
Abstract
It has been well-documented that young people of Māori ethnic status are at an increased risk of experiencing mental health problems. Ethnic trends in psychiatric morbidity data suggest that young Māori are at a heightened risk of developing anxiety, mood, and substance use disorders and are more likely to engage in suicidal ideation and suicide-related behaviours when compared with other New Zealanders [1], [2]. This pattern of Māori overrepresentation in New Zealand's mental health indices emerged in the early 1970s when the rate of Māori first admissions to psychiatric services converged with, and then surpassed, the admission rates of other New Zealanders also classified by ethnicity [3–5]. These trends have been reported in the New Zealand mental health epidemiological study (Te Rau Hinengaro), which found higher rates of mental disorder in Māori using a community-based survey [6]. As a consequence, a body of literature has arisen on the origins of Māori overrepresentation in the area of mental health problems [7–13].
The themes in this literature refer to socio-historical factors as being of specific causal relevance in understanding the disproportionate representation of Māori. Briefly described, these themes pertain to one or more of the following: historical oppression [14], [15]; institutional racism [8]; acculturation stress arising through rapid urbanization [4], [16]; unequal access to treatment services [17]; lack of ethnic matching between clinician and client leading to clinical biases [18]; and; finally, the careless collection of demographic information [19].
On the strength of these contributions, there has been a range of policy-led reforms within New Zealand to address the problem of Māori overrepresentation in mental health indices [20], [21]. These policies have been directed toward theorizing about the role of cultural identity and social adversity in relation to mental health. Two questions pertinent to this literature arise.
The first question concerns the role of ethnic identification in determining risks of mental health problems. For research and policy purposes, New Zealand's population has traditionally been demarcated as Māori and non-Māori [22]. But an accumulating body of evidence has suggested that those classified in official statistics as Māori are in fact a diverse population that varies in its identification with, and level of involvement in, Māori culture [23], [24]. Simple dichotomous Māori and non-Māori comparisons fail to reflect this diversity at a population level so recommendations for the improvement of collecting ethnicity data were widely instituted [25]. In line with this move to recognize the diversity within the Māori population, attention was directed toward developing Māori cultural identity scales [26], [27]. With regard to the overrepresentation of Māori in the mental health indices, it has been proposed that variations in Māori identity may modify the associations between ethnicity and psychosocial outcomes. Two different perspectives regarding the role of Māori identity to influence mental health status can be identified.
The dominant perspective suggests that a secure Māori identity is a protective factor that reduces risks of mental health problems [4], [28], [29]. This view leads to the prediction that rates of mental disorder should be lower among those with a sole Māori identity when compared with those having a mixed cultural identification. Other authors, however, have argued to the contrary and suggested that individuals who identify solely as Māori are more likely to experience institutional racism and other environmental insults when compared to their counterparts who identify less with Māori ancestry and culture [8], [30]. Based on the premise that the stronger that one identifies as being Māori the more likely they will be to occupy a disadvantaged position and experience discrimination, this perspective implies that those with sole Māori identity may be at greater risk of developing mental health problems.
A second question in this area concerns the extent to which associations between mental health and ethnicity are mediated by socioeconomic factors. Specifically, it may be proposed that the association between ethnicity and mental health is described by a causal chain process in which: (i) because of historical processes those of Māori ethnicity are exposed to greater social and economic disadvantage; and (ii) greater disadvantage among Māori leads to higher rates of mental health problems.
These two main issues regarding the ways in which ethnic identification and social disadvantage combine to influence ethnic differences in mental health in the New Zealand population require empirical investigation. Against this background, this paper uses data gathered over the course of the Christchurch Health and Development Study to examine the linkages between ethnic identification, socioeconomic disadvantage, and mental health in adolescence/young adulthood (18–25 years). The specific aims of the paper were twofold: (i) to examine the linkages between Māori ethnic identity and rates of mental disorders and suicidal behaviour during adolescence and young adulthood (18–25 years); and (ii) to examine the extent to which any associations between Māori ethnic identity and risks of mental disorders/suicidal behaviours were mediated by social and economic disadvantages.
Methods
The data were gathered during the course of the Christchurch Health and Development Study (CHDS). In this study a birth cohort of 1265 children (male, n = 635, female, n = 630) born in the Christchurch (New Zealand) urban region in mid-1977 has been studied at birth, 4 months, 1 year and annually to age 16 years, and again at ages 18, 21 and 25 years. Information from a variety of sources has been used including parental interviews; teacher reports; self-reports; psychometric assessments; and medical and other record data [31], [32]. The analyses were based on 984 study participants for whom information was available for ethnic identity at age 21 years (77.8% of the original sample). All study information was collected on the basis of signed and informed consent from study participants.
Ethnic identity
At age 21 years respondents were asked about their ancestry, ethnic identification, level of participation in Māori cultural domains, and proficiency in the Māori language [23]. On the basis of this questioning, 11.1% of sample members self-identified as New Zealand Māori. A further breakdown of this group showed 45.9% reporting sole Māori identity and 54.1% reporting Māori ethnic identity and identity with another ethnic group. For the purposes of the present analysis, those reporting sole Māori identity were classified as having a sole Māori identity, while those reporting both Māori identity and another ethnic identity were classified as having Māori/other ethnic identity. All other participants were classified as being non-Māori. Comparisons of the sole Māori and Māori/other group showed consistent differences between the groups in terms of participation in Māori culture, including frequency of marae visits (p < 0.001); being a member of a Māori group, organization or sports team (p < 0.05); being a member of a kapa haka (cultural performance) group (p < 0.001); attending tangi (funeral) or unveiling (p < 0.001); listening to Māori language radio programmes and watching Māori language television programmes (p < 0.001); and listening and watching programmes in the English language about Māori (p < 0.001). The descriptors of ‘sole Māori’, ‘Māori/other ethnic identity’, and ‘non-Māori’ were originally recommended by Pomare et al. in their analyses examining ethnic trends in public health epidemiology [30].
Mental health outcomes, ages 18–21 and 21–25 years
At ages 21 and 25 years cohort members were questioned about mental health issues since the previous assessment using questionnaires based on the Composite International Diagnostic Interview (CIDI) [33], supplemented by additional measures. The following measures of the young person's experience of mental health problems over the intervals 18–21 years and 21–25 years were constructed.
Major depression and anxiety disorder (ages 18–21, and 21–25 years)
These disorders were assessed using CIDI items and DSM-IV [34] diagnostic criteria for major depression and a range of anxiety disorders (including generalized anxiety disorder, panic disorder, agoraphobia, social phobia, and specific phobia).
Anti-social personality disorder (ages 18–21, and 21–25 years)
Anti-social personality disorder was assessed using custom-written survey items reflecting the DSM-IV criteria for anti-social personality disorder.
Substance dependence (ages 18–21, and 21–25 years)
This was assessed by items from the CIDI to assess DSM-IV symptom criteria for dependence upon alcohol, cannabis, or other illicit drugs. Separate questioning was conducted for each substance.
Suicidal ideation (ages 18–21, and 21–25 years)
Suicidal ideation was assessed by asking sample members whether they had ever thought about killing themselves during the assessment period and the frequency of such thoughts.
Overall number of disorders (ages 18–21, and 21–25 years)
The overall number of disorders was calculated by summing the responses for each of the five categories of mental health disorder for each participant at each assessment period, resulting in scores that ranged from 0 (reported no mental health disorders) to 5 (reported each of 5 mental health disorders).
Covariate factors
Socioeconomic background
The socioeconomic background of cohort members was assessed using three indicator measures. These included the following.
(1) Family socioeconomic status (at birth): This was assessed at the time of the survey child's birth using the Elley–Irving scale of socioeconomic status for New Zealand [35]. This scale classifies socioeconomic status into six levels on the basis of paternal occupation.
(2) Maternal education. Maternal education was assessed at the time of the survey child's birth using a 3-point scale that reflected the highest level of educational achievement attained. This scale was as follows: 1 = mother lacked formal educational qualifications; 2 = mother had secondary level educational qualifications; 3 = mother had tertiary level qualifications.
(3) Leaving school without qualifications. At age 18, sample members were questioned regarding their educational history. In particular, information was obtained on the number of School Certificate subjects attempted and grades received. Sample members who left school without obtaining any formal qualifications (school certificate or higher) were classified as leaving school without qualifications.
Family adversity
Family adversity measure
A measure of family adversity was calculated using a count measure of 38 different measures of family disadvantage during the period 0–15 years, including measures of disadvantaged parental background, poor prenatal health practices and perinatal outcomes, and disadvantageous child-rearing practices [36].
Statistical analysis
The unadjusted association between ethnic identity and the repeated measures of total number of mental health disorders was tested for statistical significance by fitting generalized estimating equation (GEE) models [37], [38] to the data. A Poisson regression model was fitted of the form:

To adjust the observed associations between ethnic identity and rate of mental health disorders for confounding, the aforedescribed regression model was extended to include the covariate factors in two stages. In the first stage, socioeconomic factors were entered into the model, while in the second stage, the measure of family adversity was added to the model containing both ethnic identity and socioeconomic factors.
Results
Associations between cultural identification and mental health outcomes
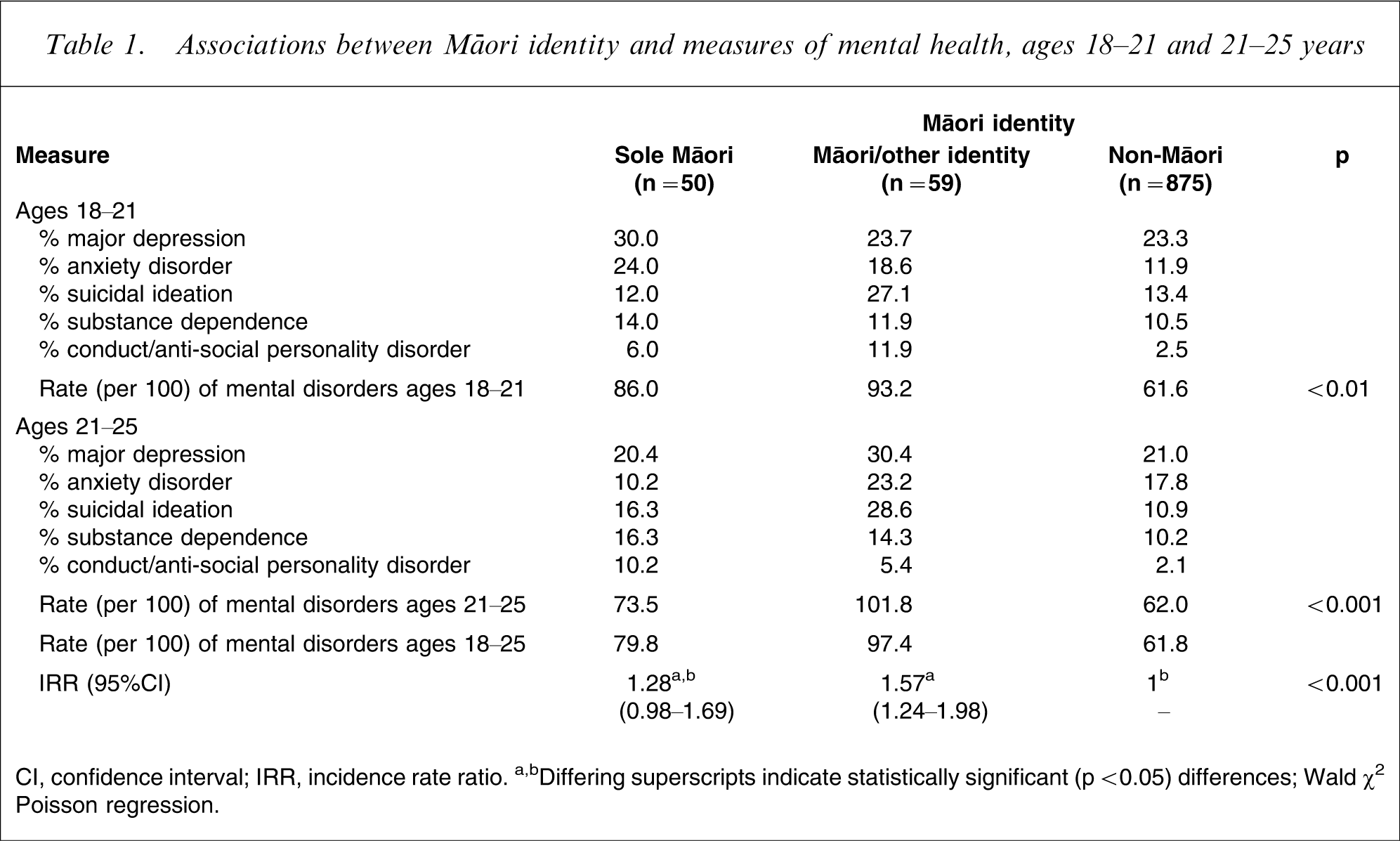
Table 1 shows the sample classified into three groups on the basis of ethnic identification reported at age 21: non-Māori (n = 875), sole Māori identity, (n = 50) and Māori/other ethnic identity (n = 59). For each group Table 1 shows rates of mental health outcomes over the periods 18–21 and 21–25 years. Inspection of Table 1 shows that (i) over the period for ages 18–21, non-Māori reported the lowest rates of total mental health disorder (61.6 per 100); sole Māori the next highest rates (86.0 per 100) and the Māori/Other identity group the highest rates (93.2 per 100); and (ii) the same pattern is evident at ages 21–25, with non-Māori having the lowest rate of total mental health disorders (62.0 per 100), sole Māori the next highest rates (73.5 per 100), and the Māori/other identity group the highest rates (101.8 per 100).
Associations between Māori identity and measures of mental health, ages 18–21 and 21–25 years
CI, confidence interval; IRR, incidence rate ratio.
a,bDiffering superscripts indicate statistically significant (p < 0.05) differences; Wald χ2 Poisson regression.
To test these trends for significance, a Poisson regression model was fitted to the rate data at ages 18–21 and 21–25. The results of this analysis are summarized at the foot of Table 1, which reports the following.
Overall significance of ethnicity as a predictor of the overall rate of mental health problems
The results show a highly significant tendency (p < 0.001) for overall rates of mental disorder to vary with ethnic identification.
Pairwise contrasts between the three groups
These show that non-Māori had rates of mental health problems that were marginally significantly lower than those of sole Māori (p < 0.10), and significantly lower than those of Māori/other identity (p < 0.05).
Estimates of the pooled IRR
These estimates show that those of sole Māori ethnicity had rates of mental health problems that were 1.28-fold higher (95%CI = 0.98–1.69) than for non-Māori. The Māori/other identity group had rates that were 1.57-fold higher (95%CI = 1.24–1.98) than non-Māori.
While the overall results in Table 1 suggest that rates of disorder followed the ordering given here, this pattern is not evident for all of the specific comparisons in Table 1. For example, at ages 18–21 sole Māori had higher rates of major depression than the Māori/other identity group, whereas at 21–25 years this pattern is reversed. It is likely that such inconsistencies reflect the relatively small group size of the sole Māori and Māori/other identity groups and the relatively low rates of disorder within these groups. Both factors would appear to contribute to the apparent instability and inconsistency between groups. For these reasons, the present analysis has been confined to an examination of overall mental health problem rather than to differences in specific outcomes.
Adjustments for socioeconomic and family adversity
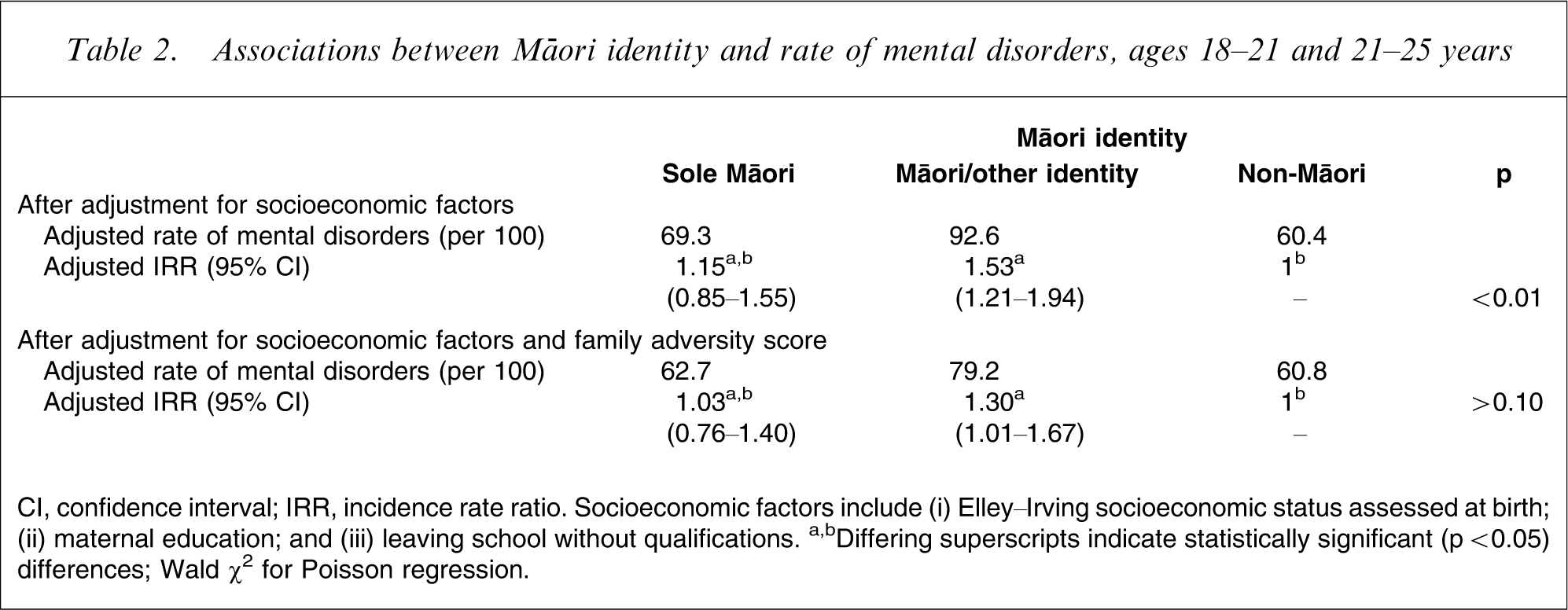
One explanation for the ethnic differences observed in Table 1 is that these differences reflect between-group differences in exposure to (i) socioeconomic disadvantage; and (ii) family adversity. Specifically, further analyses suggested that there were associations between cultural identification and (i) socioeconomic status at birth (p < 0.0001); (ii) maternal education (p < 0.001); (iii) leaving school without qualifications (p < 0.01); and (iv) exposure to family adversity (p < 0.0001). These findings suggest that the higher rate of mental health problems among Māori could be due to these factors. To examine these issues, the association between cultural identification and overall rates of mental health problems shown in Table 1 were adjusted to take account of these socioeconomic and family adversity factors. The results of this analysis are shown in Table 2, which shows rates of mental health problems and IRR after adjustment for socioeconomic and childhood factors, including the following.
Associations between Māori identity and rate of mental disorders, ages 18–21 and 21–25 years
CI, confidence interval; IRR, incidence rate ratio.
†Socioeconomic factors include (i) Elley–Irving socioeconomic status assessed at birth; (ii) maternal education; and (iii) leaving school without qualifications.
a,bDiffering superscripts indicate statistically significant (p < 0.05) differences; Wald χ2 for Poisson regression.
(1) Adjustment for socioeconomic factors explained a substantial component of the association between cultural identification and mental disorder. Nonetheless, there was still a significant association (p < 0.01) between cultural identity and rates of disorder, with those of sole Māori identify having rates that were 1.15-fold higher (95%CI = 0.85–1.55, p > 0.30) than non-Māori, and those of Māori/other identity having rates that were 1.37-fold higher (95%CI = 1.21–1.94, p < 0.0001) than non-Māori.
(2) Adjustment for family adversity and socioeconomic factors reduced the associations further. After this adjustment, rates of disorder for sole Māori were almost the same as among non-Māori (IRR = 1.03, 95%CI = 0.76–1.40, p > 0.80). But those in the Māori/other identity group had significantly higher rates of disorder than non-Māori (IRR = 1.30, 95%CI = 1.01–1.67, p < 0.05).
Discussion
In this paper we have used data gathered over the course of a 25 year longitudinal study to explore the linkages between Māori cultural identity, socioeconomic disadvantage, and risks of mental health problems in young adults. The findings confirm recent research that suggests that Māori continue to have higher rates of mental disorder than non-Maori [39]. In the present study, sole Māori had rates of disorder that were 1.3-fold higher than non-Māori, and those of mixed Māori/other identity had rates that were 1.6-fold higher than non-Māori. These results are consistent with the findings reported in Te Rau Hinengaro: the New Zealand Mental Health Survey that found that overall, Māori had rates of mental disorder that were 1.28-fold those of non-Māori before correction for age and other factors [6].
The results of the present study suggest that the higher rates of mental disorders among young Māori in this cohort were shaped by two sets of processes. First, much of the elevated rate of disorder among young Māori was explained by the fact that members of this group tended to come from socially disadvantaged backgrounds and had higher exposure to childhood adversity. In these respects, the risk factors and life processes that place young Māori at risk of mental disorder seem to be very similar to those that place non-Māori at risk of disorder. These conclusions are borne out by international comparisons, which show that social disadvantage and childhood adversity are factors common to increased risks of mental health disorders in a wide range of cultural settings [40–43]. However, more refined analyses suggested that the effects of social disadvantage and childhood adversity on mental health risks for Māori were modified by cultural identity status. In particular, being of sole Māori status was a protective factor that appeared to mitigate risks of mental health problems. This pattern of results provides some support for the current theorizing on the role of a secure Māori cultural identity to serve as a safeguard against mental ill health [4], [28]. At the same time, however, other explanations for these results require consideration.
In particular, the analyses undertaken assumed a unidirectional relationship in which variations in Māori identity have the potential to influence mental health status. But, given that the measurement of cultural identity of respondents included in the present study was recorded at age 21, it is unclear in which direction the causal relationship between cultural identity and mental health status is best interpreted. That is, while we may assume that respondents with a sole Māori identity are more likely to experience good mental health, it is equally feasible that having good mental health leads one to more strongly identify as being sole Māori. Concomitantly, individuals who are experiencing psychological difficulties may be less inclined to identify with the criteria used to establish cultural identity status. Further research is needed to clarify the causal ordering of Māori cultural identity and mental health status in more detail.
Further, it is not clear what features of a secure Māori identity protect the development of poorer mental health outcomes for Māori. A standard set of criteria was used in the present study to establish the cultural identity status of Māori respondents; but a similar scale was not used to classify non-Māori respondents in the same regard. It is therefore difficult to determine with any certainty what the mechanisms leading to either protection from, or risk of, mental illness for Māori might in actuality consist of.
Two views have come to dominate discussion in New Zealand regarding the persistent differences in mental health status between Māori and non-Māori. The first view has argued that the discrepancy between groups is best understood as resulting from Māori becoming dislocated from traditional cultural domains and activities [4], [26], [44]. Macro-influences such as colonization and the rapid urbanization of Māori have been identified as significantly impacting on Māori social organization. As a consequence of these influences, Māori collective well-being has been diminished, which has led to the overrepresentation of Māori in the mental health indices. From this perspective, poor mental health outcomes for Māori are related to an afflicted cultural identity. Therefore, it is believed that improvements in the mental health status of Māori will be achieved through taking into consideration the diversity within the Māori population and by focusing on enhancing the collective cultural identity of Māori [4].
The alternative view proposes that the disparity in mental health status between Māori and non-Māori is a result of Māori occupying a more marginalized position within New Zealand and being more likely to experience discrimination through institutional and interpersonal racism [7], [8], [19]. From this position, it is changes in current systemic structures and processes that will improve the socioeconomic position of Māori and by association lead to better mental health outcomes. Proponents of this view consider the previous perspective to be built on a cultural deficit model and therefore largely reject the conclusions that it draws about contemporary Māori society [45]. Moreover, it is believed that it is the disparities between Māori and non-Māori that require ongoing investigation rather than examining the diversity within the Māori population.
The present findings suggest that both perspectives are partially true but incomplete, and that the elevated rates of mental health problems seen in Māori within this cohort were the result of a combination between cultural identity factors and social disadvantage. Those most at risk in this study were respondents who possessed a Māori/other ethnic identity and who were exposed to higher social adversity. These conclusions suggest the need for a revision and expansion of the explanatory frameworks within which the mental health of Māori is currently theorized to recognize the accumulative effects of cultural identity and social adversity on risks of mental health problems.
There are a number of important caveats that should be imposed on these conclusions. First and foremost, the present findings are based on a particular birth cohort born in a particular geographic region and study over a specific time period. The extent to which the findings based on this cohort generalize to other New Zealand cohorts and regions remains to be determined. A second limitation of the study is that because of the relatively small sample of Māori and the relatively low rates of specific disorders, it was not possible to conduct a fine-grained analysis of the linkages between cultural identity and specific disorders. There is clearly a need for further research to examine these issues in larger samples. Third, we acknowledge that the construct of cultural identity should not be conflated with individual self identity. To do so would be to deny the complexity integral to identity. Finally, the research reported here is subject to the usual limitations of reporting and other errors in data provided by survey methods. Within these limitations, the present results suggest that although social adversity is the principal contributing factor leading to the higher rate of mental health problems experienced by Maori, cultural identity may also play an important role.
Footnotes
Acknowledgements
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.