
Abstract
There continues to be debate about the status of cannabis in New Zealand [1], [2]. An important feature of this debate, which has recently gained prominence, is the issue of ethnic differences in patterns of cannabis use [3]. Te Rau Hinengaro: the New Zealand Mental Health Survey indicated that cannabis abuse and dependence by Māori is a major contributor to the overrepresentation of Māori with diagnosable substance use disorders [4]. The New Zealand Health Behaviours Survey corroborated and extended upon this finding, reporting that when compared to other New Zealanders, Māori began using cannabis at an earlier age, consumed more potent forms of the substance, used it more frequently, and were more likely to engage in either daily or binge use [5]. Moreover, Māori were significantly more likely to report harmful effects from their cannabis use including having experienced a physical health-related problem [5]. These findings have been reinforced by a range of studies that have conducted comparative analyses examining ethnic differences in cannabis use and dependence [6–9]. A further aspect of the debate has involved linkages between the disproportionate use of cannabis by Māori and an elevated risk of Māori engagement with police authorities [10], [11].
The consistent associations between Māori ethnicity and cannabis use raise a number of significant issues. Perhaps the most important of these concerns the factors that place Māori at greater risk of cannabis use and dependence. There are at least three explanatory frameworks that are frequently used to account for inter-ethnic differences in cannabis use by New Zealanders.
The first framework favours a socioeconomic explanation and is informed by the social deprivation thesis. It has been well-documented that Māori are at greater risk of socioeconomic disadvantage when compared with other New Zealanders classified by ethnicity [12–15]. On this account, it is the relative economic disadvantage of Māori that leads to Māori overrepresentation in cannabis use and dependence. This view implies that Māori are no more likely to be involved in cannabis use than non-Māori experiencing similar social and economic circumstances. The influence of this perspective is evident in current policies that aim to reduce ethnic disparities in drug-related harm by encouraging the economic transformation of Māori communities [3].
A second explanation emerges from social learning theory and suggests that ethnic differences for cannabis use in New Zealand may be the result of a process involving the inter-generational transmission of behaviours linked to ongoing social and familial adversity. Accordingly, the elevated rate of cannabis use among Māori arises from their being over-exposed during childhood and adolescence to the adverse factors that are known to be associated with illicit drug use in later life. It has been well-documented that Māori are at higher risk of experiencing social and familial adversity in younger life and also more likely to engage in higher levels of behavioural risk during adolescence when compared to other New Zealanders [13], [16–18]. Therefore, independently of socioeconomic disadvantage, the higher exposure of Māori to social and familial adversity may explain the higher rate of cannabis use among Māori. The influence of this view is evident in a range of policy documents, which advocate the whanau ora concept whereby Māori families are supported to achieve maximum health and well-being [19], [20].
The third framework involves a systemic theory of colonization and relates to Māori cultural identity. From this perspective, current disparities, where Māori are overrepresented, are the direct result of historical and structural processes originating from the colonial settlement of New Zealand [21], [22]. The imposing of Eurocentric beliefs, values, and practices upon Māori along with the introduction of psychoactive substances has led to the social fragmentation of Māori society. As a consequence, it is contended that Māori have experienced cultural dislocation and social defeat, which has led to Māori becoming estranged from traditional cultural domains and concepts, resulting in diminished cultural identities [23], [24]. Therefore, this perspective proposes that the disproportionate use of cannabis by Māori is directly linked to loss of attachment to cultural domains and a thwarted cultural identity. The influence of this explanatory framework is observable in current alcohol and drug interventions specifically targeting Māori whereby the focus is on fostering cultural reattachment and restoration of cultural identity [25], [26].
A further and equally important question pertinent to the cannabis debate is the extent to which ethnic differences in others areas such as health, education, and well-being are attributable to the overrepresentation of Māori using cannabis. It has now been well-documented that the heavy use of cannabis may lead to a number of adverse outcomes, including reduced levels of school achievement; increased risks of mental health problems; and increased risks of unemployment and welfare dependence [27–29]. The overrepresentation of Māori in each of these domains has been well-established [4], [13].
Against this background, this paper uses data gathered over the course of a 25 year longitudinal study to address two general issues relating to ethnic difference in cannabis use in New Zealand. The first part of the analysis explores the extent to which ethnic differences in cannabis use, abuse, and dependence can be explained by socioeconomic differences, social learning processes, and variations in cultural identity. The second part of the analysis examines the extent to which ethnic differences in cannabis use may account for ethnic differences in educational achievement, employment, and mental health problems. The aims of the paper are to explore the origins of the higher rate of cannabis use by Māori and to examine the contribution of cannabis to ethnic disparities in health, education and socioeconomic outcomes.
Methods
The data were gathered during the course of the Christchurch Health and Development Study (CHDS). In that study a birth cohort of 1265 children (635 boys, 630 girls) born in the Christchurch (New Zealand) urban region in mid-1977 has been studied at birth, 4 months, 1 year and annually to age 16 years, and again at ages 18, 21 and 25 years. Information from a variety of sources has been used including parental interviews; teacher reports; self-reports; psychometric assessments; medical and other record data [30], [31]. The present analyses were based on those individuals for whom data on ethnic identity were available from the age 21 assessment (n = 1011, 79.9% of the original cohort).
Ethnic identity
At age 21 years respondents were asked about their ancestry, cultural identification, level of participation in Māori cultural domains, and proficiency in the Māori language [32]. On the basis of this questioning, 11.1% of sample members self-identified as New Zealand Māori (in the 2006 New Zealand census, 14.6% of the population were reported to have self-identified as New Zealand Māori [33]). A further breakdown of this group showed 45.9% reporting sole Māori identity and 54.1% reporting Māori ethnic identity and identity with another ethnic group. For the purposes of the present analyses, those reporting sole Māori identity were classified as having a sole Māori identity, while those reporting both Māori identity and another ethnic identity were classified as having Māori/other ethnic identity. In addition, both groups were combined to form a Māori ethnicity group. All other participants were classified as being non-Māori. Comparisons of the sole Māori and Māori/other group showed consistent differences between the groups across several aspects of participation in Māori culture [32]. The descriptors of ‘sole Māori’, ‘Māori/other ethnic identity’, and ‘non-Māori’ were originally recommended by Pomare et al. in their analyses examining ethnic trends in public health epidemiology [34].
Cannabis use outcomes, ages 14–25
At the 15, 16, 18, 21, and 25 year assessments, participants were questioned as to the number of occasions on which they had used cannabis during each year since the previous assessment, and the frequency with which they had used cannabis during that year. For the purposes of the present study, these questions were used to form several measures of cannabis use during the period 14–25 years. These measures included the following.
Percentage using cannabis, ages 14–25. All participants who indicated using cannabis on at least one occasion during the period 14–25 years were classified as having used cannabis. Percentage using cannabis weekly, ages 14–25. All participants who indicated that they had used cannabis at least weekly during one of the annual intervals at ages 14–25 were classified as having used cannabis weekly. Mean number of times using cannabis, ages 14–25. The measures of the number of occasions on which participants reported using cannabis were summed for the period 14–25 years to arrive at an estimate of the total number of times participants had used cannabis during the period 14–25 years (mean = 228.1, SD = 473.9).
In addition, a measure of cannabis dependence during the period 14–25 years was obtained using questions based on the generic DSM-IV [35] criteria for substance dependence derived from the Composite International Diagnostic Interview (CIDI) [36]. Participants were classified as being cannabis dependent during the period 14–25 years if they met the DSM-IV criteria for cannabis dependence at any point during that period.
The percentage measure of cannabis use (ever) is similar to those used in a number of prevalence studies [37–40]. In addition, the measure of weekly cannabis use was included due to evidence suggesting that weekly use may serve as a threshold for later problems with cannabis [41]. Finally, the measure of total number of occasions using cannabis has been used in a previous study of the present cohort, in which increasing numbers of occasions using cannabis were linked to a range of adverse outcomes, including lower levels of education, higher levels of welfare dependence and unemployment, and lower levels of relationship and life satisfaction [42].
Life outcomes
Over the period 18–25 years, cohort members provided information regarding a range of life outcomes. The outcomes examined in the present investigation included the following.
Education
Left school without qualifications
Sample members were classified as leaving school without qualifications if they had left school by age 18 without achieving a passing grade in at least one School Certificate examination.
Attained university degree or equivalent (by age 25)
Sample members were classified as having attained a Bachelor-level or higher degree by age 25.
Income and employment
Below median income level (age 25)
Individuals in the lower 50% for income at age 25 were classified as being below the median income level.
Unemployed for ≥6 months (ages 21–25)
Participants who reported being unemployed and looking for work for >6 months consecutively at any time during the period 21–25 years were classified as having been unemployed for ≥6 months.
Welfare dependence (ages 21–25)
Participants who reported receiving an unemployment benefit, a domestic purposes benefit (available to single parents with dependent children), or a sickness or invalid benefit at any point in the period 21–25 years were classified as having been welfare dependent.
Mental health
Rates of mental disorder (ages 21–25)
Mental disorder was assessed using the CIDI [36], supplemented by additional measures. This information was used to construct a measure of mental health problems over the interval 21–25 years, which was the sum of the responses for each of five categories of mental health disorder (major depression; anxiety disorder; substance dependence; suicidal ideation; anti-social personality disorder), resulting in scores that ranged from 0 (reported no mental health disorders) to 5 (met diagnostic criteria in all five categories).
Criminal offending
Self-reported property/violent offending (ages 18–21)
Criminal behaviour was assessed using the Self-Report Delinquency Inventory [43] supplemented by additional custom-written survey items. This information was used to derive count measures of the number of self-reported property/violent offences committed in each year during the period 18–21 years.
Intimate partner violence
Intimate partner violence perpetration and victimization (age 24–25)
Intimate partner violence (IPV) was assessed using a 22-item scale that incorporated selected items from the Revised Conflict Tactics Scale [44], including items pertaining to psychological aggression, and both minor and severe physical violence. To devise measures of IPV perpetration and victimization, the frequency scores for each item were summed to create measures of the number of incidents of IPV perpetration and victimization experienced by the participants.
Covariate factors
Socioeconomic background
The socioeconomic background of cohort members was assessed using several indicator measures chosen from the database of the study. These included the following.
Maternal age
Assessed at the survey child's birth.
Paternal education (at birth)
The education level of the natural father of each participant was assessed at the time of the survey child's birth using a 3 point scale that reflected the highest level of educational achievement attained.
Family living standards (0–10 years)
At each year an assessment of the material living standards of the family was obtained via interviewer rating on a 5 point scale that ranged from ‘very good’ to ‘very poor’. These were averaged over the 10 year period to give a measure of family living standards during this period.
Family socioeconomic status (at birth)
This was assessed at the time of the survey child's birth using the Elley–Irving scale of socioeconomic status for New Zealand [45].
Family functioning factors
Measures of family functioning were also chosen from the study database. These measures included the following.
Parental illicit drug use (0–11 years)
Cohort members were classified as having a parent history of illicit drug use if one of his/her parents was reported to have a history of illicit drug use.
Parental alcoholism (0–15 years)
A dichotomous measure of whether or not the young person's parents reported experiencing alcoholism or problems with alcohol.
Parental criminality (0–15 years)
Cohort members were classified as having a parent history of criminality if one of his/her parents was reported to have a history of offending.
Family adversity measure (0–15 years)
A measure of family adversity was calculated using a count measure of 38 different measures of family disadvantage during the period 0–15 years, including measures of disadvantaged parental background, poor prenatal health practices and perinatal outcomes, and disadvantageous child-rearing practices [46].
Results
Associations between cannabis use, cannabis dependence, and cultural identity
Table 1 shows the cohort divided into Māori (n = 114) and non-Māori (n = 897) groups. For each group Table 1 reports a number of summary statistics describing patterns of cannabis use and dependence to the age of 25. These statistics include the percentage ever using cannabis by 25; the percentages meeting DSM-IV diagnostic criteria for cannabis dependence; the fraction of the cohort who had ever been regular weekly users of cannabis, and the mean number of times that respondents had reported using cannabis to age 25. Each comparison was tested for statistical significance using logistic regression (for percentage outcomes) and negative binomial regression (for count measures). In addition, Table 1 shows estimates of the odds ratio (OR) and incidence rate ratio (IRR), which provides an approximate measure of the risks of a given outcome among Māori when compared to the risk for non Māori. In all comparisons there was evidence of significant relationships between cultural identity and cannabis use outcomes, with those reporting Māori identity having rates of cannabis use and dependence that were significantly higher (p < 0.05) than rates for non-Māori.
Cultural identity and cannabis use outcomes, ages 14–25
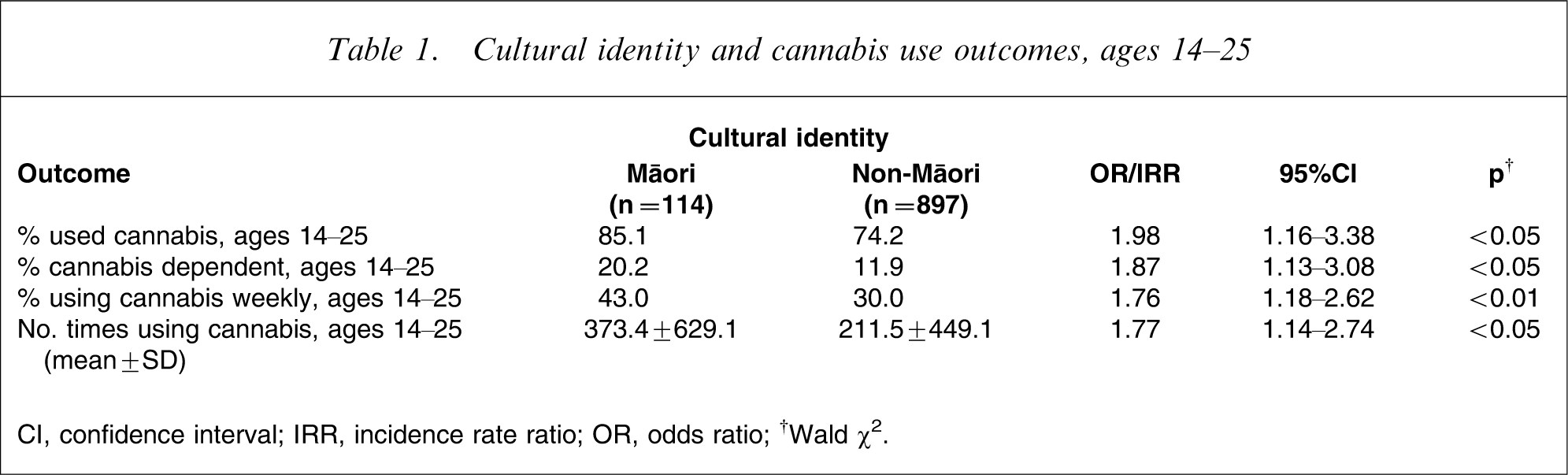
CI, confidence interval; IRR, incidence rate ratio; OR, odds ratio.
†Wald χ2.
In order to examine differences among the two Māori identity groups, further analyses compared cannabis use outcomes among those individuals in the sole Māori (n = 52) and Māori/other identity (n = 62) groups. Table 2 shows the results of comparisons between sole Māori and Māori/other identity groups, and these were not significantly different. These results suggested that cannabis use and dependence did not vary with degree of cultural identity among Māori. Because no significant differences were found between the two Māori identity groups, for the purposes of statistical precision, all subsequent analyses were conducted using the two-group classification of ethnicity (Māori and non-Māori groups).
Māori identity and cannabis use outcomes, ages 14–25
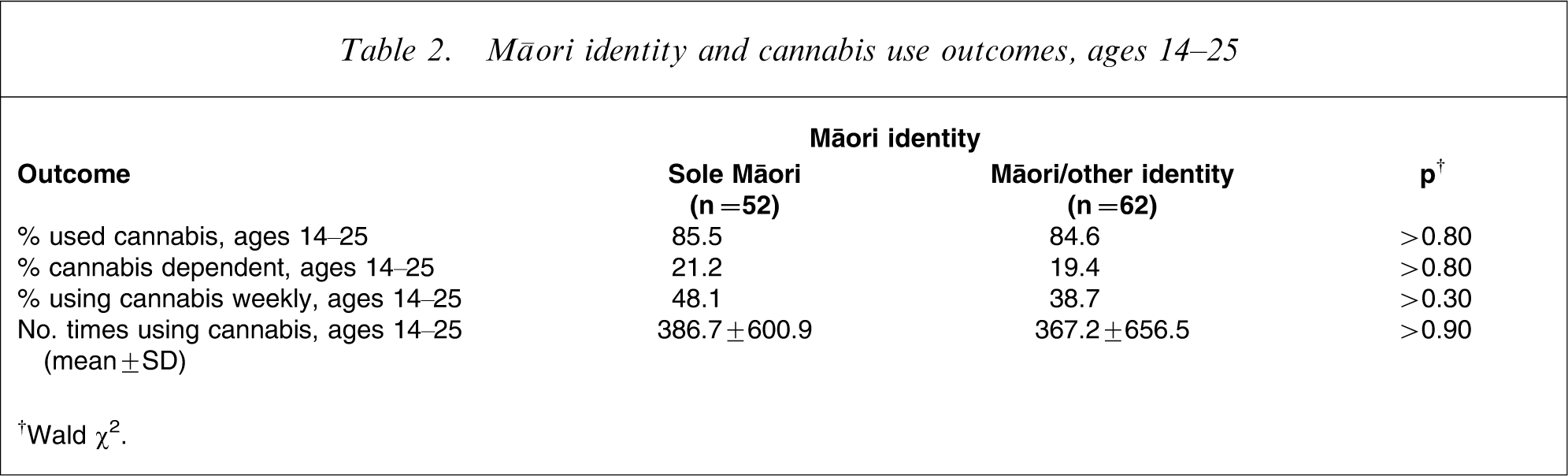
†Wald χ2.
Tests of socioeconomic and social learning explanations
To examine the extent to which ethnic differences in cannabis use could be explained by socioeconomic factors and social learning processes, the associations between cultural identity and cannabis use abuse and dependence were adjusted for socioeconomic and childhood factors using a two-stage regression approach.
The first-stage model fitted to the data controlled the associations for measures of socioeconomic status including maternal age, paternal education, socioeconomic status at birth, and average family living standards to age 10. All covariate factors were entered into the models. In the second stage of the analysis the first-stage model was extended to include a series of childhood and family factors that were known on the basis of previous research into this cohort to be associated with cannabis use. These factors included parental alcohol problems, parental criminal offending, parental illicit drug use, and a measure of family adversity. Again, all covariate factors were entered into the models.
The results of this analysis are shown in Table 3, which reports ORs and IRRs for the associations between cultural identification and cannabis use after adjustment for: (i) socioeconomic factors; and (ii) socioeconomic and childhood/family factors. Table 3 shows that (i) adjustment for socioeconomic factors reduced the associations between cultural identity and cannabis use and dependence to statistical non-significance, although there remained some suggestion of an association between cultural identity and cannabis use (the association between cultural identity and cannabis use remained marginally statistically significant, p > 0.05); and (ii) adjustment for both socioeconomic and childhood/family factors further reduced the magnitude of the associations between cultural identity and cannabis use and dependence.
Adjusted models of ethnic identity and cannabis use outcomes (ages 14–25)
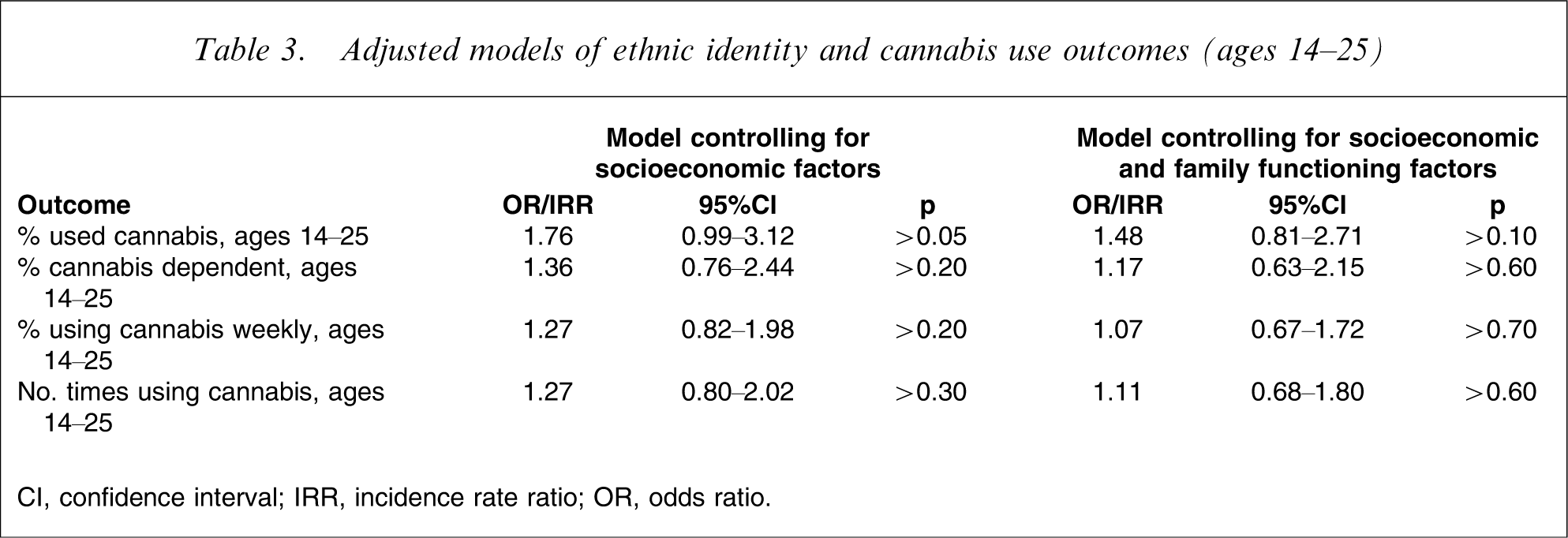
CI, confidence interval; IRR, incidence rate ratio; OR, odds ratio.
The implication of the findings in Table 3 is that the associations between cultural identity and cannabis shown in Table 1 were largely, if not wholly, explained by the greater exposure of young Māori to socioeconomic disadvantage and childhood/family adversity. After adjustment for these factors there was little evidence to suggest that being of Māori ethnicity per se was a risk factor for cannabis use and dependence.
Consequences of cannabis use for ethnic disparities in outcomes
To examine the contribution of cannabis use to ethnic differences in rates of education completion, income and employment, mental health, criminal offending, and IPV, the associations between ethnicity and these outcomes were estimated before and after adjustment for cannabis use prior to age 21. The results of these findings are summarized in Table 4, which compares the associations between ethnicity and each outcome before and after adjustment for cannabis use. The measures of association reported are the OR and IRR, which provides an approximate measure of the risks of a given outcome among Māori when compared to the risk for non-Māori.
Ethnic identity and life outcomes by age 25 before and after control for cannabis use during ages 14–21
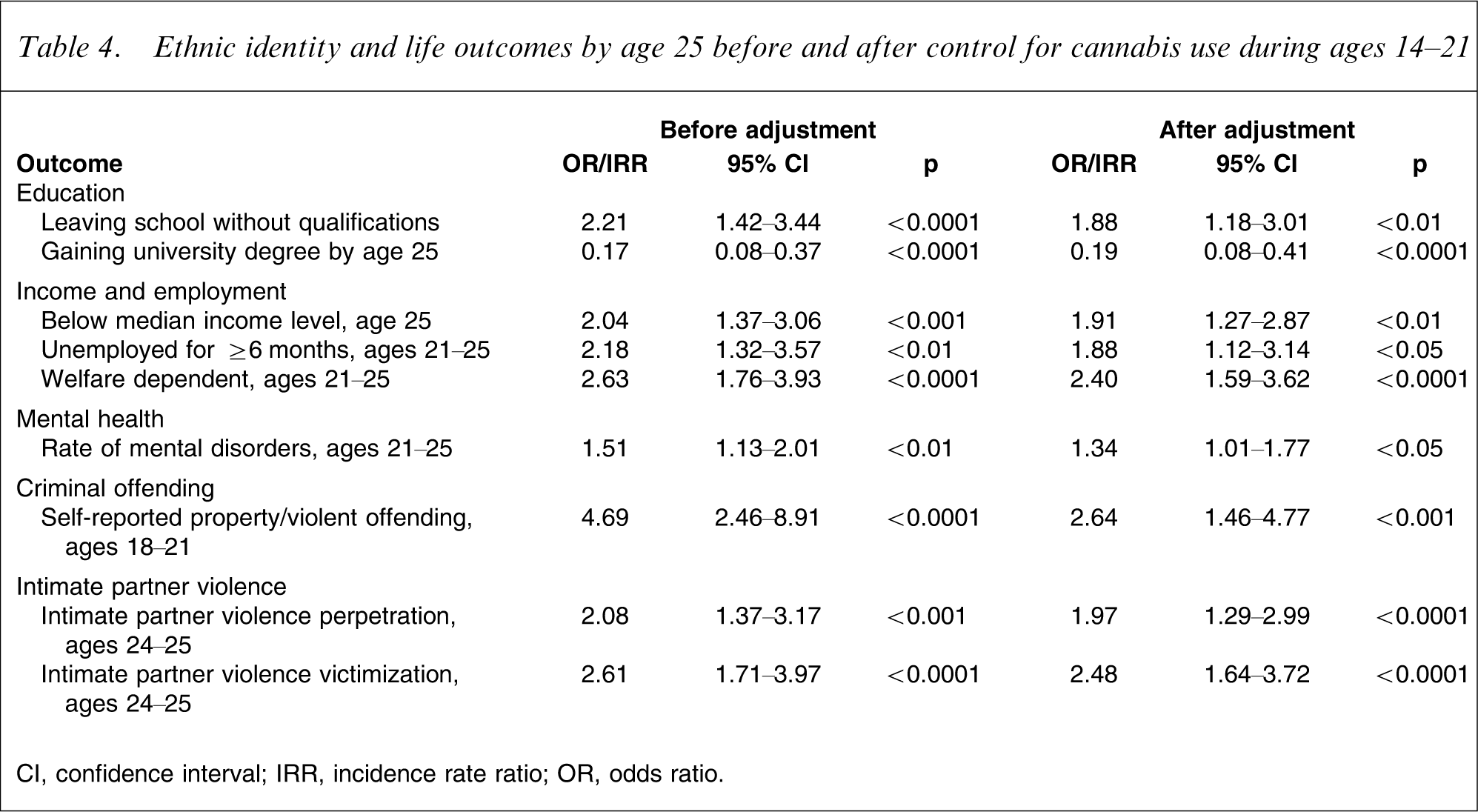
CI, confidence interval; IRR, incidence rate ratio; OR, odds ratio.
Table 4 shows that in all cases, control for cannabis use reduced the associations between cultural identity and outcomes. The size of this reduction varied from outcome to outcome, with control for cannabis use having greatest effect on measures of self-reported offending, leaving school without qualifications, and being unemployed for ≥6 months. These findings suggest that the use of cannabis made a small but detectable contribution to rates of Māori disadvantage, with this contribution being most evident in the areas of crime, education, and unemployment.
Discussion
This research has used data gathered over the course of a 25 year longitudinal study to examine the linkages between ethnicity and cannabis use, and to explore the role of cannabis use as a driver of disadvantage among Māori. This study leads to three major conclusions.
First, in agreement with previous research [5–9], there were consistent trends for cohort members reporting a Māori identity to have higher rates of cannabis use and dependence during adolescence and young adulthood. This finding is in general agreement with a number of studies that have found high rates of cannabis use and dependence among a range of indigenous communities [47–49]. Among those reporting Māori identity, however, rates of cannabis use and dependence did not differ detectably between those reporting a sole Māori identity and those reporting a Māori/other identity. These results led to the conclusion that among Māori in this cohort, variations in cultural identity did not influence patterns of cannabis use. This conclusion is contrary to the assumptions underpinning the systemic theory of colonization, which suggest that strength of Māori cultural identity is inherently related to risk of cannabis use and dependence [21], [22]. Clearly, this result raises important questions about the potential efficacy of current intervention models developed by and for Māori, which pivot on the notion that strengthening cultural identity will lead to reductions in cannabis-related harm experienced by Māori.
Second, the results of regression analyses suggested that the linkages between ethnicity and cannabis were largely explained by two general pathways that place young Māori at greater risk for cannabis use and dependence. The first pathway involved the linkages between ethnicity and socioeconomic disadvantage. Statistical adjustment for socioeconomic factors including: maternal age; paternal education level; socioeconomic status at birth; and average family living standards to age 10; in part explained the associations between ethnicity and cannabis use. The second pathway involved the higher exposure of Māori to childhood and family factors known to increase risks of illicit drug use. These factors included parental alcohol problems and illicit drug use; parental criminal offending; and family adversity. The net effect of socioeconomic disadvantage and higher exposure to early adversity was to place young Māori at greater risk of cannabis use and dependence.
These findings clearly suggest that the factors influencing the higher rate of cannabis use among Māori are socioeconomic and familial rather than cultural in origin. The risk factors and life processes that led young Māori to cannabis use and dependence appear to be the same as those leading non-Māori to engage in the same behaviour [39]. These results provide empirical support to the social deprivation and social learning models described earlier, to account for ethnic differences in cannabis use between Māori and other New Zealanders. The major implication of this finding is that improvements in the economic welfare of Māori along with the provision of early intervention programmes tailored to enhance healthy family development may provide the most promising avenue to improve later outcomes for Māori [50]. It should be noted, however, that based on the evidence provided, such initiatives are likely to be of equal benefit to non-Māori experiencing similar problems with cannabis and who are also raised in environments characterized by economic disadvantage and socio-familial adversity.
Third, the study examined the extent to which the higher rate of cannabis use by Māori contributed to ethnic disparities in the areas of education, income and employment, mental health, crime, and IPV. This analysis suggested that a component of the associations between ethnic identification and adverse outcomes was explained by cannabis use, with these contributions being most evident for early school leaving, unemployment, and crime. These findings suggest that the higher rates of cannabis use by Māori may make a small but detectable contribution to disadvantage among Māori, and in particular in education, unemployment, and crime.
The present findings are subject to a number of caveats. In particular, the study findings are based on a particular cohort born in a specific geographic region and studied over a specific time period. The extent to which the study findings generalize to other cohorts, times and regions is not known. In addition, the present findings may be limited both by the accuracy of the self-reported cannabis use and outcomes among the cohort members, and by the choice of measures used to assess cannabis use and dependence during the period 14–25 years.
Within the limitations of the study the research suggests three major conclusions about ethnic disparities in the use of cannabis. First, Māori ethnic identification is associated with increased risks of cannabis use and dependence. Second, the higher rate of cannabis use by Māori can be attributed to a combination of socioeconomic factors and greater exposure to environmental factors known to influence risk of cannabis use. Finally, the higher rates of cannabis use by Māori may make a small contribution to the higher rates of early school leaving, crime, and unemployment among Māori.
Footnotes
Acknowledgements
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.