
Abstract
School bullying is associated with high levels of distress in childhood, and the cross-sectional evidence for the ill effects of school bullying on children's mental and physical health is strong. Bullied children are often socially anxious, and their lives are characterized by feelings of loneliness, depression and low self-esteem [1]. School bullying is also associated with many of the common health complaints of childhood including headaches, abdominal pain, nausea, recurrent upper respiratory tract infections, sore throats and palpitations [2–4]. Reflecting the impact of bullying on overall quality of life, bullied children and adolescents report poorer scores on health-related quality of life (HRQoL) questionnaires [5,6].
There is emerging evidence that the effects of school bullying can have long-lasting effects on emotional functioning. In a longitudinal study of a population sample of Finnish children born in 1981, bullying during the early school years was found to be predictive of psychiatric disorder in early adulthood even after controlling for childhood levels of psychiatric symptoms [7]. Adults who recall school bullying also experience higher rates of emotional disorders. Gladstone et al. found that one-quarter of adults surveyed in an outpatient depression clinic reported being bullied in childhood and they experienced higher rates of comorbid anxiety [8]. Lund et al., from a general population survey, found that adult reports of bullying at school were associated with higher levels of depressive symptoms and a significantly increased risk of being diagnosed with depression between ages 31 and 51 years [9]. This suggests that school bullying could be a preventable cause of mental health problems in the adult population at least into mid-life.
The findings from these studies suggest that school bullying could be aetiologically significant in increasing the risk of adult depression and anxiety. It is not known, however, whether the psychosomatic symptoms and poorer HRQoL experienced by bullied children also persist into adulthood. The current study sought to extend the research into school bullying by surveying HRQoL and past histories of peer victimization among a representative sample of South Australian adults. Specifically we hypothesized that those adult respon dents who reported having been bullied at school would experience both poorer physical and mental health compared with adults who did not report having been bullied at school.
Methods
Data were collected in the South Australian Health Omnibus Survey (HOS). The HOS sampling procedures have been described in detail previously [10,11] but, briefly, a large representative sample of South Australians aged ≥15 years is surveyed in face-to-face interviews. In Autumn 2008, 4830 households were sampled and a response rate of 62.8% was achieved. In the present study, data from participants in the HOS who were ≥ 18 years of age and who were no longer in school (n=2833) were used in the analyses.
Self-reported bullying at school was determined from the following question: ‘When you were at school did you experience traumatic bullying by peers that was particularly severe, for example, being frequently targeted or routinely harassed in any way by ‘bullies’?’ Responses to this question were coded as no = 0, not bullied; and yes= 1, bullied.
Physical and mental health were measured using the Medical Outcomes Study Short Form 36-item health survey questions (SF-36). The SF-36 has eight subscales (physical function, role physical, bodily pain, general health, vitality, social function, role emotion, mental health) and two summary components (one each for physical and mental health). For ease of comparison, normed t-scores (mean = 50, SD=10) of the SF-36 sub-scales were used in analyses. Data were weighted according to the algorithms for use with the South Australian population [12].
Analyses were performed using Stata/IC version 10.0 (Statacorp, College Station, TX, USA). Survey data were weighted by gender, age and demographic variables (country of birth, marital status, educational attainment and household income) in order to be representative of the South Australian population [13]. Some small discrepancies in frequency and percentage totals reported in the tables occur due to rounding in the presence of weighted data. Logistic regression was used to identify the independent predictors of the characteristics of adults reporting that they had experienced school bullying and multiple regression was used to identify the impact of school bullying on Mental and Physical health SF-36 Component Summary scores.
Ethics approval for including the bullying survey question in the HOS was provided by the South Australian Department of Health–Human Research Ethics Committee.
Results
Overall, 18.7% of participants reported recalling bullying at school. Table 1 shows the percentage of persons who reported having experienced bullying at school vs demographic variables. Higher proportions of younger people, those born in Australia and people who had never married reported that they had experienced bullying at school.
Reporting of bullying vs demographic variables
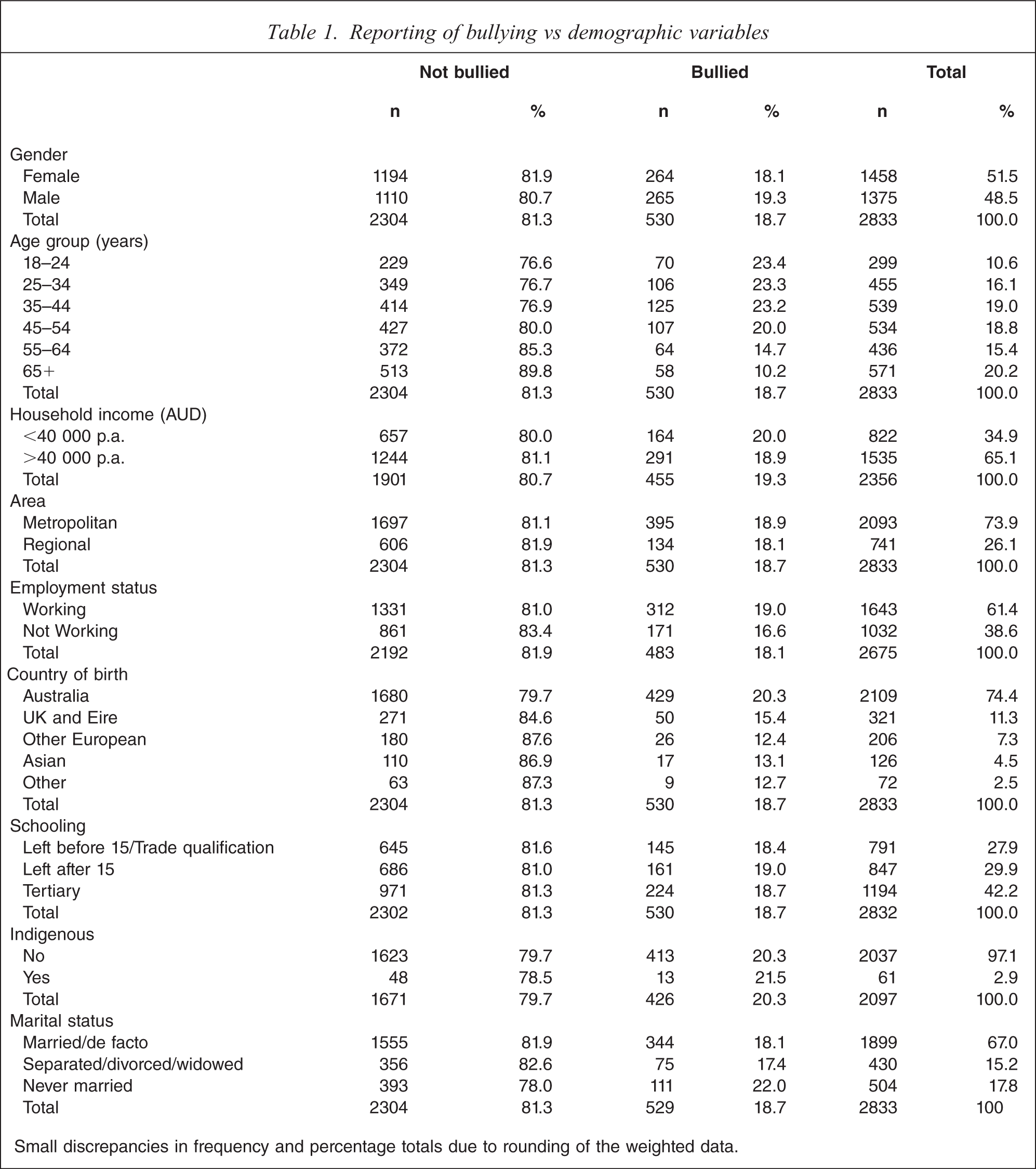
Small discrepancies in frequency and percentage totals due to rounding of the weighted data.
The results from a series of univariate logistic regressions (Table 2) showed that those aged 55–64 years (odds ratio (OR) = 0.56, 95% confidence interval (95%CI) = 0.37–0.85) and ≥65 years (OR=0.37, 95%CI=0.24–0.56) were approximately half as likely to report recalling that they were bullied at school compared with respondents aged 18–24 years of age. Respondents born in the UK and Eire (OR=0.71, 95%CI=0.51–1.0) or other European countries (OR=0.56, 95%CI=0.35–0.87) were also less likely to report having been bullied at school compared with Australian-born respondents. In a multivariate analysis that included both variables (age group and country of birth) simultaneously, both variables retained their significance.
Predictors of self-reported experience of school bullying
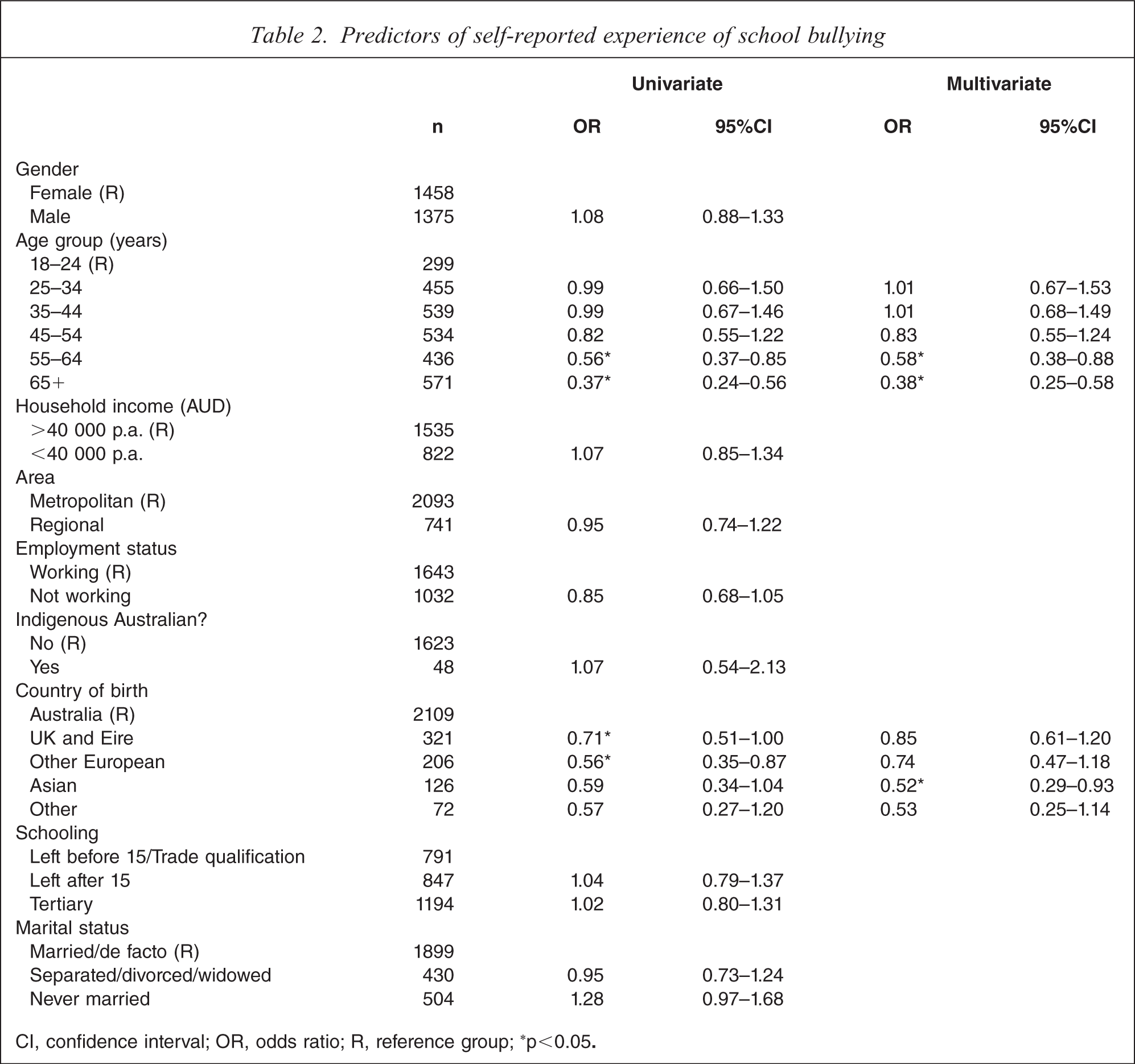
CI, confidence interval; OR, odds ratio; R, reference group; ∗p<0.05.
The mean scores on SF-36 subscales were compared between those who reported being bullied and those who had not (Table 3). Participants who reported having been bullied had statistically significantly poorer outcomes on seven of the eight SF-36 subscales: bodily pain, role physical, general health, vitality, social function, role emotion and mental health.
SF-36 subscales as a function of having experienced bullying
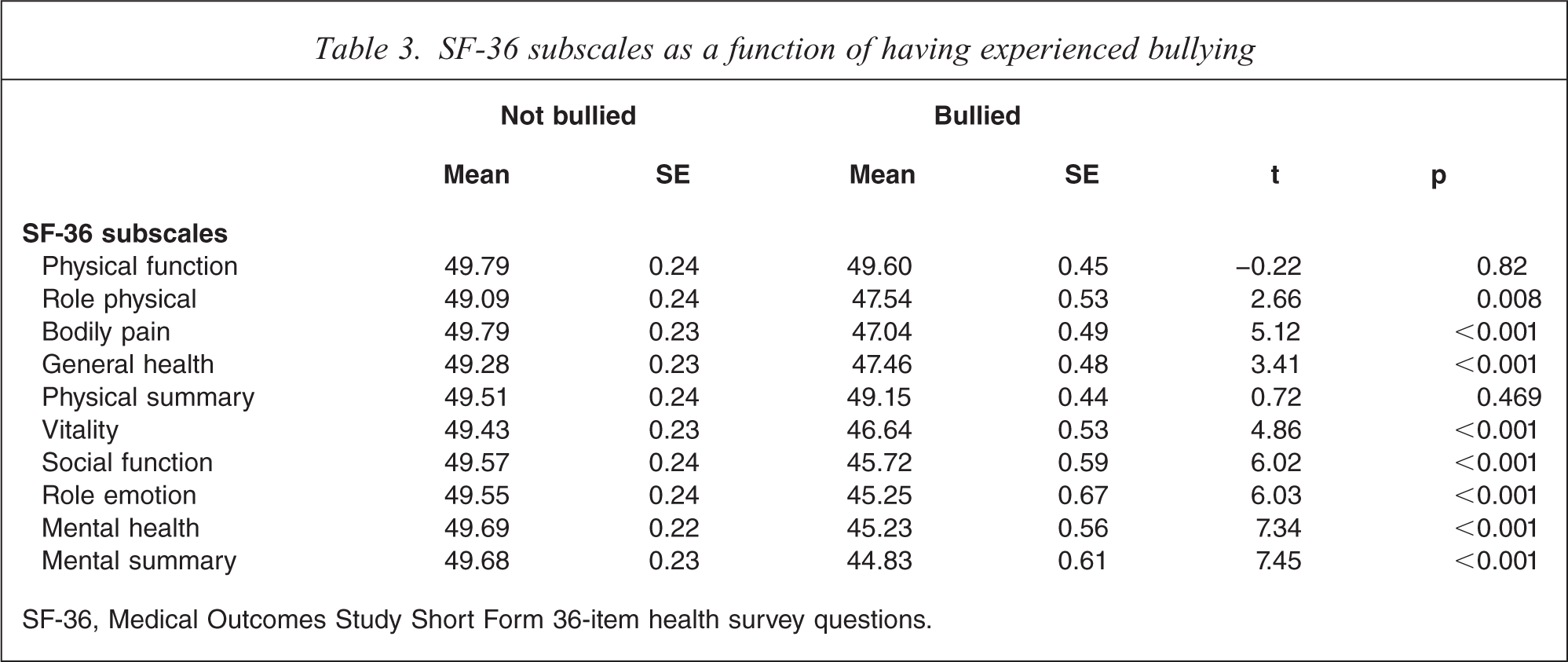
SF-36, Medical Outcomes Study Short Form 36-item health survey questions.
The negative effects of bullying on Mental Health Component Summary Scores was assessed in a multivariate model adjusting for demographic factors associated with mental health (Table 4). A series of univariate analyses showed that age, gender, income, employment, education, marital status and identification as an Indigenous Australian were related to Mental Health Component Summary Scores. These variables were simultaneously entered into a multiple regression in addition to the variable ‘Bullied’. After adjusting for demographic variables the effect of bullying remained significantly associated with poorer levels of self-reported mental health (t=−5.58, p<0.001).
Factors associated with SF-36 Mental Health Component Summary Scores
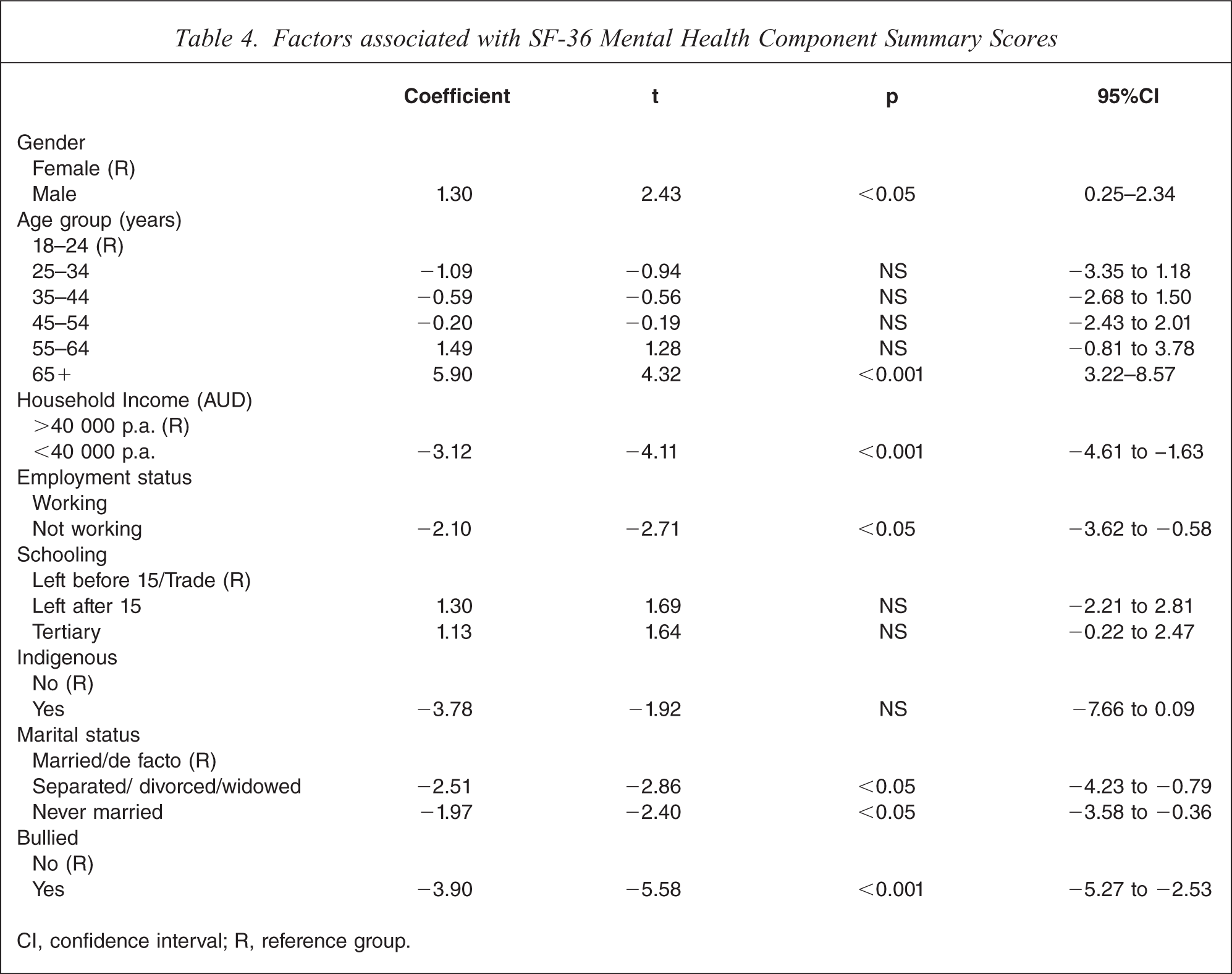
CI, confidence interval; R, reference group.
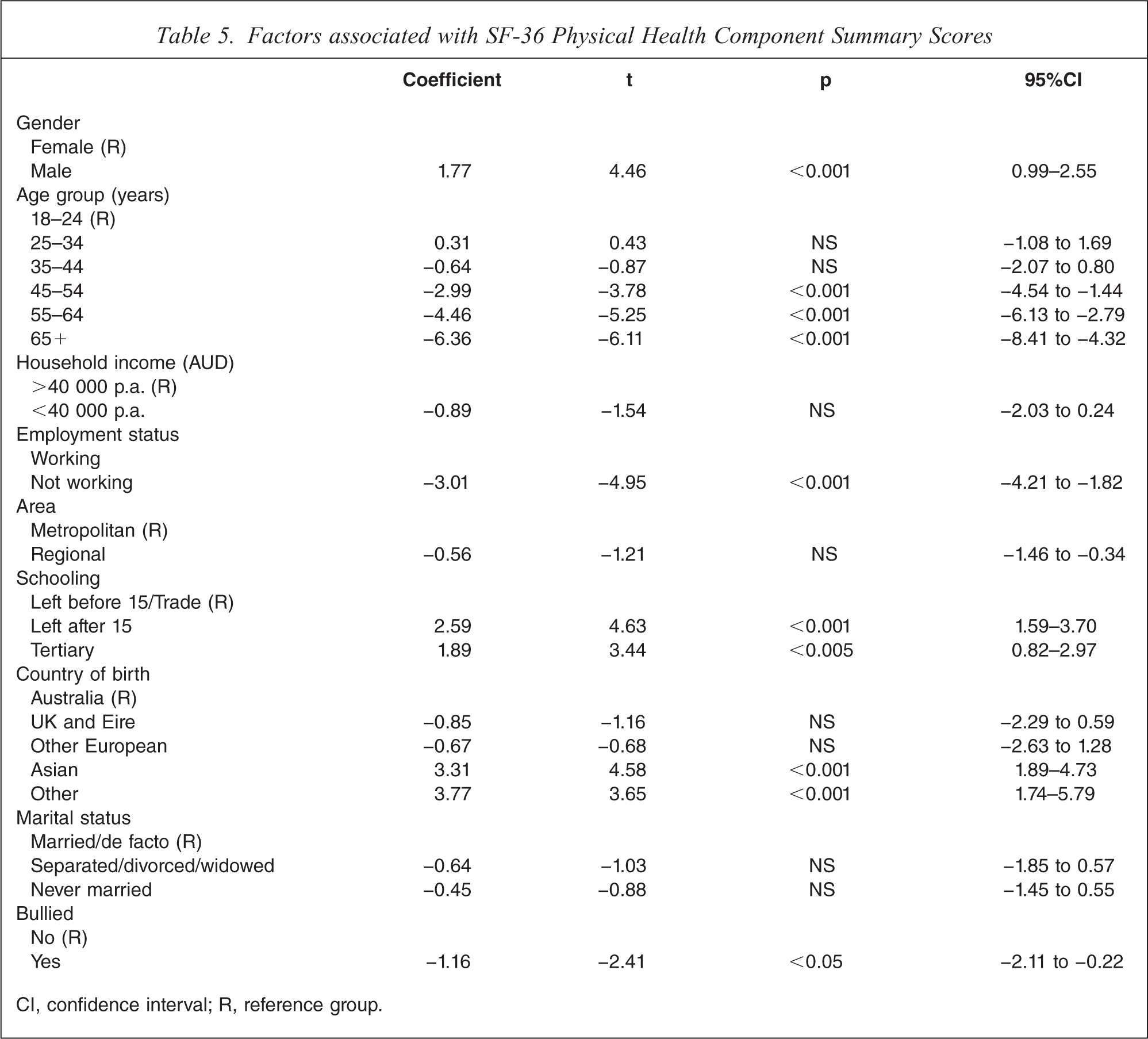
The effects of bullying on Physical Health Component Summary Scores was assessed in a multivariate model adjusting for demographic factors (Table 5). A series of univariate analyses showed that gender, region, age group, household income, employment status, country of birth, schooling and marital status were related to Physical Health Component Summary Scores. These variables were simultaneously entered into a multiple regression in addition to the variable ‘Bullied’. After adjusting for demographic variables (and in particular the variable age group), the effect of bullying was significantly associated with poorer levels of self-reported physical health (t = −2.41, p<0.05).
Factors associated with SF-36 Physical Health Component Summary Scores
CI, confidence interval; R, reference group.
Discussion
School bullying is common in the community and in the present survey nearly one-fifth of South Australian adults reported recalling experiences of bullying while they were at school. The results from the present study indicate that reports of early exposure to bullying were associatedwith an increased risk of emotional and psychosomatic disorders. Adults recalling school bullying experienced more psychiatric symptoms and greater impairment across all of the SF-36 mental health scales. They reported more anxiety and depressive symptoms such as feeling nervous, downhearted and depressed, together with low vitality and poorer functioning due to emotional problems. Although several demographic factors (gender, income, employment status and marital status) had significant relationships with overall mental health, the relationship between school bullying and mental health remained significant after adjusting for demographic variables.
It is only recently that systematic evidence is becoming available to estimate the strength of the association between past histories of school bullying and adult adjustment. These studies have been mostly restricted to small clinical samples but they do show increased rates of mid-life depression and higher levels of depressive symptoms for adults who recall being bullied at school [6,9,14]. The present findings extend this line of research and indicate that reports of school bullying are associated with significant adult mental health problems in the general community.
As far as we can determine, the current study is the first to examine the effects of school bullying on physical health as part of a standard assessment of HRQoL in the adult population. This is an important step because childhood studies have repeatedly found that school bullying is linked to higher rates of psychosomatic complaints. The present survey found poorer adult physical health in three of the four physical health subscales of SF-36: General Health, Role Physical and Bodily Pain. This pattern of increased symptoms of pain and frequent sickness is consistent with reports from childhood studies in which higher levels of headaches, abdominal pain and frequent illness are thought to be stress-related conditions secondary to the trauma of the bullying.
The ability of adults who reported school bullying to accomplish specific everyday physical functions such as climbing stairs, carrying groceries or heavy lifting, however, was not significantly affected. Again this is similar to the childhood pattern in which it is more common to find mild to moderate increases in physical symptoms rather than severe disability. The differences between the bullied and non-bullied groups on the HRQoL sub-scales were statistically significant but they were not large enough in absolute terms (around 2 points) to be above the clinical threshold for the SF-36 scales (>3 points different) [15].
The present study found that younger respondents were more likely to report school bullying than older respondents. This could indicate that the frequency of bullying has increased over the second half of the 20th century. Alternatively, younger respondents might have a broader interpretation of the concept ‘traumatic bullying’ and label a more extensive range of negative peer behaviour as bullying. Given the considerable public health focus on the issue in recent decades it is also possible that younger respondents feel more comfortable (or less stigmatized) reporting that they have been bullied. Further research is required to better understand the effect of age on the reporting of specific kinds of bullying behaviour.
A major limitation of the present study is that it is cross-sectional and it is not possible to determine the direction of causality between reports of past victimization and adult HRQoL. It is possible that reports of past bullying could be affected by current mood rather than the reverse. The accuracy of retrospective recall, however, has been examined in some depth in other studies and there is reasonable support for the validity of adult recall. Brewin et al. reviewed the evidence for retrospective reports and, on the basis of both experimental and naturalistic studies, concluded that recall of significant past events is not greatly affected by mood state [16]. In a longitudinal study Rivers found that retrospective recall of bullying was reasonably stable and consistent over time [17].
Further study of school bullying and adult health and well-being seems justified in the light of the findings of this population survey. School bullying could represent a preventable cause of increased adult anxiety, depression and stress-related health problems. This line of research might be useful in the investigation of the long-term potential for anti-bullying programs to improve health and well-being across the lifespan. The current study was part of a large population survey that covered a wide range of health-related behaviours. Given the restrictions on the length of the survey, the amount of information available about school bullying is limited and did not cover the full range of bullying behaviour. The survey used an item from a clinical study of school bullying among depressed outpatients [8], which was designed to capture more severe forms of peer victimization. Future studies could explore the full extent of victimization and involvement in bullying behaviour, including more specific information about the responses to bullying such as reactive aggression; involvement with bully/victim behaviour; and the overall quality of peer relationships.
Footnotes
Acknowledgement
This study was supported by the Australian Government's Primary Health Care Research, Evaluation and Development (PHCRED) Strategy.