
Abstract
Obsessive–compulsive disorder (OCD) is conceptualized as a condition that consists of obsessions and/or compulsions. There are other features of OCD that appear in response to obsessions, for example, avoidance and reassurance seeking [1–3]. However, they are usually considered non-specific or less diagnostically important. Thus, avoidance behaviour has not been regarded as part of the ‘core obsessive–compulsive experience’ [4].
It has been observed that what is avoided in OCD is directly and clearly related to the content of obsessions [5]. For example, OCD sufferers with contamination obsessions tend to avoid objects and places perceived to be dirty or infected; those who have aggressive or sexual obsessions may avoid people ‘targeted’ by such obsessions; individuals with obsessions about running over pedestrians may avoid driving; and people whose obsessions are about the significance of certain numbers may avoid counting that involves ‘unlucky’ numbers. Thus, avoidance in OCD may pertain to certain people, external objects, stimuli and situations, as well as activities and behaviours, such as driving and counting [6]. Some behaviours, for example washing, may be avoided because of the fear that it would be difficult to stop washing once started.
Avoidance has been linked most often to contamination obsessions and washing/cleaning compulsions [3–5,7–11], followed by ‘unacceptable’ obsessional thoughts (e.g. aggressive, sexual and religious obsessions) and checking compulsions [3,5,12–15]. Avoidance was also described in postpartum OCD [16,17]. Interestingly, overt compulsions were absent in these cases and avoidance of sharp objects and the baby appeared to be the main means of coping with obsessions about harming the baby. Avoidance was less frequently reported in ‘primary obsessional slowness’ [18] and ordering and arranging compulsions [19].
Why does avoidance seem to frequently accompany contamination obsessions? One possibility is that people with contamination-based OCD have relatively little difficulty identifying external, threatening stimuli related to contamination; this then leads to avoidance of such stimuli [8,20]. Strong feelings of disgust may also help explain the apparently high frequency of avoidance in contamination-based OCD, both because these feelings commonly characterize contamination-based OCD [21] and because disgust feelings may predict and maintain avoidance in OCD [11,22].
Apart from these clinical observations, there are very few research-derived data regarding the role and clinical relevance of avoidance in OCD. It appears that prominent avoidance may be associated with poorer outcome of behaviour therapy and/or pharmacotherapy of OCD [23], but there are numerous unresolved issues in this area. For example, why do some people with OCD develop extensive avoidance behaviour, whereas others do not? Do OCD people with avoidance have a more severe condition than those without avoidance? If they do have a more severe illness, regardless of the symptom-based subtype of OCD [24], could that account for the generally poorer treatment outcome in such cases?
Considering some of the aforementioned issues, the aims of the present study were threefold. First, we wanted to collect information on the nature and frequency of avoidance in people with OCD and to systematically investigate the types of obsessions related to avoidance. Second, our aim was to compare OCD individuals with and without avoidance. Finally, we aimed to elucidate factors that could predict avoidance in people with OCD.
On the basis of the reviewed literature and our own clinical observations, we hypothesized that contamination and aggressive obsessions were more commonly associated with avoidance. We also hypothesized that OCD with avoidance was a more severe illness than OCD without avoidance, based on the finding of positive correlations between avoidance and OCD symptoms [25] and on the reports that other anxiety disorders, such as panic disorder [26] and social anxiety disorder [27], were more severe with greater avoidance. Finally, we hypothesized that avoidance in individuals with OCD could be predicted by the presence of contamination and aggressive obsessions and a stronger propensity to experience disgust, as well as by female gender, higher levels of depression and more frequent and distressing obsessions. The latter was based on the findings that female gender, more prominent depression and more frequent panic attacks were risk factors for developing agoraphobic avoidance among people with panic disorder [28].
A recent review of the clinical features and diagnostic criteria of OCD has concluded that there are ‘many different types’ of avoidance in OCD [29]. This underscores our need to note that in this study we did not conceptualize as avoidance behaviours that are better understood as compulsions or compulsive acts. For example, avoidance of throwing away possessions by people with hoarding was not considered an instance of avoidance because it is an essential part of the definition of compulsive hoarding. Likewise, compulsive checking was not regarded as avoidance of catastrophic outcomes, such as one's house burning down. Furthermore, we did not focus on the avoidance of certain feelings (e.g. fear), thoughts and cognitive operations such as decision-making, because this avoidance is a different phenomenon from observable avoidance behaviours.
Material and methods
This report has resulted from the Nepean OCD study. A total of 124 individuals over the age of 18 with a principal diagnosis of OCD were recruited through the Nepean Anxiety Disorders Clinic, OCD support groups, newspaper advertisements and referrals from general practitioners, psychiatrists, clinical psychologists and mental health services. The principal diagnosis of OCD was determined on the basis of a clinician-administered semi-structured interview, the Mini International Neuropsychiatric Interview (MINI [30]). To qualify as a principal diagnosis, OCD had to be a condition for which help was sought or which caused the most distress or impairment in functioning. Therefore, individuals with a currently co-occurring psychosis, bipolar disorder or other conditions that were judged to be more severe or disabling than their OCD were not considered eligible to participate. Institutional ethics committee approval was obtained prior to commencing the study and all participants provided informed signed consent.
Assessments
Participants were assessed comprehensively by means of a number of clinician-administered and self-report instruments. In this article we report findings derived from the MINI, Yale–Brown Obsessive–Compulsive Scale (Y-BOCS) [31], Vancouver Obsessional Compulsive Inventory (VOCI) [32], Symptom Checklist 90-Revised (SCL-90R) [33] and Disgust Emotion Scale (DES) [34].
As already noted, the MINI is a semi-structured diagnostic interview that was used to establish OCD as the principal diagnosis. It also provided information on the presence of co-occurring DSM-IV disorders. The MINI has been validated against other widely used structured diagnostic interviews and its psychometric properties have been good [35,36].
The Y-BOCS is a semi-structured interview used primarily to measure the severity of obsessions and compulsions in individuals already diagnosed with OCD. It consists of a comprehensive checklist of obsessions and compulsions and a 10-item severity scale. On the severity scale, up to three most prominent obsessions and compulsions are rated in terms of time spent, interference with functioning, distress, efforts to resist and perceived degree of control. Each response is rated on a 5-point Likert scale, and ratings are summed to generate separate scores for the severity of obsessions and severity of compulsions, plus a total Y-BOCS score representing the overall severity of OCD. The Y-BOCS is a widely used instrument, with excellent psychometric properties [37,38].
The Y-BOCS also assesses avoidance related to OCD. In the course of the Y-BOCS interview we asked participants whether they engaged in any avoidance behaviour because of their obsessions or compulsions and recorded the nature of such avoidance (i.e. people, objects, situations, places or activities avoided). Our question was slightly modified from the one included in the Y-BOCS and read as follows: ‘Have you been avoiding anything because of your obsessions or because you were concerned that you would perform compulsions?’
The VOCI is a 55-item self-report instrument that measures OCD symptoms. Its items are rated on a 5-point Likert-type scale, with ratings being summed up to provide a total score and scores on six separate subscales (Contamination, Checking, Obsessions, Hoarding, Just right experiences and Indecisiveness). The psychometric properties of the VOCI were reported to be favourable [32].
The SCL-90R is a psychometrically sound instrument [39] which consists of 90 items that assess symptom distress and psychopathology by means of the scores on the Global Severity Index and nine subscales: Somatization, Obsessive–compulsive, Interpersonal sensitivity, Depression, Anxiety, Hostility, Phobic anxiety, Paranoid ideation and Psychoticism.
The DES is a 30-item scale that lists common disgust elicitors, which are rated on a 5-point Likert-type scale. The ratings yield a total score and scores on five domains of disgust. The internal consistency and convergent validity data suggest good psychometric properties of the DES [40].
Procedure
After informed written consent was obtained, participants were interviewed by a psychiatrist or clinical psychologist who had been trained in the use of the MINI and Y-BOCS. Inter-rater reliability of the MINI-derived DSM-IV diagnosis of OCD, based on 46 of the interviews, was excellent (97.8% agreement). Participants also completed a set of questionnaires that included the aforementioned instruments.
As already noted, in the course of their Y-BOCS interview participants were asked whether they avoided anything as a result of their OCD. We were particularly careful to exclude any avoidance arising as a consequence of co-occurring phobic or other conditions. We did not place a limit on the number of instances of avoidance and recorded all OCD-related avoidance. Likewise, we took into consideration that several instances of avoidance could be related to the same type of obsession. For example, we recorded and counted avoidance of public toilets and avoidance of touching people after taking a shower as separate instances of avoidance related to the same contamination obsession. If the same avoidance was related to two obsessions (e.g. avoidance of children due to both aggressive and sexual obsessions), this was recorded as two separate instances of avoidance. The instances of avoidance were then grouped in accordance with the type of obsession and compulsion that they were related to. With regard to the obsessions in participants with avoidance, we calculated obsessions related to avoidance separately from those unrelated to avoidance.
Data analysis
The numbers and percentages for the demographic variables were calculated, as were the numbers of instances of avoidance and percentages of obsessions related to avoidance. Chi-square tests were calculated to determine whether there were differences in the frequencies of demographic variables and various obsessions between participants with and without avoidance. Independent sample t-tests were conducted to determine whether there were differences in the mean age and severity of OCD and OCD symptom dimensions between participants with and without avoidance. Finally, a logistic regression analysis was performed to determine which variables independently increased the odds of avoidance.
Results
The study sample consisted of 124 individuals with OCD, of whom 76 (61.3%) were women. Their mean age was 44.98 years (SD = 16.12). Forty-eight (38.7%) participants were in a marital/de facto relationship and 45 (36.3%) were never married. Fifty-eight (46.6%) participants had post-high school qualifications, 47 (37.9%) were engaged in full-time or part-time paid employment and 29 (23.4%) were unable to work due to illness-related disability.
Of 124 participants, 74 (59.7%) reported at least one instance of OCD-related avoidance. The groups of participants with and without avoidance did not differ significantly with respect to demographic variables, except for their mean age: those with avoidance were significantly younger (mean = 41.30 years, SD = 15.97) than those without avoidance (mean = 50.44 years, SD = 14.88; t =−3.214, df = 122, p = 0.002). The two groups also did not differ significantly in terms of the frequency of co-occurring phobic disorders, so that these co-occurring conditions and avoidance associated with them did not seem to contribute to the OCD-related avoidance.
Table 1 shows the nature and number of instances of OCD-related avoidance. By far the most common type of avoidance was that related to contamination obsessions (e.g. avoidance of public toilets) or performed with the aim of preventing a contamination-related compulsion such as excessive washing. Avoidance due to aggressive obsessions (e.g. avoidance of potential victims) was somewhat less common.
Avoidance related to OCD
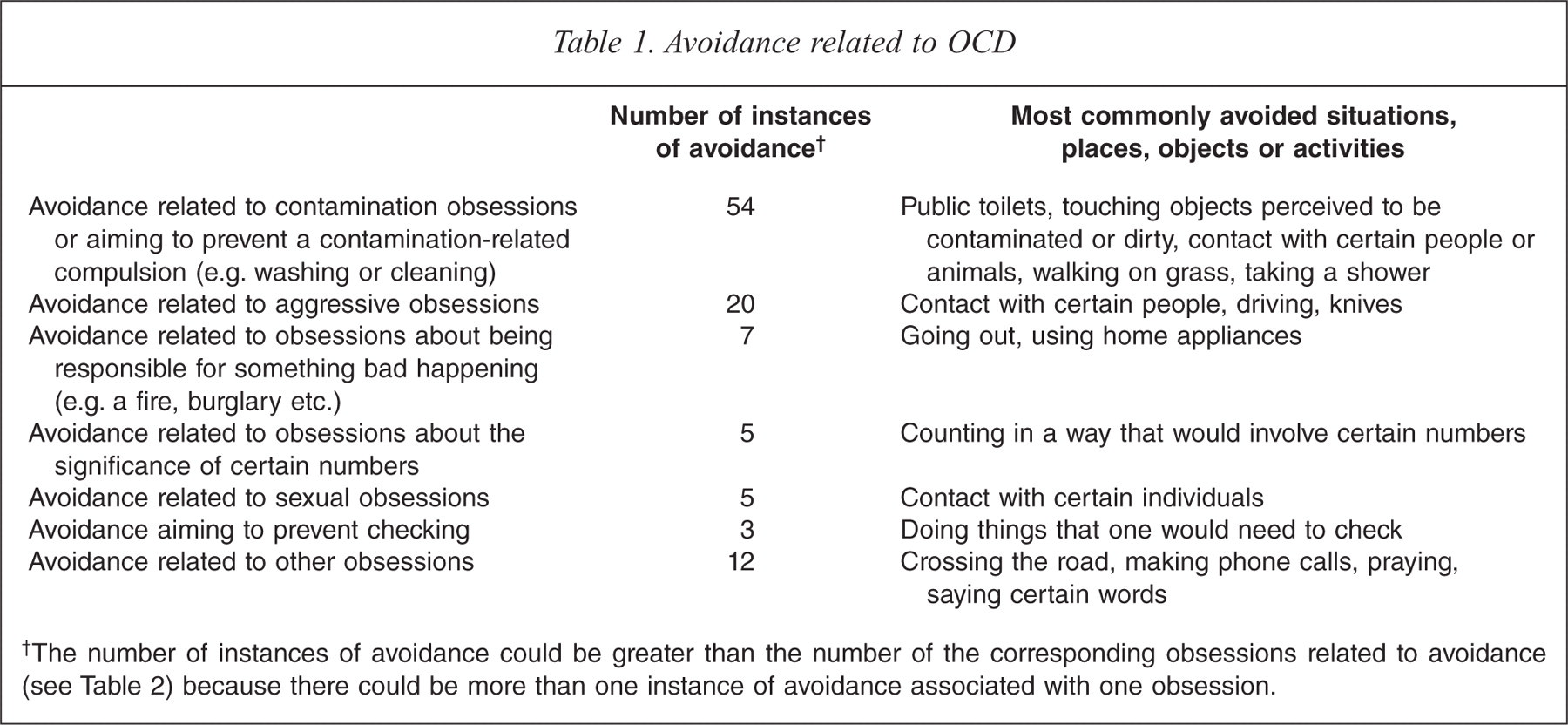
The number of instances of avoidance could be greater than the number of the corresponding obsessions related to avoidance (see Table 2) because there could be more than one instance of avoidance associated with one obsession.
Table 2 shows the frequency with which various types of obsession were associated with avoidance. Almost 80% of all contamination obsessions were associated with avoidance. More than half of the obsessions about the significance of certain numbers, obsessions about being responsible for something bad happening and aggressive obsessions were also associated with avoidance, but the total number of obsessions about the significance of certain numbers and obsessions about being responsible for something bad happening was rather small. On the other hand, very few obsessions about a need to collect and keep objects and obsessions about a need for ordering, arranging and doing things right or in an exact way were associated with avoidance.
Number of obsessions and number and proportion of obsessions related to avoidance in 124 participants with OCD
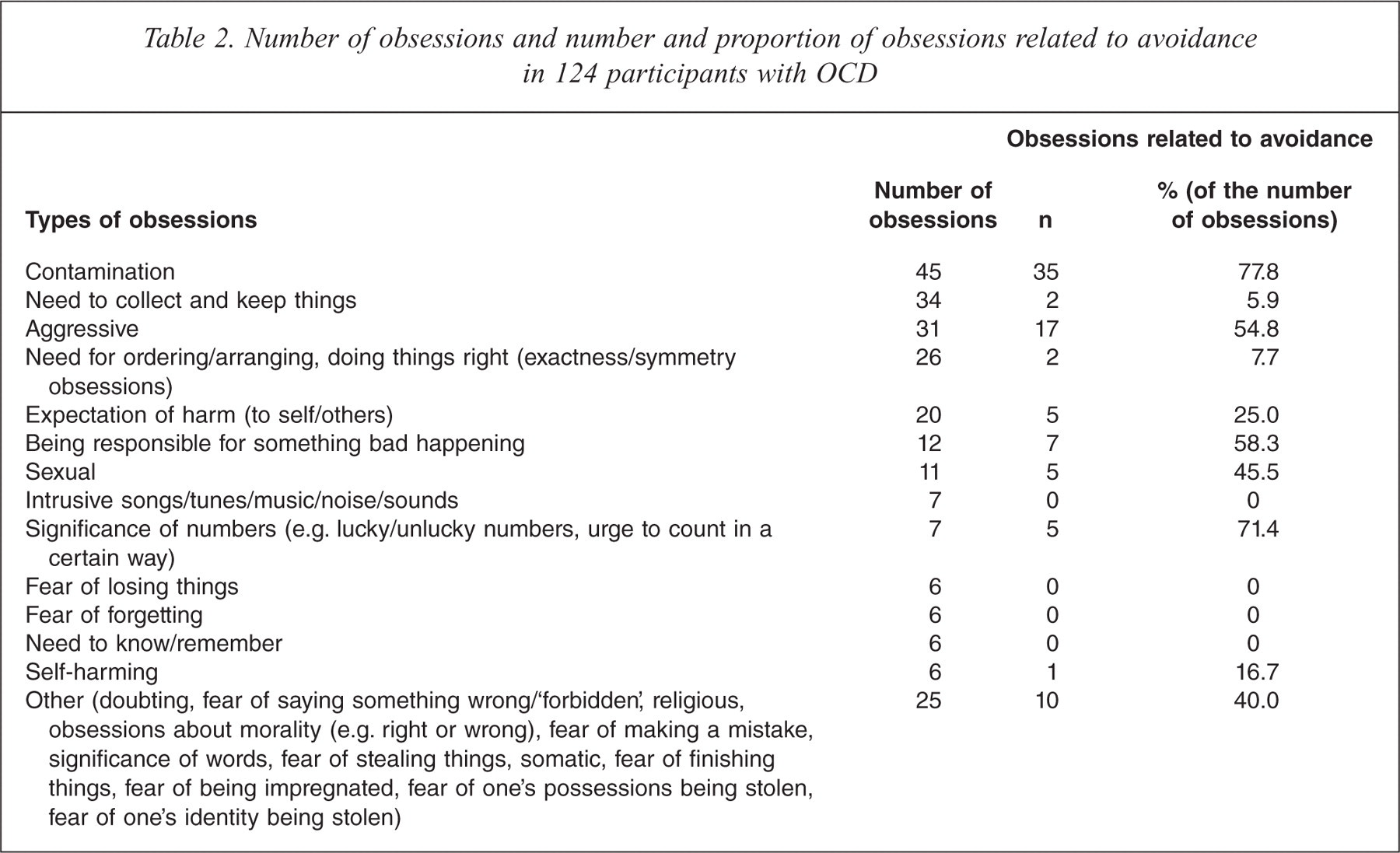
Table 3 compares the frequency of obsessions related to avoidance in participants with avoidance with the frequency of obsessions in participants without avoidance. Again, contamination obsessions were significantly more common among the participants with avoidance and obsessions about a need to collect and keep objects, and obsessions about a need for ordering, arranging and doing things right or in an exact way were significantly more common among the participants without avoidance.
Type and frequency of obsessions in 124 OCD participants with and without avoidance
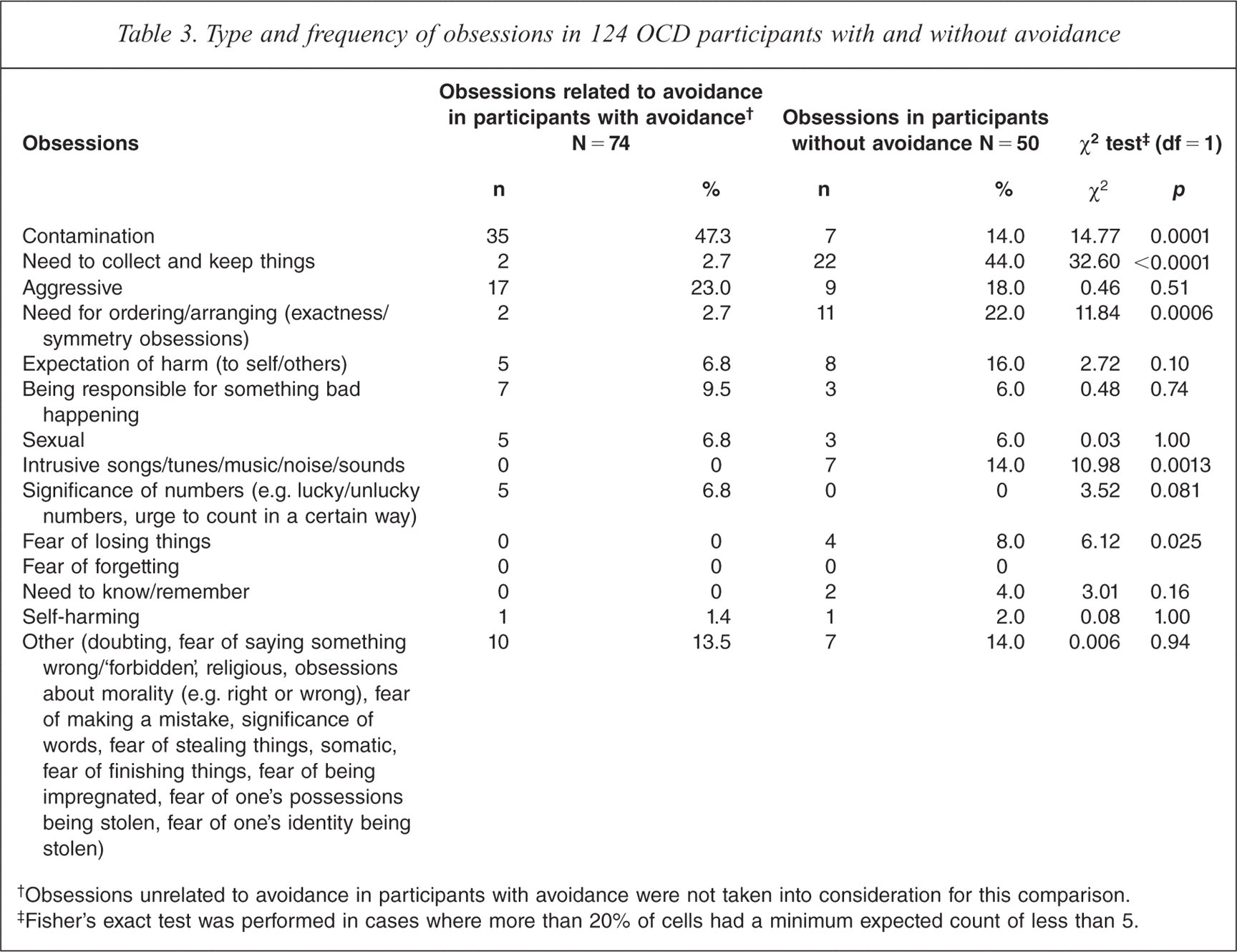
Obsessions unrelated to avoidance in participants with avoidance were not taken into consideration for this comparison.
Fisher's exact test was performed in cases where more than 20% of cells had a minimum expected count of less than 5.
Table 4 compares the overall severity of OCD and severity of the particular OCD symptom dimensions between participants with and without avoidance. Results suggest that OCD with avoidance is a significantly more severe illness than OCD without avoidance. Contamination symptoms and ‘obsessions’ (e.g. aggressive, sexual, religious and self-harming obsessions and obsessions about something bad happening) were significantly more intense among the participants with avoidance, whereas hoarding was significantly more prominent among the participants without avoidance.
Comparisons between OCD participants with and without avoidance
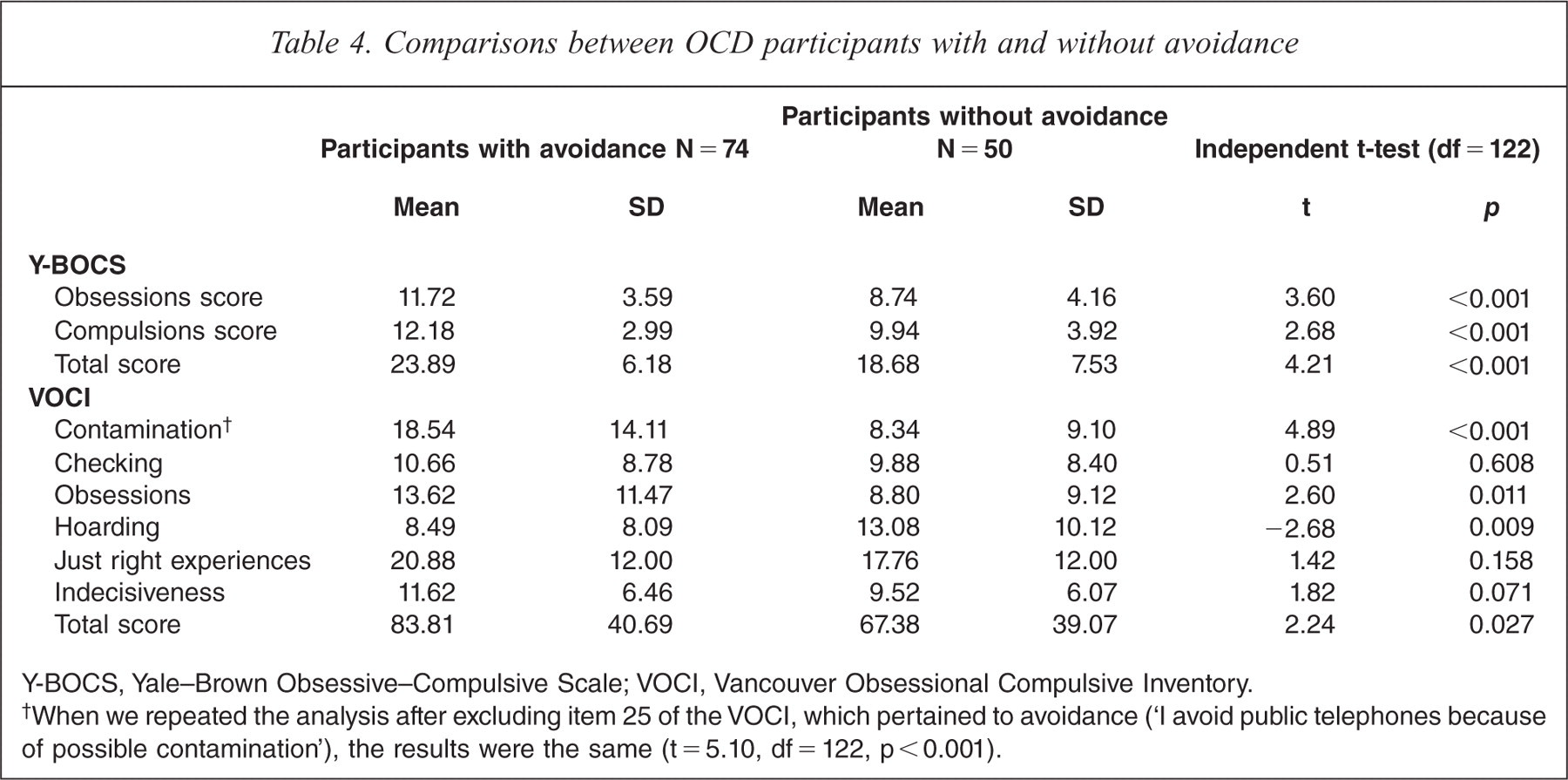
Y-BOCS, Yale–Brown Obsessive–Compulsive Scale; VOCI, Vancouver Obsessional Compulsive Inventory.
When we repeated the analysis after excluding item 25 of the VOCI, which pertained to avoidance (‘I avoid public telephones because of possible contamination’), the results were the same (t = 5.10, df = 122, p < 0.001).
Table 5 shows results of the logistic regression identifying predictors of avoidance in OCD participants. The strongest predictor of avoidance was the presence of contamination obsessions (OR = 6.07, 95%CI = 2.21, 16.66). Other significant predictors of avoidance included the presence of aggressive obsessions (OR = 2.88, 95%CI = 1.02, 8.18) and greater overall severity of obsessions, as measured by the Y-BOCS score for obsessions (OR = 1.17, 95%CI = 1.03, 1.32). In contrast, higher levels of disgust propensity, female gender and more prominent depressive symptoms failed to predict avoidance in OCD, independently of the other variables.
Wald statistics, odds ratios and 95% confidence intervals for odds ratios for the logistic regression model predicting avoidance in OCD
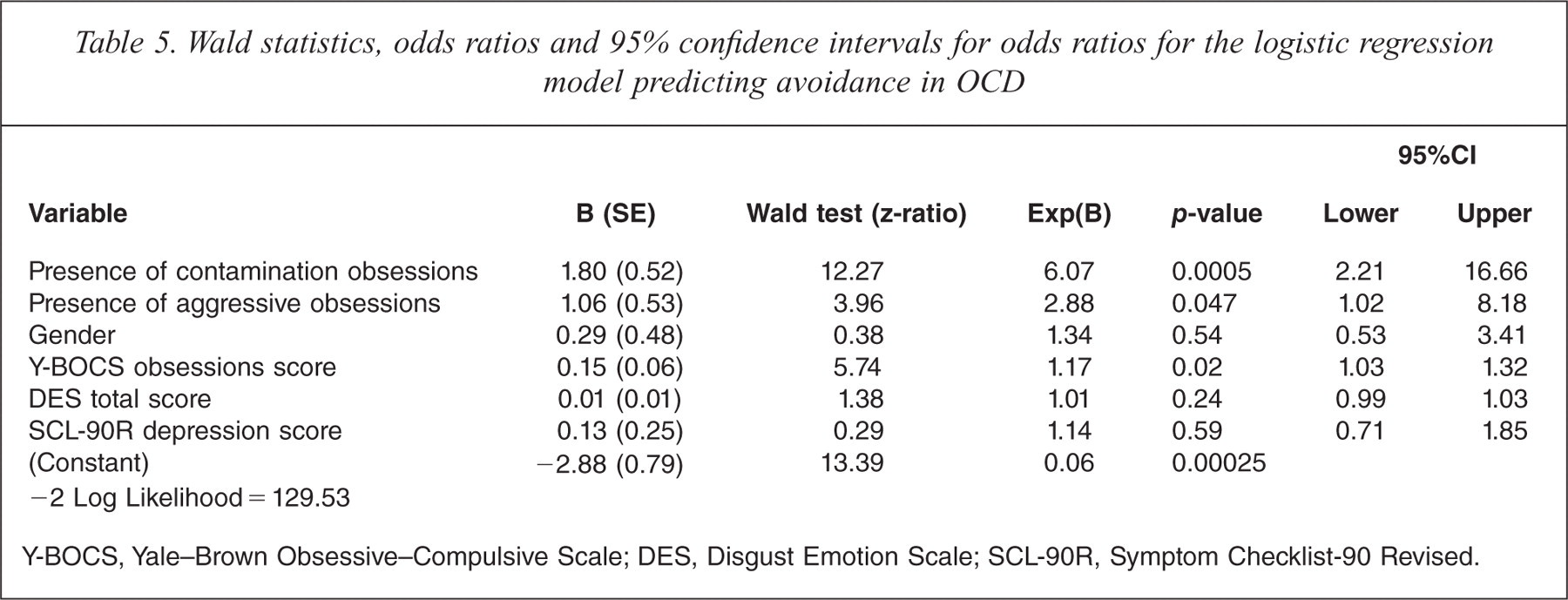
Y-BOCS, Yale–Brown Obsessive–Compulsive Scale; DES, Disgust Emotion Scale; SCL-90R, Symptom Checklist-90 Revised.
Discussion
Our findings suggest that avoidance is a common feature of OCD, reported by almost 60% of individuals with this condition. They also confirm some of the previous observations about avoidance in OCD, especially in terms of the types of obsessions and compulsions associated with avoidance.
To the best of our knowledge, avoidance in OCD has not been previously investigated in a systematic way. Our results suggest that contamination obsessions are frequently associated with avoidance and strongly predict avoidance. This is in agreement with our first and third hypotheses and with previous observations [3–5,7–11]. As already noted, the frequent tendency for individuals with contamination-based OCD to avoid may be accounted for by the likely perception that many of the objects, situations and activities that are perceived as harmful (that is, contamination-related) can be avoided relatively easily. In addition, our finding that participants with contamination-based OCD avoided a great variety of situations (as reflected by the large number of instances of avoidance) may be a consequence of the fact that the objects perceived as dangerous, such as germs, often cannot be seen with the naked eye, and that therefore such objects may be ‘around, everywhere’. Considering that levels of disgust propensity did not independently predict avoidance in our OCD participants, it does not seem very likely that more prominent disgust propensity, which characterizes some people with contamination-based OCD, could by itself account for the high frequency of avoidance in our participants with contamination-based OCD.
Also in accordance with our hypothesis and previous observations [3,5,13] was the finding that aggressive obsessions were associated with avoidance. However, the percentage of participants with aggressive obsessions was not significantly higher in the group with avoidance compared to the group without avoidance, and aggressive obsessions were a weaker predictor of avoidance than were contamination obsessions. These mixed findings can be explained by the ease or difficulty of avoiding the same objects, situations or activities related to aggressive obsessions. For instance, some people with obsessions about hitting a pedestrian can easily avoid driving, whereas others cannot.
Bearing in mind that we did not conceptualize as avoidance behaviours what are better understood as compulsions, it is noteworthy that it has not been reported before that obsessions about a need to collect and keep possessions and consequent hoarding behaviour were rarely associated with avoidance. Obsessions about a need for ordering, arranging and doing things right or in an exact way were also rarely associated with avoidance, which is in agreement with one previous report [19]. The functions served by particular compulsions [41] may explain the weak association between avoidance and hoarding and between avoidance and ordering/arranging/symmetry obsessions and compulsions. For instance, if hoarding largely serves the function of ensuring that one does not lose a valued possession, then avoiding objects and their acquisition is not necessary. Likewise, if ordering, arranging and symmetry compulsions often serve the function of ensuring that one's internal and external world feels ‘just right’, then there may be little need to avoid any objects, situations or activities.
Understanding avoidance in OCD may allow for a more precise distinction between various symptom dimensions and subtypes of the disorder. Of the three most clinically useful and valid OCD symptom dimensions [29], we found that contamination-based OCD was associated with avoidance behaviour, whilst hoarding and ordering/arranging/symmetry obsessions and compulsions were not.
In view of the strong link between avoidance and contamination-based OCD, avoidance may be incorporated either in the DSM-5 diagnostic criteria for OCD or in the accompanying description of OCD, as a frequent feature of contamination-based OCD. Avoidance would certainly need to be better defined and operationalized if it is to become a part of the diagnostic criteria.
To the extent that avoidance behaviour characterizes anxiety disorders and makes OCD ‘closer’ to the anxiety disorders, our results are in agreement with the suggestion that contamination-based OCD may resemble an anxiety disorder, whereas OCD characterized by hoarding or ordering/arranging/symmetry obsessions and compulsions seems more ‘remote’ from the anxiety disorders [42]. The results are also in agreement with the previous suggestion that there is a similarity between compulsive washing/cleaning and specific phobias [20] and with reports that hoarding and ordering/arranging/symmetry obsessions and compulsions frequently co-occur with other disorders such as schizotypal personality disorder and tic disorders, respectively [43,44].
Findings derived from both a clinician-administered and self-report instrument confirm our second hypothesis that OCD individuals with avoidance have a more severe illness than OCD individuals without avoidance. This has direct implications for treatment in that greater severity of OCD has been suggested to predict a poorer treatment outcome and poorer prognosis [45,46]. As already noted, avoidance, too, has been associated with poorer treatment outcome [23]. Perhaps one way of improving treatment outcome in people with OCD and avoidance is to pay more attention to avoidance and target it more aggressively, in addition to using the standard technique of exposure and response prevention. This calls for further research.
The findings of this study should be considered in light of the fact that there are various types of avoidance in OCD and that we chose to focus only on behavioural avoidance. For this reason, we could not investigate how behavioural avoidance may interact with experiential avoidance in people with various obsessions and compulsions. A related issue is a simple assessment of avoidance, which is due to a lack of instruments that would assess avoidance in more detail. We acknowledge that some avoidance behaviours in OCD are subtle and that their assessment may require extensive questioning or detailed clinical observation, not used in this study. Another limitation of the study is that the number of some obsessions was too small for them to be included in the analyses or to allow us to draw any conclusions. For example, this is the reason for which we could not ascertain to what extent sexual and religious obsessions may be related to avoidance. Likewise, our assessment of the extent and variety of avoidance associated with sexual obsessions and obsessions about the significance of certain numbers was limited by the small number of these obsessions.
These limitations aside, we conclude that avoidance is common in OCD, that it is associated with greater severity of illness and that it is particularly frequent among the individuals with contamination obsessions. Avoidance is rare in OCD characterized by hoarding or ordering/arranging/symmetry obsessions and compulsions. These findings have important implications for the conceptualization and treatment of OCD and call for further studies of avoidance in this disorder.
Acknowledgements
The authors are grateful to Colin Slocombe from ACEDA Adelaide, Michelle Graeber from ARCVIC Melbourne, Scott Blair-West of the Melbourne Clinic, the Blacktown OCD Support Group, Julie Leitch of the Kogarah OCD Support Group, Linda Junee of the Mental Health Association of New South Wales and the Penrith Mental Health Practitioners Network.
Declaration of interest
The Nepean OCD study was supported by the Nepean Medical Research Foundation and by a grant from the Pfizer Neuroscience Research Grants Program. The authors alone are responsible for the content and writing of the paper.