
Abstract
Large-scale epidemiological studies suggest that depression and most anxiety disorders are more prevalent in women compared with men [1–3]. Evidence from clinical or epidemiological studies also suggests a role of reproductive life phases in the onset, recurrence of symptoms or changes in symptom severity of psychiatric disorders in women [4–11].
Obsessive–compulsive disorder (OCD) is an important mental disorder associated with reproductive life events in women. OCD seems to be more frequent among pregnant and postpartum women compared to the general population. The current prevalence rates of OCD in women have been reported to be between 0.2% and 1.6% [2,12,13] in the general population, 0.2–5.2% during pregnancy [14–19], and 0.7–3.9% during puerperium [20–22]. In addition, previous studies reported an association between the pregnancy or puerperium and development of or changes in symptom severity of OCD [7,8,15,23–25].
When compared to the pregnancy and postpartum period, the relationship between OCD and the postmenopausal period, which is an important phase of life for women, has been examined less frequently. In a study by Labad et al. 9% of postmenopausal OCD patients described menopause-related onset of OCD [8]. Recently, Vulink et al. noted that OCD is exacerbated in 47% of patients during menopause [25].
Although there are some studies investigating OCD and menopause associations, the numbers remain inadequate. Moreover, the available reports are mostly retrospective in nature and they present limited data on this topic. To the best of our knowledge, there has been no published study exploring comprehensive data on OCD in postmenopausal women. In the present study the objective was to examine the prevalence rate, clinical features, related factors, and comorbidity of OCD in postmenopausal women.
Methods
Two hundred and sixty-nine postmenopausal women consecutively attending the Gynaecology Outpatient Clinic of the Research and Training Hospital of the Selcuk University were recruited for the present study. Exclusion criteria included illiteracy, history or existence of cerebrovascular or other neurological diseases, the existence of severe general medical illnesses such as uncontrolled endocrine abnormalities, rheumatological diseases cardiovascular and pulmonary system diseases, and gynaecological malignancies. In addition, subjects who received a psychotropic medication within the previous 4 weeks were not included in the study. After the objectives and procedures of the study were explained, written informed consent was obtained from all the participants.
In the gynaecology outpatient clinic, sociodemographic characteristics and gynaecological history of the participants were recorded. The postmenopausal state was confirmed on serum hormonal levels (follicle-stimulating hormone >40 mIU mL−1, oestradiol level <20 pg mL−1, luteinizing hormone >25 mIU mL−1) as well as the absence of menstruation for at least 12 months. Subsequently, the participants were referred a psychiatrist. During the psychiatric evaluations the diagnoses of OCD and comorbid psychiatric disorders were determined by means of the Structured Clinical Interview for DSM-IV (SCID-I) [26]. Obsessive–compulsive symptoms were assessed using the Yale–Brown Obsessive–Compulsive Scale [27]. Both instruments have been standardized, and their validity and reliability for the Turkish population have been determined [28,29]. The course of pre-existing OCD and onset time of OCD were determined on the basis of retrospective reports given by the patients.
Statistical analyses were performed using SPSS 13.0 for Windows (SPSS, Chicago, IL, USA). The categorical variables in postmenopausal women with and without OCD were compared using χ2 and Fisher's exact tests, as necessary. The independent sample t-test was performed for comparisons including quantitative data between the same groups. Significant level was two-tailed and set at the 0.05 level.
Results
In the 269 postmenopausal women, the mean age at assessment was 50.64 ± 5.88 years, the mean age at onset of menopause was 46.45 ± 5.02 years, and the mean duration of the postmenopausal period was 46.59 ± 38.94 months. Most of the participants were married (n = 242, 90.0%), primary school graduates (n = 233, 86.6%) and housewives (n = 255, 94.8%). Fifty-seven women (21.2%) had surgical menopause, and 20 women (7.4%) were taking hormone replacement treatment.
Nineteen women (7.1%) met the criteria for OCD according to SCID-I at the assessment. Two women (0.7% of all participants and 10.5% of OCD patients) reported that their OCD began within the first 6 months of the postmenopausal period. OCD was present before menopause in 17 women (89.5% of OCD patients). Exacerbation of OCD symptoms during the postmenopausal period was described by five of 17 patients (29.4%), whereas eight (47.1%) of the 17 women reported a decrease in their OCD symptoms. The number of women who experienced no change in their OCD symptoms during the same period was four (23.5%).
Among the postmenopausal women with OCD, the most common obsessions were contamination and symmetry/exactness, whereas the most common compulsions were cleaning/washing and checking. Table 1 lists the frequency of obsessive–compulsive symptoms in the patients.
Obsessive–compulsive symptoms in postmenopausal patients with OCD
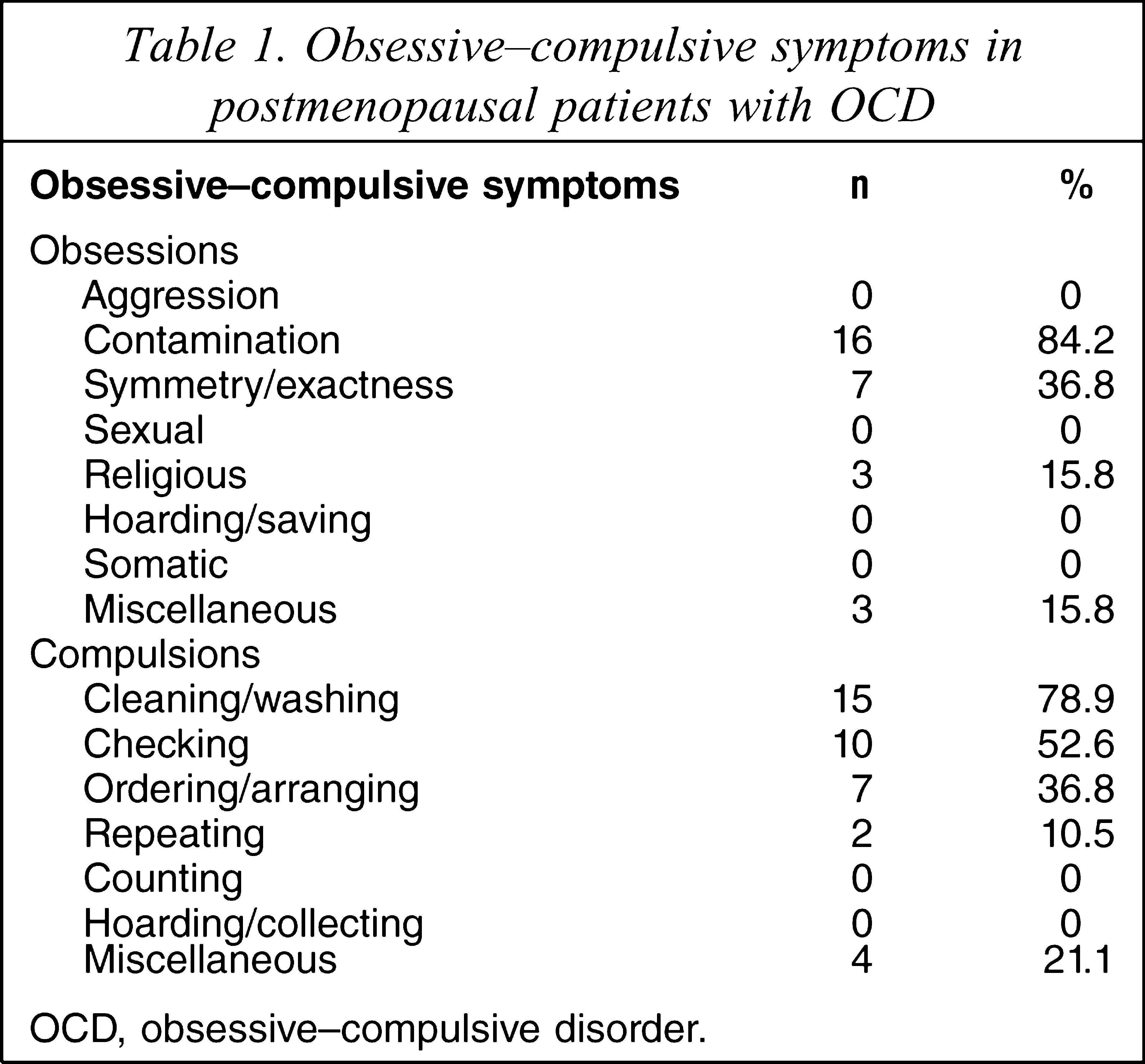
OCD, obsessive–compulsive disorder.
Postmenopausal women with and without OCD had similar socio-demographic characteristics. In addition, OCD was not significantly related to hormone replacement treatment, number of children, age at onset of menopause, duration of postmenopausal period or the type of menopause (natural or surgical). In other words, none of the variables examined in this study was significantly different between the groups (Table 2).
Sociodemographic characteristics of postmenopausal women vs OCD
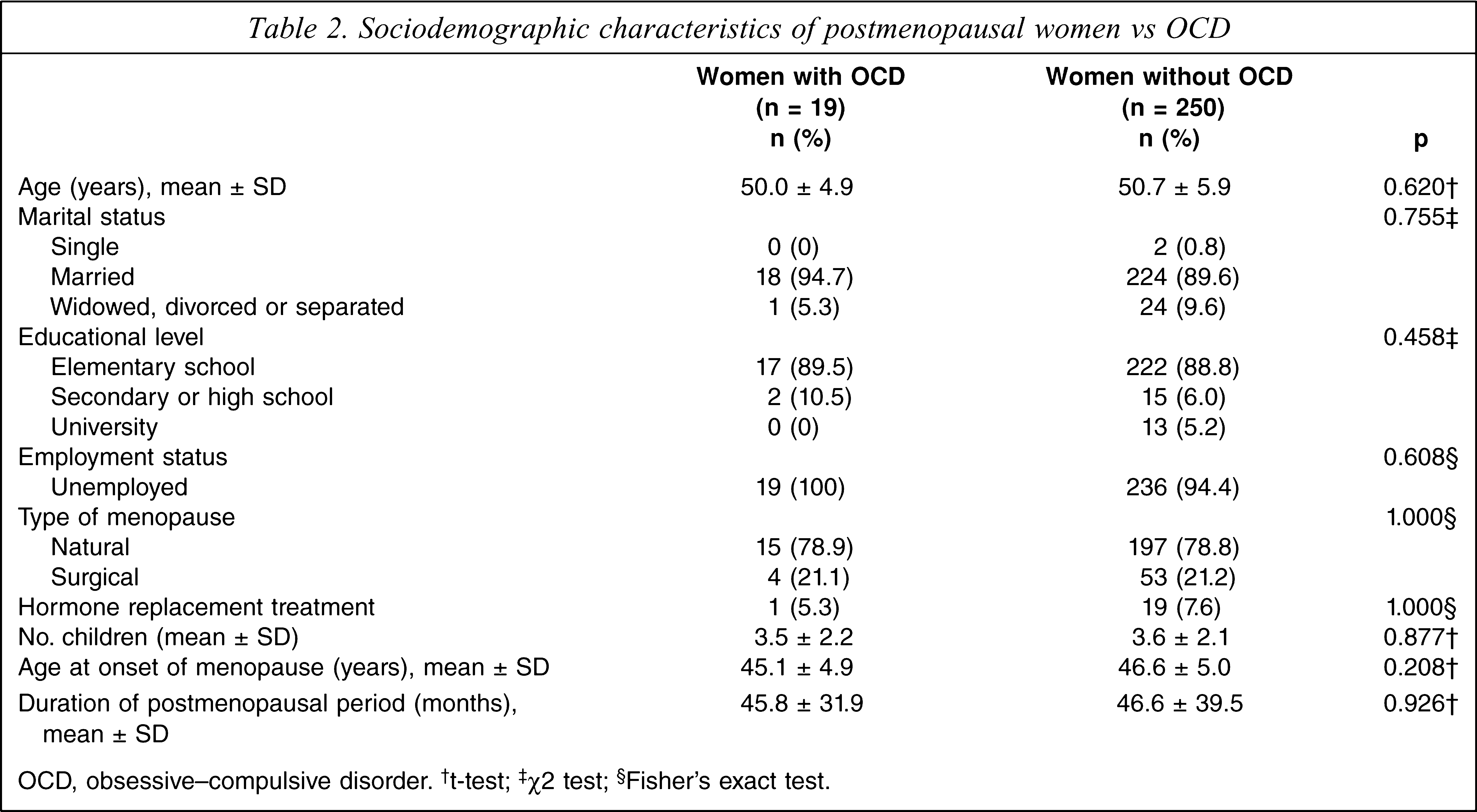
OCD, obsessive–compulsive disorder. † t-test; ‡χ2 test; §Fisher's exact test.
Twelve of 19 patients (63.2%) were currently suffering from an additional mood or anxiety disorder. The comorbidity rate of a mood disorder was 31.6% (n = 6), and an anxiety disorder was 47.4% (n = 9). Generalized anxiety disorder (n = 7, 36.8%) was the most common comorbid disorder. Major depression (n = 5, 26.3%) and panic disorder (n = 4, 21.1%) were other frequent comorbid disorders. In addition, two patients (10.5%) had comorbid dysthymic disorder and one patient (5.3%) had comorbid specific phobia. None of the women with OCD met the criteria for social phobia, post-traumatic stress disorder, bipolar disorder, schizophrenia or other psychotic disorders.
Discussion
To the best of our knowledge, to date, this study presents the most comprehensive data about OCD in postmenopausal women. In the present study the current prevalence of OCD was 7.1% in the postmenopausal women. In the epidemiological investigations conducted in Western countries, the prevalence of OCD has been estimate to be 0.5% for current prevalence and 1.2% for 6 month prevalence in older women [30,31]. OCD appears to be more frequent in the older Turkish female population when compared to women in a similar age band in Western populations. Kirmizioğlu et al. found the current prevalence rate of OCD to be 4.2% in Sivas, Turkey [32]. The 12 month prevalence rate reported by Çilli et al. in Konya, Turkey (where the present study was carried out) was 4.3% among women aged 45–64 years [33]. The present prevalence rate is higher than that reported in those studies. The discrepancies between the other studies and the present one conducted in Turkey may be related to the differences between study settings (general population and clinical sample, respectively). All clinical samples may be expected to have higher morbidity than non-clinical samples.
OCD occurred during the postmenopausal period in 10.5% of the present OCD patients. This is in agreement with the study by Labad et al. [8]. In addition, the incidence rate of OCD was 0.7% during the postmenopausal period in the present sample. We found no study regarding the incidence of OCD for the same period. The current study suggests that OCD in postmenopausal patients begins generally before the menopause. The present findings, however, were based on retrospective recall of the patients for the onset time of OCD, which is a restrictive factor in interpretation of these results. Prospective controlled research is necessary in this topic.
To the best of our knowledge, no prospective study based on the course of OCD using an objective scale exists to date. The limited available data include retrospective reports of OCD patients. Labad et al. noted that perimenopause or menopause was associated with worsening of pre-existing OCD in 8% of patients [8]. In contrast, Vulink et al. reported that 47% and 6% of menopausal OCD patients experienced an exacerbation of and an improvement of their OCD symptoms during menopause, respectively [25]. In the present study, with regard to the severity of OCD symptoms during the postmenopausal period, whereas 29.4% of the patients described a worsening, the rate of patients who reported a reduction was 23.5%. The proportion of patients who did not experience any change of OCD symptom severity in the present study was similar to that reported by Vulink et al. [25].
The frequency of obsessive–compulsive symptoms differs considerably between populations, because sociocultural factors may affect the content of the symptoms [34]. In the present sample the most common obsessions and compulsions were contamination and cleaning/washing, respectively. These have been reported as the most common obsessive–compulsive symptoms in studies conducted among Turkish female outpatients [35,36]. We did not observe, however, aggressive, sexual, somatic, hoarding/saving, and counting obsessions or compulsions, which are frequently reported in Turkish female outpatients. These discrepancies may result from differences in the age of the various study samples and in the clinical settings in which the studies were carried out (gynaecology outpatient clinic vs psychiatric outpatient clinic).
Studies suggest that 60–94% of female outpatients with OCD have additional Axis I diagnosis [35,37]. We found a 63.2% comorbidity rate of any mood or anxiety disorder in postmenopausal women. In contrast to previous studies carried out among outpatients who sought treatment at psychiatry clinics [35,37,38], generalized anxiety disorder but not major depression was the most prevalent comorbid disorder in the present study. Health-care seekers with OCD appear to exhibit comorbid major depression more frequently than non-health-care seekers with OCD [39]. None of the present patients reported any intention to seek psychiatric treatment for their OCD. Additionally, some epidemiological surveys suggested that generalized anxiety disorder tends to be more prevalent in middle-aged and older women compared with younger women in the general population [31,40]. This may be another explanation for the present findings.
The following limitations of the present study must be taken into account. First, the sample size was relatively small, and it may not be representative of all postmenopausal women because it was obtained from a clinical setting. Ideally, the studies should be performed in the general population. Second, in order to establish the course of pre-existing OCD during the postmenopausal period and onset time of OCD (before or after menopause), the data were gathered from the patients cross-sectionally. The possibility of error in recall of this information may exist. Future studies should include prospective observations using structured instruments to estimate the incidence of OCD and to determine the course of pre-existing OCD symptoms during the post-menopausal period. Third, and more importantly, the present study did not include a control group consisting of premenopausal women matched for age, marital status, socioeconomic status, and who were admitted to the same outpatient clinic. The control group would be necessary to determine whether there is any difference between the premenopausal or postmenopausal women in terms of prevalence, clinical features, and comorbidity of OCD.
In conclusion, despite the limitations, the present results suggest that postmenopausal women who were admitted to a gynaecology clinic have more frequent prevalence of OCD than that estimated among female subjects within a similar age range in the general population, and that during the postmenopausal period, approximately half of the patients experience a change in pre-existing OCD symptoms, and approximately two-thirds of the patients have a comorbid mood or anxiety disorder.