
Abstract
One of the more persistent health anomalies within New Zealand involves inter-ethnic differences in rates of tobacco consumption [1]. Although a decline in the national prevalence rate of smoking was observed between the 1980s and 1990s, analyses examining smoking by ethnic subpopulations suggest that during this period relative smoking prevalence rates for Māori increased [2–5]. In 2006 it was estimated that the smoking prevalence rate for adult New Zealanders was 23.5%, but among Māori the prevalence rate for smoking was 45%. Given the incontrovertible evidence that smoking is a significant downstream risk factor for serious health conditions such as chronic cardiovascular disease, respiratory diseases, lung and other cancers, each of which can lead to premature disability or death [6,7], these figures are of immediate as well as future concern.
Several epidemiological studies have indicated the presence of disparate smoking patterns between ethnic groups in New Zealand [3,4,8]. One focus of this research has involved elucidating the risk factors that might contribute to the elevated rates of smoking by Māori. A range of genetic, behavioural and environmental factors have been examined in these studies. For example, Lea et al. found evidence that Māori people had slower rates of nicotine metabolism than European New Zealander people, due to an increased frequency of a particular gene variant related to nicotine metabolism [9]. McLeod et al. reported that Māori ethnicity was one of the strongest predictors of smoking during the first trimester of pregnancy [10], while Scragg and Laugesen found that Māori adolescents were at greater risk of daily smoking by age 15 than were adolescents of any other ethnicity [11]. Also, Thomson et al., in a review of the literature, found evidence that Māori people had risks of being exposed to second-hand smoke that were twice those of non-Māori people [12]. In addition, a number of studies have suggested that the relative socioeconomic positioning of Māori people may be related to increased risk of smoking, nicotine dependence, and smoking-related morbidity and mortality [5,8,13].
The socioeconomic perspective is one of the key explanations in the understanding of differential rates of smoking and nicotine dependence [14]. A number of studies have shown that rates of smoking and nicotine dependence are greater among members of socially disadvantaged groups [15–17]. It has been well documented that Māori are at greater risk of socioeconomic disadvantage when compared with other New Zealanders classified by ethnicity [18–20]. This fact in turn raises the possibility that it is the relative economic disadvantage of Māori people that leads to them being more likely to smoke, more likely to meet criteria for nicotine dependence, and less likely to quit. The socioeconomic explanation also implies that Māori people are no more likely to smoke tobacco than non-Māori people experiencing similar social and economic circumstances.
A second, somewhat related perspective involves a systemic theory of colonization and relates to Māori cultural identity. From this perspective, historical and structural processes originating from the colonial settlement of New Zealand have resulted in contemporary health disparities where Māori people are overrepresented [21–25]. Such processes include the introduction of tobacco to Māori people along with the imposing of Eurocentric beliefs, values, and practices upon Māori people, which it is contended led to the social and political fragmentation of Māori society. As a corollary, it is claimed that Māori people have experienced cultural disconnection and social defeat, the results of which are observable in the higher rates of nicotine dependence, tobacco-attributed illness and mortality among Māori people today [22]. Therefore, this position proposes that the disproportionate rate of tobacco consumption by Māori people is directly linked to loss of attachment to cultural domains and a thwarted cultural identity.
Against this background, this paper uses data gathered over the course of a 25 year longitudinal study to examine the extent to which ethnic differences in nicotine dependence can be explained by socioeconomic differences. The study also examined the role of variations in cultural identity in relation to differences in nicotine dependence. More generally, the aims of the paper were to explore the origins of the higher rate of tobacco use and nicotine dependence by Māori people.
Methods
The data were gathered during the course of the Christchurch Health and Development Study (CHDS). In that study a birth cohort of 1265 children (635 boys, 630 girls) born in the Christchurch (New Zealand) urban region in mid-1977 was studied at birth, 4 months, 1 year and annually to age 16 years, and again at ages 18, 21, 25, and 30 years. Information from a variety of sources has been used including parental interviews; teacher reports; self-reports; psychometric assessments; medical and other record data [26,27]. The present analyses were based on those individuals for whom data were available on ethnic identity at birth and age 21 years, and nicotine dependence at ages 18, 21, 25, and 30. Sample sizes ranged from 987 to 1025 (78–81% of the original cohort).
Ethnic identity
The present study used two measures of ethnic identity, and one measure of cultural identity. These measures were as follows.
(1) At the time of birth, mothers of cohort members were asked a series of questions pertaining to the ancestry, ethnic identification and family history of the cohort member. As part of this questioning, mothers were asked to indicate whether the child was of New Zealand Māori ethnicity. Those cohort members whose mothers reported having Māori ancestry or Māori ethnic identification were classified as being of Māori ethnicity at birth (11.2% of the sample).
(2) At age 21 years respondents were asked about their ancestry, cultural identification, level of participation in Māori cultural domains, and proficiency in the Māori language [28]. On the basis of this questioning, 11.1% of sample members self-identified as New Zealand Māori ethnicity. Of these individuals, 81.6% had also been classified as being of Māori ethnicity at birth.
(3) In addition, self-reports of ethnicity at age 21 were used to further classify participants on a measure of cultural identity [28], using measures suggested by Pomare et al. [29], in order to examine the extent to which self-reported cultural identification, as defined by the individual's report of the extent to which s(he) identifies as Māori, may be related to nicotine dependence. Classification of participants according to cultural identity showed that, among those reporting Māori ethnicity at age 21, 45.9% reported sole Māori identity, and 54.1% reported Māori ethnic identity and identity with another ethnic group. Comparisons of the sole Māori and Māori/other group, undertaken to demonstrate the validity of the classification, showed consistent statistically significant differences (p < 0.05) between the groups in terms of participation in Māori culture. For the purposes of the present analyses, those reporting sole Māori identity were classified as having a sole Māori identity, while those reporting both Māori identity and another ethnic identity were classified as having Māori/other ethnic identity. All other participants were classified as being non-Māori.
Nicotine dependence, ages 18, 21, 25, and 30
At each assessment at ages 18, 21, 25, and 30 years, participants were questioned as to the frequency with which they had smoked cigarettes during the month prior to the assessment, using a 6 point scale ranging from non-smoker to smoking 21+ cigarettes per day. In addition, those participants who reported smoking during the previous month were questioned as to their experience with a number of symptoms of nicotine dependence during that year. These measures of nicotine dependence at ages 18, 21, 25, and 30 years were obtained using custom-written questions based on the generic DSM-IV criteria for nicotine dependence [30]. Participants were classified as being nicotine dependent at each age if they met the DSM-IV criteria for nicotine dependence at that age.
Socioeconomic background covariate factors
The socioeconomic background of cohort members was assessed using several indicator measures chosen from the database of the study. These included the following.
Maternal and paternal education (at birth)
The education level of the natural mother and father of each participant was assessed at the time of the survey participant's birth using a 3 point scale that reflected the highest level of educational achievement attained.
Family living standards (0–10 years)
At each year an assessment of the material living standards of the family was obtained via interviewer rating on a 5 point scale that ranged from ‘very good’ to ‘very poor’. These were averaged over the 10 year period to give a measure of family living standards during this period.
Family socioeconomic status (at birth, and at age 14)
This was assessed at the time of the survey participant's birth, and again when the participant was aged 14 years, using the Elley–Irving scale of socioeconomic status for New Zealand [31]. This scale classifies socioeconomic status into six levels on the basis of paternal occupation ranging from 1 = professional occupations to 6 = unskilled occupations.
Missing data
As noted previously, the analyses were based on 987–1025 sample members, depending upon the number of cohort members interviewed at each assessment. To assess the possible effects of sample selection bias, tests were conducted to examine the extent to which the obtained samples were representative of the original cohort of 1265 participants enrolled in the study. This analysis showed that there were slight but statistically significant (p < 0.05) tendencies for the obtained sample to underrepresent individuals from more socially disadvantaged backgrounds (low parental education, low socioeconomic status, single-parent family). To take these biases into account, the sample was post-stratified into a series of groups on the basis of these characteristics, and the probability of study participation estimated for each group using the methods described by Carlin et al. [32]. All analyses were then repeated with the data for the analysis samples weighted by the inverse of the probability of study participation. In addition, there were small amounts of missing data for some covariate factors. To examine the implications of missing values, regression imputation of missing data was conducted and the analyses repeated with the missing values on each covariate replaced by the imputed values. In all cases, these reanalyses produced essentially the same pattern of results to those reported here, suggesting that the conclusions of the present study were unlikely to have been influenced by missing data and selection bias.
Results
Associations between ethnic identity and nicotine dependence at age 25
Table 1 shows the cohort divided into Māori and non-Māori groups based on ethnicity reported at birth. For each group Table 1 reports on the percentage of cohort members meeting DSM criteria for nicotine dependence at ages 18, 21, 25 and 30 years. The comparison at each assessment is tested for statistical significance using the χ2 test of independence. Table 1 shows that, at each assessment, those who were classified as having Māori ethnicity at birth had rates of nicotine dependence that were significantly higher (p < 0.05) than rates for non-Māori people. Rates of nicotine dependence among non-Māori people ranged from 12.8% to 23.5%, whereas rates of nicotine dependence among Māori people ranged from 22.6% to 39.8%.
Associations between ethnicity (at birth) and nicotine dependence ages 18–30
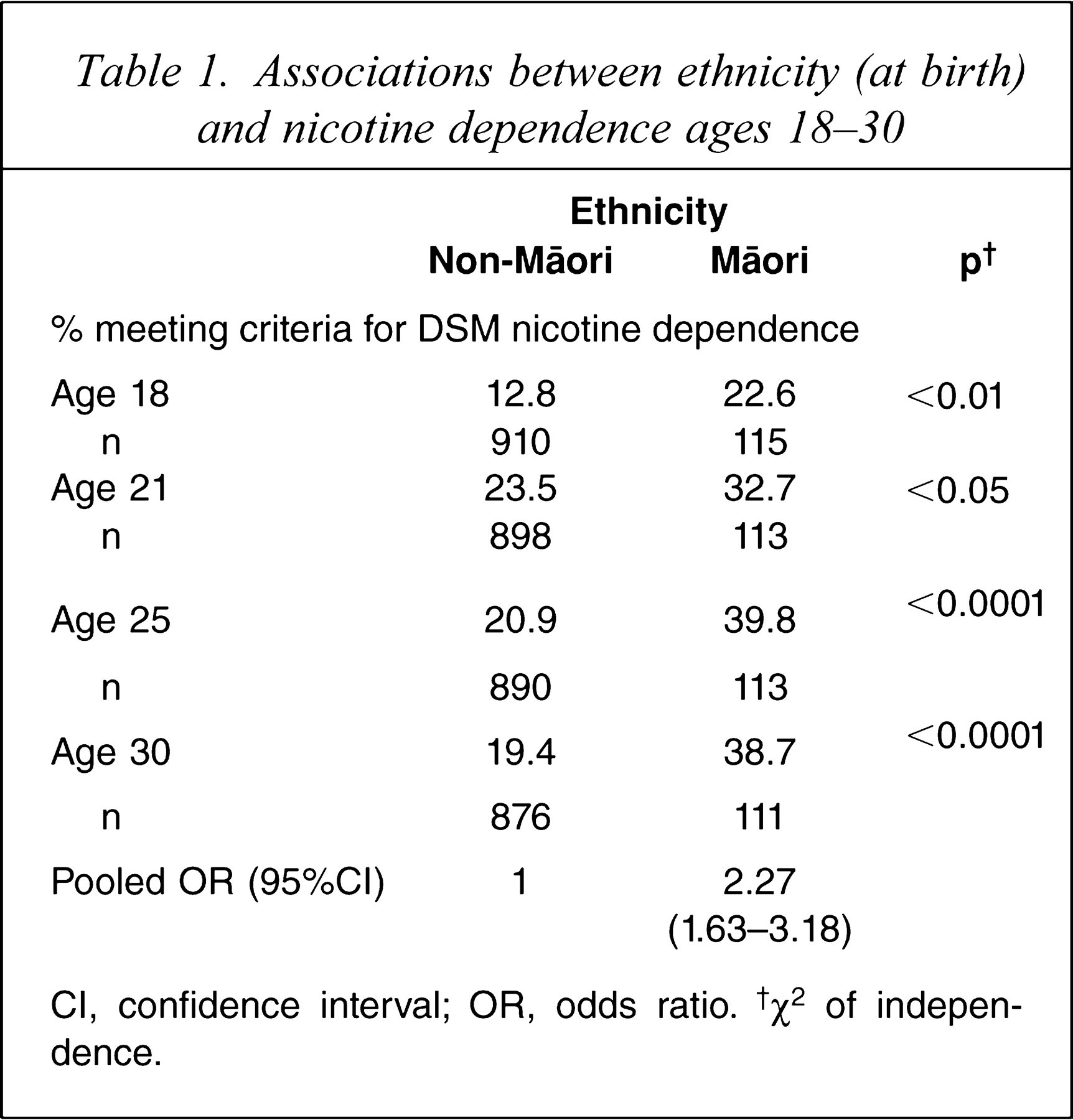
CI, confidence interval; OR, odds ratio. †χ2 of independence.
The associations between the repeated outcome measures of nicotine dependence and ethnicity were modelled using generalized estimating equation (GEE) methods [33,34] with logistic regression. The GEE approach pools the repeated measures of each outcome at each time period to produce an estimate of the population-averaged effect of the predictors on each outcome, and provides estimates of the pooled odds ratio (OR). Table 1 also reports the OR, which provides an approximate measure of the risks of a given outcome among Māori people when compared to the risk for non-Māori people, pooled over the period 18–30 years. This analysis showed that, over the period 18–30 years, Māori people had odds of nicotine dependence that were approximately 2.27-fold greater than those of non-Māori people.
Tests of socioeconomic explanations
To examine the extent to which ethnic differences in nicotine dependence could be explained by socioeconomic factors, the associations between ethnic identity at birth and nicotine dependence at ages 18, 21, 25 and 30 were adjusted for socioeconomic factors. The logistic regression model presented in Table 1 was extended to include measures of socioeconomic status including maternal and paternal education, socioeconomic status at birth and at age 14, and average family living standards to age 10.
The results of this analysis are shown in Table 2, which lists both the unadjusted and adjusted OR and 95% confidence interval (CI) for the associations between ethnic identification and nicotine dependence at ages 18–30. Table 2 shows that adjustment for socioeconomic factors reduced the associations between ethnicity and nicotine dependence to statistical non-significance, although there remained some suggestion of a small but non-significant association between ethnicity and nicotine dependence (OR = 1.39, 95%CI = 0.93–2.08). Statistically significant (p < 0.05) covariate factors included average family living standards ages 0–10; and family socioeconomic status at age 14. Estimates of the population-attributable risk suggested that, after adjustment, Māori ethnicity accounted for only 3.1% of the risk of nicotine dependence among the cohort.
Pooled OR for the associations between ethnicity and nicotine dependence ages 18–30 vs adjustment for childhood socioeconomic status factors
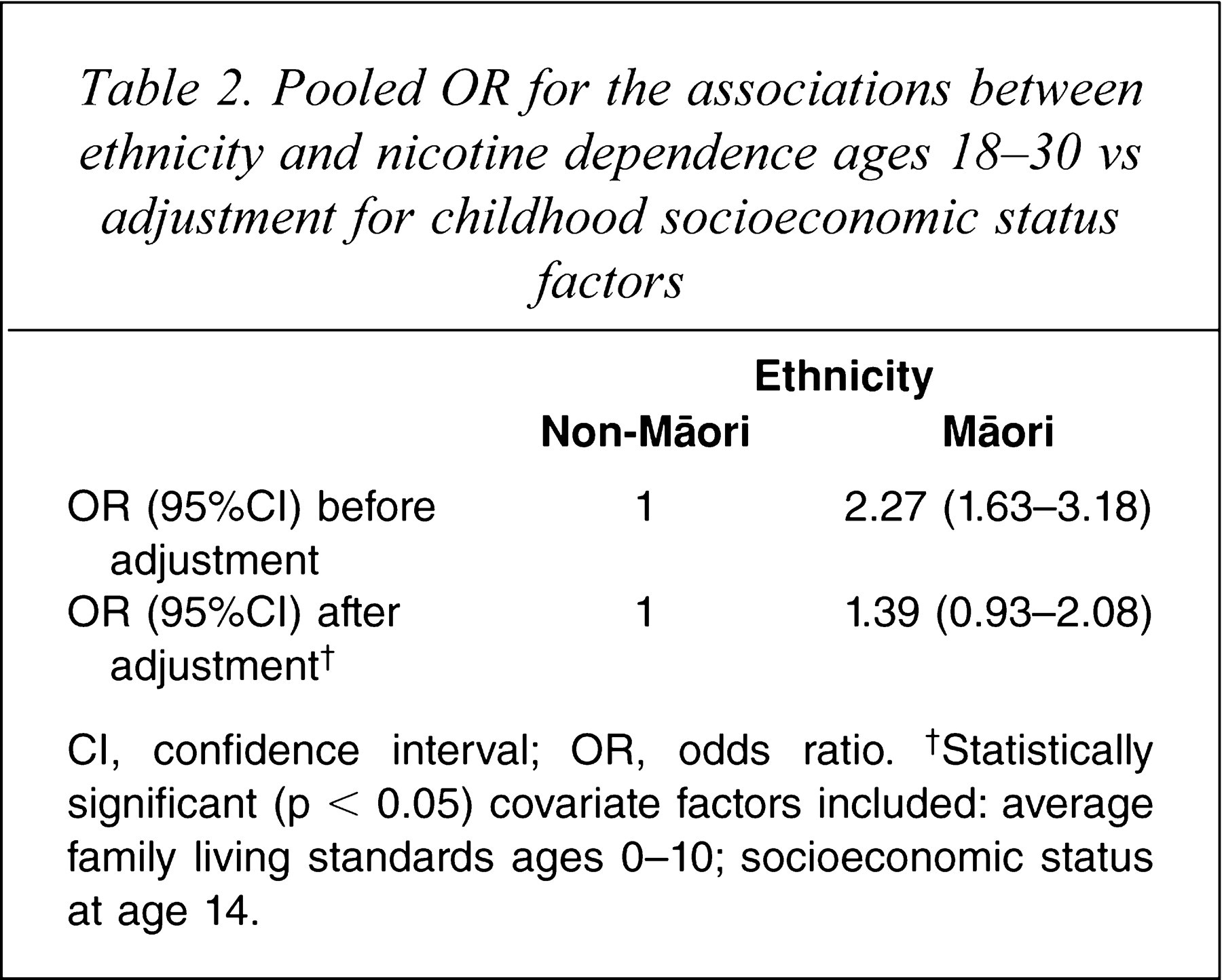
CI, confidence interval; OR, odds ratio. †Statistically significant (p < 0.05) covariate factors included: average family living standards ages 0–10; socioeconomic status at age 14.
The implication of the findings in Table 2 is that the associations between ethnicity and nicotine dependence shown in Table 1 were largely, if not wholly, explained by the greater exposure of young Māori people to socioeconomic disadvantage. After adjustment for these factors, there was little evidence to suggest that being of Māori ethnicity per se was a risk factor for nicotine dependence in adulthood.
Supplementary analyses
Ethnicity at age 21
In order to examine the robustness of the analyses to alternative methods of classification of ethnicity, the aforedescribed analyses were repeated using a measure of ethnicity (Māori; non-Māori) obtained when the participants were aged 21 years in place of the measure of ethnicity reported at birth. Estimates of the pooled OR for the association between ethnicity at age 21 and nicotine dependence at ages 18–30 showed that Māori people were at significantly increased risk of nicotine dependence as compared with non-Māori people (OR = 1.69, 95%CI = 1.19–2.40, p < 0.01). Adjustment for socioeconomic factors reduced the association to statistical non-significance (OR = 0.99, 95%CI = 0.64–1.53, p > 0.90). The results of this analysis suggested that, irrespective of the age at which ethnicity was measured, the associations between ethnicity and nicotine dependence were explained by the greater exposure of young Māori people to socioeconomic disadvantage.
Cultural identity at age 21
A further analysis examined the extent to which differences in Māori cultural identity, measured at age 21, were associated with nicotine dependence during the period 18–30 years. In this analysis the measure of cultural identity, operationalized as a pair of design variates, was used in place of the measure of ethnicity at age 21. Tests of the unadjusted associations showed that cohort members of sole Māori identity were significantly more likely (p < 0.05) than either those of Māori/other identity, or non-Māori people, to meet criteria for nicotine dependence during the period 18–30 years (sole Māori OR = 2.44, 95%CI = 1.52–3.94; Māori/other identity OR = 1.20, 95%CI = 0.73–1.97). Adjustment for family socioeconomic background in childhood, however, reduced these associations to statistical non-significance (sole Māori OR = 1.34, 95%CI = 0.75–2.42; Māori/other identity OR = 0.75, 95%CI = 0.42–1.37). The results of this analysis suggested that the associations between cultural identity and nicotine dependence were explained by the greater exposure of young Māori people to socioeconomic disadvantage.
Tests of gender differences
In order to examine whether there were gender differences in the links between ethnic identity, nicotine dependence, and socioeconomic factors, the GEE models presented in Tables 1,2 were modified to fit regression terms nested within gender for the measures of ethnic identity and each socioeconomic factor [35]. Then, Wald χ2 tests of gender equality for ethnic identity and socioeconomic factors were performed for each predictor. The results of these analyses suggested that there were no statistically significant gender differences for the measures of ethnic identity and each of the socioeconomic factors (all p > 0.05), suggesting that the associations between ethnic identity and nicotine dependence, after controlling for socioeconomic factors, did not differ according to gender.
Discussion
The present study has used data gathered over the course of a 25 year longitudinal study to examine the linkages between ethnicity and cigarette smoking in a New Zealand birth cohort. This study leads to two major conclusions.
First, in agreement with previous research, there were consistent trends for cohort members reporting a Māori identity to have higher rates of nicotine dependence from ages 18 to 25 [1–5,8,36,37]. On average, Māori people had risks of nicotine dependence that were 2.27-fold greater than those of non-Māori people.
Second, the results of regression analyses suggested that the linkages between ethnicity and nicotine dependence were largely explained by the linkages between ethnicity and socioeconomic disadvantage. Statistical adjustment for socioeconomic factors including paternal education level, socioeconomic status at birth and during adolescence, and average family living standards to age 10, for the most part explained the associations between ethnicity and nicotine dependence in young adulthood. Estimates of the population-attributable risk suggested that, after adjustment, Māori ethnicity accounted for only 3.1% of the risk of nicotine dependence among the cohort. The net effect of relative socioeconomic disadvantage was to place young Māori people at greater risk of nicotine dependence from early adulthood to age 30. These results were consistent irrespective of whether Māori identity was assessed at birth, or at age 21.
Third, the results suggested that although those reporting a sole Māori cultural identity at age 21 had higher risks of nicotine dependence than either those reporting a Māori/other cultural identity, or non-Māori, adjustment for socioeconomic factors also explained the associations between cultural identity and risks of nicotine dependence. These results lead to the conclusion that among Māori people in the present cohort, variations in cultural identity did not influence patterns of nicotine dependence, once the confounding influence of socioeconomic status was taken into account. Finally, tests of gender differences in the associations between ethnic identity and nicotine dependence, after controlling for socioeconomic factors, produced no evidence that the links between ethnicity and nicotine dependence varied according to gender.
These findings clearly suggest that the factors influencing the higher rate of cigarette smoking among Māori people are socioeconomic rather than cultural in origin. The risk factors and life processes that led young Māori people to cigarette smoking appear to be the same as those leading non-Māori people to engage in the same behaviour. These findings in turn raise complex questions as to the nature of the associations between socioeconomic status in childhood and smoking in adulthood. In an earlier study of the present cohort, Fergusson et al. found that exposure to adverse socioeconomic factors in childhood predicted smoking in adolescence and young adulthood, and that these linkages were mediated via cognitive/educational factors, adolescent behaviour, and parental and peer smoking [14].
These results also provide empirical support to the social deprivation model described here to account for ethnic differences in substance use between Māori and other New Zealand people. The major implication of this finding is that improvements in the economic welfare of Māori people may provide the most promising avenue to improve later smoking-related outcomes for them [38]. It should be noted, however, that based on the evidence provided, such initiatives are likely to be of equal benefit to non-Māori people experiencing similar problems with cigarette smoking and who are also raised in environments characterized by economic disadvantage.
The present findings may also have implications for other research examining the links between ethnicity and smoking in New Zealand. For example, it could be argued that socioeconomic status may serve as a mediating factor between genetic factors that influence nicotine metabolism and later smoking and nicotine dependence [9]. Also, it may be possible that higher rates of socioeconomic adversity among Māori people may be related to lower rates of quitting smoking among pregnant women [10], and to higher risks of exposure to secondhand smoke [12]. Further research is needed to examine more closely the links between socioeconomic adversity and other factors that may play a role in increasing the risk of smoking and nicotine dependence among Māori people.
The present findings are subject to a number of caveats. In particular, the study findings are based on a single cohort born in a specific geographic region and studied over a specific time period. The extent to which the study findings generalize to other cohorts, times and regions is not known. In addition, although analyses suggested that this was not the case, it could be argued that sample attrition may have affected the present results. Finally, although the study has linked exposure to socioeconomic adversity to higher rates of nicotine dependence among Māori people, further research is needed to elucidate the pathways by which young Māori people are more likely to begin smoking. In addition, research is needed that can identify the environmental and behavioural factors that may be linked to both socioeconomic adversity and higher rates of smoking and nicotine dependence among Māori people.
Within the limitations of the study the research suggests two major conclusions about ethnic disparities in the use of tobacco. First, Māori ethnic identification is associated with increased risks of cigarette smoking and nicotine dependence. Second, the higher rate of smoking by Māori people can be attributed to socioeconomic factors known to influence risk of cigarette smoking.
Footnotes
Acknowledgements
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.