
Abstract
Most research on incidence and age at onset of first-episode psychosis involved schizophrenia spectrum disorders in urban or mixed urban–rural samples [1,2]. The results indicated a higher incidence in male subjects [3,4], who also tend to have earlier age at onset than female subjects [5]. Most studies, however, have examined treated incidences and excluded older subjects [1,2]. Thus, most studies may not represent the diversity of psychotic presentations in the general population, and the studies may be subject to selection bias due to socioeconomic characteristics, ethnicity and substance use in the patients studied. Moreover, the findings are not consistent; some studies have found similar incidence and age at onset in male and female subjects, and some have found higher incidence and earlier age at onset in female subjects [4–8]. For affective and other psychoses – and for psychoses with late onset – the findings are less clear [2,6,9]. Nevertheless, most studies have reported similar male/female incidence rates of bipolar disorder [10].
The Lundby population is a complete population that was followed from 1947 to 1997 [11]. All subjects with psychotic disorders have been described, giving us the opportunity to report the epidemiology of all psychoses in the Lundby population.
The aims were to quantify and compare male and female first occurrences of different psychoses according to DSM-IV in terms of age at onset, overall incidence of first episodes and age-specific incidence.
Methods
Population
The Lundby area is located in the south of Sweden. On 1 July 1947 and 1 July 1957 everybody on the parish registers was enrolled in a longitudinal study of mental health (n = 3563; male, n = 1823; female, n = 1740; Tables 1, 2). There have been four waves of field work: 1947, 1957, 1972 and 1997. At the follow ups the subjects were investigated regardless of whether they remained in the Lundby area or not; 2550 were followed from 1947 and 1013 from 1957. At the point of intake the subjects were aged between 0 and 95 years (median = 31 years). The Lundby area, and the study population drawn from it, have been exposed to considerable societal changes. The area – originally rural – has acquired a suburban character, and more than half of the population have moved away. In 1997, 602 of the surviving population lived in the Lundby area, and 1195 elsewhere (69.8% in communities with <10 000 inhabitants).
Data sources supporting diagnosis and attrition (n = 3563)
†Including the population from 1947 (n = 2550) and the newcomers in 1957 (n = 1013).
Demographic data and neurotic disorders in subjects at risk for psychosis (n =3498)
†In patients with a psychotic disorder neurotic disorder refers to separate episodes with a perceptible onset and termination that preceded the onset of the psychotic disorder.
Data have been accumulated from semi-structured face-to-face interviews by psychiatrists, registers (e.g. the national patient register, regional registers and regional hospital archives), case files (inpatient, and outpatient case files from psychiatric clinics, other clinics and general practitioners) and key informants (e.g. relatives and nursing staff). Thanks to the many sources (Table 1), the data have been sufficient for psychiatric evaluations in 99% (1947–1972) and 94% (1972–1997) of the subjects. Details about the population, the interviews, the other data sources and the attrition have been published elsewhere [11,12]. Social status was classified according to the Swedish socioeconomic classification [13]: (i) blue-collar workers: unskilled, semiskilled and skilled workers; (ii) white-collar workers: assistant non-manual employees, intermediate non-manual employees, employed and self-employed professionals, and higher civil servants and executives; and (iii) self-employed (other than professionals). The basic demographic data are presented in Table 2.
The ethics committee of Lund University Hospital approved the follow up of the Lundby Study, and the participants provided written consent.
Diagnostic assessment
In 1947 mental disorders were diagnosed according to Essen-Möller et al. [14]. From 1957, however, a revised diagnostic system was used, according to which the 1947 diagnoses have also been re-diagnosed. The different disorders are classified as neurotic, psychotic or organic in a hierarchy – in which organic takes precedence over psychotic, which in turn takes precedence over neurotic – allowing only one diagnosis per episode of psychiatric disorder [15]. In psychotic disorders the sufferer – in the absence of insight – experiences: hallucinations, delusions, formal thought disorder, manic behaviour, catatonia or confusion. Psychotic states due to substances or organic factors are included in the general psychosis category. Dementia, however, excludes the diagnosis of psychosis; and psychosis that appears only during a depressive episode is diagnosed as ‘depression plus other psychiatric symptoms’ [15].
At the 50 year follow up in 1997, consensus diagnoses according to the DSM-IV were assessed alongside the Lundby diagnoses [11,16]. To achieve DSM-IV diagnostic comparability for the whole study period, a DSM-IV evaluation of ‘psychosis’, and ‘depression plus other psychiatric symptoms’, was made for the period 1947–1972. All episodes 1947–1997 were then assigned to one of five DSM-IV-based diagnostic groups (Table 3): (i) psychotic disorder due to a general medical condition, including delirium; (ii) substance-induced psychotic disorder, including substance-induced delirium/intoxication with psychotic features; (iii) schizophrenia, and schizoaffective disorder; (iv) other non-affective psychotic disorder (note: groups iii and iv together constitute the total group of non-affective psychoses); and (v) affective psychotic disorder, including major depressive disorder with psychotic features, and bipolar disorder with or without psychotic features. Groups (i) and (ii) are at the top of the diagnostic hierarchy. Also, a hierarchy was introduced for groups (iii–v); once subjects had contracted schizophrenia/schizoaffective disorder they were no longer considered to be at risk for other non-affective psychotic disorder and affective psychotic disorder. Age at onset for the DSM-IV diagnoses was meant to be the earliest age at which an episode met the criteria for the diagnosis. Age at onset was based on all relevant data available. Prodromal periods were included if they had a perceptible onset and were clearly continuous with the onset of frank psychosis.
Groups of psychotic disorders based on DSM-IV diagnoses (diagnostic modifications indicated)
AP, affective psychotic; BP, bipolar; GMC, general medical condition; MDD, major depressive disorder; NAP, non-affective psychotic; NOS, not otherwise specified.
There were 39 subjects already with psychotic disorders at the point of intake and these were excluded; they had contracted their disorders between 15 and 67 years of age (median = 30 years). Moreover, 26 subjects with dementia at the point of intake were excluded, thus leaving 3498 subjects at risk for psychosis (male, n = 1795; female, n = 1703).
Statistical procedures
Calculations of first-incidence rates were based upon subjects who, by the start of the follow up, had been free from the outcome under study, and other outcomes of higher diagnostic rank. Male–female differences of mean age at onset were tested by constructing 95% confidence intervals (CIs) for the differences. Incidence rate for first episodes (IR) were obtained as the number of first occurrences of a disorder in subjects aged ≥15 years divided by the total number of person-years at risk for that disorder. Male/female differences in IR were tested by constructing 95%CI for the male/female IR ratios [17].
Results
Incidence of cases 1947–1997
There were 108 subjects with a first onset of any psychotic disorder: 63 male and 45 female subjects (Table 4). The number of first-onset diagnoses, however, was 111, because three female subjects with an initial other non-affective psychotic disorder later developed psychotic disorder due to a general medical condition, schizophrenia and affective psychotic disorder, respectively.
New cases and age at onset of DSM-IV psychotic disorders among subjects aged ≥15 years in the Lundby population who were at risk for psychosis at point of inception 1947–1997 (n =3498)
AP, affective psychotic; BP, bipolar; C, cases; n, no. subjects free from any psychotic or bipolar disorder at point of inclusion in the study; GMC, general medical condition; NAP, non-affective psychotic; SIP, substance-induced psychotic. †The total number of episodes in female subjects was 48, because three female subjects had two diagnoses each. †Including delirium (GMC and SIP) and intoxication (SIP). §Including schizoaffective disorder. ††Including brief psychotic disorder, delusional disorder, psychotic disorder NOS (no case of schizophreniform disorder was identified). ¶Including major depressive disorder with psychotic features and bipolar I, II and NOS disorder, with or without psychotic features. ∗Statistically significant difference of mean age at onset in male and female subjects (p < 0.05).
Age at onset of psychotic disorders 1947–1997
The male age at onset was lower than that for female subjects for any psychotic disorder, psychotic disorder due to a general medical condition, non-affective psychotic disorder and schizophrenia (Table 4).
Medical conditions involved in psychotic disorder due to a general medical condition
Several medical conditions were found to be aetiologically related to the psychotic states in psychotic disorder due to a general medical condition (Table 5). Moreover, visual and hearing impairment was judged to play an aetiological role in some cases. It was common that multiple aetiologies were present in individual cases with insufficient evidence to establish a single specific aetiology. In Table 5 the medical conditions associated with psychosis may be seen.
Aetiological medical conditions† involved in psychotic disorder due to a GMC
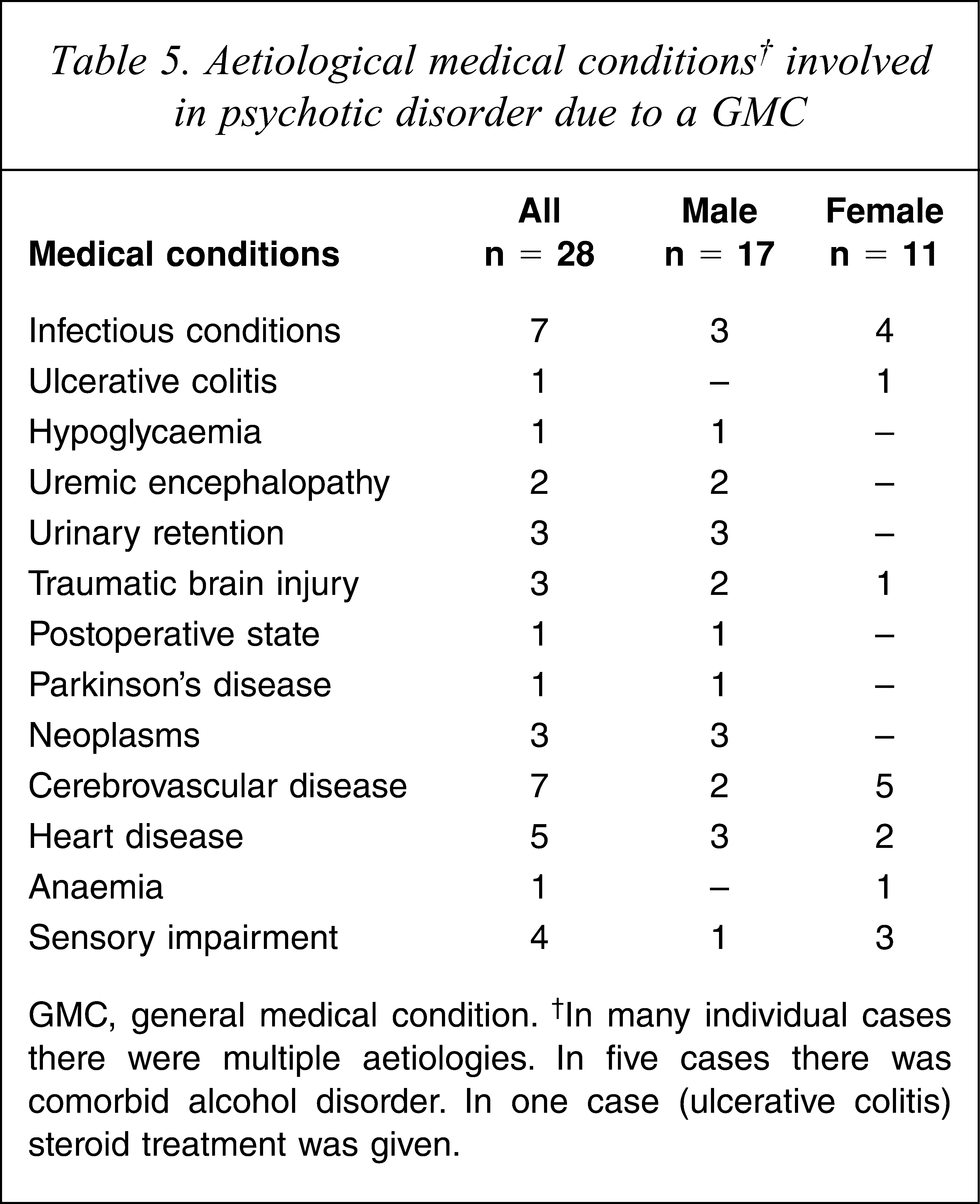
GMC, general medical condition. †In many individual cases there were multiple aetiologies. In five cases there was comorbid alcohol disorder. In one case (ulcerative colitis) steroid treatment was given.
Incidence rates of psychotic disorders 1947–1997
The male incidence rate of substance-induced psychotic disorder was higher than that for female subjects, but for the other disorders the rates did not differ between the sexes (Table 6).
Incidence rate and male/female IRR for first episodes of DSM-IV psychotic disorders in subjects aged ≥ 15 years in the Lundby population 1947–1997 (n = 3498)

AP, affective psychotic; BP, bipolar; Cl, confidence interval; GMC, general medical condition; IR, incidence rate; IRR, incidence rate ratio; NAP, non-affective psychotic; NOS, not otherwise specified; SIP, substance-induced psychotic; Y, years under risk for any psychotic or bipolar disorder. †Incidence rate per 10 000 person-years at risk. ‡Including delirium (GMC and SIP disorder) and intoxication (SIP disorder). §Including schizoaffective disorder. ††Including brief psychotic disorder, delusional disorder, psychotic disorder NOS (no case of schizophreniform disorder was identified). ¶ including major depressive disorder with psychotic features and bipolar I, II and NOS disorder, with or without psychotic features. ∗Statistically significant difference between male and female subjects (p < 0.05).
Sex- and age-specific incidence rates of psychotic disorders 1947–1997
The incidence rate by age for any psychotic disorder was higher in male than female subjects for all age bands except the ≥65 age band (Figure 1). For psychotic disorder due to a general medical condition the rates were fairly equal between the sexes and increased in the ≥65 age band. For substance-induced psychotic disorder, male subjects had a higher rate than female subjects across all age bands. For non-affective psychotic disorder the male rate trended down from the peak in the 15–29 year age band, while the female rate peaked in the 30–44 and ≥65 year age bands. The male rate was higher than that for female subjects in the 15–29 year age band, but the female rate was higher in the other age bands. For schizophrenia the rate peaked in the 15–29 year age band in both sexes, although male subjects had more than double the rate of female subjects. After age 29 the trend for men reduced to reach zero, whereas female subjects retained a low rate. For other non-affective psychotic disorder the male rate was fairly stable, while the female rate peaked in the 30–44 and ≥65 year age bands. For affective psychotic disorder the male rate was stable, whereas the female rate tended to peak in the 45–54 and ≥65 year age bands.
Discussion
This is the first study to analyse a population cohort for incident psychoses for a period of 50 years. Interestingly, the overall incidence rates did not differ between male and female subjects, except for in the case of substance-induced psychotic disorder. This finding stands in contrast to recent studies of psychosis incidence, in which the incidences of non-affective psychoses and schizophrenia have been higher in male than female subjects [2,6].
Psychotic disorder due to a general medical condition
The age at onset of psychotic disorder due to a general medical condition was lower in male subjects, but the incidences were similar between the sexes. We did not identify any study with which to compare our findings.
Substance-induced psychoses
The community rate of substance-induced psychoses is not known [18] and we found no population studies on age at onset of substance-induced psychoses. In Belarus, however, the yearly register-based incidence rate of alcohol psychoses was estimated to have varied between 6.8 and 23.7 per 100 000 between 1970 and 2005 [19]. Notwithstanding methodological differences, the present rate was within this range.
Non-affective psychoses
The present incidences were in fairly good concordance with the findings in the World Health Organization 10-country study of schizophrenia incidence [20], in which the annual rate per 10 000 population aged 15–54 years for broad and narrow schizophrenia varied from 1.6 to 4.2 and 0.7 to 1.4, respectively. In the present study the incidence rate per 10 000 person-years at risk in subjects aged 15–54 years for non-affective psychosis and schizophrenia was 4.2 (95%CI = 2.7–5.8) and 2.1 (95%CI = 1.0–3.2), respectively.
Additionally, the non-affective psychoses rates were also in accordance with the result from a register study of the Swedish population aged 25–64 years for non-affective psychoses incidence in which the rates, correlated to increasing levels of urbanization, ranged from 31 to 75 and 30 to 84 per 100 000 person-years in male and female subjects, respectively [21].
In a treated incidence study of a large catchment area that included older subjects, the mean age at onset for schizophrenia was 31.2 years for male subjects and 41.1 years for female subjects, which is moderately compatible with the present age at onset [22].
In the Lundby population the male age at onset was lower than that for female subjects for non-affective psychoses and schizophrenia, but we found no significant differences between the sexes for the overall incidence rates of these disorders. Many schizophrenia incidence studies have found an earlier/sharper peak and an earlier age at onset in male subjects compared to female subjects [20,22–27] although a sex difference in age at onset has not been observed in familial schizophrenia [24,28], and there are some findings of non-differing male–female age at onset [29], as well as earlier onset in female subjects [30]. Many studies, however, have shown an increased overall risk of schizophrenia in male subjects compared to female subjects [3,4], although many have excluded older subjects.
The risk of inception, however, of DSM-IV schizophrenia and delusional disorder in cognitively intact individuals seems to extend above age 60 and 70 years [9]. In a review approximately 23% of all schizophrenia patients had their onset of symptoms after age 40 [31]. In the Lundby population, in 33% (6/18) of schizophrenia cases onset occurred after age 44.
In the present study the incidence in the ≥65 age band was 8 per 100 000 person-years for DSM-IV schizophrenia (male 0 and female 16 per 100 000). Previous register data have indicated an incidence rate of 15–20 per 100 000 person-years for late paraphrenia [9], and in one sample the incidence of DSM-III-R schizophrenia was 12.6 per 100 000 person-years in the population aged ≥65 years [22]. The inclusion of late-onset schizophrenia patients in the Lundby Study – who were all female – explains the non-differing overall incidence of schizophrenia in males and female subjects.
The finding that male subjects are prone to getting ill earlier than female subjects, and/or that the disorders are delayed in female subjects, has been suggested to be explained by male–female biological dimorphism [5], different ageing processes in male and female subjects [32,33] and the fact that oestrogen exerts a protective anti-dopaminergic action in female subjects [26,34,35]. Another hypothesis says that male and female subjects are differently prone to subtypes of schizophrenia, with male subjects more often having an early neurodevelopmental form and female subjects more often a late disorder related to affective psychosis [22,36–39].
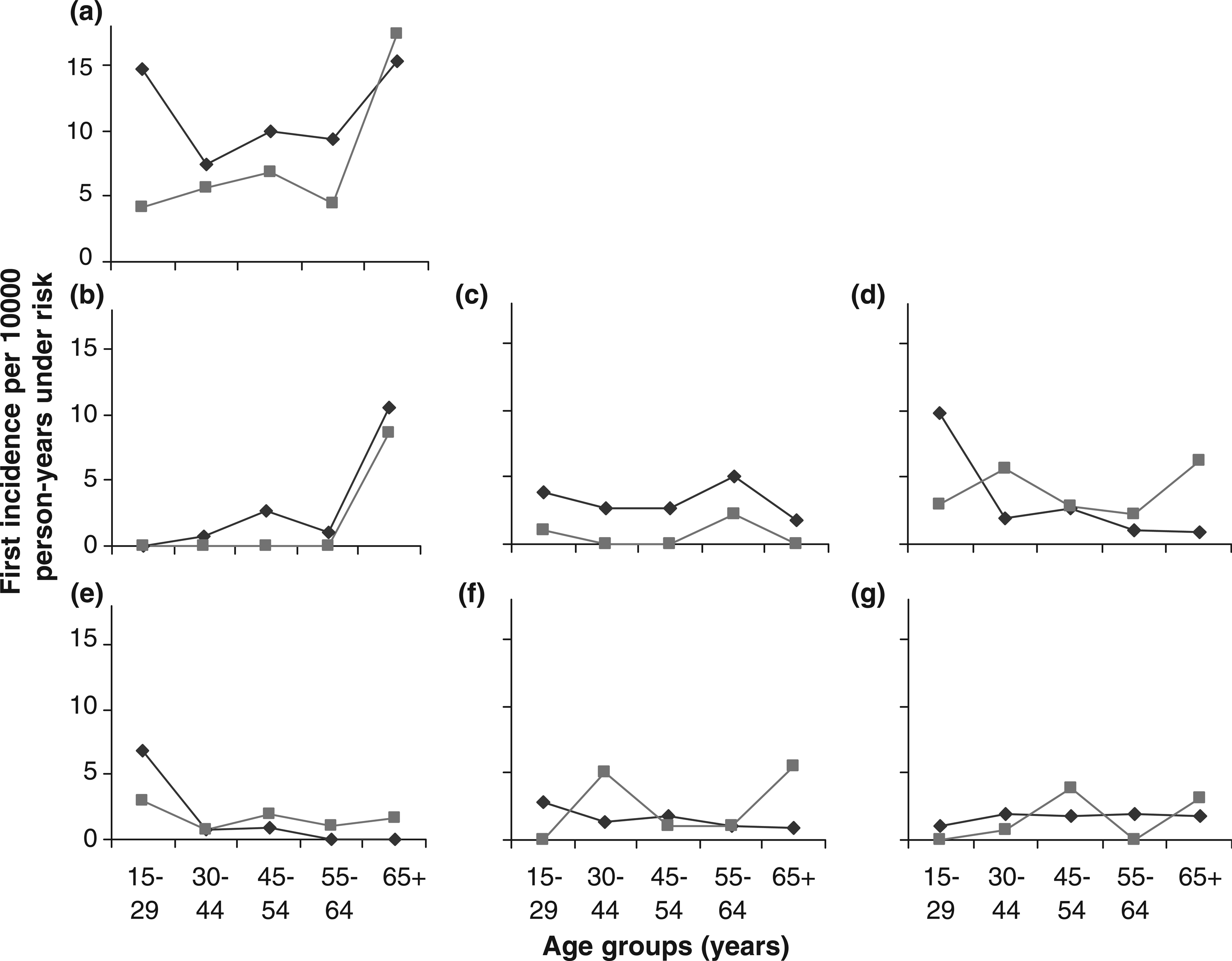
Incidence rate of first episodes of psychotic disorders by sex and age in the Lundby population 1947–1997. (♦) Male; (▪) female. (a) Any psychotic or bipolar disorder; (b) psychotic disorder due to a general medical condition; (c) substance-induced psychotic disorder; (d) non-affective psychotic disorder; (e) schizophrenia; (f) other non-affective psychotic disorder; (g) affective psychotic disorder.
It should be noted, however, that we did not adjust for psychosocial factors such as marital status, premorbid personality and family history of mental disorder [40].
Due to there being only a few cases, we grouped brief psychotic disorder, delusional disorder and psychosis not otherwise specified together as ‘other non-affective psychoses’ (we found no case of schizophreniform disorder). The overall incidence rate and the age at onset did not differ significantly between the sexes, although male subjects were on average 13.5 years younger than female subjects when contracting other non-affective psychoses.
We found few community studies on the incidence of other non-affective psychoses. Nevertheless, the present findings approximately accorded with them [41,42].
Affective psychotic disorder
The present results support non-differing age at onset and incidence of affective psychoses in male and female subjects. Most previous studies have also reported nonsignificant differences between age at onset of male and female subjects for affective psychosis/manic episode [2,23,43,44], although some have reported a higher age at onset in female subjects [1,45]. In a review the mean age at onset of treated bipolar disorder ranged between 20.7 and 33 years in men and 21.5 and 31.6 years in women [46]. Some studies of affective psychoses have reported a greater incidence in female subjects than in male subjects [23,27], but most have reported no male/ female difference in the rates of bipolar disorder [2,10,47]. In a review, estimations of the treated incidence of bipolar I disorder varied from 3.0 to 15.2 per 100 000 years in male subjects and 2.0–32.5 per 100 000 years in female subjects [46].
Strengths
The Lundby population is a complete ethnically homogenous population, minimally affected by urbanicity, drug use, migration and socioeconomic segregation, implying a low degree of selection bias. The population was followed with low attrition for 50 years, meaning that many of the subjects passed their risk period for psychosis. Because diagnoses were based on many data sources, probably only a few cases were missed.
Limitations
The population was small, implying imprecise estimates. The population may not be representative of the sociodemographic structure of today. Subjects ill at the inception were not included, which may have biased the age at onset estimates and lowered the incidence rates. Acute and remitting psychoses before inception were not systematically screened for. Due to the long follow up the complementary data sources changed over time, also meaning that the concepts and diagnoses reported in the case files and registers were based on different criteria, which may have impeded the DSM-IV diagnostic ascertainment of data from 1947 to 1972.
Conclusion
In this 50 year follow up of the Lundby population some findings from previous studies of clinical samples were supported: earlier male than female mean age at onset of non-affective psychoses and schizophrenia; preponderance of male subjects among early- and female subjects among late-onset cases of non-affective psychosis and schizophrenia; and non-differing male–female age at onset and incidence rate of affective psychoses.
Moreover, male subjects were significantly younger than female subjects with regard to onset of any psychotic disorder and psychosis due to a general medical condition, which suggests that earlier age at onset of psychosis in male subjects, as opposed to female subjects, may be related to psychosis broadly.
Contrary to several recent studies we found a non-differing male–female risk of non-affective psychoses – including schizophrenia – when all age bands were included.
The male–female difference of age at onset and incidence by age for any psychotic disorder, psychotic disorder due to a general medical condition, non-affective psychotic disorder and schizophrenia may be due to differences between the sexes pertaining to protective factors and/or aetiological factors.
Footnotes
Acknowledgements
We thank the Lundby population for taking part in the study. The work was supported by unconditional grants from the Swedish Council for Planning and Coordination of Research, the Swedish Council for Social Research, the Swedish Research Council, the Swedish Medical Research Council, the Medical Faculty of Lund University, the Provincial Government of Skåne, the Professor Bror Gadelius Foundation, the Ellen and Henrik Sjöbring Foundation and the Division of Psychiatry, Lund University.