
Abstract
Volatile solvent abuse (VSA) is a worldwide problem, however petrol sniffing (also termed gasoline inhalation or huffing) is a form of VSA that occurs more commonly in disadvantaged or isolated societies, and the practice has become endemic in some remote Indigenous communities [1–3]. While petrol is not the only substance used, it can be the most accessible. In the Anangu Pitjantjatjara lands of South Australia, acquired brain injury from petrol sniffing has become the single biggest cause of disability amongst its people [3]. This may reflect the unique cultural, geographical, and social context surrounding remote Indigenous Australians, including a history of cultural oppression and dispossession, considerable geographical isolation, poor health and healthcare, as well as reduced employment and recreational opportunities. Impairments of psychomotor, memory, attention, learning and executive functions can be associated with petrol sniffing (or other solvent abuse) and these impairments can present prior to the more severe neurological symptoms such as ataxia, nystagmus and dementia [2,4,5]. Hence in individuals who abuse petrol, the measurement of cognitive function may be a useful tool for early detection of the adverse CNS effects of petrol abuse and for monitoring responses to rehabilitation strategies.
Impairment in cognitive function may reduce an individual's insight into their own behaviours and therefore on their desire or ability to seek or respond to treatment [6,7]. Furthermore, individuals with more severe cognitive impairments are more likely to drop out of rehabilitation or substance abuse treatment programs [6]. This may be because treatment programs often rely on cognitive skills such as memory, attention, and complex cognition in order to educate and achieve treatment outcomes [7,8]. Hence in addition to psychiatric, psychological, medical and social domains, cognitive function may be an important element to consider in the effectiveness of substance abuse treatment programs [9]. Clear identification of cognitive impairments would enable health practitioners to recommend and support access to treatment, and allow treatment providers to adjust the complexity or timing of treatment programs to accommodate any identified impairments, presenting more complex material as cognitive recovery proceeds [7]. For treatment providers, cognitive assessment is a useful tool to monitor the effects of abstinence and educate clients about the importance of treatment or the severity of their substance abuse. Rigorous evaluation of treatment outcomes is a key element for effective treatment programs [9] that may be strengthened substantially by inclusion of the robust psychometric indicators provided by cognitive assessment.
Conventional cognitive assessment tools can be inappropriate for Indigenous populations however, as they are typically developed in a Western European and American context and rely heavily on the use of English spoken and written language and on concepts that may be unfamiliar to Indigenous people [10]. Test interpretation can be difficult as standardisation samples are usually comprised of non-Indigenous individuals [10]. Performance impairments identified among different cultural or ethnic groups using conventional assessment tools may therefore arise from cultural or contextual determinants such as familiarity with Western European or American concepts, practices, language, or education, rather than being an accurate measure of cognitive function [11]. Appropriate assessment of any cultural group must therefore involve the use of culturally fair assessment tools where performance scores are interpreted with respect to the performances of individuals from the same group.
The CogState test battery is a set of non-verbal, computerised, cognitive tasks developed to be culturally neutral [11]. Designed in response to the need for appropriate cognitive assessments for Indigenous Australians, the test has since been applied more widely, with its scientific validity and clinical utility first demonstrated in various non-Indigenous as well as non-English speaking populations [11–13]. The validity and reliability of these assessment processes have also been established within healthy Indigenous groups [14,15] and they have been used to define specific cognitive changes associated with heavy episodic alcohol abuse in Indigenous Australians [16]. It is therefore likely that this same assessment process might be appropriate for the assessment of cognitive function for people in programs designed for the treatment of substance abuse.
The paper's aim was to investigate the utility of the cognitive assessment process for use in substance abuse rehabilitation programs. Study One considered the demographic (e.g., age) or contextual factors (e.g., locality) that may impact on cognitive performance in healthy Indigenous adults from regional and remote communities representative of those affected by petrol sniffing. Study Two investigated the nature and magnitude of cognitive impairment in Indigenous individuals who had abused petrol.
Methods
The procedure and apparatus were consistent across both Study One and Study Two and are described once here.
Procedure
Participants were recruited voluntarily from Indigenous secondary or tertiary education centres, drug rehabilitation centres, or an adult correctional facility in the Northern Territory. Indigenous specific secondary and tertiary education institutions in Darwin and Alice Springs (i.e., 4), were chosen to enable assessment of large groups of Indigenous people representing a variety of communities throughout the region. All known residential rehabilitation centres (i.e., 3) in Darwin and Alice Springs treating petrol sniffers at the time of the study were also selected. All organisations invited agreed to participate. Participants therefore represented over 25 different language groups, 60 distinct Communities, and geographical regions including the arid desert of Central Australia and the tropics of Northern Australia.
The joint Human Research Ethics Committee for the Department of Health and Community Services and Menzies School of Health Research granted ethical approval. All individuals attending treatment at the rehabilitation organisations during the 2-year period (2007–2009), who were present on the fortnightly study days, were invited to participate. All individuals attending health certificate courses at the tertiary education institutions, the entire student population of the secondary college, and all Indigenous medium security prisoners from the correctional facility who were present on the study days were invited to participate. Each participant (and a guardian if under 18 years old) gave written informed consent. Questionnaires eliciting demographic information (including age, education, community, medical history, etc.) and substance use histories (including frequency, amount, first and last use of alcohol, cannabis, solvents, cigarettes, kava or other drugs) were completed with the participants by trained researchers. Where available, this data was crosschecked with more detailed self report data, clinic notes, and proxy assessments using a consensual methodology described previously in this population [17,18].
Up to seven trained researchers conducted the assessments at the education, rehabilitation or correctional facilities with groups of up to 15 participants tested together at one time. The average ratio of supervisors to participants was 1:2. At the beginning of each task, the researchers explained the instructions and guided participants through a practice session in which they had one to five trials to demonstrate their understanding of the task. Following this, researchers explained that the practice was over and they would now do the ‘real test’. Completion of each task led straight into the practice session for the next task.
Apparatus
The CogState computerised cognitive test battery used here consisted of seven cognitive tasks selected, through previous research and consultation with Indigenous community members, to be suitable for assessing Indigenous Australians. The time for administration was approximately 20 minutes and stimuli in each subtest are presented repeatedly with data averaged over those presentations. Each has been described in detail elsewhere and is summarised below [14,15,19,20].
Card based tasks (see Figure 1A for onscreen presentation of task)
These tasks are in the form of card games with a playing card initially presented face down in the centre of the screen.
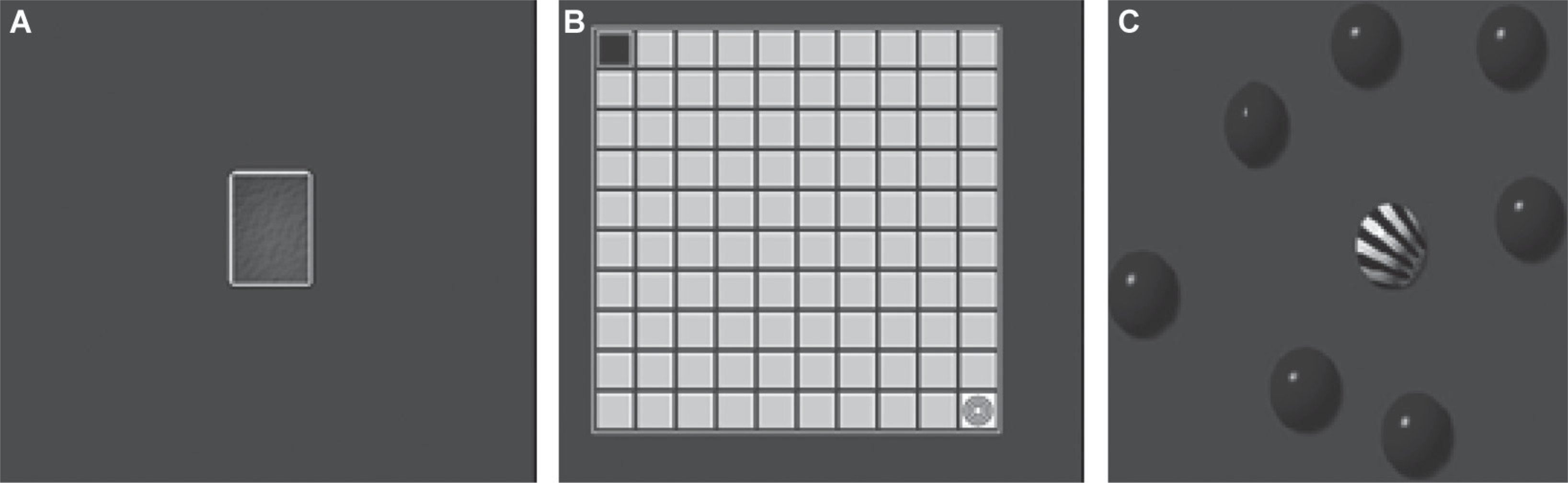
On-screen representation of card based tasks (A), Groton Maze Learning Test (B) and Continuous Paired Associate Learning task (C).
Detection task: The participant attends to the card and presses either the ‘K’ (if right hand dominant) or ‘D’ (if left hand dominant) key as fast as they can when the card turns face up. This is a simple reaction time task measuring visual attention and psychomotor function.
Identification task: The participant attends to the card and, when the card turns face up, follows the rule ‘Is the face-up card red?’. The ‘K’ and ‘D’ keys correspond to ‘yes’ and ‘no’ respectively (reversed if left hand dominant). This is a choice reaction time task measuring visual attention.
Visual learning task: Measuring working memory and attention, this task requires the participant to attend to the card and follow the rule ‘Have you seen this card before in this task?’ with ‘K’ and ‘D’ corresponding to ‘yes’ and ‘no’ respectively (reversed if left hand dominant).
Non-card based tasks
The other CogState tasks were presented using more complex visual displays.
Groton Maze Chase Test (GMCT; see Figure 1B for onscreen task layout): For this psychomotor task, a grid 10 tiles by 10 tiles is presented with a target tile in the top left. The participant has to click the target tile with the mouse and ‘chase’ it around the grid as it moves one tile at a time. The task continues for 30 seconds and records the total number of correct movements per second.
Groton Maze Learning Test (GMLT; see Figure 1B for onscreen task layout): Using the same grid as the GMCT, the participant uses the mouse to uncover a circuitous path, moving one tile at a time (across 29 ‘correct’ tiles), from one corner of the grid to the diagonally opposite corner. On the first presentation, the path can only be found using trial and error. Correct responses are indicated with a tick, and incorrect responses with a cross. If a cross is revealed, the participant must click on the last correct tile to continue. Once the pathway has been uncovered and completed, the task is repeated for four more rounds along the same path. This task measures executive function.
Groton Maze Learning Test – Delayed Recall (GMLT-R): Approximately 10 minutes after completing the five presentations of the GMLT, and with other tasks being completed in the interim, the grid is presented once more. The participant is required to remember the same hidden pathway as presented on the initial trials and complete it as quickly and accurately as they can. This task measures visual learning and memory.
Continuous Paired Associate Learning (CPAL) (see Figure 1C for onscreen task layout): This task measures learning and spatial awareness using a series of eight blue balls. During acquisition, the participant learns the location of six patterns, presented serially in individual balls leaving two ‘empty’ distracter balls. Then, one of the patterns is presented in a central location and the location of that pattern's matching pair has to be recalled and clicked with the mouse. The task will not progress until the location of the pattern is correctly recalled, and will continue until the locations of all six patterns have been remembered. After acquisition, this task is repeated for five rounds (locating all six patterns) with the patterns in the same location for each round.
Study One
Participants
Individuals were selected for Study One if: (1) their usual alcohol consumption was less than six drinks per occasion, or their consumption was between six and ten alcoholic beverages per occasion and last use was greater than 180 days ago; (2) they had never abused volatile solvents regularly (i.e., > 1 time); and (3) they had not abused any other drugs (excluding cannabis) regularly (i.e., > 1 time). Because concurrent cannabis use was common in our sample of petrol sniffers and due to its increasingly widespread use in Indigenous communities, this will be factored into the analyses described below [21,22]. Exclusion criteria included self reported psychiatric conditions or use of psychotropic medications. These individuals represented a naturalistic sample of Indigenous Australians (N = 206; 95 males and 111 females) aged between 11 and 68 years (M = 28.03, SD = 13.45) from urban, rural or remote areas.
Data analysis
A series of standard linear multiple regression analyses were conducted on data from this group to identify any relationship between performance measures and six demographic factors: age, education, level of remoteness (locality), regular long-term cannabis use, gender, and familiarity with computers (computer familiarity). Age, education, and locality were continuous variables and cannabis use (yes/no), gender (female/male), and computer familiarity (used a computer before/not used a computer before) were dichotomous variables. Daily or near daily use of cannabis for greater than 5 years has been associated with subtle cognitive impairment in non-Indigenous users [23]. Therefore, regular long-term cannabis use was defined as use of cannabis more than five times per week for greater than 5 years. Locality was defined by the Accessibility/Remoteness Index of Australia (ARIA+) for the participant's home community. This is the standard Australian Bureau of Statistics endorsed measure of remoteness and is expressed as a number on a scale from 0 (least remote) to 15 (very remote) [24].
Speed (reaction time and duration) measures were recorded in milliseconds. These measures were transformed using logarithmic (base 10) transformations and accuracy data (number of correct responses divided by number of presentations) for the card tasks were transformed using arcsine transformations as prescribed by the test developers and to achieve normal distributions [12,13,20,25]. Total number of errors for GMLT-R and CPAL exhibited very minor skew. Transformation of these variables resulted in no change to the substantive interpretation of the analyses, so results using untransformed data are presented to enable more meaningful interpretation. All other variables, including moves per second (mps; number of correct moves divided by total duration), had normal distributions. Data analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 16.0 (SPSS Inc; Chicago, IL, USA). Initial inspection of the data indicated 37 univariate outliers (greater than 2 SD from the mean) across the 15 measures which were removed. Four multivariate outliers were removed from the regression analysis for the GMCT and one was removed from the mps measure of the GMLT. As the number of statistical comparisons was high due to the exploratory nature of the study, significance levels for the tests were set at α < 0.01 to reduce the risk of Type I error.
Results
The multiple regression analyses indicated that the 6 predictors together accounted for a significant proportion of the variance in: Detection speed (F (6, 185) = 4.27; P < 0.01); Visual Learning accuracy (F (6, 184) = 5.05; P < 0.01); GMCT mps (F (6, 182) = 20.75; P < 0.01); GMLT mps, and log duration (F (6, 180) = 15.14, P < 0.01; F (6, 182) = 14.79; P < 0.01, respectively); GMLT-R mps, and log duration (F (6, 172) = 7.38, P < 0.01; F (6, 177) = 9.12, P < 0.01, respectively) and CPAL log duration and errors (F (6, 179) = 21.95, P < 0.01; F (6, 176) = 6.26, P < 0.01, respectively). There were no violations of the assumptions apart from some very slight heteroscedasticity on GMCT mps, GMLT mps, and GMLT–R mps. Mean scores, values for R, R 2 and semi-partial correlations (sr2) for significant predictors are presented in Table 1. Age and computer familiarity accounted for the greatest amount of unique variability for the more complex, non-card based measures with better performance (faster or more accurate) for those who were younger and those who had used a computer before. Age and education impacted significantly on just one of the simpler card based tasks (i.e., Detection). Those of younger age and those with more years of education had better reaction times than older or less educated participants. As age was the most significant predictor of performance (up to 22% of the unique variance explained), particularly on the more complex speed measures, these effects were investigated in more detail by expressing figuratively performance by six age categories (i.e., under 15s, 15–18, 19–29, 30–39, 40–49 and 50+). Results indicated a gradual worsening in performance with increasing age, beginning primarily around the 30s but in some cases beginning in the late teens with a plateau in young adulthood (20s–40s).
R, R2 and significant semi-partial squared correlations for multiple regression analyses (Study One)
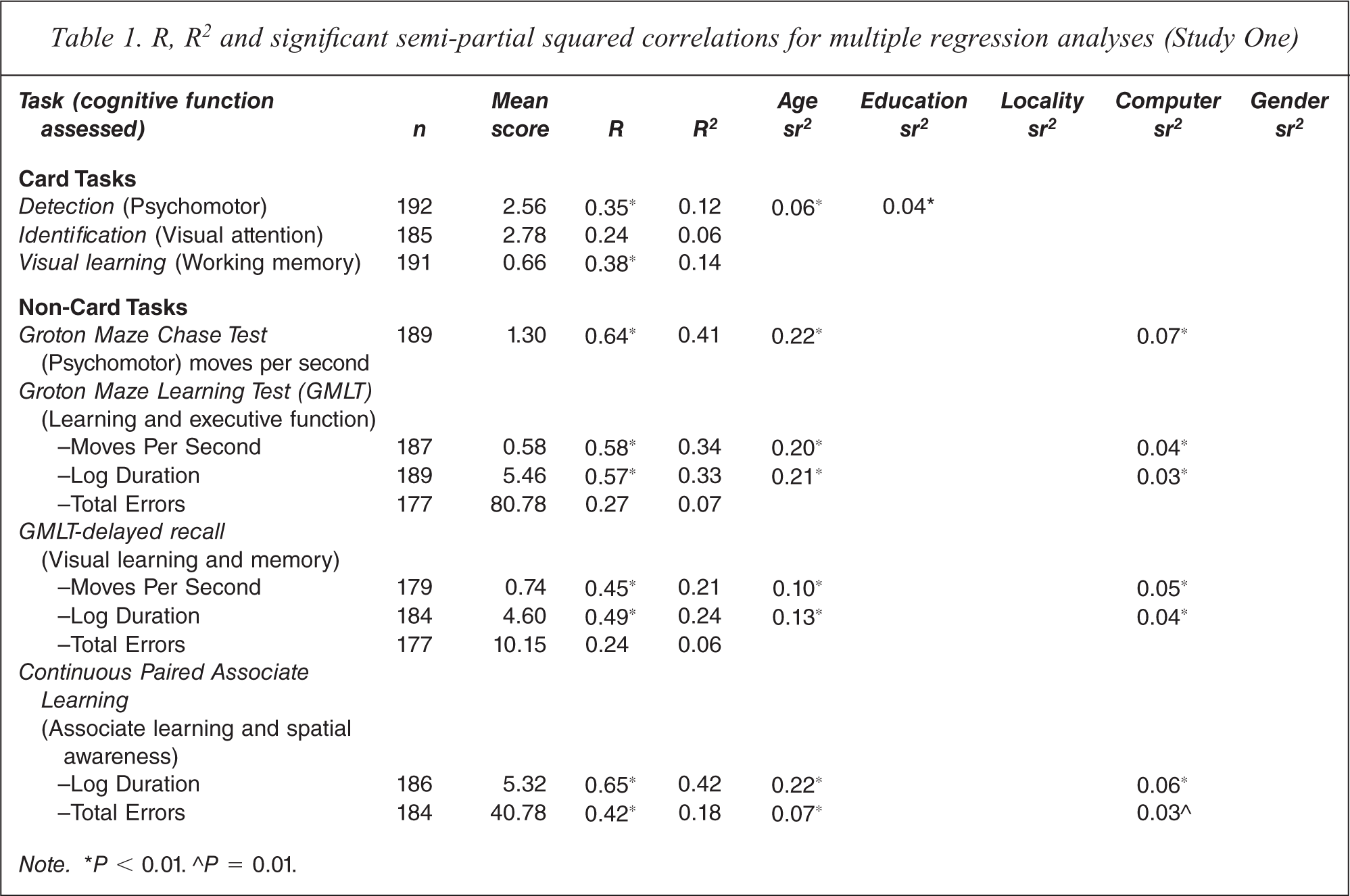
Note. ∗P < 0.01. ∘P = 0.01.
Study Two
Participants
Participants 25 years or younger who were classified as either healthy controls (from Study One; n = 96) or current petrol sniffers (n = 50) were included in this study. Petrol sniffers were defined as those who inhaled petrol regularly or episodically and had done so within the past 60 days (but not < 12 hours prior to testing). These individuals had been excluded from analysis in Study One due to their history of petrol sniffing. Five participants had inhaled substances other than petrol (i.e., paint, glue or aerosols); however, removal of these participants resulted in no change to the significance or magnitude of results so their data were included. Frequency of petrol sniffing ranged from once per week to everyday with the majority sniffing daily. Demographic characteristics of the two groups are presented in Table 2.
Demographic characteristics of controls and petrol sniffers in Study Two
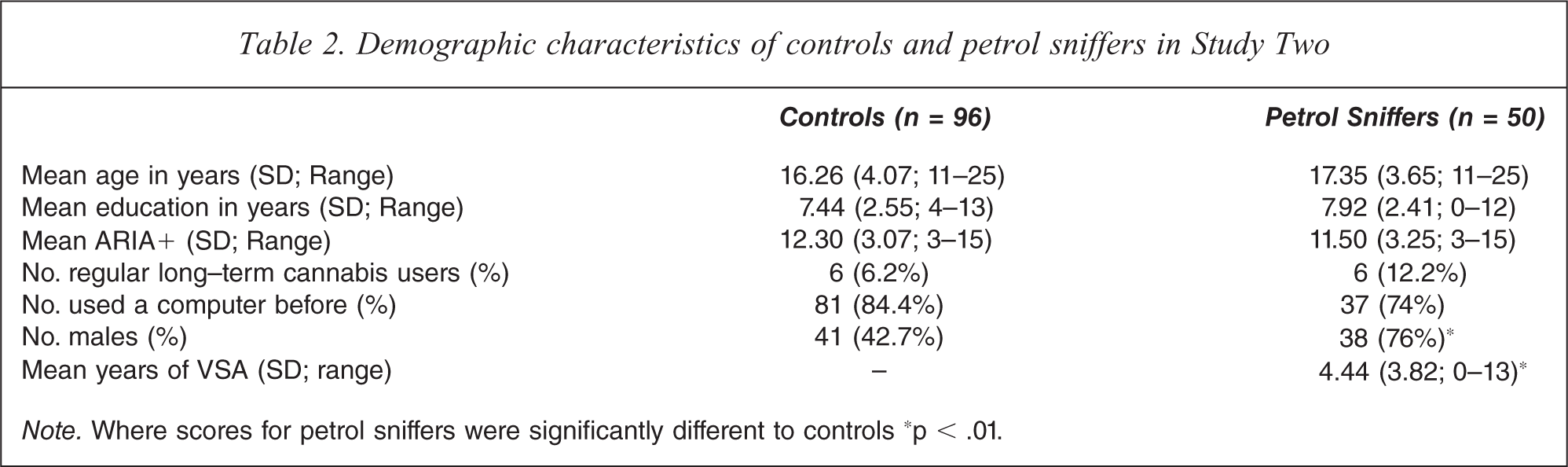
Note. Where scores for petrol sniffers were significantly different to controls ∗p < .01.
Data analysis
Independent groups t-tests and chi-square analyses were conducted to investigate whether the groups were equal on those factors found in Study One to impact on cognitive performance (i.e., age, education, computer familiarity). Independent groups t-tests with each of the cognitive measures as dependent variables were then used to identify any differences in cognitive performance between the two groups (controls and petrol sniffers).
Speed and accuracy measures were transformed as per Study One to achieve normal distributions. Total errors for GMLT was slightly skewed, however transforming the data resulted in no change to the substantive interpretation, so results from untransformed data are presented. All other variables had normal distributions. Initial inspection of the data resulted in removal of 39 univariate outliers (greater than 2 SD from the mean) across the 15 measures. Significance levels were again set at α < 0.01 to reduce the risk of Type I error.
Results
Mean age (t (141) = −1.97; P = 0.051), years of education (t (141) = −1.25; P = 0.21), and proportions of individuals who had or had not used a computer before (χ2 = 2.19; P = 0.14; continuity correction) were not significantly different between the controls and petrol sniffers (see Table 2). Petrol sniffers had significantly worse performance compared to controls for Identification speed (t (135) = −3.67; P < 0.001), GMCT mps (t (138) = 8.64; P < 0.001), GMLT mps (t (135) = 4.84; P < 0.001), GMLT log duration (t (130) = −4.68; P < 0.001), GMLT total errors (t (52) = −2.82; P < 0.01; equal variances not assumed), GMLT-R mps (t (131) = 4.18; P < 0.001), GMLT-R log duration (t (131) = −4.49; P < 0.001), CPAL log duration (t (137) = −6.35; P < 0.001), and CPAL total errors (t (125) = −5.79; P < 0.001; see Table 3). Levene's test of homogeneity of variance was significant for Visual Learning accuracy, and GMLT total errors so SPSS results with equal variances not assumed are presented for these variables. Effect size estimates (Cohen's d) are presented in Table 3 suggesting medium to large effect sizes (0.66 to 1.52) for significant measures, according to Cohen's classifications [26].
Group means (standard deviations) and effect sizes for each of the cognitive measures (Study Two)
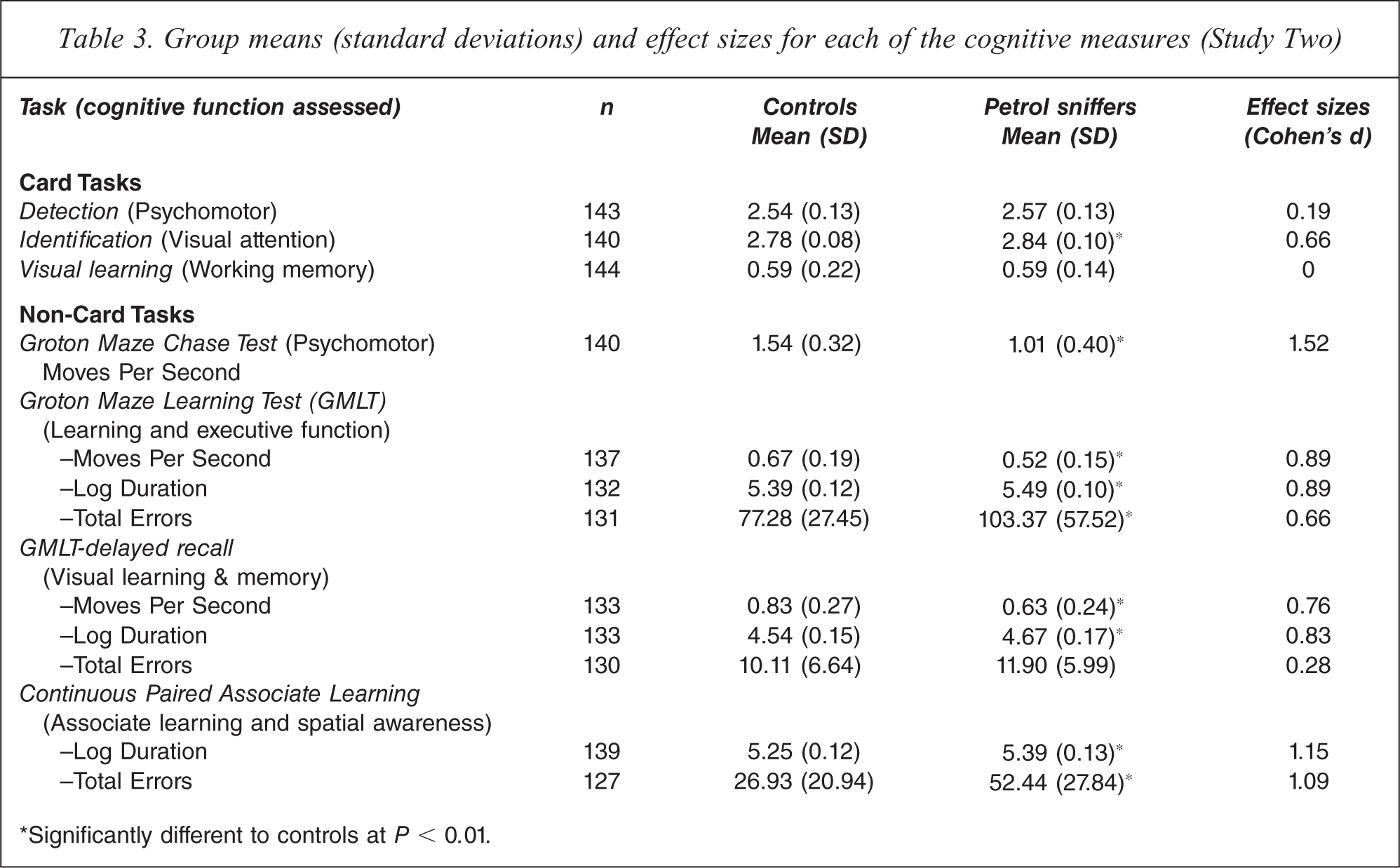
∗Significantly different to controls at P < 0.01.
Discussion
Age, computer familiarity, and education were shown in Study One to impact on the cognitive performance of a group of healthy Indigenous Australians. While the amount of unique variance accounted for by computer familiarity and education was low (between 3 and 7%), age accounted for up to 22% of the unique variance in performance on some measures. Education impacted only on the simplest card based task (i.e., Detection) and age and computer familiarity impacted predominately on the more complex tests of learning, memory, psychomotor and executive functions. Study two demonstrated that after controlling for these demographic factors, petrol sniffers showed significantly poorer performance on tasks of visual attention, psychomotor skills, executive function, visual learning and memory and spatial awareness with up to 1.5 standard deviations separating the means of the two groups. This poorer performance was evidenced primarily by significantly reduced speed but also reduced accuracy on the more complex tasks with the greatest deficits (large effect sizes) observed for the psychomotor, learning and executive function, and spatial awareness domains.
The significant impact of age and familiarity with computers on performance is consistent with findings from another study using this test in older, non-Indigenous people [27]. The significant effect for age may be expected considering the large range of ages represented in Study One. Graphing performance by decade in general revealed gradual cognitive declines across the years, beginning primarily around the 30s but in some cases from the late teens with a plateau in early adulthood. Age related cognitive changes, such as these, are expected across the lifespan. Finding age to have the greatest impact on performance is consistent with previous studies in adults (aged 18–90) demonstrating that age is the strongest and most consistent predictor of memory performance [28].
The relatively small but significant effect of computer familiarity highlights the importance of familiarity and underscores approaches taken where the test can be repeated until the individual's understanding of the task has been demonstrated. A recent study using CogState in older non-Indigenous people also found an association between low computer familiarity and slower initial performance that did not persist with subsequent testing [27]. This indicates that it is possible to overcome a lack of familiarity by allowing people to do multiple tests. These results also suggest that the lower performance for some Indigenous people was not related to their ethnicity per se rather it is merely a function of computer experience and reflects similar findings in non-Indigenous groups. Taken together the results of Study One indicate that the test battery can be used appropriately with Indigenous people.
In Study Two, petrol abuse was associated with significantly reduced performance (between 0.7 and 1.5 SD) compared to healthy controls for the more complex tests of psychomotor function, memory, learning, executive function, and spatial awareness. Fewer differences were found however between petrol sniffers and controls on the simpler tests of psychomotor function and working memory. While this suggests that complex cognition and attention may be significantly compromised (with medium to large effect sizes) in those attending rehabilitation for petrol abuse, it also suggests that simpler cognitive processes may remain relatively intact. These findings reflect those of similar studies in Indigenous populations where recreational petrol abuse was associated with severe memory and attentional impairments but performance on simpler tests (e.g., simple and choice reaction time) remained unimpaired [5,29]. Removal of individuals who had abused only other solvents (e.g., paint, glue) from the analysis resulted in no change to the results. Volatile solvents such as petrol, paint, and glue comprise varying combinations of aliphatic and aromatic hydrocarbons including xylene, toluene, n-hexane and benzene which are highly lipid soluble [30]. Previous research demonstrates similarities between the pharmacological and neurotoxic effects of these substances that reflect similarities in their composition [5,29–32]. The results from this study may therefore also apply to other solvent abusers and not just to petrol sniffers.
Cognitive performance deficits such as those reported here and in other studies may be the first sign of more severe or irreversible neurological damage [5,29]. Previous research suggests that rehabilitation clients with cognitive deficits tend to make less clinical progress, spend less time in treatment and participate less throughout the treatment process [6]. The specific relationship between baseline cognitive performance and treatment outcome for this population should therefore be investigated. Previous research also suggests however, that some degree of cognitive recovery can occur with abstinence from further petrol abuse [31,33]. The treatment process might therefore be enhanced if rehabilitation centres actively monitored cognition and individual programs were modified to accommodate any cognitive impairments by delaying introduction of complex material until improvements in cognitive function are observed. Ongoing monitoring of cognition throughout the treatment process might therefore be beneficial, not only to inform the treatment process, but also to educate and illustrate to clients the effects of their substance use behaviours. More research is needed however to investigate the value of actively monitoring cognition and adapting programs to accommodate identified impairments in relation to treatment outcome. Future research should also investigate the utility of this process to assess substance abuse related cognitive changes over time.
The assessment of participants in small groups may be considered a limitation of this study as interference, distraction, and learning through observation may have introduced unexplained variance into the data. One to one supervision of participants might have enhanced the data collection process by minimising motivational or compliance issues. However, group assessments are a common method of data collection using this tool [12–15] and a ratio of supervisors to participants of 1:2 was generally achieved. With this ratio, the appropriate supervision of participants was manageable and the impact of non-compliance minimal. In treatment settings, this issue is likely to be further eliminated if assessments are conducted on initial intake interview or within one to one counselling sessions.
While Study One indicated that the impact of age and familiarity with computers should be considered when assessing the cognitive performance of Indigenous Australians with computerised assessments, other factors such as locality and gender, do not appear impact substantially on performance in this sample. Study Two identified reduced cognitive performance in petrol sniffers that worsened as the complexity of the task increased. The utility of the computerised cognitive assessment battery for detecting substance abuse related impairments for Indigenous petrol sniffers in primary care settings was demonstrated. These results provide a basis from which future research can occur investigating the specific relationships between cognitive performance patterns, defined level and type of substance abuse, and treatment outcomes.
Footnotes
Acknowledgements
This paper was supported by a project grant and a Training Scholarship for Indigenous Australian Health Research from the National Health and Medical Research Council of Australia (grant number: 383587). The funding source had no input into the preparation of this manuscript.