), functional limitations (Mallik et al., 2005) and increased health costs (Frasure-Smith et al., 2000). Due to these deleterious effects, the National Heart Foundation of Australia (2011) and the American Heart Association (Lichtman et al., 2008) now recommend routine screening for depression in all patients with cardiovascular disease.
Among younger people, early retirement due to ill health is an important outcome that has been relatively neglected in the literature, but has significant individual and societal costs. There is the personal economic burden of reduced income, with a recent study calculating that those who retire early with depression have 78% less wealth accumulated compared to people in the labour force with no chronic health condition (Schofield et al., 2011). There are also adverse health outcomes associated with ill-health retirement (IHR), with increased rates of both mortality and suicide (The Royal Australasian College of Physicians, 2010).
IHR also costs New South Wales through disability or other income replacement benefits. In Australia, the majority of people who retire early through ill health do so by claiming the Disability Support Pension (DSP), which an individual receives until they are eligible for the old-age pension. The number claiming this benefit has increased from 140,000 in 1972 to over 700,000 in 2007 and only a minority of these DSP recipients will ever return to work (Cai et al., 2006). The proportion of female claimants has also increased dramatically over the past 20 years such that in 2007, 42.2% of claimants were female compared to 26.2% in 1987 (Australian Government, 2009). Furthermore, in many Organization for Economic Cooperation and Development (OECD) countries the proportion claiming for mental illness (predominantly depression and anxiety) has also increased, reflecting the changing nature of the workforce (OECD, 2003).
The relationship between heart disease, depression and IHR is unclear. Both depression (Conti et al., 2006; Karpansalo et al., 2005; Pit et al., 2010) and heart disease (Pit et al., 2010) are individually associated with early IHR, but the effect of depression in those with pre-retirement heart disease has been less well studied. In those with heart disease pre-retirement, gender may also influence the effect of comorbid depression on retirement. The different needs, obstacles and opportunities men and women have as a result of biological differences and gender roles (World Health Organization, 2002) are recognised in Australian health policy by the publication of the separate National Male (Australian Government Department of Health and Ageing, 2010) and National Women’s Health Policies (Australian Goverment Department of Health and Ageing, 2011). Specifically, we know that women aged 45–64 years are less likely to be participating in the labour force than men (Australian Bureau of Statistics, 2010), and post- myocardial infarction (MI), are more likely than men to report depression (Brisson et al., 2005). There is also some evidence that women are less likely to return to work following a MI (Boudrez and De Backer, 2000; Davoodi et al., 2010; O’Neil et al., 2010).
Our objective was therefore to examine the association of heart disease, depression and IHR in a large community sample. We had three specific aims:
Examine the relative independent associations of heart disease and depression with early IHR;
Examine the extent to which depression is associated with early IHR in those with heart disease prior to retirement;
Determine if, in those with heart disease prior to retirement, gender influences the association of depression with early IHR.
Materials and methods
Sample
We used data from the 45 and Up Study (45 and Up Collaborators et al., 2008), a large study of healthy ageing in the state of New South Wales, Australia. As detailed elsewhere (45 and Up Collaborators et al., 2008), participants were recruited through the Medicare Australia enrolment database. Eligible individuals were mailed an invitation to take part, an information leaflet, the study questionnaire, a consent form and a reply-paid envelope. Medicare is the federal, publicly funded, universal health-care system and the enrolment database provides almost complete coverage of the general population. We gained permission from The Sax Institute (Haymarket, New South Wales, Australia) to use data from the 45 and Up Study and ethical approval had been given from the relevant ethics committees. The 45 and Up Study questionnaire may be viewed at the study website (The Sax Institute, 2011).
We analysed data from the second and third versions of the questionnaire, which contained more complete information on prior depression. We restricted our sample to the 26,298 participants who had fully retired between the ages of 45 and 64.
All measures were extracted from the 45 and Up Study questionnaire. This contained questions about demographic information (current age, age at retirement, education and gender), the presence of depression, the presence of heart disease, physical disability, psychological distress and the reason for retirement.
Case definition: IHR
The reason for retirement was determined according to a multiple-choice question. Participants were asked if they had retired for one or more of the following seven reasons:
Ill health;
Reached usual retirement age;
Lifestyle reasons;
To care for family member/friend;
Made redundant;
Could not find a job;
Other.
Cases were defined as IHR if they selected the ill health response as the reason for retirement, even if they also selected other options. Controls were defined as non-IHR if they retired before the age of 65 for alternative reasons.
Exposures: doctor-diagnosed heart disease and depression
The presence of depression was determined by the question: Has a doctor EVER told you that you have … depression? The presence of heart disease was determined by the question: Has a doctor EVER told you that you have … heart disease? There were also questions as to each participant’s age at diagnosis of depression and heart disease. As we were interested in the association of depression and heart disease with retirement, we only used those participants who reported the onset of doctor-diagnosed depression and/or heart disease before their stated retirement age.
Potential confounders
Retirement age was grouped into 5-year intervals. The education groups were determined by whether the individual had left school early without a leaving certificate, had completed high school (or equivalent) or had gone on to attain further qualifications.
The presence of physical disability was assessed using the ‘yes/no’ question: Do you regularly need help with daily tasks because of long-term illness or disability? Although this referred to disability at the time of questionnaire completion, we used it as a proxy for long-term disability.
Psychological distress was assessed by the 10-item Kessler Psychological Distress scale (K10) (Kessler et al., 2002), which provides a global measure of distress based on depressive and anxiety symptoms experienced in the last 4 weeks. The cut-off scores were based on the Clinical Research Unit for Anxiety and Depression (CRUfAD, 2011) levels and have been validated by the Australian Bureau of Statistics (2003). Scores of 10–15 were considered ‘low’, 16–29 ‘moderate’ and 30–50 ‘severe’ levels of psychological distress. The K10 has been validated for use in the Australian population (Andrews and Slade, 2001).
Statistical analyses
All statistical analyses used the Statistical Package for the Social Sciences (SPSS 17.0.0 for Windows, PASW, Chicago, Illinois, USA). We excluded participants if they had any missing data. Descriptive statistics were performed and baseline characteristics for the cohort generated. Two sets of analyses were then run. First, we examined the whole sample of 20,655 and modelled univariate associations between the demographic variables, the psychological and physical health measures identified above and the reason for retirement. Based on a priori assumptions, we then modelled the association of gender, education, physical disability and the presence of depression and heart disease with IHR in a multivariate logistic regression, with all variables entered simultaneously. Second, we restricted the sample to those with heart disease pre-retirement and repeated the above univariate analyses and multivariate logistic regression.
To determine whether the association of depression with IHR in those with heart disease differed by gender, multiple logistic regression analyses were modelled for each gender separately. We also examined for the presence of an interaction between depression and gender using an interaction term in a multiple logistic regression analysis.
Results
Association of depression and heart disease with IHR
There were 26,928 respondents who had fully retired between the ages of 45 and 64. Of these, complete data were available on 20,655 participants. Missing data on IHR (up to 9.9%) and date of diagnosis (up to 12.7%) was more common in women than men. Nearly one in five (3836 out of 20,655; 18.6%) of the participants retired early due to ill health. A prior diagnosis of depression was associated with a threefold increase in the risk of IHR (odds ratio (OR) = 2.98; 95% confidence interval (CI) = 2.61–3.40) as was a prior diagnosis of heart disease (OR = 3.11; 95% CI = 2.75–3.52) (Table 1). Early IHR was also strongly associated with younger age at retirement, male gender, a lower level of education and more physical disability.
Baseline characteristics of the whole group and associations of variables with early ill-health retirement
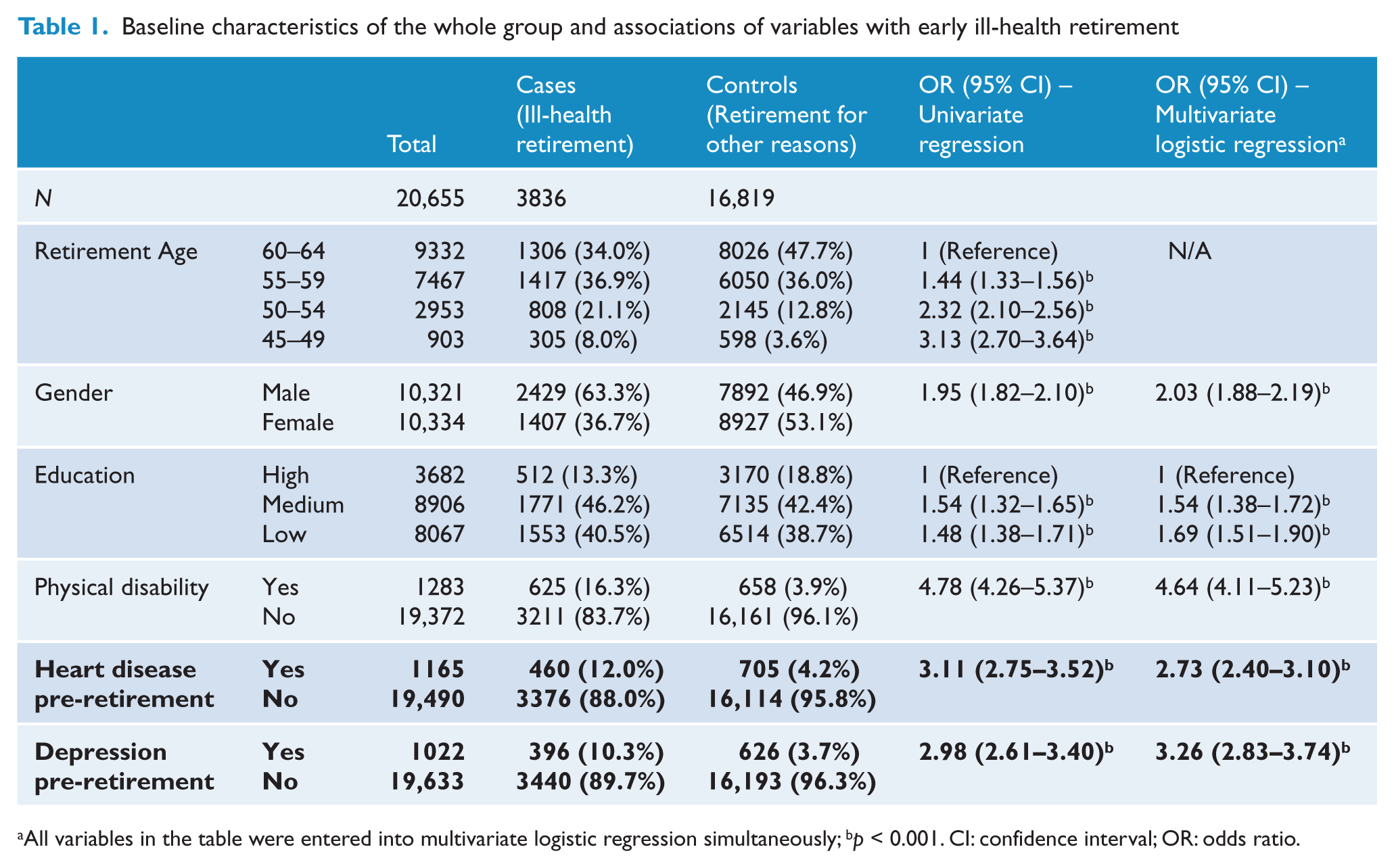
All variables in the table were entered into multivariate logistic regression simultaneously; bp < 0.001. CI: confidence interval; OR: odds ratio.
With regard to their current characteristics (not shown in Table 1), univariate analyses suggested that those who retired early due to ill health were slightly younger at the time of questionnaire completion (mean = 67.94 years, SD = 7.89) compared to those who retired early for other reasons (mean = 69.86 years, (SD = 8.19); mean difference = 1.92, 95% CI = 1.65 − 2.20). Ill-health retirees also reported much higher levels of psychological distress at the time of the survey, several years after retiring, with 1380 out of 3836 (36%) participants reporting moderate and severe distress compared to 2573 out of 16,819 (15.3%) of those who retired before the age of 65 for other reasons: (OR = 6.74; 95% CI = 5.34–8.51).
In the multivariate analysis (Table 1), both depression (OR = 3.26; 95% CI = 2.83–3.74) and heart disease (OR = 2.73; 95% CI = 2.40–3.10) remained independently associated with IHR. Male gender, a lower level of education and physical disability were also independently associated with increased odds of IHR.
The association of depression with IHR among people with heart disease
Of the 1165 participants who reported a diagnosis of heart disease prior to retirement, 460 (39.5%) retired due to ill health. Results from the univariate analysis (not tabulated) were similar to those seen with the whole sample, with IHR in those with prior heart disease being associated with the presence of depression pre-retirement (OR = 1.63; 95% CI = 1.01–2.63, p = 0.05), a younger age at retirement, male gender (OR = 2.58; 95% CI = 1.92–3.46, p = 0.00), a lower level of education and more physical disability (OR = 2.58; 95% CI = 1.69–3.96, p = 0.00). When adjusted for multiple potential confounders in the multivariate analysis, depression remained significantly associated with IHR (OR = 1.69; 95% CI = 1.02–2.79, p = 0.04) (Table 2). Male gender, a lower level of education and current physical disability also remained strongly and independently associated with IHR.
Factors associated with ill-health retirement in those with heart disease prior to retirement: multivariate logistic regression (N = 1165)
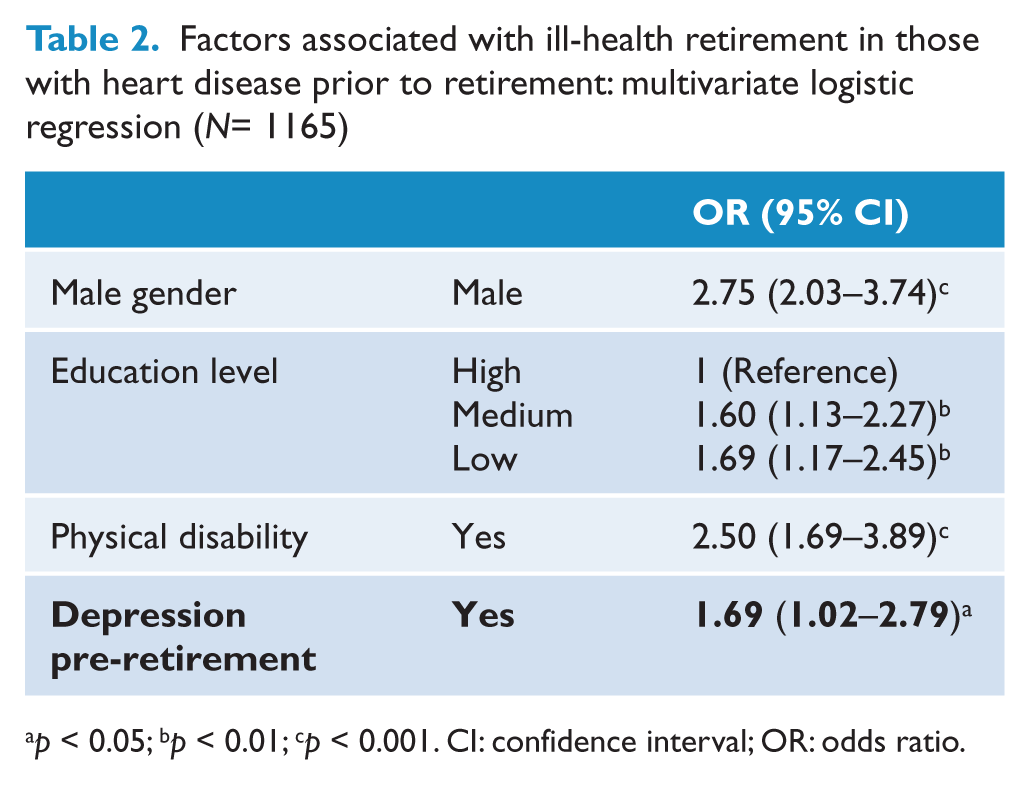
p < 0.05; bp < 0.01; cp < 0.001. CI: confidence interval; OR: odds ratio.
When stratified by gender, 11 of the 24 women (46%) with depression comorbid with their heart disease retired early due to ill health compared to 63 of the 283 women (22%) without depression. This is very different to the figures observed in men, where 25 of 47 men (53%) with depression comorbid with their heart disease retired early due to ill health compared to 361 of 811 men (45%) without depression. The disparity of effect is illustrated in Figure 1. The fully adjusted multivariate logistic regression analysis showed that for women with heart disease pre-retirement, the presence of comorbid depression was strongly associated with IHR, with a threefold increase in its likelihood (OR= 2.85; 95% CI = 1.20–6.77, p = 0.02). The effect of comorbid depression on IHR was not seen in men (OR = 1.34; 95% CI = 0.73–2.50, p = 0.34). We found a significant interaction between sex and depression using a forward stepwise logistic regression analysis (OR= 1.45; 95% CI = 1.01–2.10, p = 0.045).
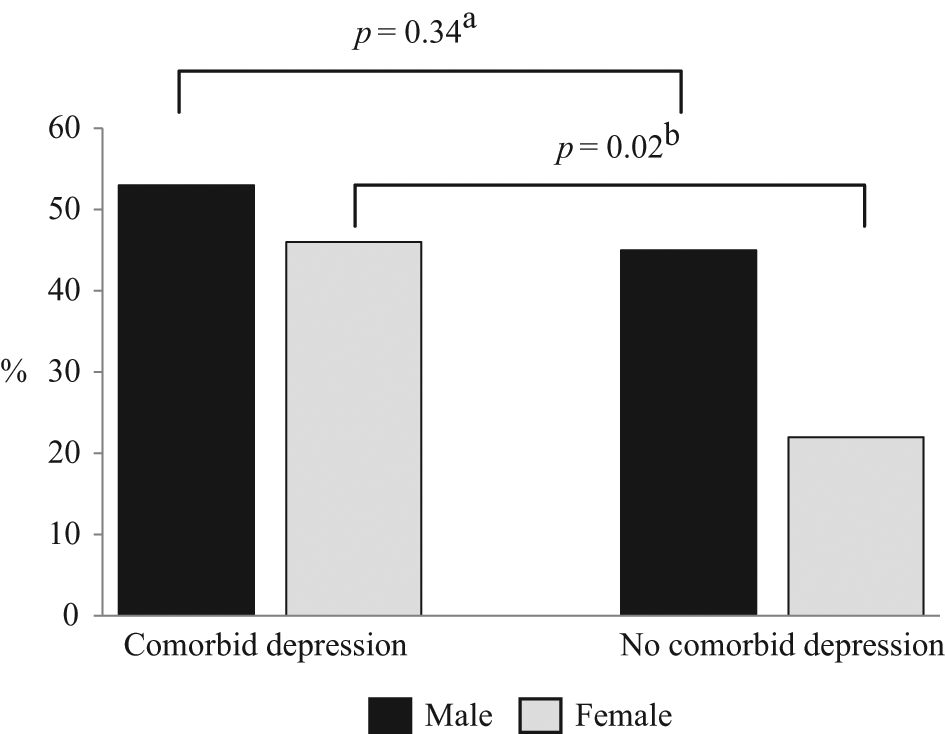
Gender interaction with the association of comorbid depression with ill-health retirement (IHR) in those with heart disease pre-retirement (N = 1165).
Post-hoc analysis revealed this effect was not seen in the whole cohort of 20,665, where the association of depression with IHR did not significantly differ between genders. To evaluate the possibility of a type I error due to the large sample size, we ran a sensitivity analysis with a smaller control group. A random sample of 3836 was selected from the 16,819 controls, so that the case and control groups were matched for size. This did not alter our findings and the strength of association between depression and IHR remained similar, including when stratified by gender.
Discussion
This paper has confirmed that both depression and heart disease are strongly and independently associated with IHR in a large, population-based sample of middle-aged Australians. We also showed a possible deleterious effect of IHR, with those retiring early due to ill health having greater levels of current psychological distress compared to those retiring early for other reasons. Among those with heart disease, the presence of comorbid depression prior to retirement was only associated with an increased risk of early IHR in women, increasing its likelihood threefold. This effect was not seen in men.
The finding that depression and heart disease are strongly and independently associated with IHR is consistent with the existing literature (Conti et al., 2006; Karpansalo et al., 2005; Pit et al., 2010). This is not surprising given the well-established morbidity associated with both these conditions. Indeed, depression and heart disease are set to be the two largest contributors to global burden of disease by 2020 (Murray and Lopez, 1997). Recent research has also suggested that official statistics may even have underestimated the cost of depression in terms of disability pensions and lost productivity, by misclassification of disease and the under recognition of common mental disorders (Mykletun et al., 2006).
A number of publications have highlighted the deleterious clinical effects of comorbid depression in those with heart disease (Frasure-Smith et al., 1993; Frasure-Smith et al., 2000; Glassman and Shapiro, 1998; Goldston and Baillie, 2008; Mallik et al., 2005; Nicholson et al., 2006; Ruo et al., 2003; Rutledge et al., 2006; Thombs et al., 2008).
With an ageing population and increasing retirement ages in several OECD countries, the outcome of early IHR can be a significant problem for individuals and the state. The effect of depression on work and functional outcomes in those with heart disease has been less well studied. A recent systematic review of 12 studies investigating return to work (RTW) following an MI found an impact of depression in the majority of the studies and no contrary results (O’Neil et al., 2010). They concluded that the presence of comorbid depression was a predictor of not returning to work, consistent with earlier studies (Hlatky et al., 1986; Maeland and Havik, 1987). RTW and IHR are different, albeit related concepts. Individuals may return to different forms of work such as restricted or part-time duties that may not require them to completely leave the workforce. Further, some groups may not be eligible for IHR, or choose to not access such a scheme, e.g. those in precarious employment or those who do not meet means-tested thresholds. Some of the conflicting results seen in the literature are due to this lack of consistency in the definition and measurement of depression and particularly workforce exit. A further issue, raised by the authors of the systematic review (O’Neil et al., 2010), is the lack of representativeness of female participants in most of the studies of RTW following a cardiac event. In their review, a third of studies included only male participants and the highest percentage of female participants in any study was 27% (Mayou et al., 2000). For the reasons discussed below, this is likely to influence strongly any association between comorbid depression and early IHR.
The finding of comorbid depression being associated with early IHR among women with heart disease pre-retirement, but not men, is a novel finding. Interestingly, of the 12 studies in the post-MI review (O’Neil et al., 2010), three of the five studies which reported a null association between depression and RTW involved all-male samples (Engblom et al., 1997; Ladwig et al., 1994; Mittag et al., 2001), compared to only one of the seven studies (Soejima et al., 1999) which did find an association. This is supportive of our finding that it is women who are susceptible to the effects of depression on IHR in those with heart disease. It is unclear why in those with heart disease prior to retirement, comorbid depression should have a differential effect on IHR in women and men. Research in this area is very limited but several factors may be important. Firstly, spousal income has been reported as more important for women when considering retirement than men (Warren, 2006). With the onset of depression, this may have allowed greater freedom to decide to retire.
Men by contrast, even with depression, may have felt more financial obligation to continue working. However, our results suggest that this may not be the case as the effect of depression in women was to bring the proportion taking IHR to that of men (50%). It appears rather that not being depressed is somehow protective for women. Women also reported different sources of pressure to retire than men. Women were more likely than men to experience pressure from their spouse or partner to retire, but less likely to experience pressure from their doctor (Warren, 2006). This differential pressure may have a mediating effect when the decision to retire due to ill health is made, and could certainly be perceived differently if one were depressed or not. The observation that women were slightly less likely to specify their retirement age than men (90 vs. 95% respectively) may indicate that some women’s transition from the workplace may be more gradual as is common with precarious type or short-contract roles that women are more likely to occupy. Finally, one can speculate that the different types of jobs women and men perform have a differential role in mediating the effect of depression. Census data showed that for those aged 45–64, women are more likely to be employed in clerical and administration roles as well as working in community and personal support jobs (Australian Bureau of Statistics, 2006). Men in this age bracket are more likely to work as tradespeople, machinery operators and drivers. It may be that the greater interpersonal skills needed in roles such as personal support jobs makes them less compatible to continued working in the presence of depression (Mechanic, 1998).
Although depression had a strong effect on IHR in the whole sample of 20,665, this did not differ by gender. Further research is therefore needed to determine whether this effect is specific to depression comorbid with heart disease or whether women, but not men, are more likely to retire early in the presence of depression comorbid with other common health problems (e.g. chronic obstructive pulmonary disease).
Limitations
There are limitations to our study. First, we did not have a measure of pre-retirement physical health. We used current physical disability as a proxy for disability pre-retirement but we cannot corroborate the validity of this approach. Secondly, the diagnosis of heart disease and depression was self-reported, based on a previous medical diagnosis, but without objective verification. The term heart disease also encompasses a range of conditions, including both heart failure and ischaemic heart disease. With up to 12.7% missing data on disease onset or time of retirement, the sample included may have been subject to selection bias. In all categories these missing data were either more common in women than men, or equal by gender. Given that non-response is more likely in those with psychiatric disorders and those leaving the workforce early (Knudsen et al., 2010), this would imply that, if anything, the impact of female gender on the association between depression and IHR would be underestimated in our models. Finally, the severity of depression pre-retirement could not be assessed. The participation rate of the 45 and Up Study was low, at 18% for the first 100,000 participants. However, comparison with the NSW Population Health Survey demonstrated good generalisability (Mealing et al., 2010). Studies of this kind are also susceptible to attrition bias. Those who were the most unwell, either with depression or heart disease, are more likely to have passed away by the time of the survey and so the respondents may represent a more healthy cohort. If this were true, it is again likely to underestimate the effect of depression or heart disease on retirement. However, it is difficult to see how attrition and measurement bias could explain the findings of a differential gender effect of depression on IHR.
Strengths of the study included its size. To the best of our knowledge, it is the largest study to examine the effect of depression and relevant potential confounders on IHR in those with heart disease. The size allows simultaneous analysis of the confounders while retaining good power. By not restricting the duration of retirement post-heart disease diagnosis, we also get a more naturalistic view of the effect of heart disease over many years. Even with over 20,000 participants, however, the absolute number of women with heart disease and depression retiring early was small and further studies are needed to confirm our findings and explore the relationships between gender and early retirement in those with heart disease.
Conclusions
We have confirmed that both depression and heart disease are strong independent predictors of IHR in the population. In those with heart disease, IHR is twice as common as in the general sample. Comorbid depression is a strong predictor of IHR in women with heart disease, but not in men. IHR is associated with a number of adverse outcomes for both the individual and society and so women with heart disease may represent a group particularly amenable to screening for and selective prevention of depression. This study has highlighted the need to consider gender in future studies examining the relationship between depression, heart disease and psychosocial outcomes. Clinicians working in consultation-liaison settings or rehabilitation should be aware of gender differences in the effects of depression, when trying to optimise outcomes for their patients.
Footnotes
Acknowledgements
The 45 and Up Study is managed by The Sax Institute in collaboration with major partner Cancer Council New South Wales and the following partners: the National Heart Foundation of Australia (NSW Division); NSW Health; beyondblue: the national depression initiative; Ageing, Disability and Home Care, Department of Human Services NSW; and UnitingCare Ageing.
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.