
Abstract
I get two kinds of depression. In the first kind I have no energy, no interest and no enthusiasm. I am flat and lethargic, don't want to get out of bed, and could sleep the day away. In the second, I am miserable, and agitated and so irritable I could burst. My thoughts are churning, awfully negative, and I contemplate suicide. Initially, I mainly had the first kind of depression, but as time has gone on, I get more and more of the other. Now the depressions seem to be coming more often and for shorter times and I seldom seem to be well.
The first descriptions of bipolar disorder were that of Aretaeus of Cappadocia, who believed that mania and depression were part of the same disease. Kraepelin recognized mixed episodes believing that the two states can co-exist. He describing six variants of mixed states which included depression with flight of ideas, excited depression, depressive-anxious mania, inhibited mania, unproductive mania and manic stupor [1].
Bipolar mixed states are a common area of diagnostic difficulty, yet it is crucial to make an accurate diagnosis if the condition is to be treated effectively. Fundamentally it is necessary to ascertain whether a patient presenting with apparent mixed symptoms suffers from an agitated depression or a mixed manic episode.
Symptomatically, agitated depression and bipolar mixed states have a very similar presentation and the inclusion of agitated depression as a bipolar mixed state has been suggested [2]. Controversy exists in delineating between these two disorders. In a study of 151 unipolar and 226 bipolar II patients suffering from a major depressive episode, agitated depression was significantly more prevalent amongst the bipolar patients than the unipolar patients (p < 0.0001) [3]. Elsewhere, in a study of inpatients during a 15-day placebo wash-out period, patients with dysphoric mania were clearly distinguished from those with agitated depression using a mania rating scale [4].
Treatment resistance in depression has been associated with many causes, including physical illness, psychiatric comorbidities and substance abuse [5], however, misdiagnosis may also be a cause. Sharma et al. [6] studied a cohort of 61 patients initially diagnosed with ‘unipolar’ treatment resistant depression. Using the Structured Clinical Interview for DSM-IV [7] a diagnosis of bipolar disorder was made for 35% of patients at intake and 59% of patients at a 1-year follow up. At follow up 80% of patients showed evidence of a bipolar diathesis and a switch to mood stabilisers was the most common change in medication.
The efficacy of mood stabilisers, such as lithium [8] and lamotrigine [9] as augmenting agents in treatment resistant depression have been reported. We suggest that this may be due at least in part to a significant number of participants in these studies being having bipolar spectrum disorders.
Mixed states represent a substantial subgroup of bipolar patients. In a study of 179 patients hospitalized with acute mania [10], reported that 58% had classic mania, 38% had mixed or dysphoric mania and 4% were rapid cyclers. A preponderance of mixed states amongst females is a consistent theme in reviews of mixed states [11]. Dell'Osso [12] for instance, described 45.4% of female inpatients with mood disorders as having mixed episodes. However, despite the potential clinical significance of mixed features in cohorts with predominantly depressive presentations there is little prevalence data for this subgroup.
Clinical features
Characteristically, patients with mixed states have higher rates of comorbid substance use and have a greater propensity for psychosis, suicidal ideation and attempts [13–16]. Indeed increased emotional intensity and reactivity are thought to be a core feature of manic and mixed states [17]. In a study of suicidality, Dilsaver et al. [15] examined 93 patients with pure and mixed mania and using a score of 3 or over on the Schedule for Affective Disorders and Schizophrenia (SADS) suicide subscale, reported that 24 of 44 patients with mixed mania had suicidal ideation as compared with only 1 of 49 patients with pure mania. The presence of depressive symptoms amongst those of mania seems sufficient to confer a significant risk of suicidality. Goldberg et al. [18] reported that even with 3 or less depressive symptoms suicidal ideation was present in 44% of patients with dysphoric mania and that this increased to 77% in those that also fulfilled criteria for major depression.
Cassidy [19] in a large study of 316 manic or mixed subjects described motor activation, accelerated thought processes, pressured speech and decreased sleep as the most common signs and symptoms of mania with grandiosity, euphoric mood, and pressured speech significantly more common in the pure manic group. In the mixed group, dysphoric mood, mood lability, anxiety, guilt, suicidality, and irritability were found to be more common. Similarly, Goldberg [20] in a study of 183 manic bipolar I inpatients reported that overall mixedmanic patients manifested fewer manic symptoms than patients with pure mania, and that grandiosity, euphoria, pressured speech, and a decreased need for sleep were more common in the latter. Suicide was again shown to feature more commonly in mixed states. A consistent theme in reports of bipolar patients with mixed states is the finding that they have worse outcomes than pure mania [13],[21–23]. Clinically, the time to syndrome resolution is longer for mixed states than the depressive phase, which in turn is longer than the manic phase [11], [24]. Clearly, mixed states have poorer prognostic implications the underpinnings of which may be biological. For instance, as compared to patients with pure manic states patients with mixed states have higher levels of thyroid-stimulating hormone (TSH) (3.14 mU/mL versus 1.61 mU/mL) and lower levels of thyroxine (T4) (7.03 nmol/L versus 8.64 nmol/L), indicative perhaps of greater thyroid dysfunction [25].
Classifying and defining mixed states
Although DSM-IV requires the full complement of features of both mania and depression to be satisfied in order to make a diagnosis of mixed state bipolar disorder clinically there are essentially two manifestations. Perhaps the best recognized and accepted is that of manic dysphoria, in which irritable and dysphoric mood intrudes into mania. Most treatment studies involve this group. However, Swann [26] argues that the current focus on manic episodes with depressive features risks loosing sight of the clinical significance of manic features in depression. This is reflected by the wider acceptance of manic mixed states as opposed to depressive mixed states.
This converse mix involving the emergence of manic features in a dominantly depressive presentation is often more difficult to diagnose, especially as it overlaps with the concept of agitated depression [27]. Patients in this group tend to have low scores on mania rating scales and the hyperactivity they experience tends not to be goal directed [4], [28]. Consequently, Cassano et al. [29] have argued that undue diagnostic emphasis is placed on alterations in mood and that this distracts clinicians from eliciting/detecting more subtle but clinically meaningful signs and symptoms, such as changes in energy, neurovegetative symptoms and distorted cognitions, which characterize the manic or hypomanic component of such mixed presentations.
The various definitions of bipolar mixed states together form a spectrum that extends from the occurrence of depressive features within mania to the occurrence of manic features within depression, with admixtures in between. The DSM-IV defines mixed states as the concurrent presence of a full manic and depressive syndrome (see 29], highlighting the restrictive nature of the DSM-IV criteria (30]. Sato et al. [31] found that depressive mixed states were more common in bipolar than unipolar depressed inpatients. It is interest to note that the unipolar subjects with mixed states had many characteristics such as age of onset and family history of bipolar disorder in common with the bipolar group suggesting again the spectral context of mixed states.
DSM-IV criteria for a mixed episode
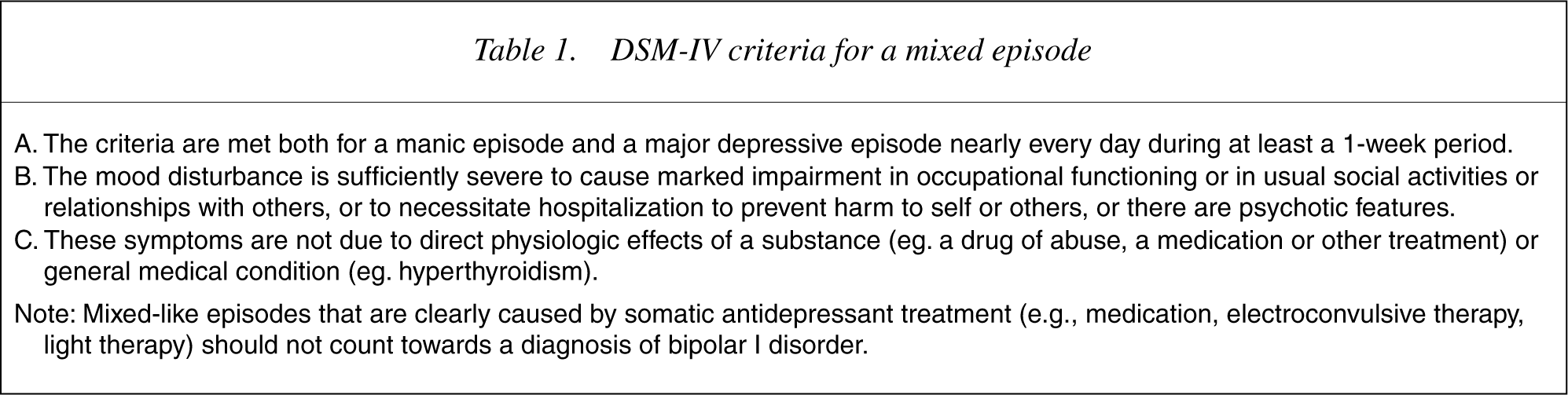
An alternative approach, proposed by Maggini [32], suggests the separation of mixed states into stable and unstable, such that the former represents a synchronous coexistence of manic and depressive symptoms, and the latter reflects a spectral relationship to rapid cycling. Others suggest links to agitated depression [2], [27], [33] by virtue of the fact that a quarter of bipolar depressed subjects have agitated depression with symptoms such as racing thoughts, pressured speech, motor activation and symptom clusters encompassing paranoia, aggression and irritability. Not surprisingly patients with such symptoms take longer to recover, receive more antipsychotic agents and are more likely to require antidepressant discontinuation, providing support for the notion that ‘unipolar’ treatment algorithms may not be the preferred modality in this group.
Going one step further Dayer et al. [34] propose that in addition to depressive and manic mixed states, there is a third state, namely that of dysphoria, on the basis of which they define two additional phenotypes. Thus in their system of classification in addition to DSM-IV mixed state, which they called type I, type IIM consists of mania with dysphoria and some depression, and type IID consists of depression with dysphoria and some mania.
Other definitions of mixed mania include that of McElroy et al. [35] who accept the presence of mania or hypomania and the concurrent presence of three or two depressive symptoms, respectively. Examining the converse Benazzi [36] has defined depressive mixed states (DMX) as a major depressive episode with two or more (DMX2), or with three or more (DMX3) simultaneous intra-episode hypomanic signs and symptoms. Applying this definition, a study of 161 outpatients revealed that DMX2 occurred in 73.1% of bipolar II, and in 42.1% of unipolar major depressive disorder (MDD), while DMX3 occurred in 46.3% of bipolar II, and in 7.8% of unipolar MDD. The most common hypomanic features described were irritability, distractibility, and racing thoughts and the figures prompted the authors to comment that adherence to current clinical definitions and derived diagnostic interview instruments would severely limit the detection of mixed states.
Applying this same definition of DMX2 to a sample of bipolar depressed subjects Benazzi noted that 81.8% had mixed features. Hypomanic symptoms again included irritability, distractibility and racing thoughts but also increased time spent in pleasurable activities, a reduced need for sleep, psychomotor agitation, grandiosity, talkativeness, and pressure of speech reflecting flight of ideas [37], [38]. Some of these symptoms are included in a definition proposed by Kukopoulos [27] in which mixed depression is a major depressive episode plus any two of the following features – motor agitation, psychic agitation or intense inner tension and racing or crowded thoughts.
Another group [39] that also applies a threshold of two symptoms describes a set of six dysphoric symptoms namely depressed mood, anhedonia, guilt, suicide, fatigue and anxiety that can occur in a mixed episode. Applying these criteria in a study of 366 manic or mixed subjects the researchers found that 21.6% of their sample was mixed, compared to 13.9% using DSM-IIIR criteria. Furthermore, mixed patients had an earlier first psychiatric hospitalization and a longer duration of illness [40]. Similarly, Akiskal et al. [41] compared diagnoses of mixed mania using either the full DSM criteria (5 or more depressive symptoms) or a threshold of two. Using the more conservative criteria, the rate of mixed mania was 6.7%, compared to 37% using the broad definition. Mixed states were characterized by female predominance and lower levels of manic symptomatology and more complex temperamental dysregulation including cyclothymic, and irritable dimensions. The authors conclude that mixed states are a common and clinically distinct form of mania, with subthreshold depressive features being the most common variety. This is broadly in keeping with Perugi's conceptualization of mixed states as the intrusion of an expansive-excited phase into a depressive temperament, or a melancholic episode intruding into a hyperthymic temperament [42]. Using a cluster analysis of a range of behavioural items, Dilsaver et al. [43] found four factors corresponding to manic activation, depressed state, sleep disturbance, and irritability/ paranoia. Further analysis separated the manic episodes into classic (predominately euphoric), dysphoric, or depressed.
Treatment implications
It has long been recognized that mixed states predict a poorer response to treatment [44]. For instance there is a large body of evidence that the response to lithium in mixed mania is poorer than in euphoric mania [23],[45–47];. In the National Institute of Mental Health Collaborative Study [48], an antimanic response to lithium was observed in 10 out of 11 patients with pure mania, compared to only 2 out of 7 patients with a manic mixed state.
Antimanic medications are considered to be necessary in the treatment of manic mixed states and in this regard valproate and carbamazepine hold preference over lithium. Post et al. [49] described a preferential response to carbamazepine in mixed mania. Freeman [50] reported that higher depression ratings in mania predicted a response to valproate. Conversely, depressive symptoms in mania predict lithium non-response [45], [51]. In general, valproate and carabamazapine have similar antimanic efficacy in mixed episodes, with varying efficacy in the treatment of the depressive component. There is also some consensus that mixed states warrant combination treatment strategies more so than other phases of the illness. However, the rapid titration of mood stabilizers is a strategy that has been reported to be associated with better outcomes in both pure and mixed mania [22].
Atypical antipsychotics also appear to be helpful in treatment of mixed states. Treatment results for mixed samples within larger trials of acute mania indicate similar efficacy [52], [53]. There are case reports [54] and open trials [55] of adjunctive olanzapine that suggest a beneficial effect. For example, in a 52-week maintenance study, in which patients who had an index manic or mixed episode were randomised to olanzapine (n = 225) or placebo (n = 136); higher relapse rates were observed following an index mixed rather than a manic episode, particularly into the depressive phase [56]. Mixed states were predictive of a depressive relapse whereas a manic index episode was predictive of relapse into mania [56]. While atypical agents are increasingly used in depressive mixed states, data in this group is urgently needed.
Electroconvulsive therapy (ECT) shows antimanic and antidepressant efficacy in the treatment of mixed states. A study by Small et al. [57] reported a greater response to ECT than to lithium with ECT alone also proving to be effective in treatment refractory mixed states [21], [58]. However, a chart review study [59] that compared depressed (n = 38), manic (n = 5), and mixed (n = 10), bipolar patients found that all three groups had a robust response but that the mixed group had longer hospital stays and needed more ECT. Thus even though mixed states may be more difficult to treat than patients with pure depression or mania, the utility of ECT is suggested. Furthermore, given the increasing realization of the limitations of antidepressants, the use of ECT in mixed states may warrant earlier consideration in clinical algorithms.
The use of antidepressants in mixed states needs to be considered. Given that depression is the predominant mood state in bipolar disorder [60], [61] it is not surprising that antidepressants are widely used [62]. However, antidepressants can increase mood instability in vulnerable patients [63], [64] and precipitate mixed states [65], [66]. Furthermore, certain antidepressant adverse events such as increased agitation and panic, and worsening of suicide and psychosis may be more likely in mixed states [27]. However, their role remains the subject of debate, as many researchers still believe that antidepressants have a role in the long term management of bipolar disorder [67–70]. Their role in maintenance is however, not supported by any positive randomised controlled data, and their role in induction of cycling and mixed states is increasingly a focus of concern [71].
Discussion
Despite the high prevalence of mixed states, and the fact that they are often treatment refractory, there is a paucity of controlled data to inform treatment [28]. As regards clinical management many questions remain unanswered. Mixed states need to be examined specifically as opposed to extrapolating from subsets of mixed patients within studies of manic patients. Within mixed states research most treatment studies have focused on mixed mania, and it therefore remains unclear how much is applicable to patients with depressive mixed states. Depressive mixed states are however, more complex to assess. Furthermore, while mania and manic mixed states share a relatively similar therapeutic algorithm, there is increasing consensus that depressive mixed states may need to be treated differently, particularly with regard to the use of antidepressants. This latter group needs to be investigated prospectively with a view to resolving the risk benefit ratio of antidepressants and antidepressant mood stabiliser combinations as opposed to the use of mood stabilizers alone. For instance, the concept of stabilizing mood from below as opposed to above baseline, proposed by Ketter [72], suggests that therapeutic agents differ with lamotrigine for example operating from below and valproate or atypical agents from above. Trials examining the specificity of these agents in depressive and manic mixed states would be of great theoretical and practical interest and would provide much more relevant and informative clinical guidelines. However, before any of this can be achieved, a requirement is a consensus regarding the definition and operationalization of criteria for manic and depressive mixed states. Without this first step bipolar mixed states will continue to be missed and poorly understood.