
Abstract
It has long been accepted that certain demographic, lifestyle and medical factors place an individual at higher risk of coronary heart disease (CHD). During the last decade, however, evidence has emerged that certain psychosocial factors, particularly depression, can also be risk factors for CHD [1]. Depression appears to place an individual at greater risk of developing CHD, and those who already have CHD who are also experiencing a coexisting depression face a higher rate of mortality and morbidity [2,3]. There is also growing evidence of a similar link between symptoms of anxiety and prognosis for patients with known CHD [4].
Although it is commonly accepted that the interventions that are effective in treating depression in the community will also be effective for patients with CHD, there is as yet no conclusive evidence that treatment improves outcome in terms of morbidity and mortality [5]. There is, however, evidence that treatment for depression, in addition to improving mood, is associated with increased quality of life [6], improved social support [5], decreased hostility [7] and better adherence to medications [8].
Although the Australian National Heart Foundation has encouraged the identification and treatment of depression in cardiac patients since 2003 [1], no specific recommendations regarding strategies to do so have been proposed. At the Centre for Brain and Mental Health Research, University of Newcastle, New South Wales, routine screening for depression and anxiety in cardiac rehabilitation patients was found to be feasible and has been implemented. A group programme was proposed as a potentially cost-effective specialized therapy for patients with continued depression and symptoms of anxiety at the end of their enrolment in cardiac rehabilitation. A local established and efficacious community-based group cognitive behaviour therapy (CBT) programme was initially utilized but was found to be clinically inappropriate for the CHD patients who were typically older men and unaware of their depression. The early focus on cognitive restructuring did not allow for necessary psychoeducation regarding the symptoms and causes of depression and anxiety. Because no other suitable group programme could be identified for this population, the objective was to develop and evaluate a group treatment programme suitable for the needs of people experiencing depression and symptoms of anxiety while living with heart disease.
Methods
Design
Between July 2003 and March 2006 all participants enrolled in a cardiac rehabilitation programme at John Hunter Hospital, Newcastle, Australia, were screened in week 4 of their 6–8 week programme using the Hospital Anxiety and Depression Scale (HADS) [9]. Week 4 was chosen because this was approximately 6 weeks after the cardiac event, allowing time for psychological adjustment [10] and for the beneficial effects of cardiac rehabilitation [11,12]. The HADS was chosen because it has been validated on medical patients; it is brief; and it includes assessment of both depression and anxiety. A score of ≥8 on either subscale signals ‘probable’ problems with depression or anxiety [9].
From July 2003, cardiac rehabilitation participants with scores ≥8 on the depression (HADS-D) or anxiety subscales (HADS-A) of the HADS were offered the option of participating in the BraveHeart programme, a group run as part of usual service provision. Group participants completed the HADS and the Beck Depression Inventory-II (BDI-II) [13] at baseline, week 1 and week 6 during the last group session, and at 1 and 6 month follow ups via mail. If participants’ HADS and BDI-II scores were below a pre-identified clinical threshold at session 1 (i.e. between screening and session 1 a decline had occurred in their HADS-D or HADS-A scores to <8; and their BDI-II scores were below the suggested cut-off of 14 for mild depressive symptoms), they were able to participate in the group, but their data were not included in the analysis. Patients’ partners or carers were not specifically invited nor excluded, data for those that did attend were collected but not included in these analyses. The opportunity for feedback was built into the programme structure, with time during the final session allowing both verbal and written feedback. Feedback was used to guide minor modifications to the programme.
Participant group
Six BraveHeart groups were conducted between April 2004 and October 2005 with a total of 44 patients starting the programme. Of these 44 patients, the data of four were excluded because their scores at session 1 were below the identified clinical threshold described earlier. Data from another patient were excluded because behaviour during the programme was strongly suggestive of dementia. All five patients were given the opportunity to complete the group; two dropped out after session 1. Of the remaining 39 patients, nine did not complete the programme (including five women). Thus, 30 patients (77%) comprised the final participant group (mean age ± SD = 60.0 ± 20.0 years; 26.7% (n = 8) female) at post-treatment assessment. All 30 completed the 1 month follow-up assessment and 25 completed the 6 month follow up. Three partners also attended the programme and participated as group members (data not included).
Measures
Because this was a service evaluation project, active consent was not sought. Completion of the limited set of measures was deemed sufficient to indicate consent.
Hospital Anxiety and Depression Scale
The HADS is a 14-item scale, designed for use with medical outpatients, which measures both anxiety and depression symptoms [9]. It is well-validated and relatively quick for participants to complete, with suggested cut-offs to describe severity of symptoms.
Beck Depression Inventory-II
The BDI-II is a 21-item depression scale designed to measure the severity of DSM-IV symptoms of depression and is considered the gold standard of self-report depression measurement [13].
Participant feedback
Quantitative feedback was obtained via 5-point Likert scales regarding participants’ enjoyment of the programme, how helpful they found it and how well they thought the facilitator/s led the group (1 = not at all, 2 = a bit, 3 = moderately, 4 = quite a lot, 5 = very much) [14].
Intervention
BraveHeart is a 6 week group-based CBT programme. It uses a manualized tool kit’ approach, likening CBT strategies to car maintenance tasks (Table 1). Each session included programme overview; revision of homework from the past week; new information and new homework tasks; and a session summary. Core strategies included mood monitoring; problem solving; activity monitoring and planning; and thought monitoring and challenging. In the first and last session, participants completed the measures (HADS, BDI-II) and feedback on their scores was provided during the session. The groups were facilitated by clinical psychologists (authors AT and JH for five groups; AT and AB for one group). Copies of the therapist and treatment manuals are available from the authors.
Final BraveHeart session content
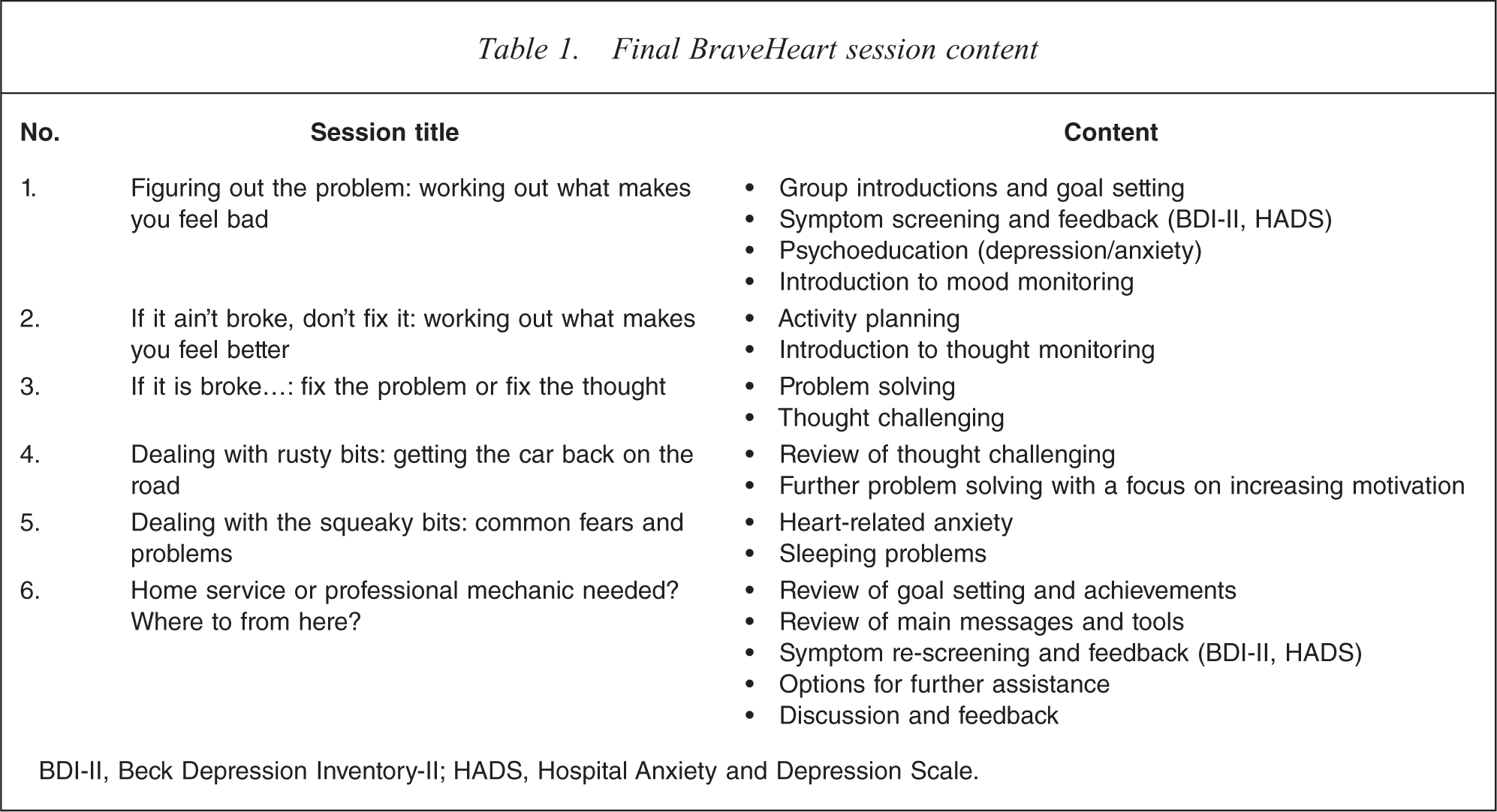
BDI-II, Beck Depression Inventory-II; HADS, Hospital Anxiety and Depression Scale.
Results
Screening and sample characteristics
During screening of cardiac rehabilitation outpatients, 628 HADS forms were returned and 558 were correctly completed. Demographic information was provided for 614, mean age ± SD was 63.8 ± 11.4 years, with 74.6% (458/614) male. Using a score of ≥8 on either the depression or anxiety subscales, clinically significant scores were occurring at rates of 17% (95/558) of patients for depression symptoms and 26% (145/558) for anxiety. Thirteen per cent of patients (73/558) were experiencing both high depression and high anxiety scores. Those who met threshold were more likely to be female (33.5%, 56/167) and younger (mean age ± SD = 61.7 ± 11.7 years, χ2(1) = 8.2, p < 0.01) than those who did not meet threshold (22.3% female, 37/167; mean age ± SD = 64.4 ± 11.1 years, t(583) = 2.8, p < 0.01).
Of the 70 incomplete HADS, 29 had no items completed, 28 had 13 items completed, and the remaining 13 had 3–12 items completed. For those who provided demographic information (n = 614), non-completers were significantly older (mean age ± SD = 68.8 ± 11.0 years) than completers (mean age ± SD = 63.1 ± 11.3 years, t(613) = 4.0, p < 0.001). No differences between completers and non-completers were found for gender, nor in HADS scores (using data from non-completers who answered ≥3 items on the questionnaire).
With regards to identifying potential participants on the HADS, if enough of the questionnaire had been completed to indicate that the person scored ≥8 on the HADS-D or HADS-A subscales, they were identified as eligible if contact information had been provided (n = 182). Of those, 44 patients accepted the invitation (24.1%) and attended session 1. Attendees were not significantly different to non-attendees with regard to age, gender or HADS scores. Eight (18.2%) were on antidepressant medication at baseline.
Group attrition and feedback
Completion of the programme was defined as attending at least four sessions and completing at least one follow-up assessment. Of the nine who did not complete the programme, five attended one session, and one completed four sessions but not the follow-up assessment. For the 30 who completed the programme the mean number of sessions attended was 5.3 ± 0.7.
Characteristics of those participants who started but did not complete the programme (n = 9) were compared to those who did complete the programme (n = 30). There were no significant differences in gender, age or baseline HADS or BDI-II scores between completers and dropouts. Although the difference in dropout rates between men and women was not significant, 56% of those who did not complete the programme were female despite women comprising only 26.7% of the baseline sample.
With regards to feedback about the programme, mean scores on the 5 point Likert scale for the Enjoyment, Helpful and Leader items were 4.2 ± 0.8 (median = 4), 3.9 ± 0.9 (median = 4) and 4.6 ± 0.6 (median = 5), respectively. For all responses regardless of item, 83% of ratings were a score of 4 or 5.
Change in depression and anxiety
Repeated measures analyses of variance were conducted, taking into account unequal intervals between assessment occasions, to examine patterns of change over time (Table 2). There was a significant overall reduction in HADS-A, HADS-D and BDI-II scores in all cases (linear trend), which was more pronounced between baseline and post-treatment assessment for the HADS-D and BDI-II for those 25 followed up at 6 months (quadratic trend), and on all three measures for the group followed at 1 month (n = 30). In addition, moderate–strong effect sizes (0.57–0.95) were found for all three measures, for all time point comparisons (baseline vs after treatment, baseline vs 1 month and baseline vs 6 months; Table 2). On all scales, mean scores fell below the suggested clinical cut-off of 14 for the BDI-II and 8 for the HADS-A and HADS-D at 6 months. Scores were categorized into severity ratings and can be seen in Table 2. On all follow-up occasions >50% of participants had depression scores in the ‘minimal’ range.
HADS-A, HADS-D and BDI-II scores vs assessment timepoint
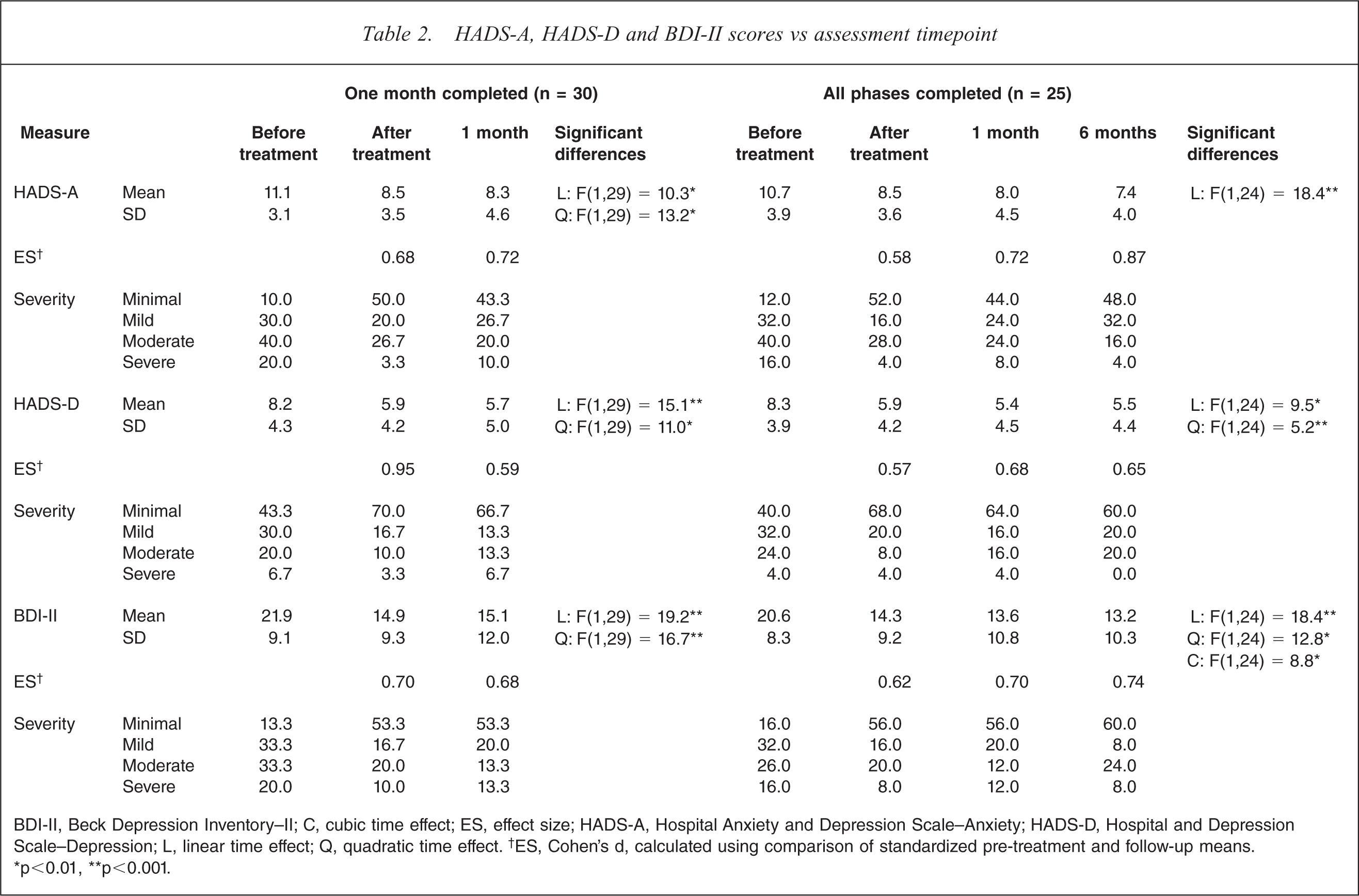
BDI-II, Beck Depression Inventory–II; C, cubic time effect; ES, effect size; HADS-A, Hospital Anxiety and Depression Scale–Anxiety; HADS-D, Hospital and Depression Scale–Depression; L, linear time effect; Q, quadratic time effect. †ES, Cohen's d, calculated using comparison of standardized pre-treatment and follow-up means. ∗p < 0.01, ∗∗p < 0.001.
Discussion
The main finding of the present study was that a specially developed CBT programme for depression among CHD patients was associated with clinically significant changes in depression and also anxiety. Significant improvements in depression and anxiety occurred for attendees during treatment and were maintained at 6 months. Traditional CBT tools, in combination with the presentation of CHD and lifestyle-specific examples and information, were utilized.
In the present pilot study the focus was on ‘emotional distress’. As such, people with high depression and/or high anxiety scores were invited into the programme. HADS-A scores tended to be higher than HADS-D scores at baseline. The programme did not use any anxiety-specific techniques (e.g. breathing retraining, exposure therapy), apart from education provided in session 5 around heart-related anxiety. Although a significant reduction in anxiety symptoms was found, post-treatment mean scores were still above entry criteria levels. These had dropped below threshold, however, at 6 months. The present pilot evaluation does not have detailed information on anxiety disorders that participants had been experiencing. It may be that BraveHeart addresses health-related or generalized anxiety symptoms, but not those of specific disorders such as panic disorder or post-traumatic stress disorder.
The average age of the cardiac rehabilitation population screened in the present study was 64 years, three-quarters of whom were male. Younger patients and women, however, were more likely to be identified as distressed when screened, while older patients were less likely to complete all questions on the screening form. Although >50% of treatment non-completers were female, there was no difference between the symptom severity of those who dropped out early in therapy and those who completed treatment. It may be that a primarily male group is less appealing to women if the group is small and closed (compared to cardiac rehabilitation, which is a larger group, in a rolling format, requiring less personal disclosure), or that the more male-oriented metaphors used in the programme were less appealing to women. Lower rate of programme completion by women, however, has also been found in cardiac rehabilitation in general, leading to the creation of programmes specifically designed for women [15]. Once engaged, most people attended at least five sessions (67%), and gave positive ratings (83%) for the programme with regard to it being enjoyable, helpful and well-facilitated.
Most people were in the mild–moderate range of symptoms on the HADS-D and BDI-II. Mild major depressive episodes are best treated by supportive counselling with psychoeducation and teaching of problem-solving skills [16], suggesting that BraveHeart would meet the needs of this population. Further work would need to be undertaken to determine efficacy in a group with higher levels of depression at baseline to determine its utility in that population.
Of all people screened, 8% commenced the programme (with 32% identified during screening as potentially benefiting from an intervention and 24% of those accepting). This is comparable to rates achieved from the Enhancing Recovery in Coronary Heart Disease (ENRICHD), MIND-IT and SADHART trials, where there was a 7%, 7% and 3% participation rate from all cardiac patients identified, respectively [5,6,17,18]. Eligibility criteria, however, were more stringent in these studies. Although the liaison psychiatry Identifying Depression as a Comorbid Condition (IDACC) trial had a higher participation rate (20% of all screened), eligibility rates were higher (43.4%) and the intervention was delivered while the patient was still in hospital [19]. These comparisons suggest that a group approach is as appealing to these patients as individual or medication approaches. Dropouts tended to discontinue after the first session, suggesting that patients decide early whether or not the group approach suits them. Although reasons for non-participation were not recorded, stepped care approaches that seek to deliver less intensive interventions first (e.g. brief interventions; bibliotherapy; Internet-based therapy) may start to provide additional appropriate treatment options to engage a proportion of the remaining three-quarters of the population of interest.
Because this was a pilot trial of a new intervention, the present study has two major limitations: absence of a control group, and absence of diagnostic information regarding depressive and anxiety disorders. A significant proportion of patients with depression after heart events spontaneously improve in mood with no intervention [20], and further work has involved evaluating BraveHeart in the context of a randomized controlled trial (RCT) [XXX: unpublished data, XXX]. The present pilot study recruited people with existing symptoms of depression and/or anxiety according to the HADS and conclusions cannot be made about responses based on diagnostic categories. Lesperance et al., however, were able to show that mild depression symptoms that do not meet criteria for a depressive disorder can impact on prognosis [21]. Although the BraveHeart RCT continues to have as its focus group people with mild or worse symptoms of depression, it includes a more comprehensive pre-treatment assessment and feedback session. Additional assessment includes structured diagnostic measures for depression and anxiety and disorders, cardiac risk factors, quality of life, and demoralization. It is expected that this RCT will provide additional information on the efficacy of BraveHeart as compared to a brief intervention (feedback and advice regarding treatment options) and on the patients for whom it is most appropriate and effective.
Overall, the present study resulted in the creation of a screening procedure and a group treatment programme for cardiac patients with depression and anxiety symptoms. Treatment resulted in significant reductions in symptoms of emotional distress. In Australia, group CBT has been found to be one of the most inexpensive depression treatments when delivered in a public setting, second only to bibliotherapy [22]. BraveHeart enables provision of a specialized medical psychology intervention that can be provided to large numbers of people with fewer resources than required by individual psychological therapy.
Footnotes
Acknowledgements
The authors wish to thank Colleen Grace and the cardiac rehabilitation nurses at the John Hunter Hospital, Newcastle, Australia, at the time of the evaluation; the patients participating in the programme; and Terry J. Lewin (Research Manager, Centre for Brain and Mental Health Research) for statistical advice. Evaluation of the programme was made possible through a bequest from Jennie Thomas in memory of Philip Emyln Thomas.