
Abstract
Lithium is a unique and effective psychotropic agent with a long-standing history of clinical use yet it is increasingly overlooked in lieu of newer agents. The purpose of the present paper was to succinctly review the therapeutic profile of lithium particularly with respect to the treatment of mood disorders and consider its unique properties and clinical utility. A comprehensive literature review pertaining to lithium was undertaken using electronic database search engines to identify relevant clinical trials, meta-analyses and Cochrane reviews. In addition articles and book chapters known to the authors were carefully reviewed, and the authors appraised published guidelines. The evidence from these sources was rated using National Health and Medical Research Council evidence levels and synthesized according to phenotype and mood states. In addition, the authors have drawn upon published guidelines and their own clinical experience. Lithium has specificity for mood disorders with proven efficacy in the treatment of both unipolar depression and bipolar disorder. The recommendations are based predominantly on Level I evidence, but its clinical use has to be tempered against potential side-effects and the need for ongoing monitoring. In practice, lithium should be considered a first-line option in bipolar disorder, especially in prophylaxis and when onset of action is not an imperative. Lithium has been in use in modern medicine for 60 years and as such has been tried and tested across the full range of mood disorders. Arguably, lithium is the only true mood stabilizer and because of its unique properties is in a class of its own.
All pleasures contain an element of sadness
Jonathan Eibeschwitz
At the molecular level, lithium is a relatively simple element. Classified as an alkali metal, it is highly reactive and therefore usually exists in nature as a compound. Lithium was discovered approximately two centuries ago in the mineral, petalite, hence the derivation of its name from lithos, the Greek word for stone. Used widely in industry for the manufacture of alloys, batteries and heat-resistance glass, lithium serves no vital biological function, but is of interest because of its medicinal properties [1].
Lithium salts were initially used to treat gout and rheumatism in the 19th century and this led to its introduction into mainstream medicine. The realization of its psychotropic effects culminated eventually in its use for the treatment of mood disorders, specifically manic depressive illness. Its clinical role, however, has become less defined, in part due to the arrival of competing agents but also because it lacks commercial interest. Further, as the classification of mood disorder subtypes has developed, the illnesses that lithium treats have effectively become more difficult to define [2]. Another possible explanation for its fall out of favour, however, is the ever-increasing sophistication of clinical trials [3] and the truism that the longer an agent is available, the harder it is to prove its efficacy. This has meant that older studies are regarded methodologically as less rigorous and that overall early data are considered to be less important. This is particularly problematic for an agent such as lithium, for which many salient findings pertaining to its clinical effects emanate from studies conducted decades ago. Further, compared to empirical data, the findings from randomized placebo controlled studies have been assigned increasing significance. These studies compromise lithium for a number of reasons; first, many trials are enriched by requiring response to the competing agent before randomization, which biases against the lithium comparator arm. Second, many individuals who are responding poorly to available options are drawn to trials of novel agents, adding bias. It is important to recall that disproving the null hypothesis (the end-point of most studies) only demonstrates the existence of a difference between two treatments. It does not speak to efficacy per se or indicate whether a particular intervention is effective or even helpful. Indeed, often the differences between the active agents and placebo are clinically meaningless.
These biases and constraints have meant that lithium has not been studied in recent years other than when it has served as a comparator or formed part of ‘treatment as usual’. The data concerning the use of lithium in the treatment of mood disorders have been largely forgotten partly because they are piecemeal but also because they are seldom promoted. Further, the evidence for its use in the treatment of mood disorders has been significantly limited by trial designs that subtly favour the comparator agent and collectively this has resulted in declining enthusiasm for lithium as a therapeutic option. Given its pedigree as a mood-stabilizing agent, proven efficacy in research trials and long history of clinical effectiveness, this is quite simply remarkable.
Aims
The aims of the present brief paper were to succinctly review the therapeutic evidence base in relation to lithium and appraise its clinical utility.
Methods
The literature pertaining to lithium, and particularly its role as a treatment for bipolar disorder, was retrieved using electronic database search engines (MEDLINE and PsychINFO) to identify clinical trials, meta-analyses and Cochrane reviews. In addition articles, book chapters and other literature known to the authors were carefully reviewed. Data identified from these sources were rated according to National Health and Medical Research Council (NHMRC) levels of evidence criteria and have been tabulated (Table 1) [4].
Summary of evidence for lithium in mood disorders and schizophrenia
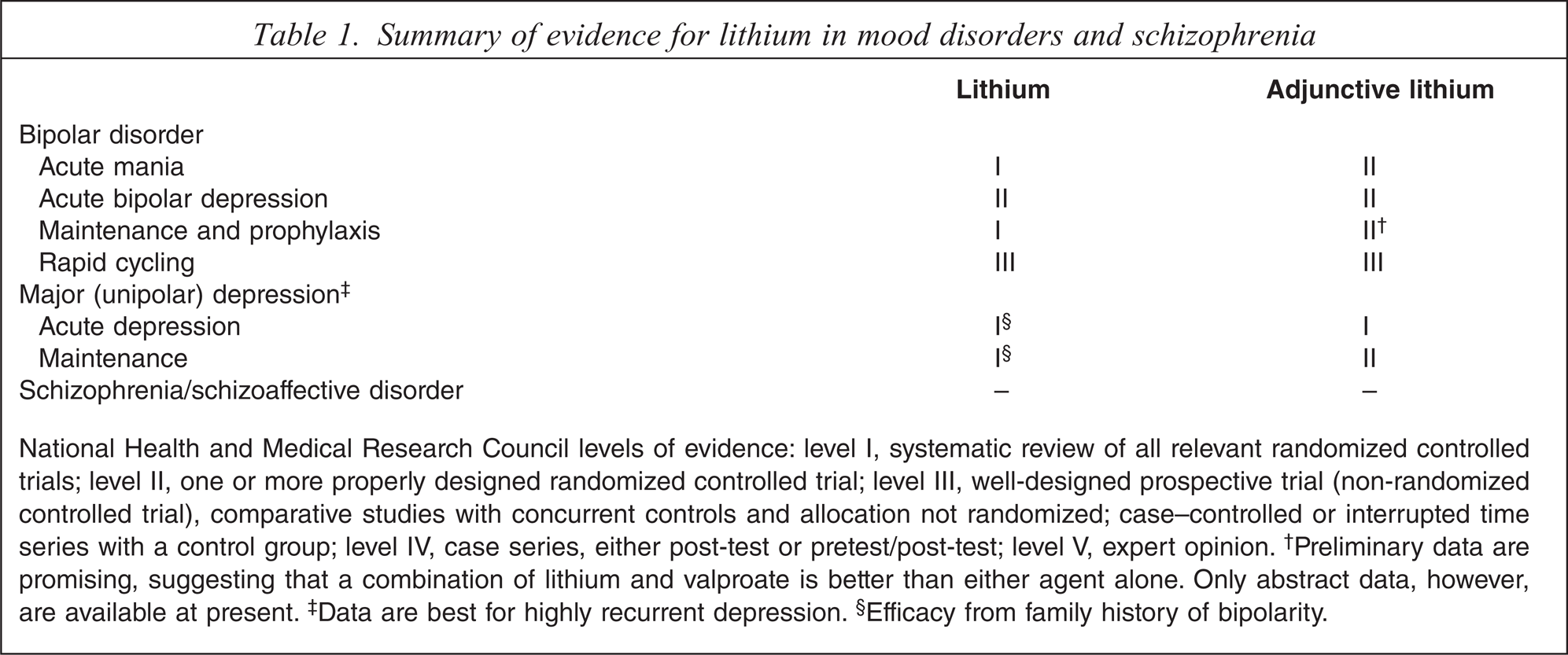
National Health and Medical Research Council levels of evidence: level I, systematic review of all relevant randomized controlled trials; level II, one or more properly designed randomized controlled trial; level III, well-designed prospective trial (non-randomized controlled trial), comparative studies with concurrent controls and allocation not randomized; case–controlled or interrupted time series with a control group; level IV, case series, either post-test or pretest/post-test; level V, expert opinion. †Preliminary data are promising, suggesting that a combination of lithium and valproate is better than either agent alone. Only abstract data, however, are available at present. ‡Data are best for highly recurrent depression. §Efficacy from family history of bipolarity.
Results
Efficacy evidence
Lithium has been studied for more than half a century. During this time mood disorder diagnoses have undergone many revisions and therefore early studies often included bipolar patients within unipolar depressed cohorts. Further, the evidence from research trials includes findings from studies that range from case reports to randomized controlled trials and meta-analyses. The evidence from these diverse investigations that have been conducted in a variety of settings has been synthesized and presented according to phenotype and mood states (Table 1).
Bipolar disorder
Acute mania: Lithium is the benchmark treatment for acute mania and continues to be used as the gold standard comparator in trials assessing the efficacy of other medications [5]. It therefore remains unmatched in terms of the body of evidence that has been accrued in support of its efficacy in the treatment of mania. Although earlier trials demonstrating lithium's superiority to placebo [6–9] have been subject to scrutiny for methodological flaws including the adoption of crossover designs or non-randomized group allocation, a more recent review of trials spanning three decades reaffirmed its clinical effectiveness in treating the manic phase of bipolar disorder [10].
The use of lithium in acute mania does, however, have some limitations, for instance it has diminished efficacy in patients with agitation [11–13] that is not related to psychotic symptoms per se [14–18]. In practice, some of its perceived inefficacy is likely to be attributable to a slower onset of action (6–10 days) as compared to other drugs such as the atypicals that have a more immediate sedative effect, if not anti-manic action. In this context, lithium combined with an antipsychotic appears to be more effective in treating acute mania than either as monotherapy [18–20].
Of note, lithium is regarded to have specificity for classic bipolar disorder that is characterized by recurrent, recognizable mood episodes separated by periods of complete symptom-free remission. In contrast, a reduced response to lithium is usually noted in dysphoric or mixed mania [2,21]. Interestingly, lithium reduces psychotic symptoms in bipolar disorder, particularly in mania, suggesting primacy of mood in this context [22].
Acute bipolar depression: Remarkably, the acute antidepressant effect of lithium monotherapy has not been firmly established by randomized controlled trials [23,24]. Lithium maintains a prominent role, however, in most treatment guidelines for the management of acute bipolar depression, reflecting perhaps its established benefits in bipolar disorder prophylaxis and expert preference [25,26].
Early trials of lithium in unipolar and bipolar depression demonstrated its superiority over placebo [8,9,27–33] but the generalizability of these findings has been questioned in light of the fact that most of these studies involved small sample sizes and that trials were generally of short duration. Additionally, concerns have been raised that in some instances the abrupt cessation of lithium prior to the commencement of the double-blind phase may have contributed to an elevated relapse rate in placebo groups [34]. More recently, findings from the EMBOLDEN I trial found that lithium (600 mg day−1) did not separate from placebo in the acute treatment of bipolar depression [35], although in that particular study the efficacy may have been affected by lower than usual (<0.8 mmol L−1) plasma lithium levels.
Clinically, lithium is disadvantaged because as an antidepressant it takes 6–8 weeks to produce an effect [36]. As a consequence of this significant delay in onset of action, clinicians treating bipolar depression tend to use lithium in combination with other agents. In this context the adjunctive use of lithium as an augmentation strategy is less contentious and has demonstrated efficacy in both bipolar and unipolar depression [36,37].
Maintenance and prophylaxis: Maintenance therapy is arguably the most important aspect of managing bipolar disorder. Therefore, it should be given suitable consideration from the outset of treatment, including when initiating medication for an acute episode [38,39]. It is in this context, namely long-term maintenance and prophylaxis, that lithium outperforms all other agents, as shown by both the burgeoning evidence base that demonstrates its efficacy in trials, and its ongoing clinical use that spans more than half a century. Its robust prophylactic properties in bipolar disorder and superiority over placebo have been corroborated by a systematic review of randomized controlled trials [40] and two meta-analyses, particularly in relation to prevention of manic relapse [41,42]. Most recently, data from the Balance study suggested that lithium has superior maintenance efficacy compared to valproate, with the combination showing greatest overall efficacy [43]. Further, it is important to note that the effects of lithium stabilization are usually sustained for many years and, if treatment is briefly interrupted, prophylactic efficacy can often be re-established [44].
Rapid cycling: Rapid cycling bipolar disorder is defined by DSM-IV as the occurrence of four or more mood episodes during a 12 month period. Episodes are demarcated by partial or full remission for at least 2 months or by a switch to an episode of opposite polarity [45]. In practice, bipolar illnesses that cycle rapidly can often be difficult to differentiate from those with a pattern of highly recurrent mixed episodes [46]. Further, patients with rapid cycling bipolar disorder generally have a poor treatment response to most agents and sustained remission is often difficult to achieve. Hence, there is no clear consensus for optimal treatment [47].
Lithium, along with valproate, arguably has the largest evidence base in the treatment of rapid cycling bipolar disorder [48–52]. Further, in light of its established maintenance properties and reduced risk for suicide, lithium is generally regarded as a reasonable treatment option [53]. Evidence for combination strategies, however, remains weak, but in the clinical setting an incomplete treatment response in rapid cycling bipolar disorder often necessitates a more aggressive approach. In this context open label treatment has demonstrated some benefit of lithium combined with valproate or carbamazepine [48,54].
Major (unipolar) depression
In modern-day practice lithium is rarely used as a treatment for unipolar depression, but early trials that investigated its use in the treatment of acute major depressive episodes identified it as an effective antidepressant with demonstrable efficacy [55–60]. A meta-analysis of these studies in unipolar depression indicates that across a range of plasma levels lithium is superior to placebo, both as an acute treatment and in prophylaxis [61]. It is interesting to note, however, that in these studies bipolarity or a family history of bipolar disorder were found to be predictive of better outcomes, further suggesting that perhaps lithium is ultimately better suited to treating bipolar disorder [29,32,62]. Incidentally, it also points to continuity between bipolar disorder and highly recurrent unipolar disorder, a model that is concordant with genetic data.
In practice, the outcome of major depression following antidepressant treatment is clearly suboptimal, with one-third to one-half of depressed patients failing to show a sufficient response to adequate first-line treatment [63]. Patients who respond only partially, or not at all, to an antidepressant monotherapy trial can then be either switched to another medication or have an augmenting agent added. The latter option of augmentation has the advantage of avoiding a transition period between one medication and another and also builds on any partial response that may have occurred without losing the benefit gained from the initial treatment.
Lithium has been used as an augmentation agent for more than one-quarter of a century. It is now widely recognized as an effective strategy in the management of unipolar depression following an inadequate response to suitable antidepressant treatment [64]. Further, it has repeatedly demonstrated efficacy in combination with selective serotonin re-uptake inhibitors, monoamine oxidase inhibitors (MAOIs) and tricyclic antidepressants in more than 12 double-blind controlled trials and many open-label studies [65,66]. Its efficacy, however, as an augmentation agent in combination with newer agents, such as venlafaxine, mirtazapine or duloxetine, is yet to be comprehensively assessed, but, given its ability to augment both serotonergic and noradrenergic drugs, it is likely that it will confer additional efficacy [67]. Indeed, lithium augmentation has already been shown to be as effective as other strategies such as adjunctive use of MAOI and thyroid hormone or the use of antidepressant combinations [68,69].
Schizophrenia and schizoaffective disorder
While earlier studies suggested some effect in schizoaffective disorder, albeit less than in bipolar disorder [70–74], a more recent systematic review of randomized controlled trials failed to support the use of lithium in treating schizophrenia, either as monotherapy or adjunctively [75]. In that Cochrane review, lithium was found to be useful in only those individuals with prominent affective symptoms. Therefore, in early studies and trials of patients with psychoses the response rate to lithium is diminished when patients with schizoaffective disorder are removed from the analyses. Hence, the clinical effects of lithium appear to specifically target mood and have limited benefit for psychotic symptoms.
Unique properties of lithium
Anti-suicidal
The risk of suicide is significantly elevated in bipolar disorder, with a lifetime risk approximately 15-fold that of the general population. If untreated, it is estimated that up to 20% of patients with bipolar disorder eventually commit suicide [76,77]. In this regard lithium is unique in that it has a recognized anti-suicidal effect such that long-term use reduces the risk of suicide and suicidal behaviour in mood disorders [78,79]. In bipolar disorder this translates to a reduction in suicidality by up to 80% [80–82].
Neuroprotection
Enhancing neuroprotection is a strategy intended to slow or halt neuronal loss, which in turn prevents or slows the natural course of the illness. Although bipolar disorder is not considered to be a classic neurodegenerative disorder, imaging and post-mortem studies have clearly demonstrated neuronal dysfunction including neuronal/glial stress and atrophy. More recently, an active process of neuroprogression in the disorder has been uncovered [83] and, in this regard, the neuro-protective properties of lithium are thought to underpin its mechanism of action and may be responsible for its mood-stabilizing effects in bipolar disorder [84].
Indeed, since the pioneering research of John Cade [85], lithium has been associated with the activation of neurotropic pathways and its neuroprotective qualities are one of its most replicated biological effects [86]. In particular, lithium treatment has been associated with increased grey matter volume in areas associated with emotional processing and cognitive control [87], and the direct targets of lithium, such as inhibition of glycogen synthase kinase-3 and mitochondrial/endoplasmic reticulum key proteins, are thought to have aetiological significance with respect to bipolar disorder [86]. A better understanding of lithium's neurotrophic effects and its interactions with second messenger systems is therefore likely to assist researchers in identifying novel agents that are potentially useful as future bipolar disorder treatments.
Discussion
Clinical utility
Positioning
A cursory examination of recent guidelines for the treatment of bipolar disorder indicated that lithium as monotherapy is widely advocated as a first-line agent in the management of each phase of the illness and that it ranks highly, alongside other recommended agents [25,26,88–94]. Further, its use in combination with anti-convulsants and antipsychotics also features prominently as a first-line option in the treatment of mania, and either as a first- or second-line option in the treatment of bipolar depression and prophylaxis. Similarly, lithium is an important option in most major (unipolar) depression guidelines, particularly as an adjunctive augmentation strategy in cases of non-response, and for prophylaxis [64,88,95]. This is important because it suggests that most authorities acknowledge the importance of lithium as an effective treatment and that it is clinically valued, especially when bedside experience and clinical wisdom have been incorporated into guidelines and recommendations [96]. Given that most guidelines, however, struggle to achieve widespread implementation it is unclear what influence, if any, the prominent positioning of lithium has on real-world clinical practice.
Monitoring
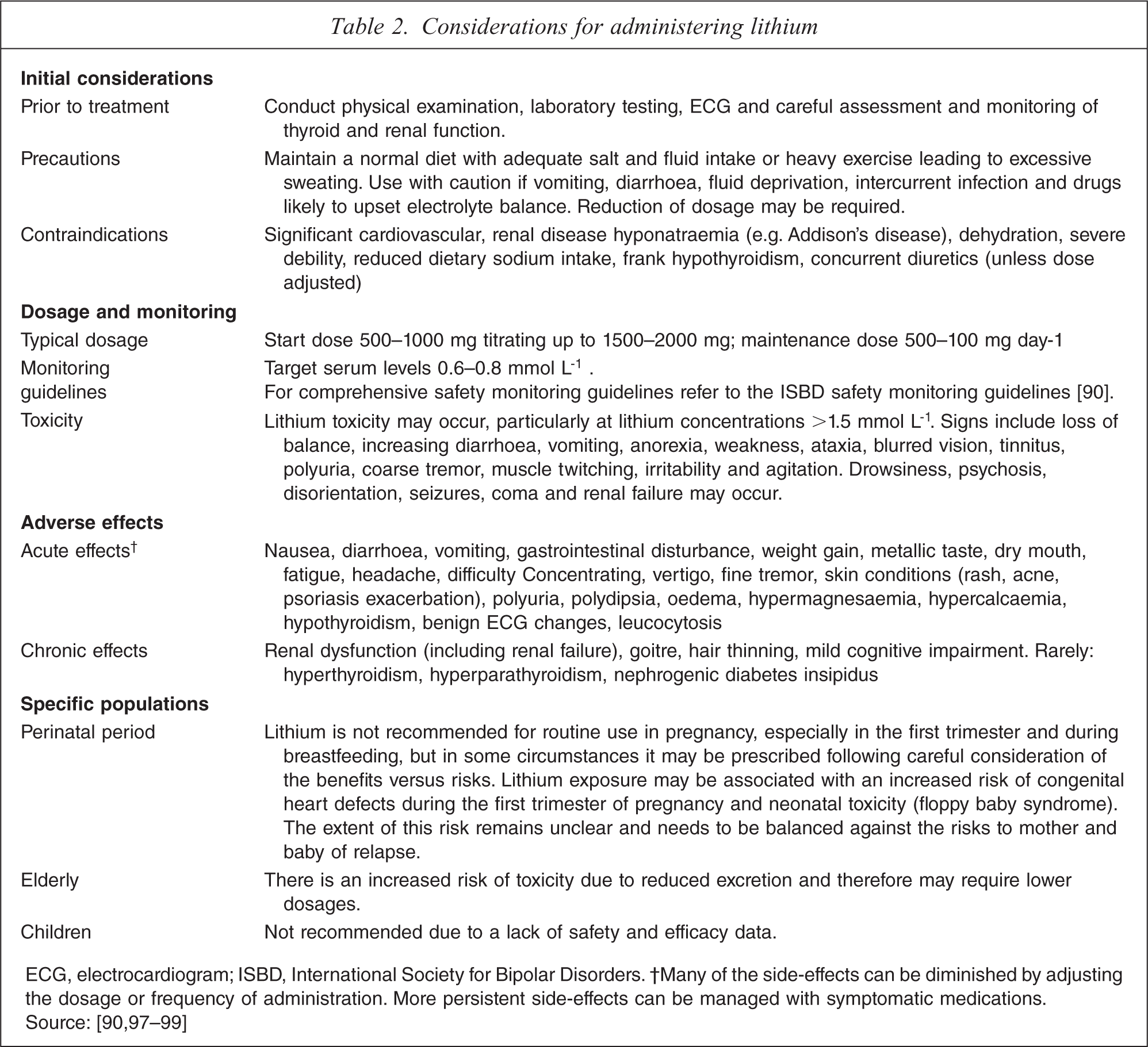
Clinically, lithium warrants early consideration but should be administered judiciously. Individuals about to commence treatment with lithium should be fully informed of its potential side-effects and must undergo appropriate screening (Table 2). Treatment, once initiated, should be reviewed periodically and blood levels must be monitored regularly. Ideally, a level of 0.6–0.8 mmol L−1 should be maintained [90], but lower levels can be occasionally useful and higher levels are sometimes necessary. In these circumstances careful surveillance is required and individuals should be informed about signs of potential toxicity.
Considerations for administering lithium
Maintaining
When lithium is used to treat bipolar disorder or highly recurrent unipolar depression, long-term maintenance therapy is advocated. In cases when lithium is used in the short term, or has to be withdrawn because of side-effects or pregnancy, the dosage should be tapered gradually. Abrupt cessation can precipitate relapse and therefore, wherever possible, should be avoided. If indicated lithium therapy can be reinstituted after discontinuation, but it is important to note that previous levels of efficacy may not always be achieved.
Conclusion
Lithium is not a new drug. It has been in use in modern medicine for 60 years and has therefore been trialled across the full complement of psychiatric conditions. Gradually over the years it has developed a clinical niche in the treatment of mood disorders in which it has remained a useful medication. But lithium now faces a major problem in that it is an old drug, and one that has no commercial champion. Without such support or clinical interest its importance is likely to diminish and its role as gold standard comparator in clinical trials may also disappear.
Pharmacologically and therapeutically, lithium clearly is in a class of its own because it is not a typical anticonvulsant, antipsychotic or antidepressant. Indeed, in our current bipolar armamentarium it is arguably the only true mood stabilizer [100]. This term, however, lacks official recognition and does not, in any regulatory sense, grant lithium any special status. Couple this to its relatively slow onset of action and need for ongoing plasma monitoring and it is perhaps understandable that lithium is gradually losing its appeal. Research has clearly demonstrated, however, that mood disorders are recurrent illnesses and that in the absence of a cure, long-term success can be achieved only by preventing relapse. In this realm lithium has an impressive track record particularly when considering long-term treatment, over periods of years and decades. Further, it is thus far the only agent that protects against suicide, possibly the most important recurrent risk conferred by mood disorders. It is these aspects of lithium that it should be noted for because they truly differentiate it from other available treatments. At a time when increasing therapeutic specificity is being sought it is likely that lithium holds an important key to understanding bipolar disorder, if not the key.
Footnotes
Acknowledgements
The authors acknowledge the NHMRC Program Grant (510135) for essential financial support. In the past 3 years Professor Gin Malhi has served on a number of international and national pharmaceutical advisory boards, received funding for research and has been in receipt of honoraria for talks at sponsored meetings worldwide involving the following companies: Astra Zeneca, Eli Lilly, Jansen-Cilag, Organon, Pfizer, and Wyeth. Professor Michael Berk has received funding for research from Stanley Medical Research Foundation, MBF, NHMRC, Beyond Blue, Geelong Medical Research Foundation, Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, Organon, Novartis, Mayne Pharma, Servier; has received honoraria for speaking engagements from Astra Zeneca, Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, Janssen Cilag, Lundbeck, Pfizer, Sanofi Synthelabo, Servier, Solvay, Wyeth; and served as a consultant to Astra Zeneca, Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, Janssen Cilag, Lundbeck, Servier. Danielle Adams has received honoraria from Eli Lily for speaking engagements.