
Abstract
Aim: We review the research literature examining neuropsychological performance in migraine. Findings were organized by neuropsychological construct assessed and results were reported using effect size conventions. Factors considered in explaining results included sample characteristics, migraine factors, and control for non-migraine variables.
Findings: There is weak evidence for deficits in processing speed, attention, verbal memory, verbal skills, working memory, sustained attention, and inhibition in migraine relative to healthy controls. There are mixed results regarding deficits in visual memory, motor dexterity, visuospatial/constructional skills, visual reasoning, and mental flexibility in migraine relative to healthy controls. Mixed findings do not seem to be consistently related to study characteristics or presence of aura; other important migraine factors (such as migraine severity or presence of neuroradiological findings) remain understudied. Relative to non-healthy control groups, however, there is weak evidence for an effect of migraine in any cognitive domain. Longitudinal studies provide little evidence that neuropsychological functioning worsens over time in migraine or that migraine is a risk factor for Alzheimer’s disease.
Research implications: It remains possible that cognitive dysfunction is seen in only a subset of migraine sufferers, perhaps those with more severe illness or neurological involvement; however, more research is needed to examine this issue. Non-migraine differences among migraine sufferers, including medical and psychiatric comorbidities and variables associated with treatment seeking, may partially account for inconsistent findings and should be evaluated for in future research.
Clinical implications: Clinicians should refer migraine patients for comprehensive neuropsychological evaluation only when there is sufficient evidence for concern. Such evaluations should include consideration of other psychological, neurological, and medical contributors to both migraine and cognitive status.
Patient awareness of increased risk for brain events in migraine, coupled with their own sense of cognitive changes during migraine attacks, may increase requests for neuropsychological testing from migraine patients. Common conceptualizations of migraine continue to emphasize its relatively benign long-term neurological consequences (1). However, some researchers have suggested that recent neuroimaging findings represent underlying progressive neurological consequences of migraine (2–6). Although mild transient cognitive complaints and impairments are to be expected in the context of the active presence of severe pain during a migraine attack and in the immediate neurological consequences of a migraine attack (7–10), some migraine patients also complain of cognitive impairments outside of the migraine attack (11–15). In fact, in one study, more than half of migraine patients reported impaired daily functioning and cognitive symptoms (16). However, cognitive complaints are not specific to one type of headache and are ubiquitous across many medical and psychiatric conditions that commonly co-occur with migraine (17,18). Thus, a better understanding of the specific relationship of migraine to cognitive impairment is needed. Below we critically review evidence for interictal cognitive impairment in migraine, providing general effect size data across cognitive constructs commonly assessed in migraine. Consideration is given to migraine and non-migraine factors that may account for findings, as well as comparisons with appropriate control groups. Finally, we consider implications for future research and clinical practice.
Review of neuropsychological findings by cognitive domain methods
Characteristics of studies included in the review


Processing speed
Effect of migraine on processing speed

Cohen’s effect size conventions (trivial d = 0–0.19, small d = 0.20–0.49, medium d = 0.50–0.79, large d ≥ 0.80 (19)) were used to describe the general size of the effect of migraine.
Basic attention
Effect of migraine on attention

Cohen’s effect size conventions (trivial d = 0–0.19, small d = 0.20–0.49, medium d = 0.50–0.79, large d ≥ 0.80 (19)) were used to describe the general size of the effect of migraine.
Memory
Effect of migraine on verbal memory

Cohen’s effect size conventions (trivial d = 0–0.19, small d = 0.20–0.49, medium d = 0.50–0.79, large d ≥ 0.80 (19)) were used to describe the general size of the effect of migraine.
Effect of migraine on nonverbal memory

Cohen’s effect size conventions (trivial d = 0–0.19, small d = 0.20–0.49, medium d = 0.50–0.79, large d ≥ 0.80 (19)) were used to describe the general size of the effect of migraine.
In the nonverbal memory domain, findings were much less consistent. Although several studies found small to medium effects of migraine on immediate figure recall tasks (11,24–26,32), some studies found no effects or even findings in the opposite direction (i.e. migraine patients performed better (11,22,25,30). This general pattern was also seen in delayed figure recall, with effects in the medium to large range in several studies (24–26,32), but with some exceptions (11,30). Aura was not related to the size of the effect on either immediate or delayed recall tasks (24–26,30). No clear pattern of study characteristics explained inconsistencies in nonverbal memory findings. Relative to non-healthy controls, migraine had no negative effect on nonverbal memory; in fact, migraine patients performed better than individuals with mild traumatic brain injury (12,22,30). On other visual memory and visual/verbal memory tasks, the effect of migraine tended to be trivial to small (20,25,26,30,32,33), with only rare exceptions seen in older studies (14,26).
Verbal skills
Effect of migraine on verbal skills
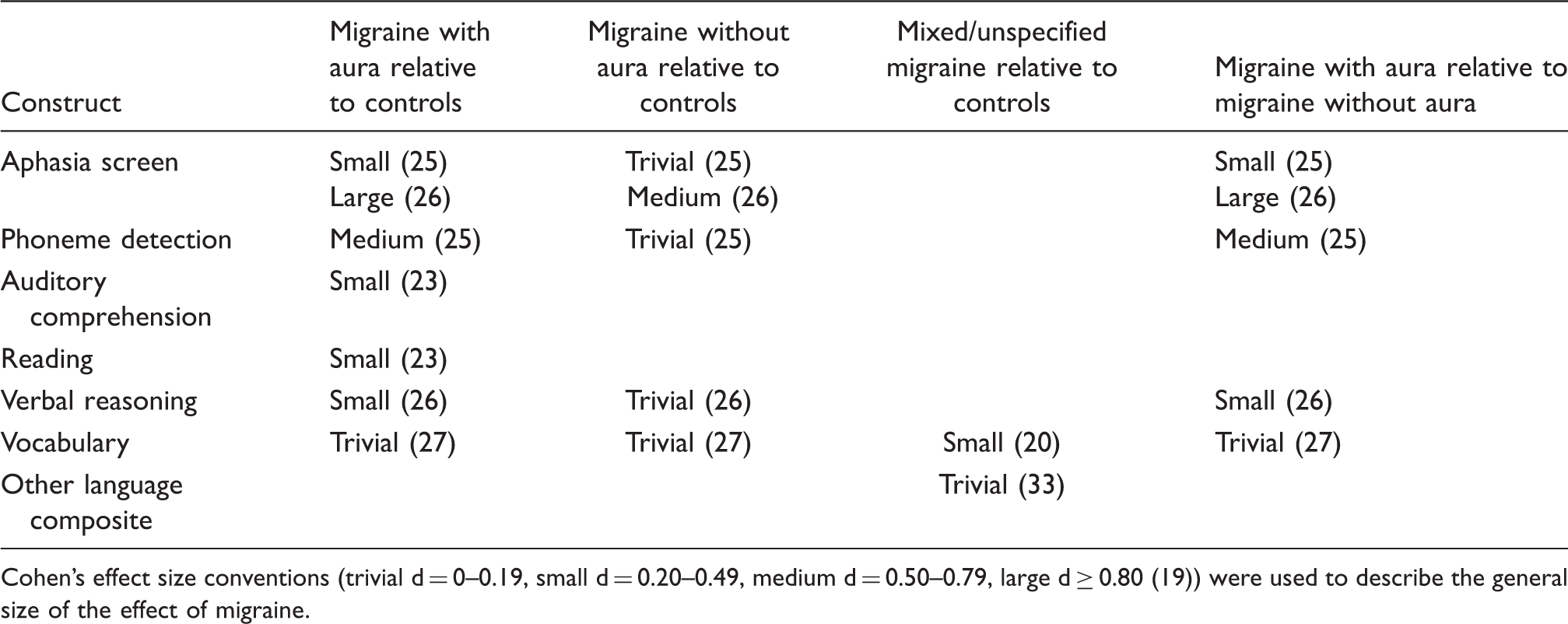
Cohen’s effect size conventions (trivial d = 0–0.19, small d = 0.20–0.49, medium d = 0.50–0.79, large d ≥ 0.80 (19)) were used to describe the general size of the effect of migraine.
Nonverbal skills
Effect of migraine on nonverbal tests

Cohen’s effect size conventions (trivial d = 0–0.19, small d = 0.20–0.49, medium d = 0.50–0.79, large d ≥ 0.80 (19)) were used to describe the general size of the effect of migraine.
Executive functioning
Effect of migraine on executive functioning measures

Cohen’s effect size conventions (trivial d = 0–0.19, small d = 0.20–0.49, medium d = 0.50–0.79, large d ≥ 0.80 (19)) were used to describe the general size of the effect of migraine.
Longitudinal findings
If migraine is a neurodegenerative disorder, successive migraine attacks should collectively contribute to increased cognitive impairment or the development of dementia over time. Four population-based longitudinal studies have addressed this question. One of these studies used diagnosis of Alzheimer’s disease as the outcome variable. Tyas and colleagues examined 694 cognitively intact adults, 36 of whom went onto develop Alzheimer’s disease within 5 years (40). History of migraine was a risk factor for developing Alzheimer’s disease (RR = 3.5, 95% CI = 1.39–8.77). Three additional longitudinal studies used changes in neuropsychological test performance over time as an outcome variable, rather than diagnostic status. Baars and colleagues examined 99 migraine sufferers and 1,724 healthy controls over 6 years and found no evidence for cognitive decline in migraine sufferers relative to healthy controls on measures of mental status, verbal memory, working memory, and divided attention (28). Kalaydjian and colleagues examined 204 migraine sufferers and 1,244 healthy controls over 9 years (34). Migraine sufferers performed more poorly on measures of verbal memory at the first evaluation, but their performance actually declined less over time than healthy controls; these effects were more pronounced in migraine sufferers with aura (34). A recent report using data from the Epidemiology of Vascular Ageing study further confirmed no evidence of cognitive decline across multiple cognitive domains, including general mental status, processing speed, verbal and visual memory, and visual reasoning, with the exception of only one processing speed task, for which there was actually evidence of less decline over time in migraine than in healthy controls and non-migraine headache (22). Finally, although cross-sectional in nature, two additional studies suggest that migraine status is not related to cognitive decline or dementia. In a review of eight case-control studies examining medical factors related to Alzheimer’s disease risk, history of severe headaches and migraine was related to lower risk of Alzheimer’s disease, (RR = 0.7, 95% CI = 0.5–1.0) (41). In another study, migraine patients were divided into younger (below 40) and older (above 40) participants; in those under 40, migraine sufferers performed more poorly on motor speed relative to healthy controls, while there was no migraine effect in those above 40 (35). Thus, overall, there is not consistent and convincing evidence that neuropsychological functioning worsens over time in migraine.
Relationship of migraine factors to neuropsychological findings
In total, findings regarding neuropsychological dysfunction in migraine suggest small to trivial effects (processing speed, attention, verbal memory, verbal skills, working memory, sustained attention, inhibition) or highly inconsistent effects (visual memory, motor dexterity, visuospatial/constructional skills, visual reasoning, mental flexibility). It is possible that the inconsistent findings are related to migraine factors, such as presence/absence of aura, severity of migraines, or presence/absence of neuroradiological findings, to name a few. However, migraine factors, with the exception of aura, have been examined in only a few studies, all of which were cross-sectional in nature. As reviewed in Tables 2–7, aura status is not consistently associated with cognitive impairment in migraine. Duration of illness has not been significantly related to processing speed, attention, verbal or visual memory, nonverbal skills, or executive functioning (11,14,21), with the exception of isolated findings (11). With regard to frequency of migraine attacks, results are more mixed. In the domain of processing speed, two studies reported no effect of frequency (14,21), whereas two studies showed a medium to large effect of frequency (11,24). In the attention domain, two studies showed no relationship of migraine frequency to performance (11,21), whereas one study found large effects, especially in individuals with frequent migraine with aura (24). In the domain of memory, two studies found no effect of frequency (14,21), while two studies found medium to large effects on some memory measures (11,24). With regard to nonverbal skills, small to medium effects of migraine frequency have been identified in two studies (11,24). Studies have consistently shown no effect of migraine frequency on executive functioning measures (11,14,24). When isolated effects of migraine frequency or duration were identified, they were seen primarily in two clinic-based studies with larger sample sizes (11,24), whereas insignificant findings were typically from a large population-based study and an older study with a small sample size (14,21).
Studies in the neuropsychological literature have largely ignored the potential influence of genetic factors such as CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) and family hemiplegic migraine, which may themselves lead to higher risk for cognitive impairment (42). Another possibility is that cognitive dysfunction in migraine is seen only in the presence of neurological changes observed in a subgroup of patients. White matter abnormalities are found in 6–47% of migraine patients (2,43), and evidence of ischemic infarct is seen in 8–31% of migraine patients (44,45). However, these neurological findings are not unique to migraine, but are also seen in 21–40% of individuals with other types of headaches (4,22,46), are highly likely in the presence of various cardiovascular risk factors (47,48), and are common in normal aging (49). Very few migraine studies to date have included assessment of both neurological and neuropsychological variables. One clinic-based study assessed both interictal neuropsychological performance and cerebral perfusion with SPECT in patients with migraine relative to healthy controls. SPECT hypoperfusion was seen in 13% (n = 2) of controls and 43% of migraine patients (n = 25, 6 with aura), which was sometimes localized but sometimes suggestive of a multi-ischemic process. Migraine sufferers with abnormal SPECT had longer disease duration. Notably, no differences in neuropsychological test scores were detected between migraine sufferers with normal and abnormal SPECT, and only one isolated memory test score distinguished migraine sufferers with abnormal SPECT from healthy controls. In another clinic-based study that included both neuroradiological data and neuropsychological tests (38), females with migraine showed decreased gray matter density, particularly in the middle frontal gyrus, compared with healthy controls, and performed worse on one of three executive function measures that emphasize speeded set shifting and inhibition skills. Gray matter density correlated with slower response time on that one task, but not with the other executive function tasks. In a recent population-based study (50), there was no association between the presence of white matter hyperintensities and functioning in multiple neuropsychological domains, including processing speed, verbal and visual memory, visual reasoning, and mental flexibility tasks, as well a general mental status measure. Finally, the presence of white matter hyperintensities or cerebral infarct did not modify the relationship between migraine and cognitive decline over time in a recent report using data from the Epidemiology of Vascular Ageing study (22).
Few studies to date have examined the relationship of migraine factors, such as frequency, duration, genetic vulnerability, and presence of neuroradiological abnormalities, to neuropsychological findings or risk of cognitive decline over time. Thus few definitive conclusions can be drawn about the contribution of migraine-specific factors to neuropsychological impairment.
Importance of non-migraine variables to interpretation of neuropsychological findings
In addition to migraine-related factors, it is possible that non-migraine differences among migraine patients, such as gender, presence of comorbid medical and psychological illness, use of medication, or factors associated with treatment seeking, contribute to the inconsistent findings across the reviewed studies, given the wide variability in assessment for and control of such factors in the existing literature.
Many, but not all, neuropsychological studies reviewed above excluded participants with cardiovascular disease, clinical stroke, diabetes, hypertension, traumatic brain injury, psychiatric disorders, and/or other ‘systemic diseases’. Results were mixed across studies that did attempt to control for these medical factors. However, of studies that did not control for medical factors, most detected cognitive differences between migraine sufferers and healthy controls (9,11,14,32,35,39), suggesting that these factors may account for at least some of the findings. Many of these factors complicate interpretation of neuropsychological findings in headache; it is conceivable that 1) migraine raises the risk for the medical condition, which is then related to cognitive impairment, 2) the medical condition raises the risk for migraine, which is then related to cognitive impairment, or 3) the medical condition directly increases the risks of both migraine and cognitive impairment.
Certain medications used to treat migraines could also influence cognitive functioning. Several studies excluded migraine sufferers using any type of prophylactic medication (9,11,30,37,51), with mixed results on neuropsychological variables. Studies that specifically tested the effects of prophylactic and acute medication (primarily ergotamine) on cognitive functioning did not find any significant effect of medication on cognitive functioning (14,24,26,28). In one study, migraine patients with medication overuse were more impaired on executive function measures relative to episodic migraine patients and healthy controls, but they also had more chronic illness and more depression and anxiety (36).
The presence of depression may have a negative impact on performance on neuropsychological tests (52,53). The prevalence of depression in migraine patients tends to be higher than expected (54–57), especially in migraine with aura (57–59). However, high rates of depression are also seen in non-migraine headache (17,58,60). Three epidemiological studies examining the impact of migraine on cognitive functioning controlled for depression (21,34). Gaist and colleagues found that the presence of depression (combined with several other potential covariates), attenuated the effects of migraine on cognitive functioning (21). However, Kalaydjian and colleagues found that a lifetime history of depression had no significant relationship to cognitive functioning (34). In a recent report using data from the Epidemiology of Vascular Ageing study, depression did not interact with migraine status in explaining cognitive decline over time (22). A single clinical study found no significant differences in executive functioning between migraine sufferers diagnosed with depression or obsessive-compulsive personality disorder and those without psychiatric disorders (39).
Another important consideration is the source of the migraine sample being studied. Population-based studies generally found that adult migraine sufferers did not perform neuropsychological tasks more poorly than healthy controls (21,22,27–29,34). A number of characteristics probably distinguish migraine sufferers presenting in clinics from migraine sufferers in the general population, such as more frequent and severe migraines, higher rates of migraine-related disability, and presence of comorbid illness, which may be associated with cognitive impairment. In addition, given that the above review suggests little if any migraine-specific cognitive impairment relative to non-healthy control groups (12,30,31,35,37), it is possible that general treatment-seeking variables account for inconsistent findings of cognitive dysfunction in migraine.
Another non-migraine factor related to treatment-seeking and not controlled for in the existing literature is non-credible performance. Non-credible performance can be seen not only in symptom reporting (when patients exaggerate or simulate symptoms of a disorder), but also in behavior (when undergoing a pressure pain threshold task, or when asked to recall a list of words). At times, non-credible performance can be judged to be deliberate, intentional, and for the purposes of obtaining secondary gain (malingering), whereas at other times, the motivation for non-credible responding is less clear (61). Regardless of motivation, non-credible responding can severely limit interpretation of neuropsychological results (concluding that the poor test scores indicate impairment rather than being invalid to interpret); therefore appropriate practice requires assessment for non-credible performance (62). Rates of non-credible performance on cognitive tasks are estimated to be relatively high in pain populations, particularly in clinical settings and when evaluations are conducted for medicolegal purposes (63). Although the studies reviewed above excluded patients who experienced posttraumatic headache, in which there is a higher likelihood of treatment seeking and compensation seeking and thus an increased possibility of non-credible performance, there is ample evidence that non-credible effort can contribute to misinterpretation of neuropsychological performance in several medical conditions, including pain, outside of the context of litigation (61).
Given the importance of these non-neurological factors to neuropsychological test interpretation, future studies examining the neuropsychological consequences of migraine should use non-healthy control groups, assess for and consider the impact of comorbid medical, neurological, and psychiatric conditions and medication use, and include well-validated measures of non-credible responding to address potential treatment and compensation seeking in their participants.
Conclusions
In general, evidence for neuropsychological impairment in migraine is weak. Evidence suggests that migraine has a trivial effect in the cognitive domains of processing speed, attention, verbal learning and recall, working memory, sustained attention, and inhibition relative to healthy controls. There is inconsistent evidence of possible effect of migraine in the cognitive domains of visual memory, motor dexterity, visuospatial/constructional skills and visual reasoning, and mental flexibility relative to healthy controls. There is no evidence of a migraine effect in any cognitive domain in comparison with non-healthy control groups. There is no clear evidence that either migraine or non-migraine characteristics are associated in any consistent manner with the neuropsychological findings reviewed above. However, the contribution of both migraine and non-migraine characteristics remains woefully understudied. Further research is required to examine the relationship of such characteristics to cognitive performance in migraine.
Implications for future research
Although existing data suggest trivial or inconsistent findings when comparing the average performance of a group of migraine patients with the average performance of healthy controls, the only question answered is whether, on average, the entire group of migraine patients performed relatively differently than the average of the control sample. The question of whether there is a subset of migraine patients who have clinically impaired cognitive performance cannot be answered by such methodology. In fact, one possible explanation for the inconsistent findings is that clinically relevant cognitive impairment might be seen in only a subset of migraine patients, such as those with more severe illness, those with structural brain changes, those with medical or psychiatric comorbidities, or those who are performing non-credibly. In other words, it is possible that the presence of a few individuals with clinically impaired scores can drive the overall group average of a migraine sample; the percentage of such individuals in any given study would determine how much influence their impaired scores have on the overall group mean. Of the studies reviewed, only one (12) considered the clinical significance of neuropsychological findings, by using well-validated measures with large normative datasets and examining whether each participant’s scores would have been considered clinically impaired based on those population norms. In that study, 10% of the migraine patients met their definition of clinical impairment, compared with 15% of chronic pain patients and 40% of mild traumatic brain injury patients. Future studies should consider using well-standardized and normed neuropsychological tasks to assess cognitive performance and should report their findings not only in terms of group averages, but also in terms of percentages of patients who are clinically impaired in cognitive performance relative to well-established norms for the measure. Such data might help to determine how ‘common’ neuropsychological impairment in migraine is and to identify which migraine or non-migraine factors, if any, are specifically associated with the presence of clinical impairment.
Although population-based longitudinal studies are ideal to address the question of whether all migraine disorders lead to cognitive impairment, typically such designs are limited by the amount of data that can be collected on any given participant to make the study feasible. For example, thorough neuropsychological evaluation with sensitive measures cannot be accomplished with use of brief cognitive screening tools such as the Mini-Mental Status Exam. Furthermore, assessment of both migraine and non-migraine factors that might contribute to findings is, of necessity, more limited in such designs. Clinic-based prospective studies may be better equipped to examine subsets within the population of migraine sufferers who may be at higher risk for cognitive impairment. The question that such studies would answer is not ‘does migraine cause cognitive impairment’ but rather ‘are there migraine or non-migraine factors that are related to a higher risk of cognitive impairment in those seeking treatment for migraine?’ Such studies should include: 1) careful attention to migraine diagnosis at baseline, 2) baseline imaging data, 3) baseline neuropsychological data (including assessment for non-credible performance), 4) careful clinical interview and review of medical records for baseline confounding psychological and medical conditions, 5) use of non-healthy clinical control groups to control for non-migraine factors that might affect cognitive performance, and 6) regular follow-up that includes re-assessment of migraine status, repeat imaging and neuropsychological re-evaluation, re-assessment of medical and psychological issues, and more careful and regular assessment of migraine frequency, severity, presence of aura, and use of medications. It is only through careful, well-planned prospective studies that the nature of neuropsychological changes in migraine can be truly understood.
Clinical implications
Consensus guidelines from the American Academy of Neurology and the US Headache Consortium (64) suggest that neuroimaging is not generally warranted in migraine evaluations, unless the patient has atypical symptoms, an abnormal neurological examination, recent change in the pattern of their headaches, or other risk factors for neurological events. Similarly, our review suggests that routine neuropsychological assessment is probably not warranted in migraine, unless patients have either self-reported or observed declines in cognitive or behavioral functioning that strongly suggest neurological involvement. It is important to note that self-reported cognitive changes are unlikely to be accurate, and thus any concern expressed by a migraine patient that their cognitive functioning is impaired should be followed by neuropsychological evaluation rather than an assumption that the patient’s self-report is valid. Furthermore, simple mental status evaluation or cognitive screening is unlikely to be sensitive enough to the cognitive domains of concern, and thus the evaluation should include neuropsychological measures of known sensitivity and that have adequate normative data to address gender, education, and age effects on cognitive functioning. Should neuroimaging data be available, the neuropsychological evaluation should carefully address any areas of cognitive functioning that might be suggested by structural or functional neuroimaging findings. In addition, consideration of ‘third-variable’ explanations, including depression, treatment-seeking, diminished effort/non-credible performance, and presence of neurovascular or other health conditions that can have an impact on cognition, would need to be considered, to rule out other explanations for any self-reported or observed cognitive decline.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interests
The authors declare that there is no conflict of interest.