
Abstract
Adverse effects of cannabis use on mental health are becoming increasingly well documented [1]. For example, cannabis use is associated with psychological responses ranging from mild changes in mood and lack of motivation [2], [3] to symptoms of anxiety [4] and depression [2],[4–7]. There is equivocal evidence that cannabis use is implicated in suicidal ideation [8], [9]. Acute reversible psychotic symptoms are likely with intoxication, but whether cannabis causes psychoses is more contentious [2], [10]. Importantly, cannabis use is associated with serious mental illness such as schizophrenia [2], [6],[10–14]. There is evidence of dependency [2], [15], withdrawal syndromes [16], [17] and acute cognitive impairment [18], while long-term cognitive impairment associated with cannabis use [19] also remains contentious [20]. The present study considers whether such adverse effects have emerged in indigenous Australian cannabis users in remote communities in the Northern Territory (NT), where a recent rapid rise of regular cannabis use has occurred [21].
In remote communities in eastern Arnhem Land and in others across the NT's ‘Top End’, cannabis use was rare in the late 1980s [22] and early 1990s [23]. By 1999, around 41% of men and 12% of women in younger age groups (16–29 years) were using cannabis [24], although few of these used the drug regularly (A. Clough, unpublished data). In one locality in eastern Arnhem Land, in just over a year, between 1999 and 2000, cannabis use doubled among men and emerged among women for the first time [24] suggesting that its use was still expanding in those years. It is of interest that this increase in cannabis use occurred in adults of all ages, largely from the late 1990s [21], [24]. However, the prevalence of cannabis use in the rest of Australia increased steadily throughout the 1990s [25], although rates increased more rapidly in younger age groups [26]. There is nowevidence to suggest that regular use of cannabis has become common in Arnhem Land. For instance, in 2002 in eastern Arnhem Land, those using cannabis on at least a monthly basis constituted 67% of men and 22% of women aged 13–36 years [27]. In similar age groups (14–29 years) around 14–20% of men and 9–10% of women in the rest of Australia reported using it at least monthly [28]. One possible consequence of this increased, widespread and regular use of cannabis in Arnhem Land populations is increased levels of the adverse mental health effects thought to be associated with the drug.
Method
Summary of approach
To meet challenges posed by difficulties of cross-cultural communication, language barriers, culturally circumscribed psychological experiences and limitations of standard diagnostic tools in such settings, we worked with local indigenous health workers to develop descriptive criteria that we believed reflected symptoms of mental health effects. We then applied the criteria (converted into questions) in interviews with cannabis users. We categorized the criteria into clusters of symptoms using interview data and compared these with a categorization based on a clinical interpretation of the criteria. Each participant was then classified as showing, or not showing, the symptoms in each cluster. Finally, associations between each symptom cluster and levels of cannabis use reported by study participants were assessed.
Setting
The two communities studied are located approximately 550 km east of Darwin, in eastern Arnhem Land with a combined indigenous population of 2649 (1180 aged 13–36 years) [27], [29]. Traditionally, the communities did not share their first language although they are contiguous and have a history of social interaction and intermarriage with traditional cultural practices largely intact [30], [31]. Today, English is a third language at best and with skills that vary greatly. Substances used in these communities include tobacco, alcohol and kava (in one locality) [24], the latter two substances being available on restricted bases [32], [33]. Petrol sniffing was common in the region during the late 1980s and early 1990s [23], [24] but is now greatly reduced [27].
Sampling
Local health workers built trust, making it possible to conduct interviews about highly stigmatized and illegal substance use behaviours. Health workers helped to recruit participants, to conduct interviews in the appropriate language and to overcome communication difficulties with some participants who appeared to suffer residual cognitive impairment, possibly related to past petrol sniffing or other substance abuse. A sample of 180 people (107 male and 73 female) aged 13–36 years was approached for interview concerning their patterns of substance use. Random sampling was not feasible, so convenience sampling was used with quotas in six age categories (13–16, 17–20, 21–24, 25–28, 29–32 and 33–36 years) and in men and women. Data for individuals who were under the influence of cannabis when interviewed were not included.
Exposure measures
Lifetime and continuing substance use were validated using selfreport combined with proxy assessments provided by up to five health workers interviewed separately and confirmed by documentary evidence (community health centre and hospital discharge records) [34], [35].
Participants reported their cannabis use by indicating the number of plastic packets (40mm×50 mm) of cannabis they purchased per week [27]. Cannabis is usually mixed with tobacco and smoked using handmade metal ‘cones’ in plastic ‘bucket bongs’ fashioned from soft-drink containers. Participants described their usual pattern of use (frequency of use and number of ‘cones’ smoked) and the duration (number of years) of their cannabis use [27].
Clusters of mental health symptoms
In constructing our criteria, we were guided by the Composite International Diagnostic Interview (CIDI) [36] and its shorter version the Mini-International Neuropsychiatric Interview (MINI) [37], the CAGE (Cut down, Annoyed, Guilty, Eye-opener) [38], [39] and the Alcohol Use Disorders Identification Test (AUDIT) [40] instruments. We also considered whether cannabis use could exacerbate mental health effects brought about by spiritual sorrow, disempowerment and deprivation experienced by indigenous Australians [41], [42], the possible unusual types of depression experienced by those living in small, closed communities [43] and the impact of traditional ‘payback’ and sorcery practices on mental health [44], [45], and so we avoided prompts which could lead to bias in responses framed in terms of these effects. We converted the 28 criteria into 28 questions and elicited ‘yes’ or ‘no’ answers in interviews.
Data analysis procedures and statistical methods
Identifying clusters of symptoms
A hierarchical cluster analysis was performed (SPSS v 11.0) using binary (‘yes’/‘no’) answers to the 28 questions provided by 103 participants. An unsupervised centroid method for complete linkage was chosen using Jaccard's similarity measure to emphasize differentiation between larger clusters and to give greater weight to the joint presence of criteria [46], [47].
A psychiatrist (R. Parker) with more than 20 years experience in ‘Top End’ Aboriginal communities, who was not party to developing the criteria or questions and who was blinded to interview data, classified and named clusters of symptoms implied by the questions using his own clinical criteria, observations and experience. He also identified pairs of criteria which, in his view, best characterized the symptoms imputed to each cluster. Five clusters of 28 criteria were described as indicating symptoms of ‘anxiety’, ‘dependency’, ‘mood’, ‘psychosis’ and ‘vegetative’ effects (48–50].
Criteria and questions used in interviews with 103 cannabis users in remote indigenous communities in Arnhem Land (NT) and their categorization into clusters of symptoms using cluster analysis
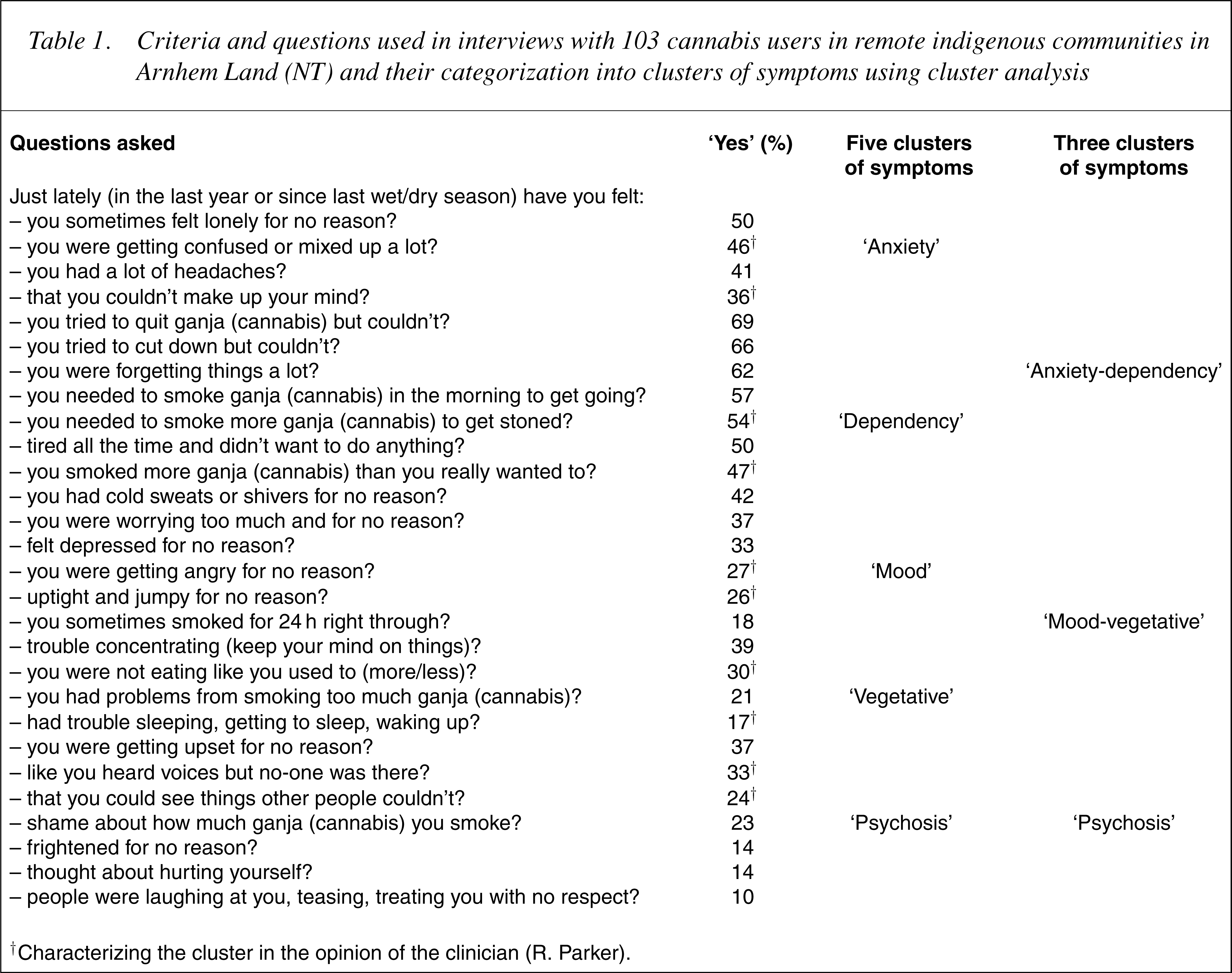
†Characterizing the cluster in the opinion of the clinician (R. Parker).
A participant was described as displaying the specific symptom cluster if they responded ‘yes’ to half or more of the questions comprising that cluster.
Associations between symptom clusters and exposure to cannabis and other substance use
Univariate logistic regressions (Stata 7.0) were performed using data for 103 participants on exposure to cannabis use (independent variables) and each symptom cluster (dependent variable). Multivariate analyses adjusted for likely confounders and considered interaction effects of other substance use in logistic regression models. The Wilcoxon signedranks test (Stata 7.0) was used to compare ordinal measures.
Ethics
The joint ethics committee of Menzies School of Health Research and NT Department of Health and Community Services provided approval, subject to a risk management strategy to avoid legal compromise for participants and researchers. All participants gave written informed consent after ethical and legal risks were explained to them.
Results
Summary of results from interviews
Approximately 73% (131/180) of participants had used cannabis at some time in their lives with 93% of these (n=122) continuing to use it. Of 122 continuing cannabis users, 103 answered all 28 questions and of these, 22% (n=23) answered ‘yes’ to at least 15 questions (median=10 questions, range=0–23). A ‘yes’ answer was recorded most frequently to the question of whether the participant tried to quit cannabis but could not (69%) and least frequently to whether the participant perceived people to be laughing at them or that others treated them with no respect (10%) (Table 1). The number of ‘yes’ answers to the 28 questions (data not shown) was associated with number of packets of cannabis usually purchased per week (Wilcoxon signedranks χ2 =7.7, p=0.021), cones usually smoked per week (χ2 =11.9, p=0.018) and frequency of use (χ2 =8.1, p=0.017), but not with years used (χ2 =2.4, p=0.492).
Average age of 103 cannabis users was 22 (SD=5.8) and 58% (n=60) were male, 15% usually purchased two packets per week or more, 18% usually smoked more than five cones per week, 35% had used cannabis for more than 5 years and 25% used it daily while 85% used tobacco, 55% alcohol, 16% kava, 50% had sniffed petrol and 5% still sniffed it.
Proportions of participants showing symptom clusters were: ‘dependency’ 51%, ‘anxiety’ 33%, ‘mood’ 23%, ‘psychosis’ 14% and ‘vegetative’ 11%. Some 46% showed ‘anxiety-dependency’ while 22% displayed ‘mood-vegetative’ symptoms.
Identifying clusters of symptoms
‘anxiety’ by confusion and indecision; ‘dependency’ by tolerance and difficulties controlling consumption; ‘mood’ by anger and irritability; ‘psychosis’ by auditory and visual hallucinations; and ‘vegetative’ by disturbances to eating and sleeping (Table 1).
At the penultimate level, the cluster analysis combined the ‘anxiety’ and ‘dependency’ cluster into one, the ‘mood’ and ‘vegetative’ cluster into a second, leaving ‘psychosis’ as the third (Table 1). Since agreement between the cluster analysis and the clinician's grouping increased to 71% (κ =0.56, p<0.001) (data not shown) at this level, associations between these three clusters and cannabis use were investigated.
Associations between three symptom clusters and measures of exposure to cannabis and other substance use
In univariate analyses (Table 2), statistically significant associations were found between ‘anxiety-dependency’ and ‘mood-vegetative’ clusters and number of cones usually smoked per week. ‘Anxietydependency’ was also associated with frequency of cannabis use. Possible confounding effects of alcohol use and a history of petrol sniffing were suggested by their statistically significant associations with the ‘anxiety-dependency’ symptom cluster. There were no associations found for the ‘psychosis’ cluster (Table 2).
Crude (univariate) associations between three symptom clusters and measures of increased exposure to cannabis use and with other substance use in 103 cannabis users in remote indigenous communities in Arnhem Land (NT)
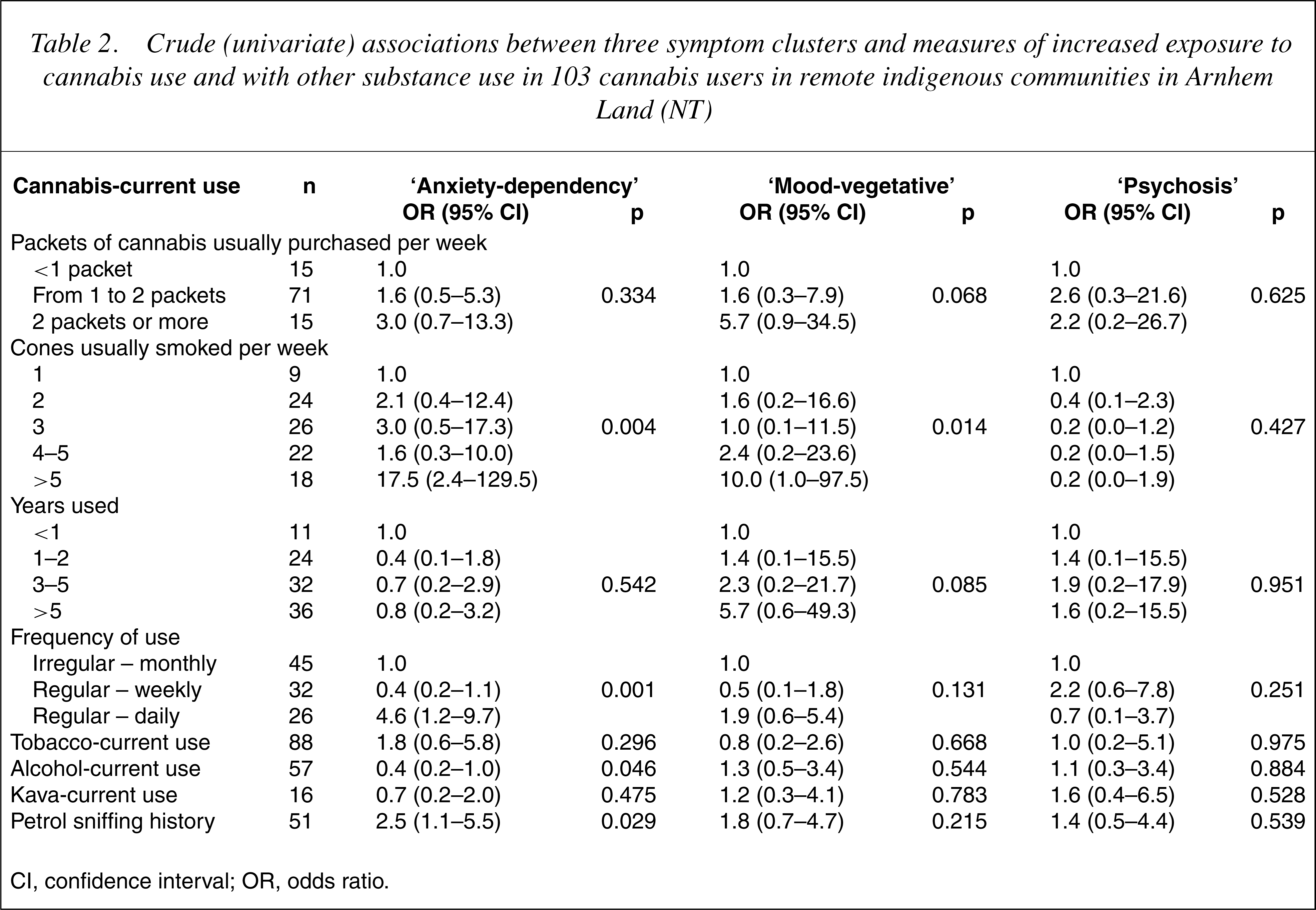
CI, confidence interval; OR, odds ratio.
Multivariate analysis of statistically significant crude associations between two symptom clusters and measures of increased exposure to cannabis use with adjustment for confounders in 103 cannabis users in remote indigenous communities in Arnhem Land (NT)
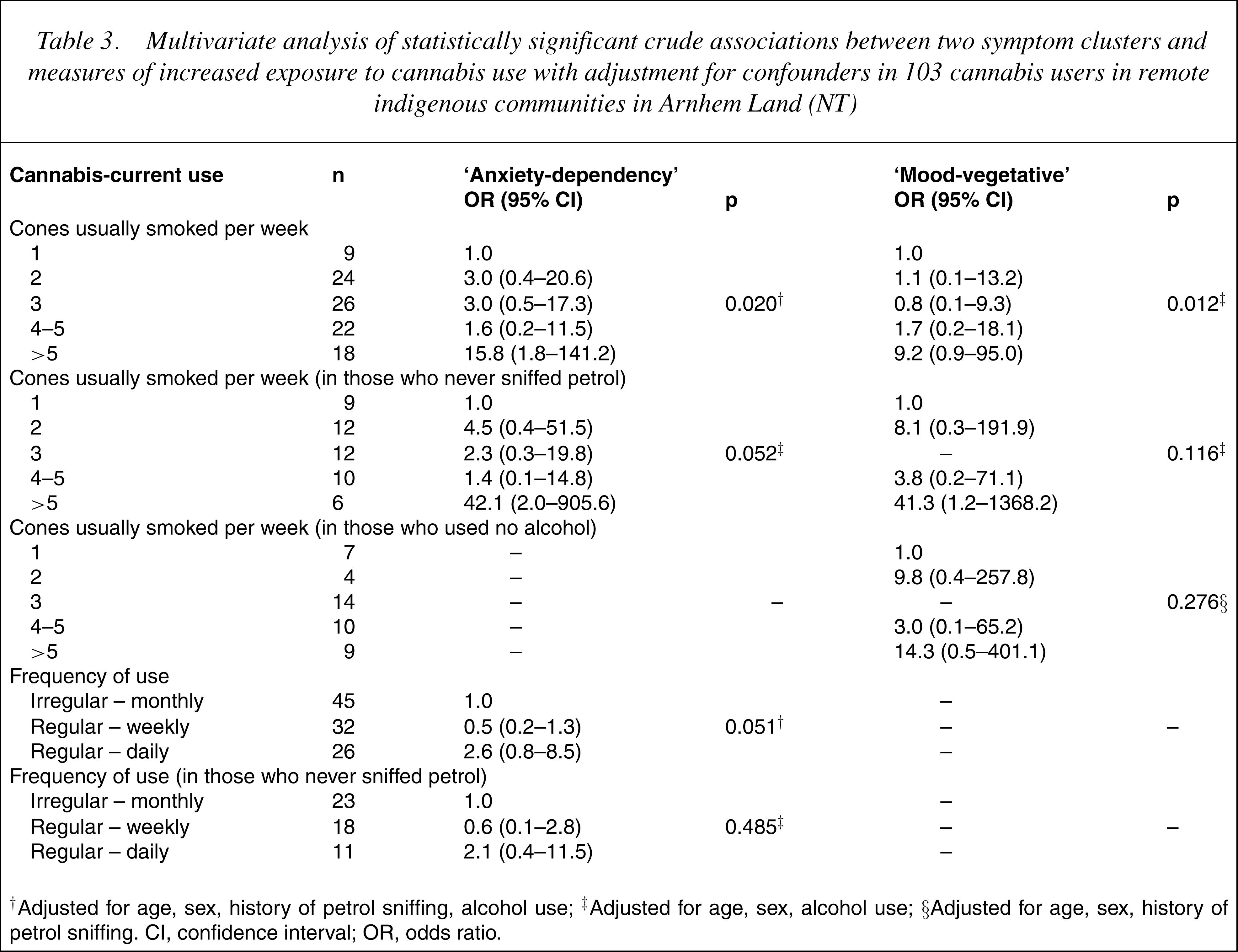
†Adjusted for age, sex, history of petrol sniffing, alcohol use; ‡Adjusted for age, sex, alcohol use; §Adjusted for age, sex, history of petrol sniffing. CI, confidence interval; OR, odds ratio.
Strong interaction effects, however, were found in the model of the association between number of cones usually smoked per week and alcohol use in the ‘mood-vegetative’ cluster (likelihood ratio χ2 =9.2, p=0.010) (data not shown) which suggests that any effect of cannabis use on this symptom cluster was distorted by independent effects of alcohol use. In those who used no alcohol, and when adjusted for confounding effects of age, sex and a history of petrol sniffing, the association between the ‘mood-vegetative’ cluster and number of cones usually smoked perweekwas no longer significant (Table 3), suggesting that alcohol use, along with petrol sniffing, combined to modify any independent role of cannabis in the expression of a ‘mood-vegetative’ effect.
Discussion
The aim of this study was to investigate the association of cannabis use with adverse mental health effects in Indigenous Australian populations in the NT.
Summary of main results
The lack of convincing associations between any symptom cluster and the variable describing years of exposure to cannabis use suggests that the associations found with other measures of exposure to cannabis use were due more to the acute effects of cannabis rather than its longterm influences. Hence, the effects observed emerged even though many participants had used cannabis for just a few years (median=4 years, range=0.5–18 years [27]). Also supporting the existence of an independent effect of cannabis is that, where crude associations with symptom clusters occurred, trends in odds ratios indicated an increased risk for symptoms with increasing exposure to cannabis use, that is, a dose–response effect (Tables 2 and 3).
‘Psychosis’ was not associated with measures of increased exposure to cannabis use. There were, however, statistically significant crude associations between ‘anxiety-dependency’ and number of cones usually smoked per week and with frequency of cannabis use. Furthermore, the association between ‘anxiety-dependency’ and number of cones usually smoked per week remained statistically significant after adjusting for confounders and showed little or no interaction effects with either petrol sniffing or alcohol use. Although data were too few to precisely describe these effects at different levels of exposure, those who smoked more than five cones per week were more likely to meet criteria for ‘anxiety-dependency’ than those who usually smoked one cone per week (OR=15.8, 1.8–141.2, p=0.013).
Crude associations between the ‘mood-vegetative’ cluster and number of cones usually smoked per week were modified by effects of alcohol and petrol sniffing in the multivariate analyses. Given close associations between cannabis use and a history of petrol sniffing in this population [24] and given petrol sniffing's likely clinical impact on normal brain function [51], [52], it is not surprising that it was a major confounder of independent effects of cannabis use in this study.
Limitations of the study
Since we did not attempt to validate or apply the criteria in those who did not use cannabis, we could not adequately examine the extent to which cannabis use adds to the mental health burden in the population as a whole in the communities studied. Future studies would ideally make comparisons with those who have never used cannabis but would recognize the difficulties of identifying control groups given that 4–16% of study participants in these populations may deny they have ever used cannabis [34].
It is plausible that the author who developed the criteria and analysed data from both the clinician's categorization and the cluster analysis (AC) and who was also directly involved in interviews with participants, inadvertently exercised bias in forming clusters. Cluster analysis is a qualitative technique which relies on the analyst's interpretation and is well known to return different classifications depending upon the grouping method and similarity measure used [46], [47]. The clinician was blinded to the development of the criteria and to the measures of exposure to cannabis use and to subsequent analyses. Without additional external data to describe the criteria, comparing the cluster analysis with the clinician's classification was the most effective way to conduct significance tests on the criteria used to create clusters [46].
Possible adverse mental health effects due to cannabis use
The data indicate that the risk of some symptoms of mental health effects increase as cannabis use increases in this population of largely traditional indigenous Australians who have only recently become exposed to the widespread availability of cannabis in their communities. These effects appear to be manifest as, at least, a cluster of symptoms of ‘anxiety-dependency’ including such symptoms as memory impairment, fragmented thought processes and confusion, indications of tolerance to the effects of the drug, withdrawal effects and difficulties in controlling consumption. Such effects are recognized in the published works [1], [2], are known to be dose-related and to be aggravated in näive cannabis users [2], [4], [10]. Whether these effects are due to toxic effects of cannabis intoxication or represent a chronic psychosis [2], [3], could not be determined from the data.
The data also suggest that symptoms of persistent fatigue are present but an amotivational syndrome would be difficult to distinguish from effects of ongoing, frequent intoxication in regular users [2]. Although criteria characterizing the ‘mood-vegetative’ cluster included irritability along with eating and sleeping difficulties, which are possible adverse effects of cannabis use [2], their interpretation would require consideration of the effects of alcohol use and petrol sniffing in further studies.
Any effects of cannabis on more serious mental health effects such as depression and suicidal ideation, and any effects on pre-existing mental illness were not indicated and, if they existed, would probably have been masked by effects of petrol sniffing and alcohol abuse. For instance, when participants were asked whether they had thought about hurting themselves in the preceding year, 14% (n=14) said ‘yes’ (Table 1). There was no association between a ‘yes’ response to this question and any of the measures of exposure to cannabis use or to alcohol use. However, the risk that participants had thought about hurting themselves in the preceding year was more than four times greater in those who had a history of petrol sniffing compared with those who had not sniffed petrol (OR=4.3, 1.1–16.7, p=0.020, adjusted for age and sex).
Given that around two-thirds of men and one-fifth of women aged 13–36 years in these communities may be using cannabis [27] and that some 46% of cannabis users may show the kinds of ‘anxiety-dependency’ symptoms described here, it is likely that mental health practitioners in these localities will find these symptoms frequently. Finally, given the dearth of formal studies of adverse mental health effects of cannabis in these populations, further research is warranted, particularly to examine the interactions between the effects of cannabis use, concurrent alcohol use and petrol sniffing.
Footnotes
Acknowledgements
The study was funded by a grant from the National Health and Medical Research Council (Australia) and the Population Health Division of the Commonwealth Department of Health and Ageing (NIDS #042). The authors declare that publication of this paper creates no conflict of interest. The authors thank the NT Department of Education, Training and Youth Affairs and the NT Department of Health and Community Services. Special thanks to Maymuna Yunupingu, Lazarus Mamarika, Joaz Wurramarrba, Donita Mamarika, Gilbert Marawili, Lennard Amagula, Muriel Jaragba, Dennis Wukun Wanambi. Also thanks to Kate Conigrave, University of Sydney, who reviewed draft versions of this paper.