
Abstract
Background:
Perception of loneliness has been identified as the strongest predictor of health-related quality of life assessed with the Assessment of Quality of Life-4D in people with psychotic disorders. We aimed to establish contributors to perceived loneliness, and ascertain the mediating role of loneliness in the relationship between identified contributors to loneliness and other known predictors of health-related quality of life with health-related quality of life.
Methods:
Data for 1642 people collected as part of the 2010 Australian National Survey of Psychosis were analysed. Health-related quality of life was assessed using the Assessment of Quality of Life-4D, and loneliness through a single-item five-level categorical variable. To identify independent contributors to loneliness, a statistical model was constructed with reference to a theoretical model comprising 23 variables. A predictive model with health-related quality of life as the dependent variable was then developed and tested to assess the mediating role of loneliness.
Results:
Nine contributors to loneliness were found (social dysfunction, experienced stigma, contact with friends, diagnosis, depressive symptoms, anxiety, mental health service utilisation, arthritis and traumatic events in childhood), with social dysfunction the strongest. In the prediction of health-related quality of life, all contributors to loneliness were partially mediated through loneliness (except service utilisation) as were negative symptoms and use of psychotropic/anticholinergic medications.
Conclusion:
Assuming a plausible causal model of mediation, loneliness was found to have direct and indirect effects on health-related quality of life in people with psychotic disorders. Findings add impetus to efforts to develop and trial strategies aimed at reducing loneliness in this population, and, in turn, improving their health-related quality of life.
Perception of loneliness, a subjective experience (Cacioppo and Patrick, 2008; Rokach, 2012) influenced by personal and situational variables (Rokach, 2012), has been defined as the individual’s feeling of social isolation regardless of the number of people around them. Loneliness is thus an unmet need for meaningful social connections (Cacioppo and Patrick, 2008), and the second most important challenge, after financial problems in people with psychotic disorders (Morgan et al., 2012). Loneliness is associated with an increased risk of physical health problems in people with psychotic disorders, such as metabolic syndrome (Badcock et al., 2019), and with the poor mental health (MH) of this population. Further, loneliness is a mediator between childhood abuse and psychiatric disorders, including psychosis (Shevlin et al., 2015), and between internalised stigma and depression in people with psychotic disorders (Świtaj et al., 2013). Perception of loneliness is the strongest of the seven predictors of health-related quality of life (HRQoL) in people with psychotic disorders, and one of the two not mediated by global functioning (Nevarez-Flores et al., 2021a). Given the importance of loneliness to HRQoL in this population, identifying factors/characteristics that are mediated through loneliness should enable the development of strategies aimed at reducing the perception of loneliness and improving HRQoL.
The factors contributing to perceived loneliness in people with psychotic disorders have undergone limited investigation. Psychosocial variables such as social support, and internalised stigma, along with socio-occupational functioning and higher numbers of psychiatric hospitalisations have been found to contribute to feelings of loneliness in this population (Chrostek et al., 2016). Self-efficacy, self-esteem, social isolation and community integration have also been found to be contributors to loneliness in people with schizophrenia (Shioda et al., 2016). Lim et al. (2018) have proposed a theoretical model of loneliness focussed on psychological and social factors, while Badcock et al. (2015) included symptoms as the main predictors of loneliness in a model that reported that ongoing disturbance of thought and loss of pleasure were significantly associated with loneliness. A possible mediating role for loneliness between sociodemographic and clinical characteristics (particularly depressive symptoms) of this population and their HRQoL has also been postulated (Nevarez-Flores et al., 2021a).
Whether physical conditions contribute to loneliness in people with psychotic disorders is unknown, but worth considering in view of relationships identified in the general population. For example, people with arthritis who suffered continuous debilitating chronic pain considered that loneliness limited their personal growth and appreciation of life, with intense pain a key element to their experience of loneliness (Rokach et al., 2006).
To obtain a holistic assessment of potential contributors to loneliness in people with psychotic disorders and their association with HRQoL, this study aims to (1) establish a model of contributors to loneliness based on a suite of sociodemographic and clinical characteristics derived from the literature and previous research, and (2) ascertain the mediating role of loneliness in the relationship between identified contributors to loneliness and other known predictors of HRQoL with HRQoL in this population (Figure 1). It was hypothesised that (1) social factors would be the strongest contributors to the perception of loneliness, (2) presence of symptoms (particularly depression) will contribute to perceived loneliness, and (3) loneliness would attenuate the effect of some variables on the HRQoL of people living with psychosis, particularly depressive symptoms (Nevarez-Flores et al., 2021a).
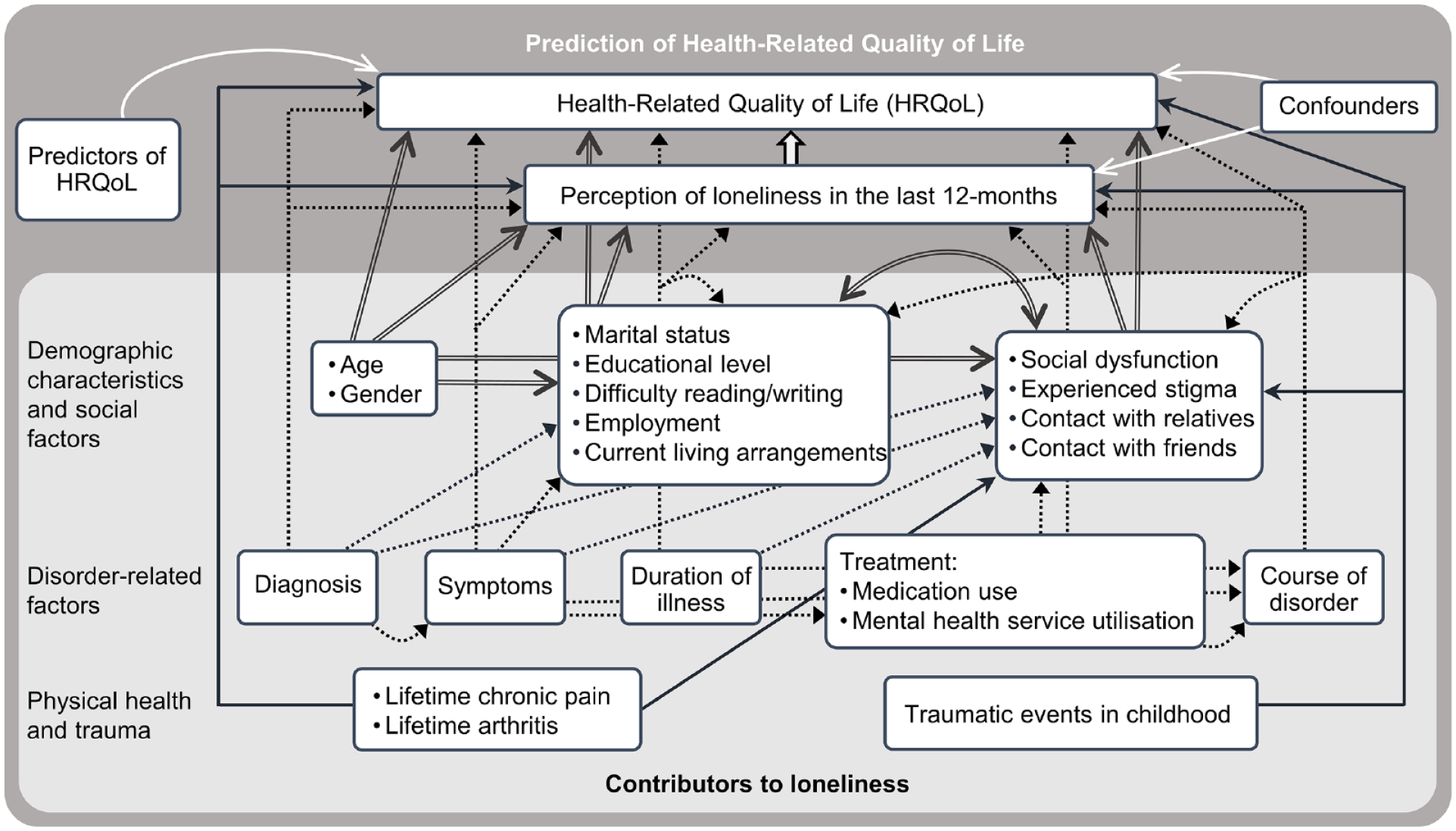
Theoretical model for contributors to perception of loneliness and loneliness’ mediating effect on the path to HRQoL.
Method
Participants
Participants were interviewees in the 2010 Australian National Survey of Psychosis (Morgan et al., 2012, 2014) (n = 1825 of 7955) who met the International Classification of Diseases 10th revision (ICD-10) criteria for a psychotic disorder (n = 1642). The survey covered about 10% of the Australian population aged 18–64 years, was undertaken at seven sites across five Australian states and employed a two-phase design: screening (March 2010) and interviews (April 2010 to March 2011). The interview comprised 32 modules and over 1500 items (see Supplemental Material) and was an enhanced version of the schedule for the first national survey of psychosis undertaken in 1997–1998 (Jablensky et al., 1999, 2000). Consistency in the schedule between the first and second national surveys enabled assessment of change over time. Further, questions from the 2007 National Survey of Mental Health and Wellbeing (Burgess et al., 2009; Slade et al., 2009) and other national surveys facilitated comparison with population norms.
Each interview was conducted face to face with participants. The interviewers were experienced MH professionals, who were trained in the use of the survey instruments and to take standardised physical measures (e.g. waist circumference and blood pressure). Questions were administered in a set order, with each interview typically lasting between 3 and 4 hours. The duration of the interview depended on the participant’s disposition to talk, and the number of extent of pauses taken by the participant.
All procedures contributing to this work complied with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. These procedures were approved by the institutional human research ethics committee at each study site. Written informed consent was obtained from all subjects. See Morgan et al. (2012, 2014) for complete information about methodological design.
Measures, sociodemographic and clinical variables
HRQoL was assessed with the Assessment of Quality of Life (AQoL)-4D (Hawthorne et al., 1999), an instrument constructed using psychometric principles (Richardson et al., 2014). The AQoL-4D has been validated for both self and interviewer administration (Hawthorne et al., 2001) and for use in people with psychotic disorders (Herrman et al., 2002). The AQoL-4D has also been found to be robust and sensitive in this population (Neil et al., 2018; Nevarez-Flores et al., 2021b). The AQoL-4D was administered by the interviewer. The instrument comprises four dimensions: independent living, social relationships, mental health and senses, each with three questions pertaining to the last 7 days. Responses across these 12 questions are used to derive a preference-based measure of health status, or ‘utility value’ which can range from −0.04 for states worse than death to 1.00, full health.
Perception of loneliness and social factors were assessed using single questions derived from previous Australian surveys (Morgan et al., 2011, 2012). Perception of loneliness was determined through the question ‘In the last 12 months have you felt lonely?’. Participants had a choice of five responses, I have (1) plenty of friends, not lonely, (2) friends, lonely occasionally, (3) some friends but lonely for company, (4) socially isolated and lonely and (5) not known.
Social factors comprised social dysfunction, experienced stigma, contact with friends and contact with relatives, each in the last 12 months. Social dysfunction was a rating made by interviewers based on participant descriptions of the extent of their involvement in social activities, relationships and contact with friends and family and frequency of time spent alone. Experienced stigma was determined through the question ‘In the last 12 months have you experienced stigma or discrimination because of mental illness?’. Any contact with friends and any contact with relatives were each assessed according to the frequency of contact in the last 12 months.
Demographic characteristics included in this study were age, gender, marital status, education level, employment status, participant’s current living arrangements and difficulty in reading/writing.
Disorder-related factors encompassed diagnosis of a psychotic disorder according to the ICD-10; number of negative symptoms in the last 12 months assessed using the items of the Carpenter deficits syndrome (Kirkpatrick et al., 1989), but without attribution; presence of positive symptoms and depressive symptoms in the last 12 months assessed with the Diagnostic Interview for Psychosis (Castle et al., 2006); a general rating of anxiety assessed through the question ‘In the last 12 months have you had an attack of fear or panic when all of a sudden you felt very frightened, anxious, or uneasy?’; duration of illness in years; course of disorder; treatment including the number of psychotropic (antipsychotics, mood stabilisers, antidepressants and anxiolytics) and anticholinergic medications used in the 4 weeks prior to the interview; and MH service utilisation, a 7-level hierarchy of MH services used in the last 12 months: inpatient admissions, specialised emergency services (e.g. emergency psychiatric services delivered face to face or by telephone, and crisis care home visits), presentation to an emergency department with an MH problem, outpatient services, community MH services, attendance at a general practitioner for MH issues and ‘non-specified services’, a category for participants not included in previous groups.
Physical health problems considered as potential contributors to the perception of loneliness were lifetime arthritis and chronic back, neck or other pain diagnosed by a doctor and self-reported during the interview.
Trauma refers to distressing or traumatic events in childhood other than separation/divorce of parents or loss of a parent, sibling or close relative.
Predictors of HRQoL
Predictors of HRQoL were determined in an earlier study that utilised the same dataset (Nevarez-Flores et al., 2021a), and comprised participant’s current living arrangements, number of negative symptoms, number of psychotropic and anticholinergic medications use, course of disorder and lifetime history of chronic pain, as well as global functioning and lifetime history of cardiovascular disease (CVD). Global functioning was assessed with the Personal and Social Performance scale (PSP) (Morosini et al., 2000).
Statistical methods
For ascertaining contributors to perception of loneliness, a multivariate regression model for perceived loneliness (the dependent variable) was constructed by means of a selection strategy committed to the identification of independent contributors to loneliness. Independent variables were chosen a priori in agreement with psychiatric and other evidence as presented in the introduction, and our previous research (Nevarez-Flores et al., 2021a). Variables were then organised into groups of related variables (Figure 1).
Purposeful selection from the large suite of possible covariates identified in the theoretical model was undertaken through a three-stage model building process. First, univariate associations between each independent variable and loneliness were tested. A relatively stringent threshold of p < 0.05 was chosen to test for univariable association, given the large size of our dataset. Next, variables that reached statistical significance were modelled in groups of related variables as per the theoretical model. Non-significant variables in these models containing related variables were excluded. Finally, retained variables were tested as independent contributors to perception of loneliness in a composite model using ordinal logistic regression. Two possible alternatives for fitting constraints to the more general multinomial regression model were tested, with the proportional odds model (Kirkwood and Sterne, 2003) found to provide a better fit to the data.
Mediation analysis aims to estimate the proportion of the effect of a factor of interest on a dependent variable that acts through another intermediate variable. This can be done by observing the amount that the total effect of the factor of interest in a model is attenuated by once the model is adjusted for the intermediate variable. For estimating the mediating effect of loneliness in the relationship between HRQoL and sociodemographic and clinical characteristics, a series of multiple linear regression analyses were modelled, with HRQoL as the dependent variable for each. Independent variables comprised contributors to loneliness resulting from the preceding analysis, other identified predictors of HRQoL (not identified as contributors to loneliness) (Nevarez-Flores et al., 2021a) and confounders of the association between loneliness and HRQoL (for valid estimation of direct effects). To estimate the proportion of each effect mediated through loneliness, loneliness was included in the second (final) model following the specifications of Baron and Kenny (1986). The sample with complete data for the final model was used for both models to enable valid comparison. Records for participants with one or more missing values were excluded from the analyses (<7% of included participants). In a sensitivity analysis, all models and mediation calculations were re-run with these missing data imputed using chained equations (50 imputed datasets). Statistical analyses were conducted using the statistical package Stata 15.0.
Results
Sociodemographic and clinical characteristics of the 1642 participants with a psychotic disorder are provided in Supplemental Material Table S1. Nearly two-thirds of participants were male and over half had the diagnosis of schizophrenia. On average, participants were 38 years old and their HRQoL was 0.50, half the maximum achievable value. Nearly one-fifth of the participants had plenty of friends and did not experience perceived loneliness, and just over one-fifth described themselves as socially isolated and lonely.
Of 23 variables tested for univariate associations with loneliness, 19 had significant associations (Supplemental Material Table S2) and were included in further analysis. Excluded variables were the level of education (p = 0.05–0.82), difficulty reading/writing (p = 0.17), employment (p = 0.12–0.82) and contact with relatives (p = 0.14–0.40). For the 19 variables with significant associations, three models of related variables according to the theoretical model (Figure 1) were tested for multivariate associations. Eight variables were not significantly associated and excluded from further analysis: age (p = 0.53), gender (p = 0.07), marital status (p = 0.08–0.85), current living arrangements (p = 0.14–0.77), positive symptoms (p = 0.66), illness duration (p = 0.10), number of medications used (psychotropics/anticholinergics) (p = 0.36–0.66) and course of disorder (p = 0.08–0.48).
To ascertain contributors to loneliness, the remaining 11 variables were included in a composite model, with nine significantly associated with loneliness. Variables with an independent effect on loneliness were social dysfunction, experienced stigma, contact with friends, two diagnoses (schizoaffective disorder and depressive psychosis), two MH service utilisation experiences (inpatient admission and specialised emergency services), depressive symptoms, anxiety, arthritis and traumatic events in childhood (Table 1). Variables without an independent effect were the number of negative symptoms (p = 0.05–0.86) and chronic pain (p = 0.78). The McFadden pseudo-R2 for this model is 13%.
Final model of contributors to perception of loneliness (n = 1544).
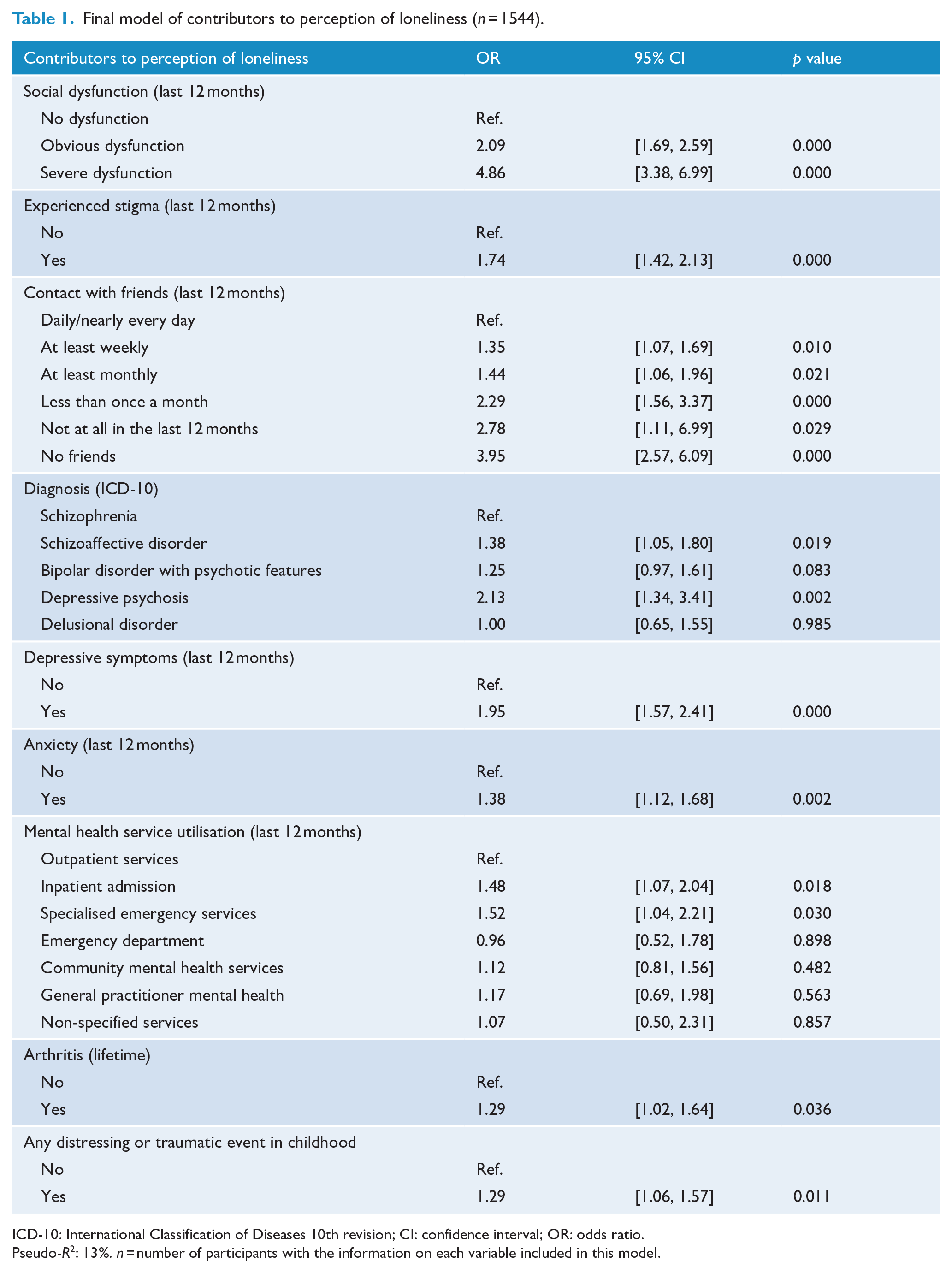
ICD-10: International Classification of Diseases 10th revision; CI: confidence interval; OR: odds ratio.
Pseudo-R2: 13%. n = number of participants with the information on each variable included in this model.
When combining contributors to loneliness (none of which were known independent predictors of HRQoL) with the seven known predictors of HRQoL other than loneliness, these 16 variables explained 40% of the variance in HRQoL (Table 2). Inclusion of perception of loneliness increased the variance explained to 49%, and led to a decrease in the total effect on HRQoL for 10 variables. Variables not mediated by loneliness were global functioning, current living arrangements, MH service utilisation, course of disorder, chronic pain and CVD (Table 2).
Mediation analysis (n = 1532).
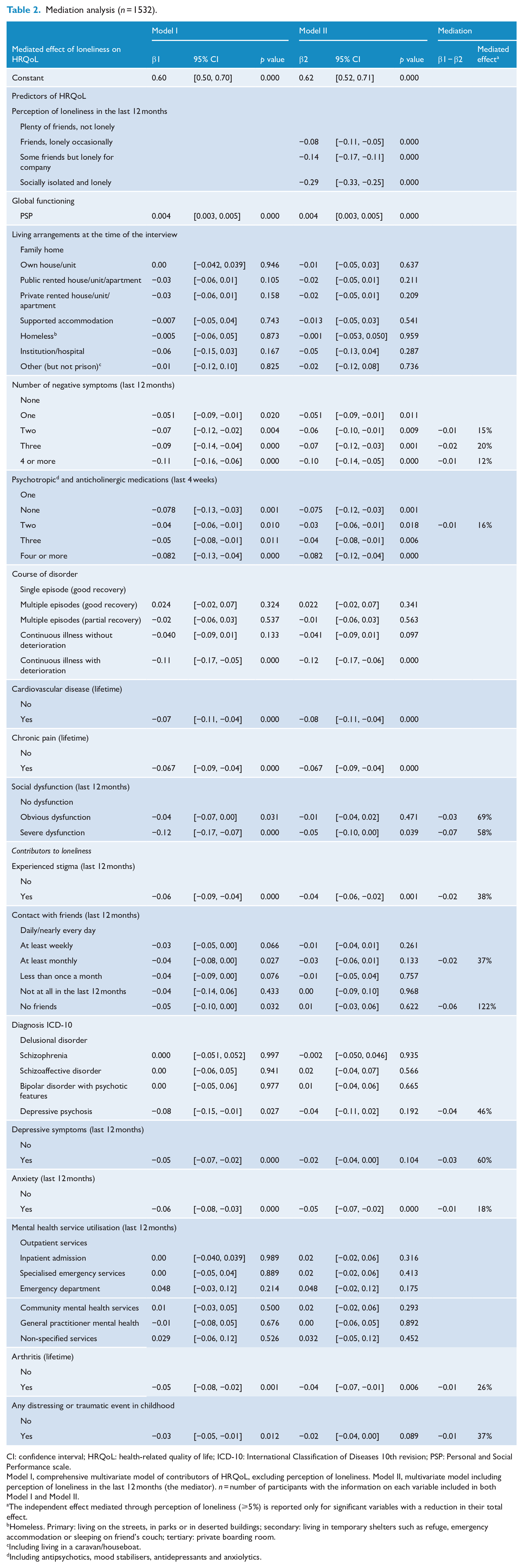
CI: confidence interval; HRQoL: health-related quality of life; ICD-10: International Classification of Diseases 10th revision; PSP: Personal and Social Performance scale.
Model I, comprehensive multivariate model of contributors of HRQoL, excluding perception of loneliness. Model II, multivariate model including perception of loneliness in the last 12 months (the mediator). n = number of participants with the information on each variable included in both Model I and Model II.
The independent effect mediated through perception of loneliness (⩾5%) is reported only for significant variables with a reduction in their total effect.
Homeless. Primary: living on the streets, in parks or in deserted buildings; secondary: living in temporary shelters such as refuge, emergency accommodation or sleeping on friend’s couch; tertiary: private boarding room.
Including living in a caravan/houseboat.
Including antipsychotics, mood stabilisers, antidepressants and anxiolytics.
Variables mediated through loneliness were all partially mediated to varying extents. The greatest mediation was observed in the variable contact with friends for the group with no friends. The second highest level of mediation was for obvious social dysfunction, while severe social dysfunction had the fourth highest level of mediation, just after depressive symptoms (Table 2).
In sensitivity analyses using imputed data, coefficients and p values were largely identical. This is unsurprising in view of the fact that no one particular variable had a level of missingness of more than 1.6%. In univariable analyses, all differences in coefficients and p values were smaller than 1%, and no variable selection changed as a result. In multivariable models for loneliness, the highest level of difference in a coefficient was approximately 10%, but the majority of coefficients and p values were within 1%. No p value changed enough to move across the 0.05 significance threshold and variable selection was unaffected. In the mediation analysis, there was no change to any coefficient greater than 0.1%. This resulted in identical percentages of effects mediated.
Discussion
Based on preliminary searches of the scientific literature and subsequent searches (December 2021) conducted in PubMed and Google Scholar, our study is the first to seek to establish contributors to perception of loneliness in people with psychotic disorders in contact with treatment services, not limited to inpatient care. This assessment is based on the largest and most comprehensive known model that includes demographic and psychosocial factors, disorder-related factors, physical conditions and traumatic events in childhood. Our study is also the first study to ascertain the mediation effect of perception of loneliness along the path towards achieving HRQoL in this population. Nine of the 23 variables tested were found to be independent contributors to loneliness: social dysfunction, experienced stigma and contact with friends, each over the last 12 months, diagnosis, MH service utilisation in the last 12 months, depressive symptoms, anxiety, lifetime arthritis and traumatic events in childhood. As hypothesised, social factors were found to be the strongest contributors to loneliness, particularly social dysfunction and contact with friends. The finding that depressive symptoms contribute to loneliness was as hypothesised. When the mediating effect of loneliness was tested, over half of the variables were partially mediated through loneliness in their relationship with HRQoL including depressive symptoms, as hypothesised. Variables not mediated through loneliness were global functioning, current living arrangements, MH service utilisation, course of disorder and lifetime histories of chronic pain and CVD (Figure 2). It was expected that CVD would not be mediated, given it was not related to loneliness in study participants.
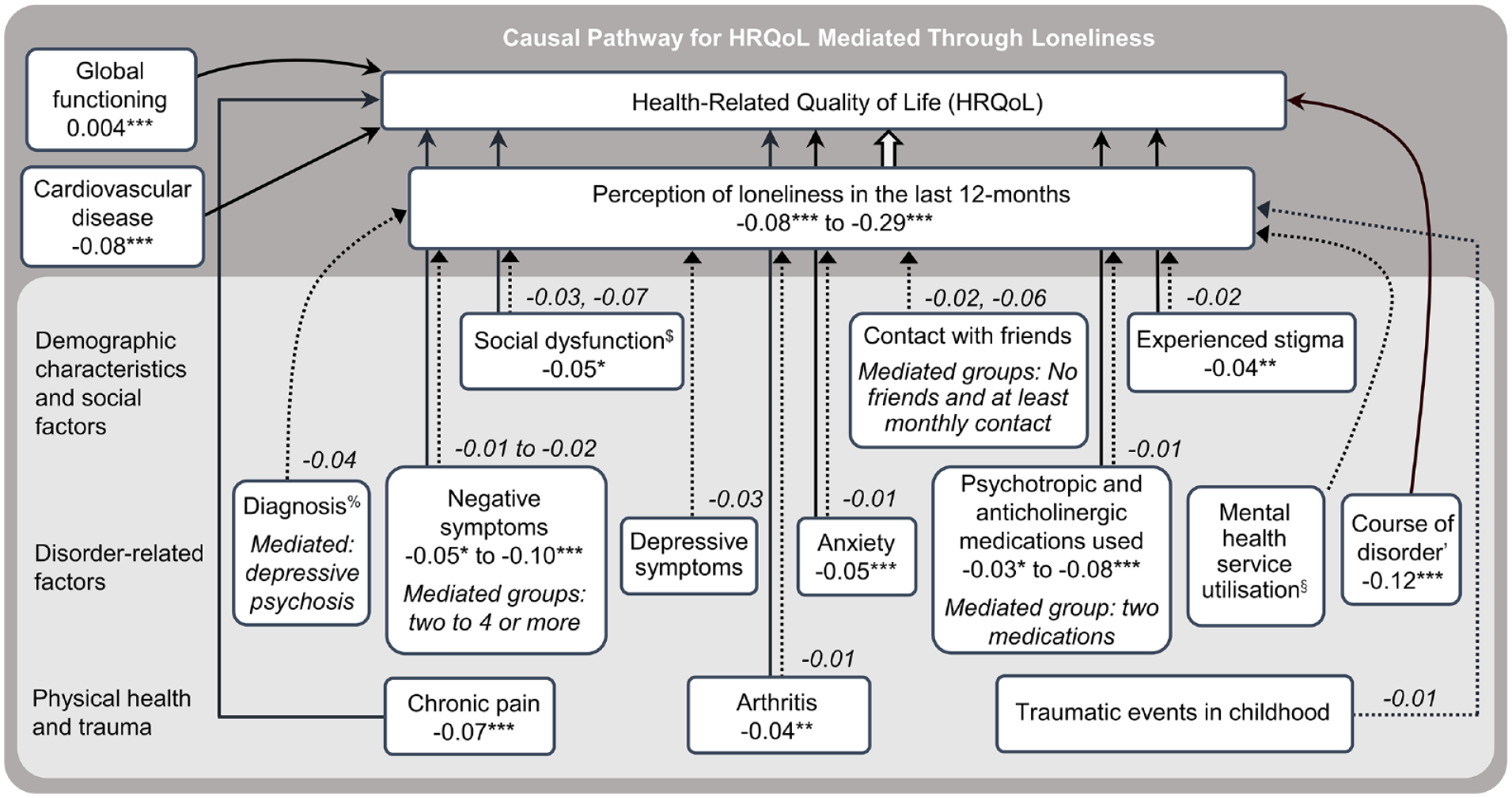
Final model for predictors of HRQoL in people with psychotic disorders and the role of loneliness.
Our findings that social factors were the strongest contributors to loneliness highlight the importance of social relationships in people with psychotic disorders (Nevarez-Flores et al., 2021a). It has been reported that the network of people with mental disorders is significantly smaller than the network of those without a mental illness, and that people with psychotic disorders have difficulties in their social relationships (Harvey et al., 2002). Consistent with this position is our finding that over one-fifth (23%) of the study participants described themselves as socially isolated and lonely, over 3 times higher than for the general population (7%) (Hawthorne, 2008). Interestingly, we found that neither contact nor lack of contact with relatives contributes to the perception of loneliness in the study population, unlike contact with friends. These findings are consistent with Hamaideh (2021) who found that inpatients with schizophrenia with low levels of social support from friends experienced higher levels of loneliness. Further, these findings arguably reflect the different roles that friends play in an individual’s life compared to relatives (Pahl and Spencer, 2010), and provide an indication of where to focus clinical interventions.
Our results show that type of diagnosis contributes to loneliness, particularly depressive psychosis and schizoaffective disorder, which replicates earlier findings (Badcock et al., 2015). Likewise, depressive symptoms were found to contribute to loneliness, which is consistent with the finding for diagnosis and with previous research (Lim et al., 2018). We also found that anxiety contributes to loneliness, which is consistent with findings that social anxiety can predict loneliness (Lim et al., 2018). In contrast, Badcock et al. (2015) found that anxiety did not contribute to loneliness in the current sample, when adjusted for a variety of psychotic and non-psychotic symptoms. As we did not consider the same symptoms, we consider that the effect of anxiety could have been attenuated by the presence of one or more of the variables considered by Badcock et al. (e.g. suicidal ideation).
Regarding MH service utilisation, our findings indicate that specialised emergency services and inpatient admission contributed to perceived loneliness in study participants. As far as we are aware, no other research has reported a significant contribution from type of service used to perceived loneliness, although associations have been examined. In a recent study on the current sample, people feeling lonely and socially isolated had significantly higher numbers of presentations to an emergency department, general practitioner visits and inpatient admissions than non-lonely people (Badcock et al., 2020). Otherwise, increased feelings of loneliness have been found with increased number of inpatient admissions (Chrostek et al., 2016), while inpatients had lower scores for loneliness than outpatients, but not significantly so (Trémeau et al., 2016). Consistent with these results, we found that people who had been admitted to hospital or who had used specialised emergency services in the last 12 months had the highest rates of loneliness (Supplemental Material Table S3). Together these findings suggest increased loneliness in those who have experienced acute psychotic episodes or relapse, arguably because more severe symptoms can affect their social life (skills and network) and routines.
Other contributors to loneliness were histories of traumatic events in childhood and of arthritis. There is evidence that childhood trauma can precede feelings of loneliness (Shevlin et al., 2015), with early stressors causing changes in the brain contributing to deficits in social attachment and regulation of mood and affect (Anda et al., 2006). These changes can be accompanied by other social or environmental factors, which together can lead to feelings of loneliness and, it has been postulated, mental disorders including psychosis (Shevlin et al., 2015). The finding of the effects of arthritis has not been described to the best of our knowledge, a situation that may have arisen because of the decreased risk for arthritis observed in people with schizophrenia (Sellgren et al., 2014). However, the finding of arthritis as a contributor to loneliness in people with psychosis is consistent with increased loneliness in people with arthritis compared with healthy people and people with other chronic diseases (Penninx et al., 1999).
Overall, we consider each of the contributors to loneliness found in our research as potential targets for clinical interventions aimed at diminishing the perception of loneliness in people with psychotic disorders. However, as the model fit had an associated pseudo-R2 of 13%, much of the variance remains unexplained by the model, so potential impacts of interventions will likely be limited. In turn, more focussed research on the foundations of the perception of loneliness in this population is required to develop potential intervention strategies for this important predictor of HRQoL.
Concerning the mediating effect of loneliness, our current analysis shows that 10 of the 16 variables were significant predictors of HRQoL, with loneliness the strongest, as per our previous study (Nevarez-Flores et al., 2021a). With the exception of MH service utilisation in the last 12 months, the effect of the other contributors to loneliness (social dysfunction, experienced stigma, contact with friends, diagnosis, depressive symptoms, anxiety, lifetime arthritis, and history of traumatic events in childhood) and two of the previously identified predictors of HRQoL (negative symptoms and medication use) were partially mediated through loneliness. The mediating effect of loneliness for social dysfunction was not surprising, as this variable was found to be the strongest contributor to loneliness for study participants, and it is well known that social factors have an important impact on the QoL/HRQoL of people with psychotic disorders (Eklund and Hansson, 2007). This result supports our previous findings that loneliness but not social dysfunction is an independent predictor of HRQoL in people with psychosis (Nevarez-Flores et al., 2021a) and emphasises not only the importance of the quality of social relationships for this population but also the overarching role of loneliness in determining HRQoL.
Contact with friends, while a significant contributor to loneliness, was not a significant predictor of HRQoL after adjusting for loneliness, indicating that the frequency of contact with friends affects the HRQoL of people with psychosis indirectly, via the perception of loneliness. Experienced stigma, which has been associated with the QoL/HRQoL of people with psychotic disorders (Nevarez-Flores et al., 2021a; Świtaj et al., 2013), was found to be partially mediated through loneliness. It has been postulated that the stigma of mental illness affects social skills, the lack of which has been identified as a cause of loneliness (Perese and Wolf, 2005). Further, that experienced stigma is socially excluding leading to loneliness. Therefore, these results support the mediating role of loneliness and reaffirm its importance in capturing social aspects of people’s experiences that can affect HRQoL.
Another important finding was the fact that more than half of the effect of depressive symptoms on the HRQoL of the study participants was mediated through loneliness, and the one diagnosis partially mediated through loneliness was depressive psychosis. Depressive symptoms have been found to predict the HRQoL of people with psychotic disorders (Stubbs et al., 2015). However, when perception of loneliness is included in a predictor model, depressive symptoms became a nonsignificant predictor of HRQoL in this population (Nevarez-Flores et al., 2021a). Therefore, while depressive symptoms are important, their impact on HRQoL is mediated by other factors, particularly perception of loneliness.
The presence of traumatic events in childhood and a lifetime history of arthritis were each found to be mediated through loneliness. Lifetime arthritis has both a direct impact on the HRQoL of people with psychotic disorders but also an indirect impact through perception of loneliness, while traumatic events in childhood were not found to predict the HRQoL of study participants. However, the current results show that traumatic events in childhood affect the HRQoL of people with psychosis indirectly through loneliness. Thus, the consideration of loneliness when assessing the HRQoL of this population is considered crucial.
Negative symptoms and medication use had the smallest percentage of effect mediated and neither was found to be a contributor to loneliness.
The mediating role of loneliness on the relationship between the factors addressed above and the HRQoL of people with psychotic disorders provides evidence of the importance of the perception of loneliness on the path to achieving better HRQoL and, in turn, indicates the importance of addressing loneliness in this population. The findings also highlight the presence of multiple variables with small cumulative impacts on the perception of loneliness in individuals with psychotic disorders.
Despite the 2010 Australian National Survey of Psychosis being one of the most comprehensive epidemiological studies into psychotic disorders globally, and the largest of its kind in Australia, the survey is cross-sectional and thus we cannot infer causality. Further, estimates of magnitude of effect mediation need to be considered with some caution, given known limitations with the traditional Baron and Kenny method of estimating direct and indirect effects. Further, constraints due to respondent burden resulted in some variables (including loneliness), being assessed with a single question instead of multi-item instruments (such as the Revised University of California, Los Angeles [UCLA] Loneliness Scale [UCLA-R]). There is also the potential for recall bias, given 12-month recollection periods. However, most questions have been used in previous data collections, such as the first Australian survey of psychosis – The Low Prevalence Disorders Study (Jablensky et al., 1999, 2000). A protocol for the analysis plan employed in this study was not separately published.
In summary, results of our study established contributors to perception of loneliness in people with psychotic disorders. Further, assuming a plausible causal model of mediation, the extent of mediation through loneliness for contributors to HRQoL was ascertained. Since loneliness was the strongest predictor of HRQoL in this population, the findings of our research add impetus to efforts to develop and trial strategies aimed at diminishing loneliness in people living with psychosis, and in turn improve their HRQoL.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211072437 – Supplemental material for Health-related quality of life in people with psychotic disorders: The role of loneliness and its contributors
Supplemental material, sj-docx-1-anp-10.1177_00048674211072437 for Health-related quality of life in people with psychotic disorders: The role of loneliness and its contributors by Adriana G Nevarez-Flores, Monique Breslin, Vaughan J Carr, Vera A Morgan, Anna Waterreus, Carol Harvey, Kristy Sanderson and Amanda L Neil in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group at that time were V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw and H. Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The 2010 Australian National Survey of Psychosis was funded by the Australian Government Department of Health and Ageing. The study sponsor had a role in the design of the original survey but did not have any role in the collection of the study data, or the design or interpretation of the data analysis reported here, or in the writing of this paper or the decision to submit this paper for publication. A. Waterreus received funding from the Western Australian Department of Health - Near-miss awards. A. Neil is supported by a Select Foundation Senior Research Fellowship.
Data Accessibility Statement
Please contact Prof Vera Morgan (at
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.