
Abstract
Objective:
The present study examined the extent to which childhood socio-economic status (SES) could account for differences in adult psychosocial outcomes between Māori and non-Māori individuals in a birth cohort of more than 1000 individuals studied to age 30.
Methods:
Data were gathered on three measures of childhood SES (family SES, family living standards, family income) and adult psychosocial outcomes including mental health, substance use, criminal offending, and education/welfare dependence outcomes, as part of a longitudinal study of a New Zealand birth cohort (the Christchurch Health and Development Study).
Results:
Those reporting Māori ethnicity had significantly (p < 0.0001) poorer scores on the three measures of childhood SES, with estimates of Cohen’s d indicating a moderate effect size. Māori cohort members also had significantly (p < 0.05) greater rates of adverse psychosocial outcomes in adulthood. Controlling for childhood SES reduced the magnitude of the ethnic differences in psychosocial outcomes, but did not fully explain the differences between Māori and non-Māori. Adjustment for childhood SES had the strongest effect on education/welfare dependence, but weaker effects on mental health, substance use, and criminal offending.
Conclusions:
Improvements in SES among Māori in New Zealand may, to some extent, ameliorate the long standing disparities in psychosocial well-being between Māori and non-Māori. However, efforts to improve Māori well-being will require an approach that moves beyond a sole focus on rectifying socio-economic disadvantage.
Keywords
Introduction
The objective of successfully eliminating health and other inequalities in liberal nation states has become a distinguishing mark of many advanced industrial democracies (Marmot et al., 2010). Often embedded within this objective is the premise that for egalitarian aspirations of the future to be met, population-level differences or ‘gaps’ of the present must be closed (Commission on Social Determinants of Health (CSDH), 2008). In high-income societies, such as the USA, UK, Canada, Australia, and New Zealand, much attention has been directed towards identifying the existence of disparities in health and psychosocial outcomes (Beckfield and Krieger, 2009; Cooke et al., 2007). More recently, research has moved beyond simply documenting the existence of health inequities to trying to discover the mechanisms that cause or contribute to them so that they may be identified and potentially eliminated (Smedley et al., 2003). With this objective in mind, research has focused on understanding the role socio-economic status (SES) plays in relation to the emergence, maintenance, and persistence of disparities in health-related and psychosocial outcomes (Adler et al., 1994; Schreier and Chen, 2013).
A distillation of the main findings concerning SES suggests that it is best understood as being a dynamic or multidimensional construct (Chen and Paterson, 2006); that it can have an acute impact on health (Christie and Barling, 2009); that there are multiple pathways by which SES can exert an influence on behaviour (Adler, 2009); and that it has an entwined association with the social environment leading to what Adler and colleagues (1994) describe as the ‘challenge of the gradient’ and what Marmot (2006) has labelled ‘the status syndrome’. These latter terms convey the significant point that SES does not just impact those who are impoverished. SES has been shown to have a monotonic influence on health outcomes by which the higher up the social hierarchy one is, the better their health (Chen et al., 2002). In order to improve our understanding of population-level disparities, attention has also been directed towards the complex interplay between SES and ethnicity (Seeman et al., 2008).
One of the major domestic dilemmas that New Zealand continues to confront is ethnic disparities within its borders (Gracey and King, 2009; King et al., 2009). Māori, who are recognised as the indigenous ethnic minority of New Zealand and who constitute around 15% of the nation’s population, continue to have poorer outcomes in comparison to their New Zealand counterparts (Bramley et al., 2005). Across numerous indicators, including health (Mason et al., 2012), education (Strategy and System Performance and Ministry of Education, 2008), economic status (Chapple, 2000; Statistics New Zealand, 2007), and criminal justice (Ministry of Justice, 2009; Marie, 2010), Māori are more likely to be disproportionately over-represented in the negative indices when compared to other New Zealanders. Relative to morbidity and mortality data, ethnic surveillance studies indicate that from prenatal development, through infancy and adolescence, and onwards to adulthood and old age, a pattern of diminished health status for Māori not only exists, but persists across the lifespan (Ministry of Health and Statistics New Zealand, 2009; Mason et al., 2012). Of considerable concern is that the factors responsible for this pattern may contribute to an intergenerational cycle of disadvantage.
However, while researchers and policymakers may be motivated to address these unequal patterns and the burden that arises from them, quite often what is missing is a coherent baseline of information that not only provides a platform, but also an insight into the complexity and interplay of factors that could lead, or contribute, to these disparities (James, 2009; Kowal, 2008). Against this background, we examined the explanatory worth of childhood SES factors to account for ethnic disparities in psychosocial outcomes. More specifically, we compared the extent to which exposure to adverse socio-economic circumstances in childhood contributes to the well-documented associations between Māori ethnicity and adverse psychosocial outcomes in adulthood, including mental health disorders, substance use disorders, criminal offending, and education/welfare dependence outcomes.
Methods
Participants
The data were gathered during the course of the Christchurch Health and Development Study (CHDS). In this study, a birth cohort of 1265 children (635 males, 630 females) born in the Christchurch (New Zealand) urban region in mid-1977 has been studied at birth, 4 months, 1 year, and annually to age 16 years, and again at ages 18, 21, 25, and 30 years (Fergusson and Horwood 2001; Fergusson et al., 1989). All study information was collected on the basis of signed and informed consent from the study participants.
Ethnicity
At age 21 years, respondents were asked about their ancestry, ethnic and cultural identification, level of participation in Māori cultural domains, and proficiency in the Māori language (Broughton et al., 2000). As part of this questioning, participants were asked to indicate which ethnic groups they ‘belonged to’ or ‘identified with’. For the purposes of the present investigation, all participants who chose ‘New Zealand Māori’ as a response option, whether alone or in combination with one or more other options, were classified as Māori (11.1% of the sample).
Adult psychosocial outcome measures
Mental health (ages 18–30)
Major depression
At ages 21, 25, and 30 years, participants were questioned regarding symptoms of major depression using Composite International Diagnostic Interview (CIDI; World Health Organization, 1993) items and criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV; American Psychiatric Association, 1994). Sample members who met the DSM-IV diagnostic criteria for a major depressive episode at any time during any assessment period were classified using a dichotomous measure as having major depression during the period 18–30 years.
Suicidal ideation
Suicidal behaviour during the period 18–30 years was assessed via self-report at ages 21, 25, and 30 by asking sample members whether they had ever thought about killing themselves or had attempted suicide during each assessment period. Participants were classified using a dichotomous measure as having suicidal ideation during the period 18–30 years if they had reported at least one instance of thinking about killing themselves at any assessment.
Antisocial personality disorder
At ages 21, 25, and 30, antisocial personality disorder was assessed using custom-written survey items reflecting the DSM-IV criteria for antisocial personality disorder. These items were considered to have face validity due to their derivation from the DSM-IV behavioural descriptors. Sample members who met the diagnostic criteria for antisocial personality disorder during one or more assessment periods were classified as having the disorder during the period 18–30 years.
Substance use outcomes (ages 18–30 years)
Alcohol use disorder
Alcohol use disorders were assessed at ages 21, 25, and 30 by items from the CIDI to assess DSM-IV symptom criteria for alcohol abuse or alcohol dependence. Individuals who met the relevant DSM-IV diagnostic criteria for alcohol abuse or dependence in any assessment period were classified as having an alcohol use disorder during the period 18–30 years.
Cannabis dependence
Cannabis dependence was assessed at ages 21, 25, and 30 by items from the CIDI to assess DSM-IV symptom criteria for cannabis dependence. Individuals who met the relevant DSM-IV diagnostic criteria for cannabis dependence in any assessment period were classified as being cannabis dependent during the period 18–30 years.
Nicotine dependence
Nicotine dependence was assessed at ages 21, 25, and 30 by custom-written survey items designed to assess the DSM-IV symptom criteria for nicotine dependence. Sample members who, at any assessment, reported smoking 10 or more cigarettes per day and who also reported three or more of the relevant DSM-IV symptom criteria were classified as nicotine dependent during the period 18–30 years.
Criminal offending outcomes
Violent offending and property offending (ages 20–21, 24–25, and 29–30 years)
At ages 21, 25, and 30, respondents were questioned about their criminal behaviours during the previous 12 months using the Self-Report Delinquency Inventory (Elliott and Huizinga, 1989) supplemented by additional custom-written survey items. For the purposes of the present study this information was used to classify cohort members on two dichotomous measures: first, a measure of self-reported violent offending for each 12-month period prior to the assessments at ages 21, 25, and 30 years; and second, a measure of self-reported property offending for each 12-month period prior to the assessments at ages 21, 25, and 30 years. Violent offences included assault, fighting, use of a weapon, or threats of violence against a person. Property offences included theft, burglary, breaking and entering, vandalism, arson, and related offences.
Arrest/conviction (ages 18–21, 21–25, and 25–30 years)
At ages 21, 25, and 30, cohort members were asked whether they had been arrested for any reason during each year since the previous assessment, and, if so, they were asked to provide details of the circumstances leading to the arrest and the consequences of the arrest, including court convictions. Those cohort members who reported having been arrested or convicted during an assessment period (18–21, 21–25, and 25–30 years) were classified using a dichotomous measure as having been arrested/convicted during that assessment period.
Education/welfare dependence outcomes
Leaving school without qualifications (by age 18)
At age 18, participants were assessed on their educational achievement to date. Those participants who reported attaining no formal secondary educational qualifications (a minimum of one grade above C on School Certificate examinations) were classified as having left school without qualifications by age 18.
Attained university degree or equivalent (by age 30)
At each assessment at ages 21, 25, and 30, sample members were questioned as to whether they had ever attained a Bachelor’s level or higher degree from a university or equivalent tertiary institution. Those individuals who reported receiving a degree or equivalent were classified using a dichotomous measure as having attained a university degree by age 30.
Welfare dependence (ages 21–25 and 25–30 years)
Welfare benefit dependence was assessed at ages 25 and 30. At ages 25 and 30, cohort members were questioned as to their receipt of a range of potential welfare benefits during each year of the assessment period from ages 21–25, and during the assessment period from age 25–30. For the purposes of the present investigation, participants who reported receiving any benefit for at least one month during any assessment period were classified using a dichotomous measure as having been welfare dependent during the period 21–30 years.
Childhood family socio-economic factors
In order to examine the role of socio-economic factors in the links between ethnicity and outcomes in adulthood, three measures of family socio-economic conditions were chosen from the study database: family living standards, family socio-economic status, and average family income.
Family living standards (0–10 years)
At each year, a global assessment of the material living standards of the family was obtained by means of an interviewer rating, based on an assessment of the condition of the family home, the area in which the home was located, and overall impressions of relative affluence or financial difficulties. Ratings were made on a five-point scale that ranged from ‘very good’ to ‘very poor’. These ratings were summed over the 10-year period and divided by 10 to give a measure of typical family living standards during this period.
Family socio-economic status (at birth)
This was assessed at the time of the survey of the child’s birth using the Elley–Irving (Elley and Irving, 1976) Scale of SES for New Zealand. This scale classifies SES into six levels on the basis of paternal occupation ranging from 1 = professional occupations to 6 = unskilled occupations.
Average family income (ages 0–10)
At each year, estimates of the family’s gross annual income were obtained from parental report. To provide a measure of the average level of income available to each family over the period from the child’s birth to age 10 years, the income estimates for each year were first recoded into decile categories and the resulting measures then averaged over the 10-year period to produce a measure of the family’s averaged income decile rank.
Statistical analyses
The data were analysed in three stages. In the first stage of the analyses, models were fitted to estimate the bivariate associations between ethnicity and each of the three childhood family socio-economic factors using multiple regression analysis. These models were of the form:

where f(Y) was the score for each socio-economic measure and B1 represented the effect of ethnicity.
In the second step of the analyses, the associations between ethnicity and each of the adult psychosocial outcomes were also modelled using logistic regression with models described as in equation 1. The percentages for each ethnicity classification (Māori/non-Māori) were used to calculate estimates of Cohen’s d for the unadjusted associations between ethnicity and each outcome.
In the next step of the analyses, the bivariate models were extended to include the three childhood socio-economic covariate factors. These models were of the form:

where ∑BjXj was the set of covariate factors included in each model, entered simultaneously. The parameter estimates of the adjusted models were used to compute estimates of the adjusted means and adjusted percentages. In turn, the adjusted means and percentages were used to calculate estimates of Cohen’s d for the adjusted associations between ethnicity and each outcome.
Sample size and sample bias
The present analyses were based on samples ranging from 987 to 1011 participants, representing 78–80% of the original cohort of 1265 participants, for whom data were available concerning ethnicity and outcomes at the assessments at ages 21, 25, and 30. To examine the effects of sample losses on the representativeness of the sample, the obtained samples with complete data at each age were compared with the remaining sample members on a series of socio-demographic measures collected at birth. This analysis suggested that there were statistically significant (p < 0.01) tendencies for the obtained samples to under-represent individuals from socially disadvantaged backgrounds characterised by low parental education, low SES, and single parenthood. To address this issue, the data weighting methods described by Carlin et al. (1999) were used to examine the possible implications of selection effects arising from the pattern of missing data. These analyses produced essentially the same pattern of results to those reported here, suggesting that the conclusions of this study were unlikely to have been influenced by selection bias.
Results
Associations between ethnicity and socio-economic factors in childhood
Table 1 shows the cohort classified according to ethnicity as indicated at age 21 (see Methods section). For each group, means and standard deviations for each of three measures of child socio-economic conditions (family SES at birth, family living standards at ages 0–10, and family income rank at ages 0–10) are provided, along with estimates of Cohen’s d for the effect size of the difference between non-Māori and Māori cohort members. The table shows that:
Cohort members who indicated Māori ethnicity had significantly (p < 0.0001) poorer scores for each of the three childhood socio-economic indicators. Māori cohort members were significantly more likely to have been raised in families with lower SES, lower average living standards, and lower average family income. The results of these analyses suggest that Māori cohort members were significantly more likely to have been exposed to socio-economic adversity in childhood than non-Māori cohort members.
Estimates of Cohen’s d ranged from 0.51 to 0.74, suggesting a moderate-sized difference on measures of childhood socio-economic factors between ethnic groups.
Mean scores and estimates of Cohen’s d for ethnic differences in measures of family socio-economic factors in childhood.
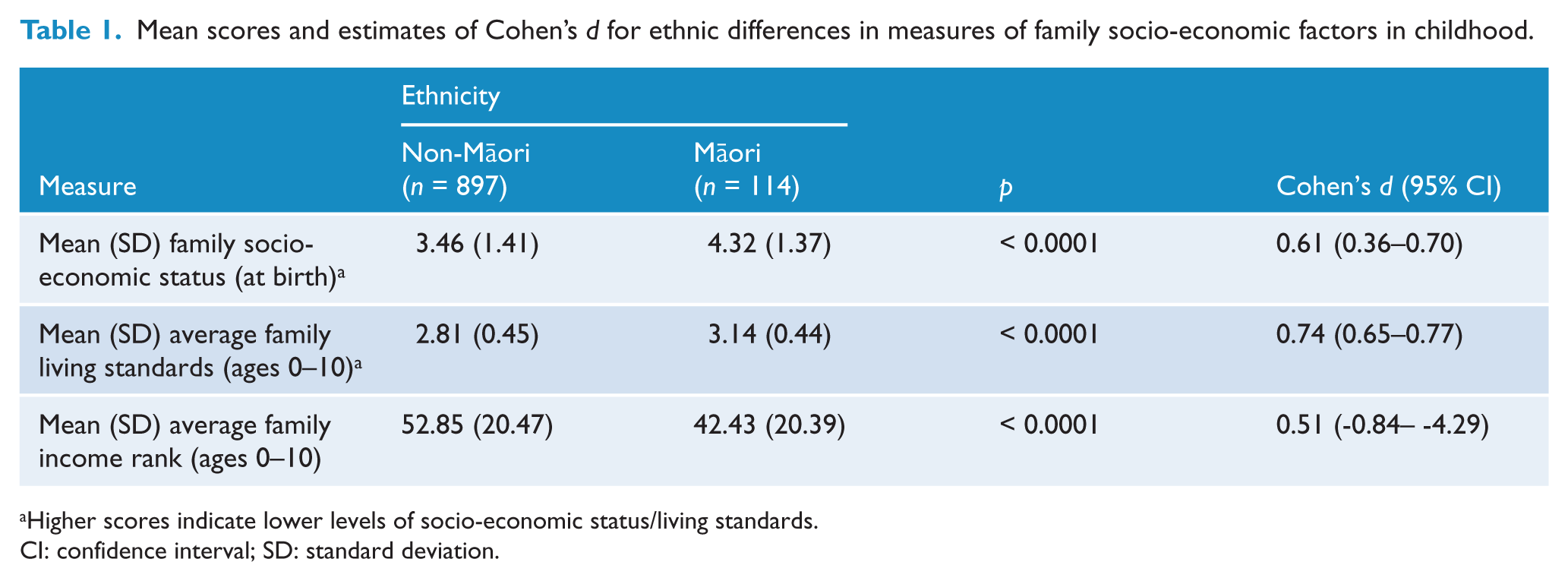
Higher scores indicate lower levels of socio-economic status/living standards.
CI: confidence interval; SD: standard deviation.
Associations between ethnicity and psychosocial outcomes (ages 18–30) before and after controlling for childhood socio-economic factors
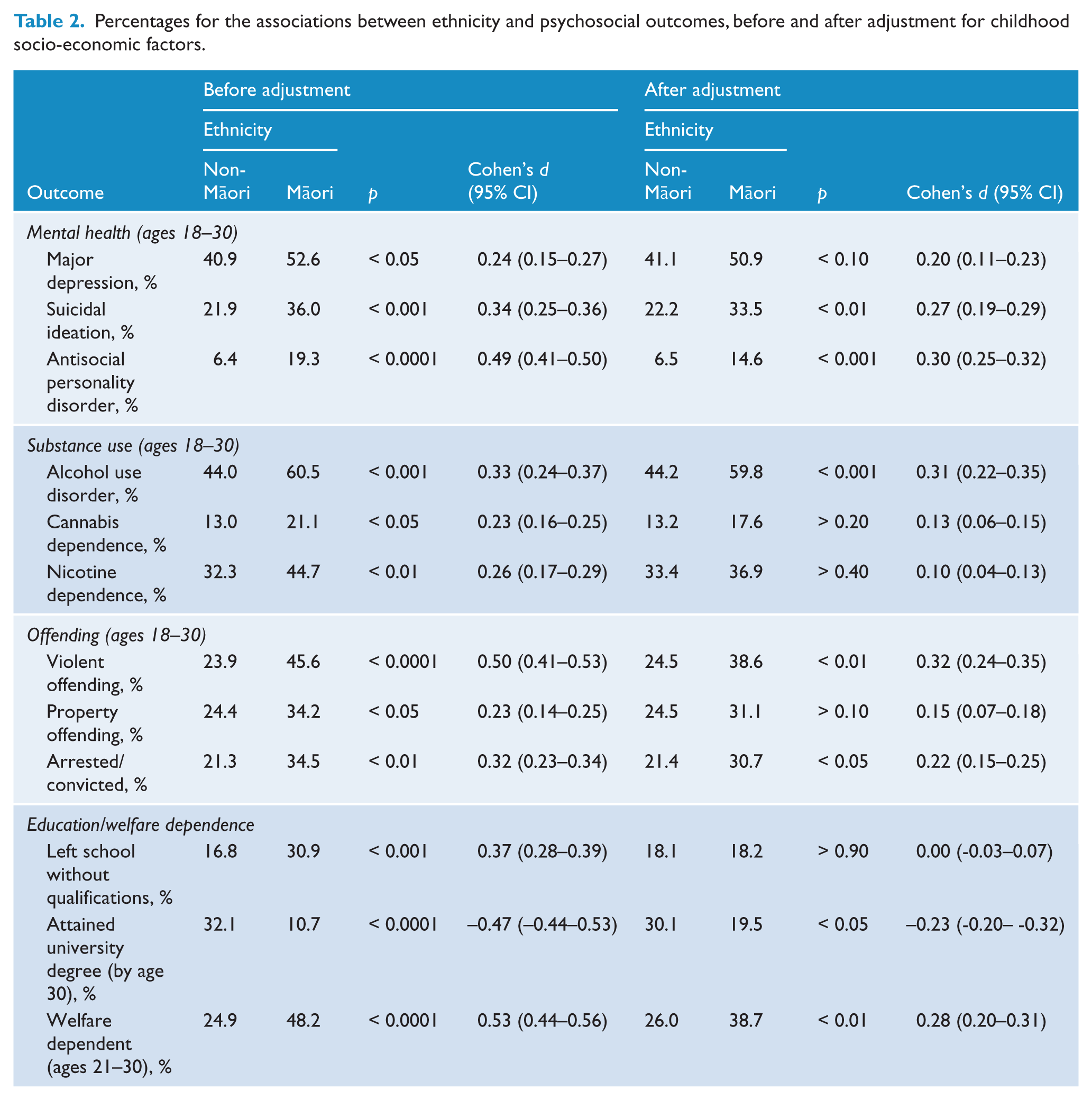
In order to examine the impact of increased exposure to socio-economic adversity on Māori cohort members, associations were modelled between ethnicity and a series of psychosocial outcomes in adulthood related to mental health, substance use, criminal offending, and educational/welfare dependence outcomes (see Methods section). In the first step, logistic regression models were fitted to estimate the bivariate associations between ethnicity and outcomes. In the second step, the models were extended to include the three childhood socio-economic indicators noted previously (family SES at birth, family living standards, and family income). After both models were fitted, estimates of Cohen’s d were obtained to ascertain the effect size for each association before and after controlling for childhood socio-economic factors. The results of these analyses are shown in Table 2, which shows the percentage of non-Māori and Māori cohort members reporting each outcome before adjustment, and the adjusted percentages after accounting for childhood socio-economic factors. The table also reports tests of significance derived from logistic regression modelling, and estimates of Cohen’s d both before and after adjustment. The table shows that:
Before adjustment, there were significant (p < 0.05) associations between each outcome and ethnicity. Māori cohort members were significantly more likely to report a range of mental health problems, substance use disorder, criminal offending, and poorer educational outcomes and welfare dependence. Absolute values for the estimates of Cohen’s d ranged from 0.23 to 0.53, with a median value of approximately 0.34, suggesting a weak to moderate effect size for the difference between ethnic groups. These differences were strongest for educational/welfare dependence outcomes (mean Cohen’s d = 0.46). Mental health, substance use, and offending had generally weaker estimates of effect size (average Cohen’s d = 0.36, 0.27, and 0.35, respectively).
Adjustment for childhood socio-economic factors generally reduced the magnitude of the associations between ethnicity and psychosocial outcomes, with a number of these associations being reduced to marginal statistical significance (p < 0.10) or statistical non-significance (p > 0.10). However, seven of the 12 outcome measures remained statistically significant after controlling for socio-economic factors, suggesting that while exposure to adverse socio-economic factors accounted for some of the ethnic differences in outcomes during adulthood, these factors did not fully explain the associations. Those outcomes that were no longer significantly (p > 0.05) associated with ethnicity after controlling for childhood socio-economic factors included major depression, cannabis dependence, nicotine dependence, offending against property, and leaving school without qualifications.
Absolute values for the estimates of Cohen’s d for the adjusted associations ranged from 0.00 to 0.32, with a median value of approximately 0.23. Comparisons between the unadjusted and adjusted estimates of Cohen’s d are shown in Figure 1. As is shown in the figure, the reduction in effect size after controlling for childhood socio-economic factors was largest for educational/welfare dependence outcomes, which had a mean effect size reduction of 0.29. The smallest reduction in effect size was for substance use, which had a mean effect size reduction of approximately 0.09. The effect size reduction for mental health outcomes and offending outcomes were also generally small (0.10 and 0.12, respectively).
Percentages for the associations between ethnicity and psychosocial outcomes, before and after adjustment for childhood socio-economic factors.
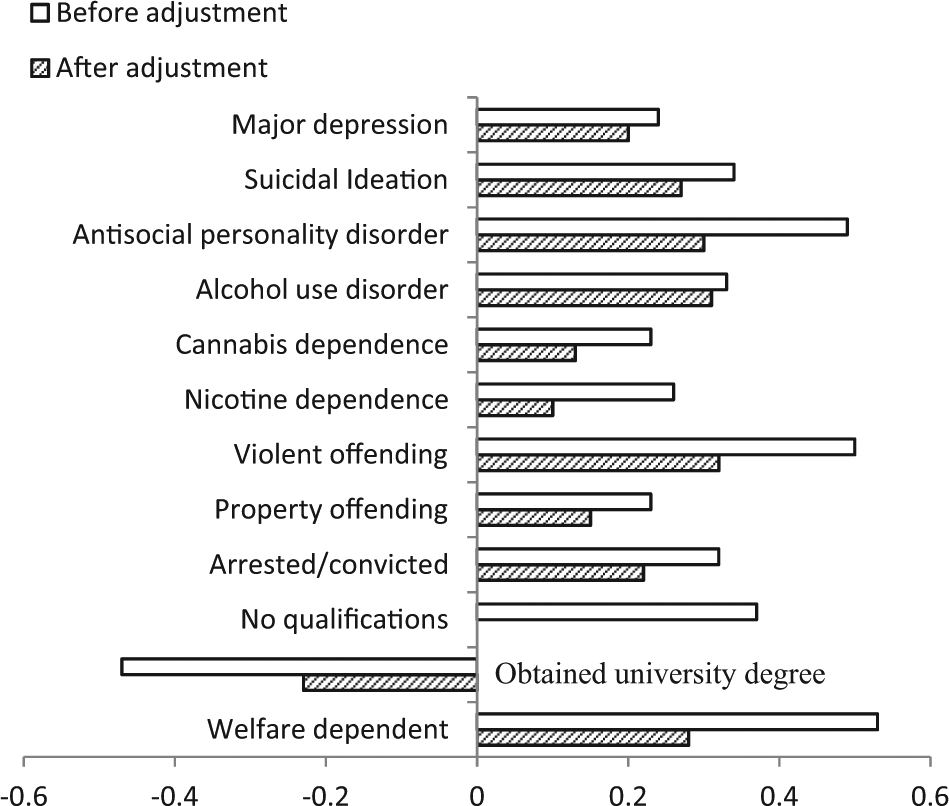
Estimates of Cohen’s d for outcomes, before and after adjustment for childhood socio-economic factors.
Discussion
A range of explanatory theories have been put forward to account for the ethnic disparities in health and psychosocial outcomes (i.e. Beckfield and Krieger, 2009; Dressler et al., 2005; Snowden and Yamada, 2005). Among these, the most dominant explanation involves SES (Adler and Stewart, 2010; Schwartz and Meyer, 2010). From this perspective, the over-representation of Māori in the negative behavioural indices is the outcome of Māori also experiencing lower SES when compared with other New Zealanders. The underlying premise of this theory is that SES confounds ethnic disparities and therefore if SES was methodologically controlled for, the magnitude of ethnic group differences would be substantially reduced or, better, disappear. The assumption of this theory is that if SES was held (or made) equal, then ethnic disparities would not exist. The present investigation used data from a 30-year study of a longitudinal birth cohort to examine this question, with the following results.
First, the present study showed a moderate sized gap between Māori and non-Māori cohort members across three measures of childhood socio-economic conditions (family SES, family living standards, and family income), reflecting the well-known risks of exposure to greater levels of socio-economic adversity faced by Māori. Controlling for these childhood socio-economic factors did reduce the magnitude of the associations between Māori ethnicity and adult psychosocial outcomes. However, the magnitude of this influence varied in direct relation to the behaviour under examination. For our cohort, controlling for childhood socio-economic factors had the strongest effect on reducing the magnitude of the associations between ethnicity and adult education and welfare dependence outcomes, with an average reduction in effect size of 0.29.
However, for the links between ethnicity and adult mental health, substance use and criminal offending, the decrease in the magnitude of association after controlling for childhood socio-economic factors was smaller, with a mean effect size reduction of approximately 0.10. These results suggest that while childhood socio-economic factors may play a small causal role in ethnic differences in adult psychosocial outcomes, they cannot completely account for the differences in adult psychosocial outcomes between Māori and non-Māori cohort members. Indeed, earlier studies examining ethnic differences in psychosocial outcomes among the CHDS cohort have shown that factors such as cultural identity and family functioning in childhood may also play key causal roles in shaping outcomes among Māori cohort members (Marie et al., 2008a; Marie et al., 2008b; Marie et al., 2009; Marie et al., 2011).
In addition, it could be speculated that childhood socio-economic factors may be indirectly linked to psychosocial outcomes via such factors as cultural identity and family functioning, or that complex inter-relationships may exist in which childhood socio-economic factors impact strongly on education and welfare dependence outcomes, which in turn may impact on longer-term mental health, substance use, and criminal behaviour outcomes. Further research is needed to address these additional possible causal pathways from childhood socio-economic factors to adult psychosocial outcomes.
Although the reasons behind the variation in the extent to which childhood socio-economic factors explained the associations between ethnicity and psychosocial outcomes were unclear, the findings were consistent with previous research on the links between exposure to adverse socio-economic circumstances in childhood and adult psychosocial outcomes. In general, previous research, including studies of the present cohort, have shown strong links between childhood socio-economic factors and educational/employment outcomes in adulthood (Fergusson et al., 2008). However, links between childhood socio-economic factors and other psychosocial outcomes, including mental health, substance use, and criminal behaviour have been observed to be generally weaker than educational and economic outcomes (Dubow et al., 2008; Gilman et al., 2002). Additional research is required to examine the direct and indirect pathways by which exposure to socio-economic adversity in childhood may influence a range of psychosocial outcomes in adulthood.
These findings suggest that improving the socio-economic positioning of Māori, therefore ‘levelling the playing field’, will help reduce ethnic disparities to some extent. However, from our analyses, it appears that improvements in the economic status of Māori will provide greater benefits in certain areas, such as education and welfare, and fewer benefits in other areas largely involving mental health, substance use, and criminal offending. Of note is the graded nature of these findings whereby improvements in childhood socio-economic factors clearly have the potential to positively impact on some behaviours, with a pattern of diminishing returns observable with respect to others. We have drawn on an ecological model of behaviour to interpret our findings, however, before doing so we first need outline two fundamental predicates underpinning our interpretation of the results.
The first predicate is that ethnicity is complex (Bradby, 2003; Kaufman and Cooper, 2001). Independent of the way it is conceptualised, it is within itself a fundamentally multi-stranded concept. It is this complexity that resists definitive characterisation. Any attempt to assign a single attribute to ethnicity or to categorise it in binary terms runs the risk of missing some of the distinctiveness of the construct. The second predicate is that ethnicity is context relevant – or contextually embedded (McLaren and Hawe, 2005). Apart from ethnicity, we are aware that there is an entire host of factors that can potentially, and often do, influence social standing. We therefore need to have a contextually embedded or an ecological understanding of ethnicity, and this understanding ought to be considered in direct relation to our state-of-the art knowledge of factors that lead to disadvantage. With these predicates in mind, along with the advantages a life course perspective provides regarding identifying factors that lead to ethnic disparities in New Zealand, we believe an ecological model provides a parsimonious framework to understand our findings.
The ecological framework suggests that human growth can only be understood within the full ecological system in which development occurs (Bronfenbrenner, 1994). In this view, the entire ecological system is comprised of five subsystems (microsystem, mesosystem, exosystem, macrosystem, chronosystem), each of which contributes a unique set of factors, which can either help or hinder healthy human development. Some of these systems (microsystem, mesosystem) are more proximal and have a direct effect on the individual, whereas others (exosystem, macrosystem, chronosystem) are more distal, exerting effects on the individual via parental/family experiences and culture. According to this framework, ethnic disparities emerge as a result of environmental risk factors not being evenly distributed across all ethnic groups.
On this account, Māori are at greater risk of being exposed to adverse environmental factors, in particular during childhood and adolescence. It is this overexposure to environmental risks, especially during the formative years, which leads to Māori featuring disproportionately in the negative behavioural indices. Targeted interventions to diminish exposure of Māori to environmental risks are therefore regarded as a feasible means to eliminate ethnic disparities in New Zealand. Our results suggest that endeavours aimed at ameliorating socio-economic disadvantage will likely show differential degrees of impact depending on the subsystem to which these efforts are directed. More specifically, interventions may have greater impact when directed at the macrosystem compared to microsystem level. For instance, the current data suggests that improving the SES of Māori children and families will likely positively influence education and welfare indices, yet have less impact on rates of mental health, substance use, and criminal offending. Behaviours more likely to involve State legislation and public monitoring, such as education and welfare, therefore appear to offer more viable intervening pathways than other less publicly observable behaviours (Beach et al., 2006; Netto et al., 2010).
It should be noted that the present study has two mainlimitations. First of these is that the data pertain to a specific cohort studied at a particular age and time frame, and the extent to which the conclusions are applicable to other populations is unclear. Second, data concerning ethnicity and outcomes were self-reported, and therefore possibly subject to biases inherent in self-report measures, which may have reduced the precision of the reported estimates of association.
Conclusion
Observed differences between populations and social groups continue to be used as a proxy to gauge the relative standing of a nation as well as its progress when compared to other nations. Reports produced by the World Health Organization and the United Nations, for example (CSDH, 2008), provide ongoing status updates identifying where disparities exist and direct attention to where improvements in the performance of specific nations are required. These reports also often serve as the conceptual precursors for more ambitious international action plans, such as those outlined by the United Nations Millennium Developmental Goals.
James (2009) has proposed that it was a move towards a human rights agenda in the mid-20th century that largely inspired the global focus on reducing disparities, the goal of which underpins much epidemiological research today. He suggested that, as an outcome of this shift, many nations developed policies and strategies specifically aimed at reducing disparities, which as a result fundamentally changed the institutional structures of many of those nations. As an outcome of this ‘global turn’ the challenges involved in accurately conceptualising and capturing the complexity of indicators related to disparities, such as economic progress and social well-being, have also been duly recognised and acknowledged (Stiglitz et al., 2009). Mindful of the limitations of the longitudinal design, we have investigated the role childhood socio-economic factors play in current ethnic disparities in psychosocial outcomes in New Zealand. Our research suggests that exposure to adverse socio-economic circumstances in childhood does lead to disadvantages. Following adjustments for childhood socio-economic factors, ethnic disparities were largely mitigated with respect to education and welfare, but were only weakly influenced relative to mental health, substance use, and criminal offending.
Footnotes
Funding
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation, and the New Zealand Lottery Grants Board.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.