
Abstract
Schizophrenia in women has a more favourable outcome than in men with the disease [1,2]. Speculations regarding the reasons as well as the implications of this sex difference in disease course have involved differential cognitive decrements, among others. The role of specific neurocognitive deficits in community functioning has been supported by several studies, which found them to act as rate-limiting factors that restrict the social and vocational functioning of schizophrenia patients in the outside world. Community functioning has been found to be related to verbal memory, card sorting (executive functioning/set shifting), as well as verbal fluency [3,4]. Other independent cognitive domains that have been suggested as predictors of community adjustment include visual memory [3,5,6] and visuospatial ability [5], executive functioning/inhibition [7], working memory [8], fluency in general (consisting of verbal and design fluency tasks) [6], and problem-solving skills [9]. Consequently, it has been suggested that sex differences in the performance of schizophrenia patients in specific domains of cognitive functioning might contribute to the poorer social course of men with schizophrenia in comparison to women suffering from the disease.
Evidence from the literature addressing sex differences in cognition in schizophrenia remains equivocal. Some of the methodological limitations that might explain inconsistencies of study results are poor sampling strategies leading to male–female differences in age, level of education, age of onset and duration of illness, psychopathology, premorbid functioning, antipsychotic regimen, and chronicity; inadequate sample sizes to test for sex effects; absence of healthy comparison subjects to adequately address empirically established normal sex differences in healthy cognitive functioning; and failure to match normal comparison subjects within sex on age and level of education [10,11]. Some researchers have suggested that male schizophrenia patients are more impaired than female patients in language, learning and verbal memory [12–14], verbal abstraction/executive functions [12,15], attention [12] and visuospatial ability [12], while others do not find significant sex differences in cognitive functioning in schizophrenia [14,16–22]. Finally, some investigators have reported greater deficits in verbal memory, spatial memory, and visual processing among women as compared with men with schizophrenia [17,23].
When studying the relative cognitive functioning of male and female schizophrenia patients, it is critical to take into account the differential pattern of cognitive performance typically observed in healthy men and women. Although men and women tend to perform equally in most cognitive domains, there are some well-documented gender-related differences in certain neurocognitive functions. This is the case for tests of visuospatial skills, especially those that require mental rotation of stimuli, where men, in general, tend to outperform women [24–31]. In contrast, women tend to perform better than men on tests of verbal abilities, mainly verbal fluency [29,31–34], and tests of verbal memory [24,25,35,36]. Several studies, however, have failed to find the putative female superiority on tests of verbal fluency [25,26,37–39]. Moreover, it is possible that women's better performance in tests of verbal fluency and verbal memory may be due to the use of gender-biased categories, such as fruits on a verbal fluency test [40,41], or spices and clothes on the California Verbal Learning Test [14]. Very few of the aforementioned studies addressing sex differences in schizophrenia took into account the performance differences observed in healthy men and women. In doing so, they assumed an equal comparison baseline for both genders, which, in fact, may be inaccurate.
In the present study we investigated whether the differential pattern of cognitive performance observed in healthy men and women is preserved in male and female schizophrenia patients. We predicted not only that schizophrenia patients as a whole would perform more poorly than healthy controls in every cognitive domain, but also that we would observe the gender differences in cognitive functioning often observed in the literature on normal information processing, namely, that male participants would outperform female participants on visuospatial tests, while female participants would do better on verbal fluency and verbal learning and memory. No prediction could be made about whether the pattern of gender differences in cognitive performance would be different in patients compared to healthy individuals, given the inconsistency of the relevant literature.
Methods
Participants
The experimental group consisted of 94 patients diagnosed with schizophrenia according to DSM-IV criteria [42]: 56 men (59.57%) and 38 women (40.43%). Diagnosis was confirmed with the Greek version (translation-adaptation to the Greek language by S. Beratis) of the Mini International Neuropsychiatric Interview (4.4) [43]. They had a mean age of 35.77 ± 10.01 years (range = 18–65 years) and a mean of 10.64 ± 3.29 years of education (range = 3–18 years). The control group consisted of 62 healthy adults, 31 men (50%) and 31 women (50%), with a mean age of 37.30 ± 13.82 years (range = 19–65 years) and a mean of 13.52 ± 4.03 years of education (range = 2–21 years).
We defined age at illness onset as the age at which the first psychotic episode occurred; thus, the mean duration of illness of schizophrenia patients was 9.53 ± 8.12 years (range=0.5–36 years). All of the patients were receiving antipsychotic medication and were clinically stable at the time of the study. Informed consent was obtained from all participants.
Symptom severity (positive symptoms, negative symptoms, and general psychopathology) of the schizophrenia patients was assessed using the Greek version [44] of the Positive and Negative Syndrome Scale (PANSS) [45]. Extrapyramidal symptoms were assessed with the Extrapyramidal Symptom Rating Scale (ESRS) [46].
Table 1 provides means and standard deviations for demographic and clinical characteristics of the research participants.
Subject characteristics
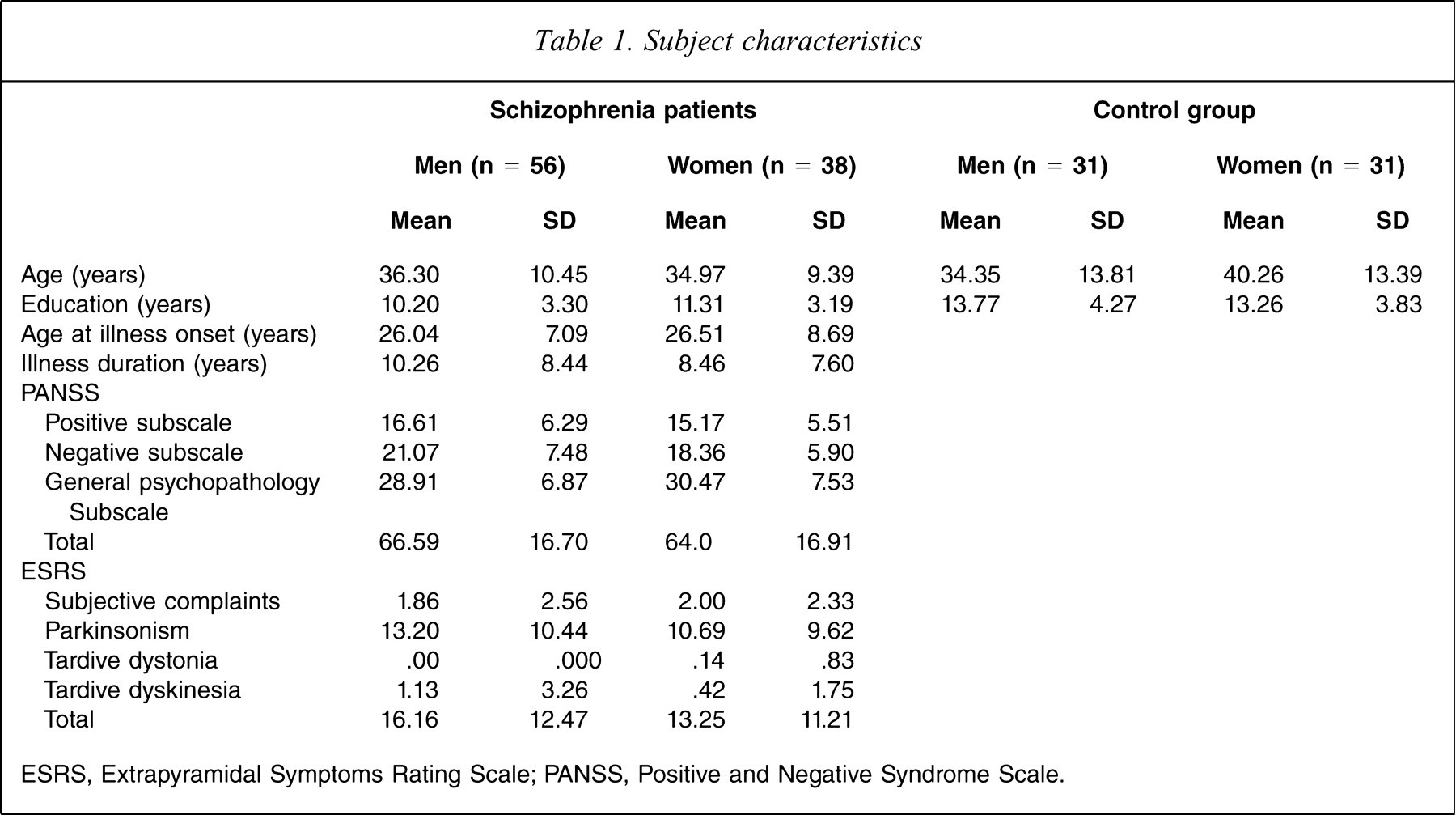
ESRS, Extrapyramidal Symptoms Rating Scale; PANSS, Positive and Negative Syndrome Scale.
Exclusion criteria were the following: non-native speakers of the Greek language, a history of neurological or developmental disorders, head injury with loss of consciousness, current substance abuse (in the last 6 months), as well as a medical disorder that may compromise cognitive performance. Additional exclusion criteria for the healthy participants were a personal or family history of a psychiatric disorder. All healthy participants were screened with a semi-structured interview by one of the experimenters (AP) before entering the study under the close supervision of the first and second authors (VPB, MHK).
Neuropsychological tests
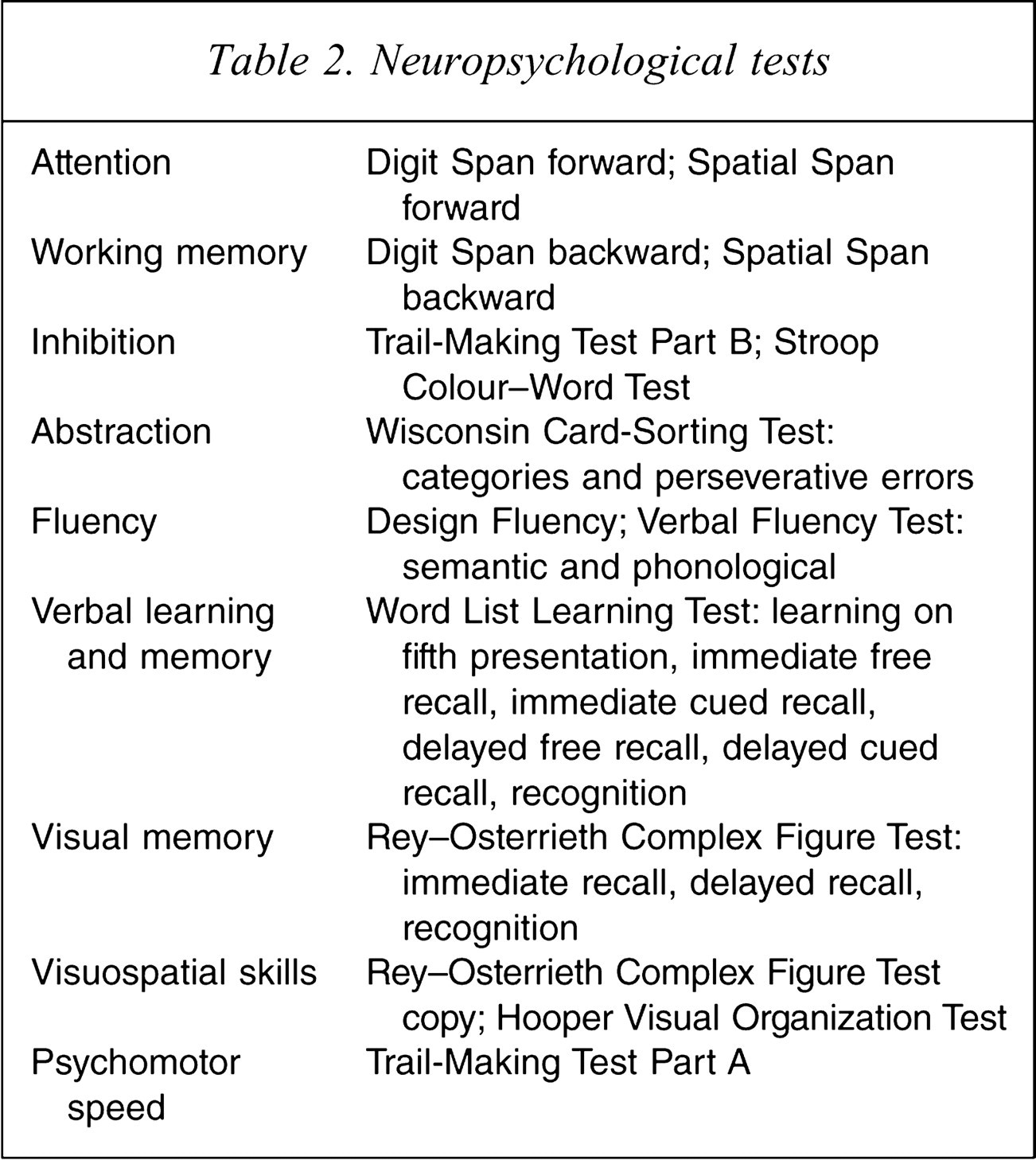
A battery of neuropsychological tests was administered to each participant in order to assess basic cognitive abilities: attention, working memory, abstraction, inhibition, fluency, verbal learning and memory, visual memory, visuospatial skills, and psychomotor speed. These tests were administered after the PANSS and ESRS and in a pseudo-randomized order, in order to avoid systematic effects attributable to fatigue or reluctance to continue. Administration of the complete neuropsychological battery lasted approximately 2 h and was carried out by trained psychologists. Table 2 lists the specific neuropsychological tests used for assessing each cognitive domain.
Neuropsychological tests
Attention
Auditory attention was assessed with the Digit Span forward, a subtest of the Wechsler Adult Intelligence Scale-III (WAIS-III) [47], and visual attention with the Spatial Span forward, a subtest of the Wechsler Memory Scale-III (WMS-III) [48]. Variables were the raw scores on each test.
Working memory
Verbal and visual working memory was measured with the WAIS-III Digit Span backward [47], and the WMS-III Spatial Span backward [48], respectively. Variables were the raw scores on each test.
Inhibition
Inhibition was assessed with the Stroop Word–Colour Test [49] according to Golden's administration [50] and the Trail-Making Test Part B [51] (for Greek norms, see [52]). The variable of interest on the Stroop Word–Colour Test was the number of incongruent colour words read, while the Trail-Making Test Part B was measured in terms of time to completion (in seconds).
Abstraction
Abstraction was measured with the Wisconsin Card-Sorting Test (WCST) [53]. Variables were the number of completed categories as well as the percentage of perseverative errors.
Fluency
Assessment of fluency included the Design Fluency Test [54] and the Greek Verbal Fluency Test [41]. The Design Fluency Test consisted of two parts. In the first one, examinees were asked to draw as many different abstract designs as possible within 5 min and in the second part, to produce as many different abstract designs as possible using four lines in 4 min. The score was the total number of acceptable designs in each condition. The Greek Verbal Fluency Test consisted of two parts: semantic and phonological. On the semantic part (categories), we asked participants to generate as many different animals, fruits and objects as possible, each in 60 s. On the phonological part (letters), we asked participants to generate as many words as possible beginning with the Greek letters χ (chi), σ (sigma), and α (alpha), each in 60 s, excluding proper nouns and variations of the same word. Variables included in the present analyses were the total numbers of words produced on the semantic and the total number of words produced on the phonological test.
Verbal learning and memory
Verbal learning and memory were measured with the Greek Word List Learning Test [55], based on the California Verbal Learning Test [56]. Variables included were: learning upon the last (fifth) presentation of the word list, immediate free and cued recall, delayed free and cued recall, and recognition.
Visual memory
The Rey–Osterrieth Complex Figure Test (ROFCT) [57] was used to assess visual memory: immediate and delayed recall and recognition. Drawings were scored based on the correctness and placement of each component of the figure drawn (Taylor scoring system).
Visuospatial skills
Visuospatial skills were measured with the ROFCT, copy condition [57], and the Hooper Visual Organization Test (HVOT) [58,59]. The latter requires mental rotation of fragmented drawings of common objects. On the ROFCT we scored the correctness and placement of each component of the figure copied, yielding an overall score; on the HVOT we calculated the number of correct responses.
Psychomotor speed
Speed of performance was assessed with the Trail-Making Test Part A, which is an index of visual scanning and psychomotor speed [51,52]. Time to completion (in seconds) was the variable of interest.
Statistical analyses
Analyses of variance, independent samples t-tests and χ2 tests were used to test for significant differences among the four groups (men with schizophrenia, women with schizophrenia, healthy men, healthy women) in demographic and clinical characteristics. Because the patient and control group were found to differ with respect to their level of education, this variable was used as a covariate in further analyses.
We calculated z scores for each neuropsychological test for the sample as a whole, so that higher z scores corresponded to better performance. We then calculated the average of all tests in each cognitive domain: attention, working memory, abstraction, inhibition, fluency, verbal learning and memory, visual memory, visuospatial skills, and psychomotor speed. Internal consistency reliability of this grouping was tested by calculating Cronbach's alpha coefficient separately for the patient and the control groups. Table 3 shows the Cronbach's alpha internal consistency reliability coefficients for each grouping of separate tests into cognitive domains, calculated separately for the patient group and the control group. In general, internal consistency reliabilities were very good. The somewhat lower reliabilities for visuospatial skills, inhibition and visual memory were probably due to the use of only two or three tests in these domains.
Cronbach's alpha internal consistency reliability coefficients
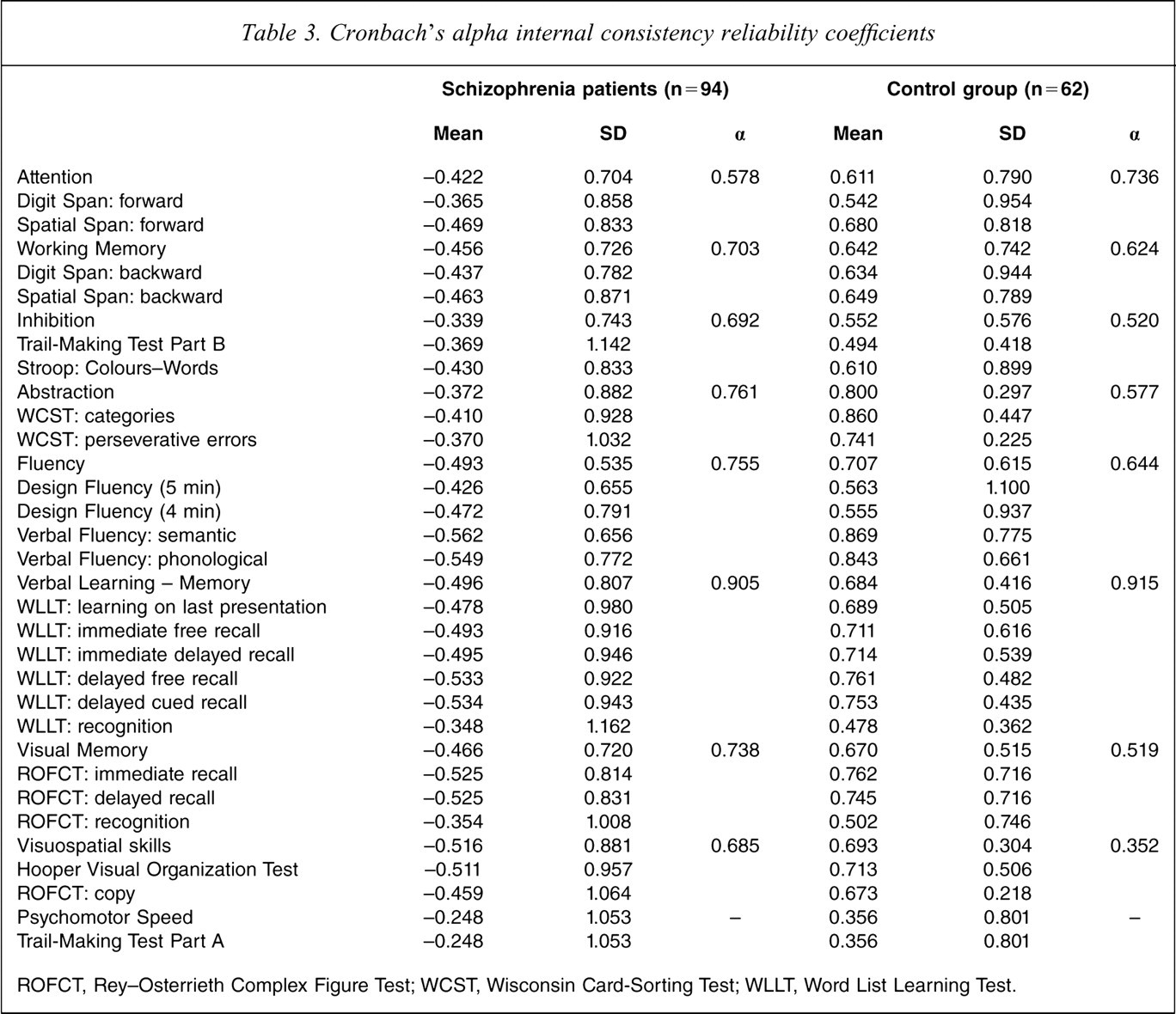
ROFCT, Rey-Osterrieth Complex Figure Test; WCST, Wisconsin Card-Sorting Test; WLLT, Word List Learning Test.
Main effects of group and sex, as well as group × sex interactions on each cognitive domain, were tested using a 2 (group: patients and controls) × 2 (sex: male and female) multivariate analysis of covariance, with sex and group as the between-subjects factors, score in each cognitive domain as the within-subject factor, and years of education of the participants as a covariate. Eventual significant effects were followed up with separate ANOVAs for each cognitive domain. Due to the large number of dependent variables tested, we applied the Bonferroni correction procedure (dividing the alpha level by the number of depended variables: 0.05/9 = 0.006) in order to make our criterion of significance more conservative.
Results
Group and sex comparisons on demographic and clinical characteristics
There was no group difference on age (F(3,152)=1.66, p > 0.05), but the groups differed in their level of education (F(3,151) = 8.74, p < 0.001). Post-hoc comparisons showed that healthy men had a mean of 3.68 years of education more than men with schizophrenia (p < 0.001) and a mean of >2.46 years of education more than women with schizophrenia (p < 0.033). Similarly, healthy women had a mean of 3.06 years of education more than men with schizophrenia (p < 0.001), but did not differ from women with schizophrenia.
The male: female ratio was similar in both the patient and the control groups (χ2 (1) = 1.39, p > 0.05). Moreover, male and female schizophrenia patients did not differ in terms of their age at illness onset (t(92)=-0.287, p > 0.05), illness duration (t(92) = 1.06, p > 0.05), PANSS subscale scores of positive symptoms (t(90) = 1.124, p > 0.05), negative symptoms (t(90)= 1.837, p > 0.05), and general psychopathology (t(90)=−1.03, p > 0.05), as well as on ESRS subscale scores of subjective complaints (t(90)=-0.27, p > 0.05), Parkinsonism (t(90) = 1.16, p > 0.05), tardive dystonia (t(90)=-1.25, p > 0.05) and tardive dyskinesia (t(90) = 1.20, p > 0.05).
Missing data
Of the 94 schizophrenia patients, 89 had complete data sets for attention, 85 for working memory, 89 for psychomotor speed, 83 for visuospatial ability, 88 for visual memory, 71 for fluency, 81 for inhibition, 84 for verbal memory, and 84 for abstraction. All healthy comparison participants completed all measures of working memory, psychomotor speed, visuospatial ability, visual memory, fluency, and inhibition, while 40 had completed all measures for abstraction and 61 for verbal memory. Despite the exclusion of some subjects due to missing data for each cognitive domain, the equivalence of the male–female ratio of the groups was preserved, as confirmed by χ2 tests run for each cognitive domain separately. Also, separate group comparisons of patient and control demographic and clinical characteristics showed that, despite the exclusion of some subjects due to missing data, the groups’ equivalence on these variables was also preserved.
Group and sex effects and their interaction across cognitive functions
There were significant effects both for group (F(9,86) = 15.31, p < 0.001), and sex (F(9,86) = 3.24, p = 0.002), but the two factors did not significantly interact with each other (F(9,86) = 1.45, p = 0.18). Therefore, although follow-up ANOVAs were conducted for all main effects and their interactions, the results were taken in the account only for group and sex effects (Table 4; Figure 1).
Standardized scores for cognitive performance vs presence of schizophrenia and gender
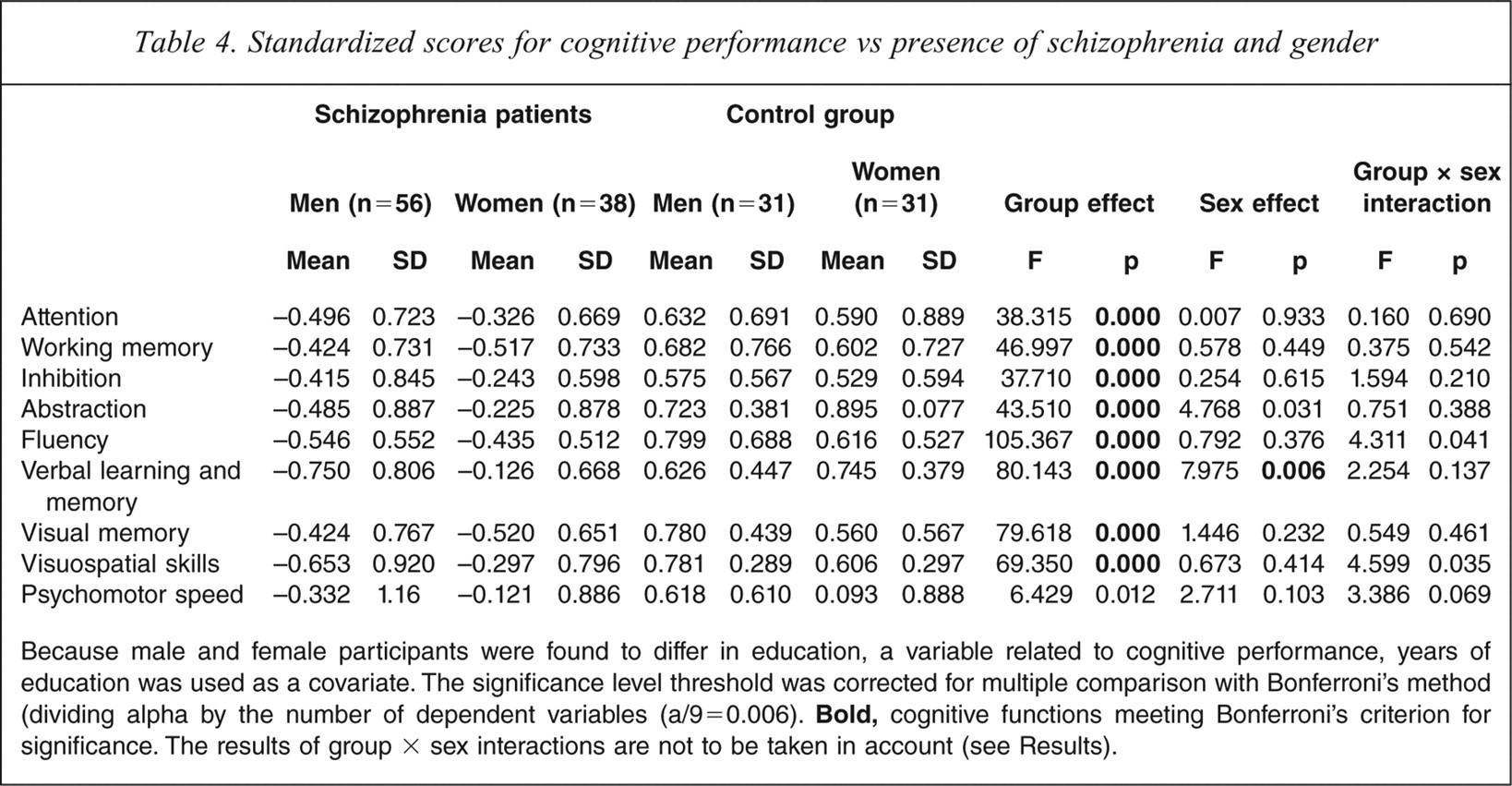
Because male and female participants were found to differ in education, a variable related to cognitive performance, years of education was used as a covariate. The significance level threshold was corrected for multiple comparison with Bonferroni's method (dividing alpha by the number of dependent variables (a/9=0.006).
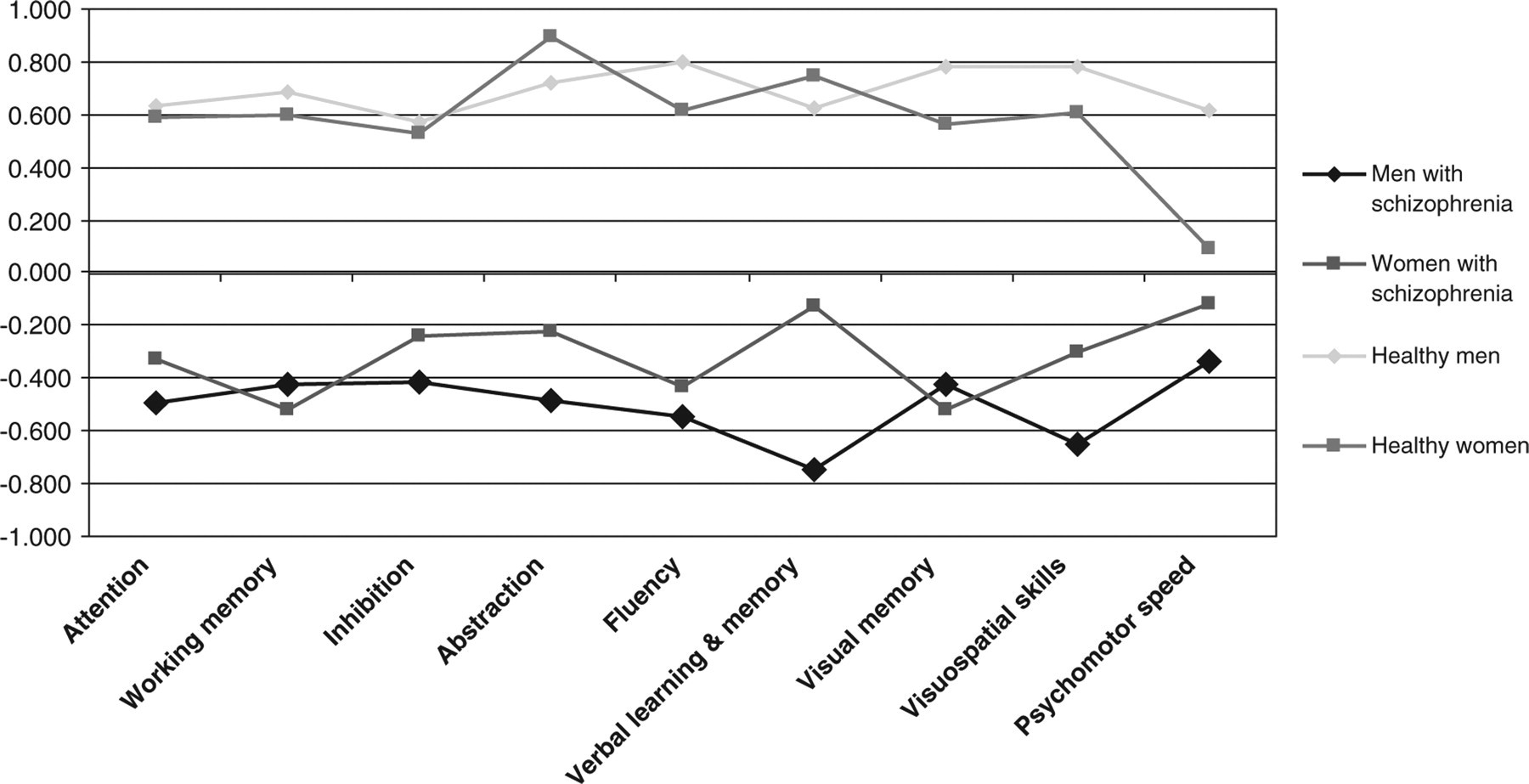
Mean z scores for cognitive performance of male and female schizophrenia patients and healthy comparisons.
With the exception of psychomotor speed (p = 0.012), all cognitive functions showed a group effect (every p < 0.001), wherein schizophrenia patients performed more poorly than healthy controls. Moreover, analysis of covariance with group (schizophrenia patients, healthy comparisons) as the between-subjects factor and education as a covariate on the z scores for each test separately indicated a statistically significant group effect for every analysis, wherein healthy controls outperformed schizophrenia patients in virtually every neuropsycho-logical test (every p < 0.05). The effect of sex was significant, after Bonferroni corrections, only for verbal learning and memory (F(1,94) = 7.98, p = 0.006), in which women outperformed men, confirming in part our initial hypothesis.
Discussion
Schizophrenia patients as a group were significantly impaired in comparison to healthy controls in each of the cognitive domains assessed, with the exception of psychomotor speed. This finding is in accordance with numerous previous studies [12,18,23,60–62] and supports the assumption of a global and generalized cognitive impairment in schizophrenia.
As regards the main question of the present study, that is, whether schizophrenia affects the cognitive functioning of both male and female patients to the same extent, the picture was clear. In no cognitive function did we find an interaction of group and sex; in other words, the advantage for women in general on verbal learning and memory compared to men was also observed in the group of schizophrenia patients. These findings are consistent with a number of similar studies supporting a lack of difference between men and women with schizophrenia in the severity of cognitive impairment. More specifically, previous studies have reported that the typically observed pattern of differential cognitive performance among healthy men and women is preserved in schizophrenia patients in a great variety of cognitive tasks [18,19,22]. Sota and Heinrichs investigated verbal learning and memory in 106 schizophrenia patients using the California Verbal Learning Test [14,56]. They found that, similarly to the normal population, female schizophrenia patients outperformed male patients both on verbal learning and on delayed free recall. Moreover, these authors calculated an index for the retention of learned verbal material, adjusted for the total number of words learned over the five learning trials. This retention rate index was calculated by multiplying by 100 the ratio of the total number of correctly recalled words in the delayed free recall condition to the total number of correctly recalled words on the fifth learning trial. They found that male and female schizophrenia patients presented the same retention rates of learned material. In order to test this finding, we calculated the same index based on data obtained in the present study. In accordance with the aforementioned study, we found that retention rate was influenced neither by group (F(1,142) = 0.291, p > 0.05) nor by sex (F(1,142) = 0.319, p > 0.05), nor was there a group × sex interaction (F(1,142) = 0.315, p > 0.05). Although schizophrenia patients learned fewer words over the five learning trials, they appeared to have retained the material learned as well as healthy controls, up to 20 min later.
Despite the consistency of the present findings with many previous investigations, they are in contrast to the findings of others. The limited scope of the present sex differences is in contrast to studies in which female schizophrenia patients outperformed their male cohorts in several cognitive domains, namely, attention, verbal memory and executive functions [12,13,15]. The present findings are also inconsistent with reports in which men with schizophrenia outperformed their female cohorts on tasks of verbal and visual memory, attention and visual perception [17,23].
In an effort to clarify the causes of this discordance, a number of considerations may be formulated regarding the aforementioned studies, in particular their methodological design and the interpretation of their findings. More specifically, some of the aforementioned studies included small samples [12,13,15]. For example, Fiszdon et al. assessed only 28 schizophrenia patients with the California Verbal Learning Test, while they did not include a control group; thus, it is very likely that their finding, that women outperformed men with schizophrenia, in reality reflects the advantage for women in such tasks also observed in the normal population [13]. The findings reported by Goldstein et al. were also based on a small sample (n = 31) of schizophrenia patients; these investigators did not control for differences in educational level [12]. The findings of Seidman et al. were derived from a small sample of 40 schizophrenia patients, and referred only to the WCST [15]. In contrast, the study by Lewine et al. included an impressively large sample of 195 schizophrenia patients [23], but although their patient group consisted predominantly of men (68%), the respective ratio of men in their control group was considerable smaller (40%). Finally, the study by Goldberg et al., which included a very large sample schizophrenia patients (n = 268), included almost twice as many men than women; moreover, it did not include a control group, thus making it impossible to conclude whether the differences found in favour of male patients in visuospatial and attentional tasks reflected differences observed between the two sexes in the healthy population [17].
Potential reasons for the more favourable course of schizophrenia in women (evidenced by older age at onset of the illness, greater level of premorbid functioning, more benign symptomatology and better outcome than in men) [2] should be sought for in other cognitive factors. Gender-specific deficits on affect recognition have been found in schizophrenia patients. In several previous studies only male patients presented significant impairment on recognition of affective prosody [63,64] and facial affect [65,66]. This is a very interesting finding given the importance of emotion processing in different aspects of social functioning in schizophrenia [67–71]. Moreover, there is evidence that facial affect recognition may be a partial mediator at baseline examination, and a potential mediator after 1 year, between basic cognitive and social functioning in schizophrenia patients [71]. Moreover, the better social outcome of women compared to men with schizophrenia may be accounted for by other factors, such as the higher level of social development at illness onset, better cooperativeness and compliance in women, or socially adverse illness behaviour in men [2].
In conclusion, the present results indicate, in accordance with previous studies, that the degree of cognitive impairment is the same for male and female patients with early onset schizophrenia. The sex differences found among patients were similar to those of the healthy population examined in the present study. Therefore, differential decrements in basic cognitive domains do not appear to account for the more favourable course of schizophrenia in women relative to men, and, thus, do not offer much in terms of elucidating the underlying pathophysiological mechanisms of impaired community functioning in these patients. Potential reasons for the more favourable course of female schizophrenia patients should be sought for in other factors, that is, affect recognition.
Footnotes
Acknowledgements
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.