
Abstract
Approximately 5000 young people aged 10–17 years were held in juvenile detention centres in Australia between 2006 and 2007 [1]. Of these, approximately 2900 were being held on remand awaiting trial or sentencing while the remainder were serving detention sentences [2].
Although several studies conducted overseas have reported a high prevalence of mental health problems among young people on remand or in detention, there is a paucity of information describing the mental health and well-being of adolescents on remand in Australia [3–6]. For example, a recent meta-analysis of 25 studies conducted between 1990 and 2008 reported that among males, 53% met criteria for conduct disorder, 12% for attention-deficit/hyperactivity disorder (ADHD), 11% for major depression, and 3% for psychotic illness. Among females, 53% also met criteria for conduct disorder, 29% for major depression, 19% for ADHD and 3% for psychotic illness [7]. However, a limitation of this meta-analysis is that 15 of the 25 studies were conducted in the USA. Different policies about remand and detention, and the different ethnic composition of young people on remand in the USA [8] as compared to other countries mean that it cannot be assumed that the prevalence of mental health problems reported among young people in the USA necessarily applies in other countries such as Australia.
Several other findings are apparent from previous studies of young people in juvenile detention. First, as highlighted in the meta-analysis conducted by Fazel et al. [7], there is evidence that females on remand have a higher prevalence of internalising problems than males. Second, there is evidence that young people on remand experience a higher prevalence of suicidal ideation and behaviour than other young people in the community. For example, 10% of the 1,829 young people who participated in the study at Cook County Juvenile Temporary Detention Center in Chicago reported suicidal ideation and 3% reported having attempted suicide in the previous 6 months [9]. In Australia, Kosky et al. [5] reported that 17% of females (n = 23) and 13% of males (n = 55) remanded in South Australia endorsed the item on the Youth Self Report asking about self harm [10]. This was a higher prevalence than that reported by young people in the community or those attending mental health services at the time of the study.
Third, a high prevalence of comorbidity has been reported among young people on remand. For example, Abram et al. [11] reported that 57% of females and 46% of males remanded in the Cook County Juvenile Temporary Detention Center met criteria for two or more disorders including: ‘major depressive, dysthymic, manic, psychotic, panic, separation anxiety, overanxious, generalized anxiety, obsessive–compulsive, attention-deficit/hyperactivity, conduct, oppositional defiant, alcohol, marijuana, and other substance’ (p. 1097). A similar pattern has been reported among adolescents on remand in Australia [3,4]. For example, Dixon et al. [4] reported that 78% of female adolescents (N = 100) on remand in New South Wales met criteria for three or more psychiatric diagnoses.
Fourth, there is evidence that the demographic characteristics of adolescents in juvenile correctional facilities differ from adolescents in the general community. A higher proportion of adolescents on remand are males and those on remand have typically received less formal education than other adolescents in the community [3–5]. A high proportion of adolescents in the juvenile justice system have experienced family disruption and lack family support. Abram et al. [12] reported being unable to locate 43% of the parents of adolescents on remand in the Cook County Juvenile Temporary Detention Center. In Australia, Kosky et al. [5] reported that prior to their being remanded, only 24% of adolescents were living with one or both their parents, 23% were living with friends, 18% were living in an institution, and 17% were living ‘on the streets’. An important consequence of this is that studies of adolescents on remand, regardless of whether they employ diagnostic interviews or behaviour checklists, invariably have to rely largely on adolescent reports when assessing the mental health and wellbeing of young people on remand.
Despite progress in the area, previous studies of young people on remand have a number of limitations. First, comparisons between the nature and prevalence of mental health problems among young people on remand and in the general community have typically relied on previously published studies of young people in the community [3,6,7,11–13]. This limits the extent to which more detailed comparisons can be undertaken between the two populations. For example, it is possible that a higher prevalence of internalising problems reported for female adolescents on remand reflects a general pattern found in the community rather than being a specific characteristic of females on remand. It is also possible that the different prevalence of mental health problems identified between adolescents on remand and in the general community reflect the different demographic characteristics of the two groups.
In the Australian context, the absence of information about the mental health and well-being of Indigenous adolescents is a significant omission given that they are greatly overrepresented in juvenile detention centres. For example, the Australian Bureau of Statistics reported that in 2005–2006, 44.4 per 1000 Aboriginal and Torres Strait Islanders aged 10–17 years, were undergoing juvenile justice supervision compared to 2.9 per 1000 non-Indigenous Australians [14]. The only previous study of Indigenous adolescents in juvenile detention compared the prevalence of problems among 48 Indigenous and 52 non-Indigenous females aged 13–19 years [4]. With the exception of substance abuse/dependence where a higher prevalence of problems was found among Indigenous females, there was no significant difference between the prevalence of problems in the two groups.
We are not aware of any previous studies that have described the health-related quality of life (HRQL) of young people on remand. HRQL is a multi-factorial construct that focuses on individuals’ perceptions of their physical, psychological and social functioning. The concept adopts a person-centred approach and employs self-reported assessments rather than assessments by clinicians or evaluations based on biomedical parameters [15]. An increasing number of studies have examined the HRQL of young people with physical illness. Results from these studies make it clear that levels of health defined solely on the basis of symptomatic or biomedical indicators do not fully describe the health and well-being of young people [16,17].
The present study builds on previous research by comparing the prevalence of mental health problems among 13–17-year-olds on remand with those in the general community using the same methodology to assess problems in each group. The study also directly compared the prevalence of mental health problems experienced by Indigenous 13–17-year-olds versus the prevalence of problems among this age group who participated in the Western Australian Aboriginal Child Health Study [18]. Finally, the study compared the prevalence of suicidal ideation and behaviour, and the HRQL of adolescents on remand with those in the general community. It was hypothesized that adolescents on remand would have more mental health problems than adolescents in the general community, and a higher prevalence of suicidal ideation and behaviour. It was also hypothesized that the broader health and well-being of adolescents on remand would be significantly worse than that of other adolescents in the community.
Materials and methods
Participants
The participants consisted of 159 adolescents aged 13–17 years, who had been remanded in custody to the Magill Training Centre by the Youth Court of South Australia between April 2008 and July 2009. The majority of eligible participants (n = 66) who did not participate could not be enrolled because it was not possible to contact their legal guardians to obtain consent. A further 14 adolescents were considered by staff to be too aggressive or distressed to participate, and 20 were excluded for other reasons. Notably, only five adolescents and five legal guardians declined to give consent for participation in the study. The community comparison group consisted of 1283 adolescents, aged 13–17 years, who participated in the Child and Adolescent Component of the National Survey of Mental Health and Well-being. Full details of this survey are available elsewhere [19]. The Indigenous community comparison group consisted of the 1,100 13–17-year-olds from a total of 5,289 aged from birth to 17 years who participated in the Western Australian Aboriginal Child Health Survey [18].
Measures
Mental health problems
All adolescents completed the Youth Self Report Questionnaire (YSR) which yields a total behaviour problem score based on responses to all questionnaire items; an externalising problem score which describes uncontrolled and anti-social behaviour; and an internalising problem score which describes over-controlled and inhibited behaviour [10,20]. As well as the three ‘broad-band’ scales, there are seven ‘narrow-band’ scales which describe mental health problems in more specific areas. The recommended borderline cut-off score was utilized in the present study to identify adolescents who scored in the higher range on the questionnaire [10]. Substantial information is available about the validity and reliability of the YSR [10,20].
Indigenous adolescents on remand also completed the same version of Strengths and Difficulties Questionnaire (SDQ) as was utilized in the Western Australian Aboriginal Child Health Survey [18,21]. For the purpose of the present study, we report results from the four SDQ scales which identify mental health problems. The scales are labelled, ‘Emotional Symptoms’, ‘Conduct Problems’, ‘Hyperactivity/Inattention’, and ‘Peer Relationship Problems’. A total problem score can be calculated by summing scores from the four scales. The recommended borderline cut-off score was utilized to identify Indigenous adolescents scoring in the higher range on the questionnaire [22]. The reliability and internal validity of this version of the questionnaire is satisfactory when used with Indigenous young people [23].
Suicidal ideation and behaviour
Items from the Youth Risk Behaviour Surveillance System Questionnaire were used to identify (by a Yes/No response) whether during the previous 12 months, adolescents had experienced suicidal ideation, made a suicide plan, attempted suicide, and/or initiated a suicide attempt which required medical treatment [24].
Health-related quality of life
Participants completed the scales on the self-report version of the Child Health Questionnaire (CHQ) which assess physical health, and the impact of physical and mental health problems on social functioning [25]. We did not utilise the CHQ scales which assess emotional/behavioural health because the results from these correlate highly with results on the YSR, and we wished to minimise the questionnaire burden on participants. The CHQ provides information about adolescents’ perceptions of their functioning in these areas over a 4-week period. For the purpose of reporting results, the raw score in each area is transformed to a 0–100 scale with higher scores indicating better health. The scales comprising the CHQ have acceptable validity and reliability [25]. Although we did not change item or summary scores, for the purpose of reporting results in the present study, the names of some CHQ scales were altered to better reflect the items that comprise each scale. We will be referring to the CHQ scales (with the published names in parentheses) as follows: Physical Activities (Physical Functioning), Pain and Discomfort (Bodily Pain), and Perceived Interference with School and Peer Activities (Role/Social).
Statistical analyses
Analyses were performed using SPSS for Windows, Ver. 15.0 and Stata Ver. 10. The statistical significance of differences between categorical variables across the groups was assessed using the chi-square statistic. Differences in mean scores across the groups were assessed using the t statistic. The statistical difference in the proportion of adolescents scoring above the SDQ cut-off in the remand group and the population proportion estimates from the Western Australian Aboriginal Child Health Survey was assessed using a one-tailed t-test of difference in proportion between two independent samples. Multiple regression analyses were used to adjust for the effects of differences in the demographic characteristics across the remand and community groups.
Ethics approval
The study was approved by the Human Research Ethics Committee at the Women's and Children's Hospital, the Research Ethics Committee at the Department for Families and Communities, and the Aboriginal Health and Research Ethics Committee in South Australia.
Results
Demographic characteristics
The demographic characteristics of the adolescents on remand and those who participated in the Australian National Survey are shown in Table 1. It can be seen that there were a number of differences in the individual and family characteristics of the two groups. For example, the percentage of males, Indigenous adolescents, and adolescents not attending school, were all significantly greater (P <0.05) among the adolescents on remand than in the community. Only 23% of parents of the adolescents on remand lived together, with 27 adolescents reporting that they did not know their father; six reporting that their father was deceased; and five reporting that their father was in jail. Significantly fewer mothers and fathers of adolescents on remand were reported to have paid employment.
Demographic characteristics (%)
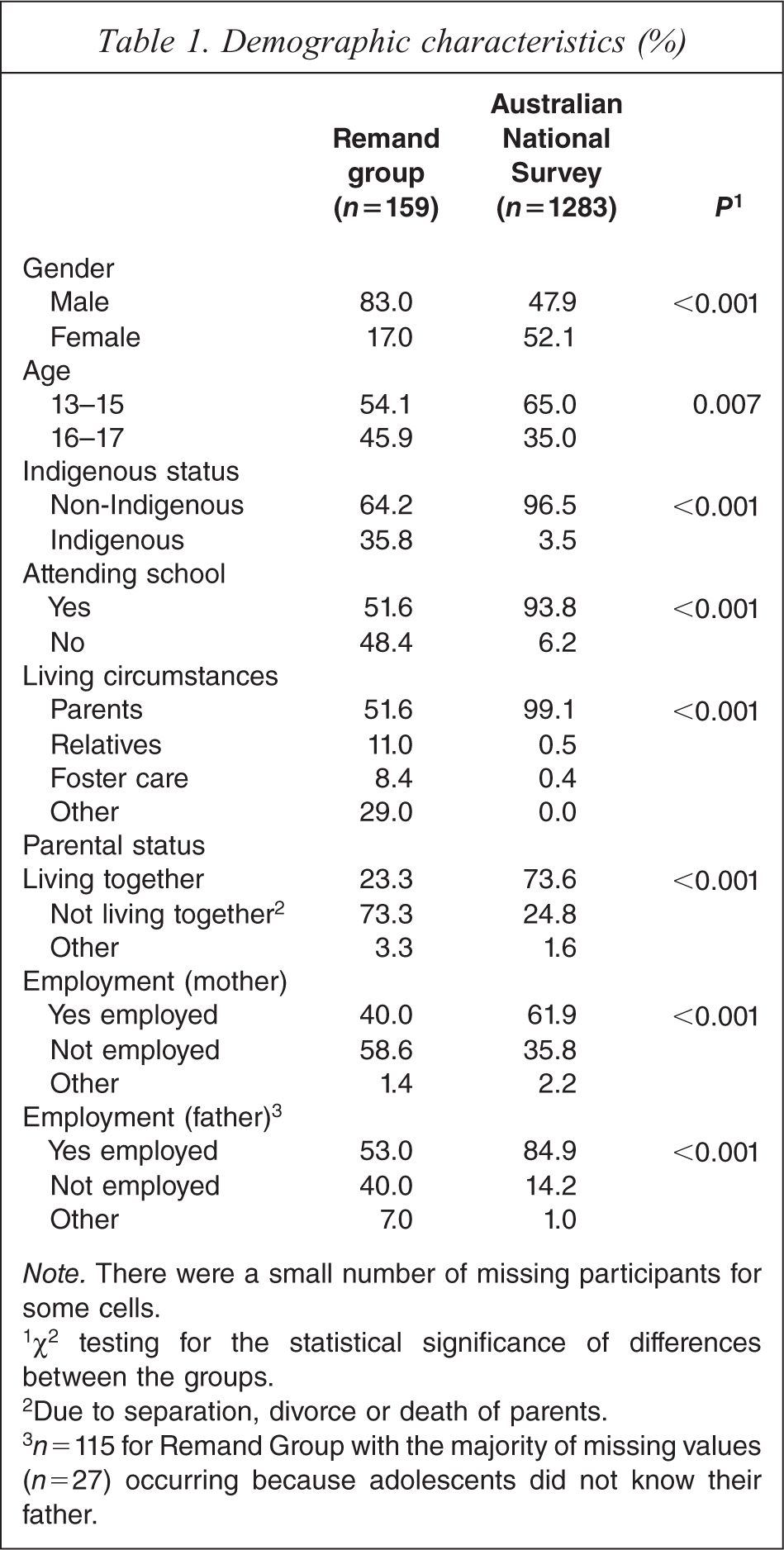
Note. There were a small number of missing participants for some cells.
1χ2 testing for the statistical significance of differences between the groups.
2Due to separation, divorce or death of parents.
3 n = 115 for Remand Group with the majority of missing values (n=27) occurring because adolescents did not know their father.
Mental health problems
The prevalence of mental health problems (defined as a score on the YSR above the recommended cut-off) among adolescents on remand and the adolescents in the community is shown in Table 2. With the exception of ‘Somatic Complaints’ (P = 0.02), differences between the groups were all significant at the level of P < 0.001. Not surprisingly, the highest prevalence of problems among the adolescents on remand was evident on the YSR scales rating externalising problems. For example, 67% of the adolescents in the group on remand scored in the range above the recommended YSR cut-off scores on the Delinquency Behaviour Scale. Multiple regression analyses were used to test the statistical significance of differences between YSR scores in the two groups, after adjusting for the effects of demographic characteristics. With the exception of the Somatic Complaints score (P = 0.16), the differences between the two groups were all statistically significant (P < 0.001) after this adjustment.
Percentage of adolescents scoring above borderline cut-off score on the youth self report
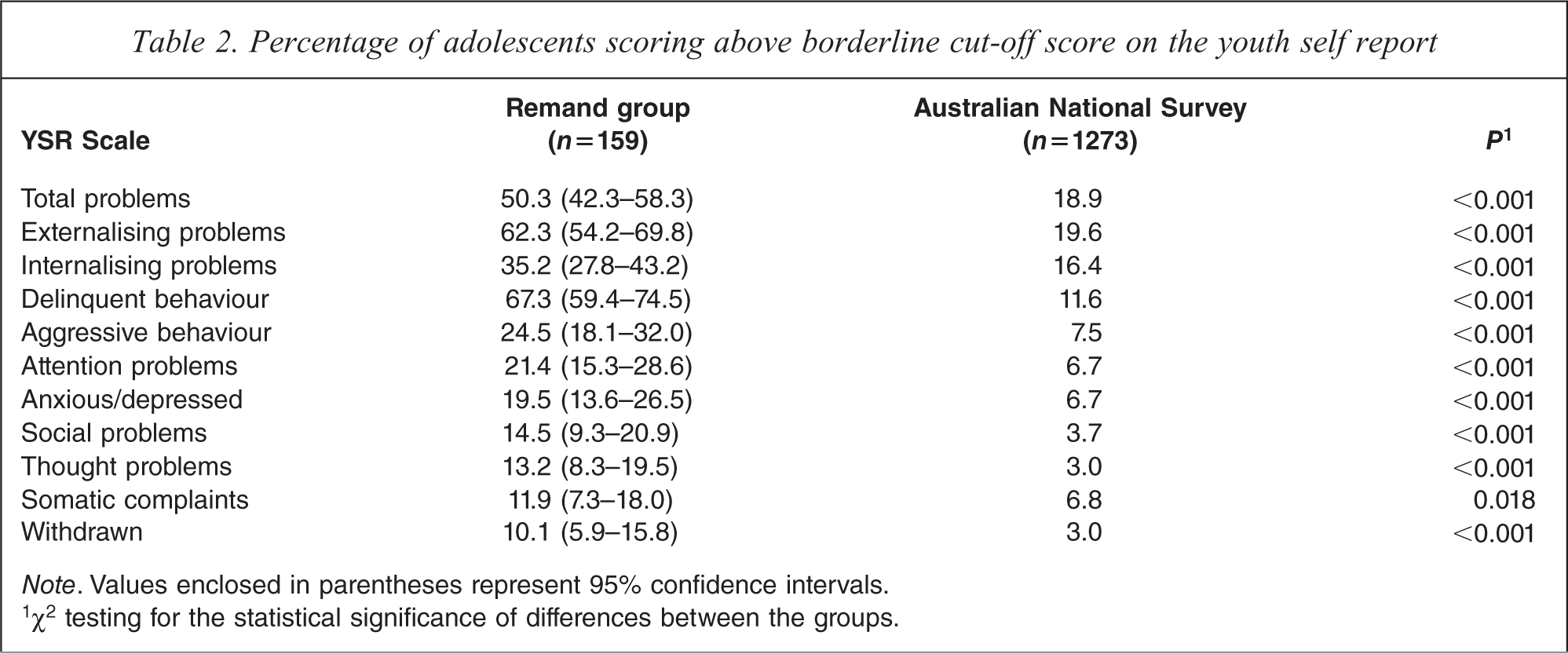
Note. Values enclosed in parentheses represent 95% confidence intervals.
1χ2 testing for the statistical significance of differences between the groups.
The prevalence of mental health problems (defined as a score above the recommended cut-off scores on the SDQ) among Indigenous 13–17-year-olds on remand and those in the Western Australian Aboriginal Child Health Survey is shown in Table 3. As compared to Indigenous adolescents in the community, a significantly higher percentage of Indigenous adolescents on remand scored above the SDQ cut-off scores on the Conduct Problems, Hyperactivity/Inattention Problems and Peer Relationship Problems Scales. There was no significant difference in the proportion of adolescents in the two groups who scored above the cut-off on the Emotional Symptoms Scale.
Percentage of indigenous adolescents scoring above the borderline cut-off score on the strengths and difficulties questionnaire (SDQ)
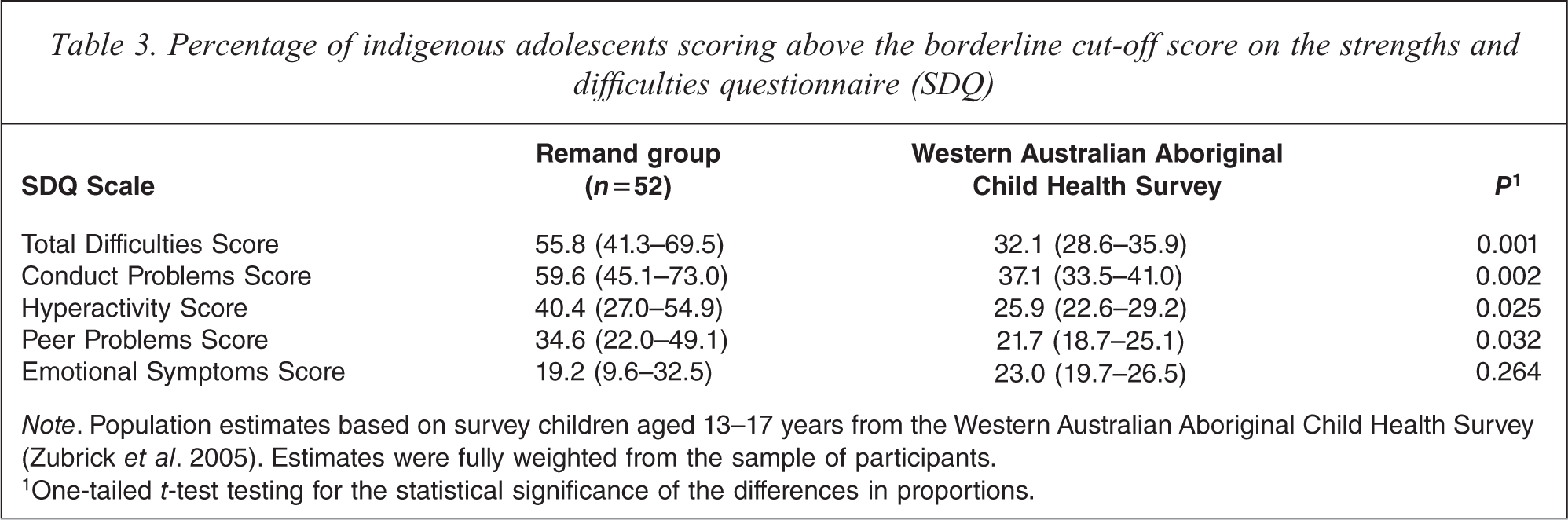
Note. Population estimates based on survey children aged 13–17 years from the Western Australian Aboriginal Child Health Survey (Zubrick et al. 2005). Estimates were fully weighted from the sample of participants.
1One-tailed t-test testing for the statistical significance of the differences in proportions.
The relationship between the demographic characteristics of adolescents on remand and their level of mental health problems are shown in Table 4. Consistent with the results from previous studies [3,26–29] female adolescents on remand had a significantly higher mean YSR internalising score than males (Table 4). Further analyses (not shown in Table 4) revealed that females also had significantly higher mean scores (P < 0.05) on the YSR narrow-band scales labelled Anxious/Depressed, Somatic Complaints and Withdrawn. To determine whether the size of the difference between female and male internalising scores differed in the remand and community groups, a Group by Gender interaction term was added to multiple regression analyses testing for differences between the remand and community groups on each of these YSR scales. None of the interaction terms was statistically significant suggesting that the sizes of the differences between scores for females and males in the remand group were not significantly different from those in the community.
Regression coefficients showing the strength of the relationship between YSR Total, Externalising and Internalising problem scores and the demographic characteristics of adolescents on remand
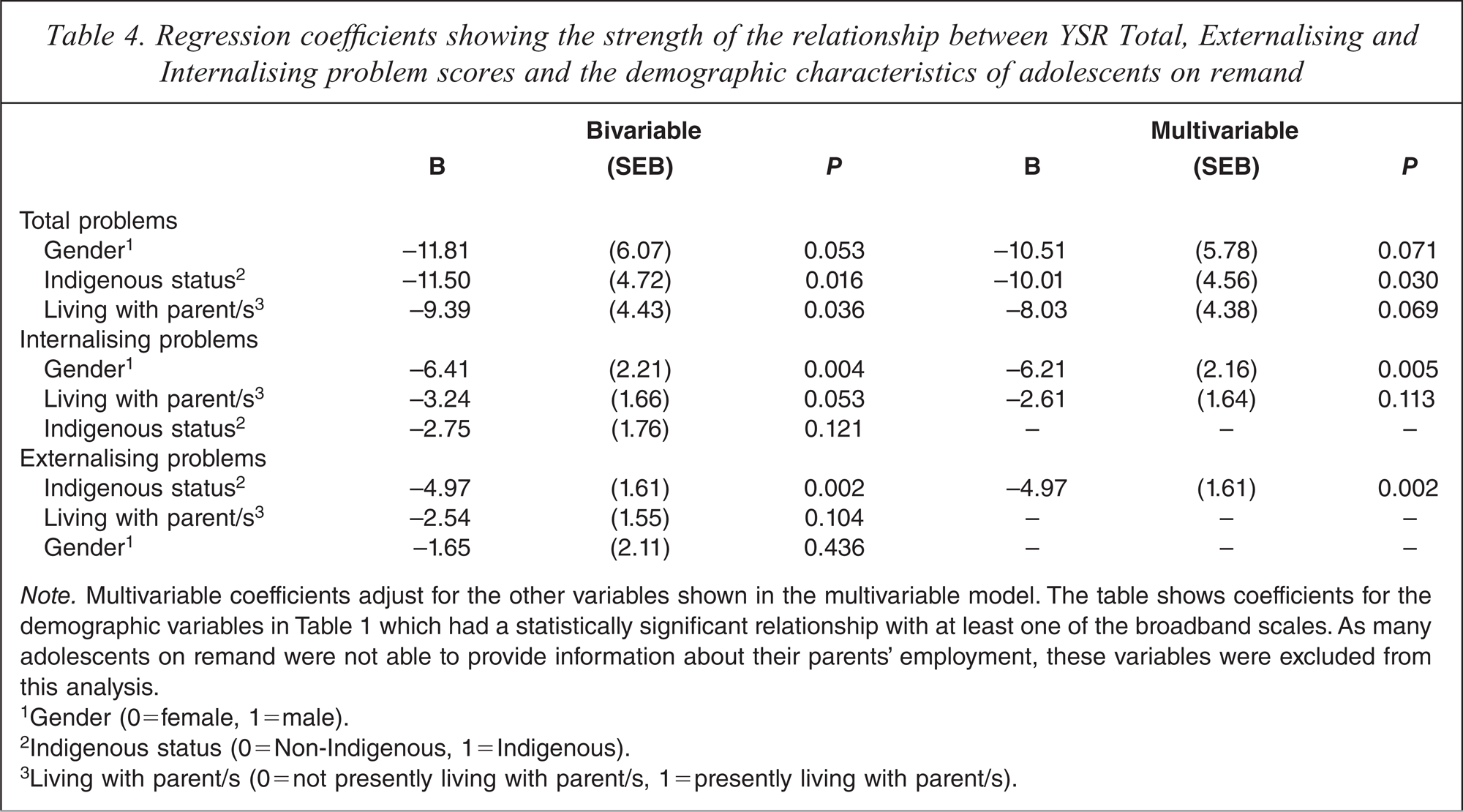
Note. Multivariable coefficients adjust for the other variables shown in the multivariable model. The table shows coefficients for the demographic variables in Table 1 which had a statistically significant relationship with at least one of the broadband scales. As many adolescents on remand were not able to provide information about their parents’ employment, these variables were excluded from this analysis.
1 Gender (0=female, 1=male).
2Indigenous status (0 = Non-Indigenous, 1 =Indigenous).
3Living with parent/s (0 = not presently living with parent/s, 1 = presently living with parent/s).
Among those on remand, Indigenous adolescents had significantly lower YSR externalising scores than non-Indigenous adolescents (Table 4). Further analyses (not shown in Table 4) showed that Indigenous adolescents also had significantly lower scores (P < 0.05) on the YSR narrow-band scales labelled Social Problems, Attention Problems, Delinquent Behaviour and Aggressive Behaviour. Once again, to determine whether the size of the differences in scores between Indigenous and non-Indigenous adolescents differed in the remand and community groups, a Group by Indigenous Status interaction term was added to multiple regression analyses testing for differences in YSR scores across the remand and community groups. As shown in Figure 1, the interaction term was significant for the broad-band YSR externalising score (coefficient = −6.91, SE = 1.84 P < 0.001). It can be seen in Figure 1 that the difference between the mean YSR externalising scores describing Indigenous and non-Indigenous adolescents was significantly greater, and in the opposite direction, in the remand group than in the community group. A similar pattern was found with scores on the YSR Social Problems, Delinquent Behaviour and Aggressive Behaviour scales.
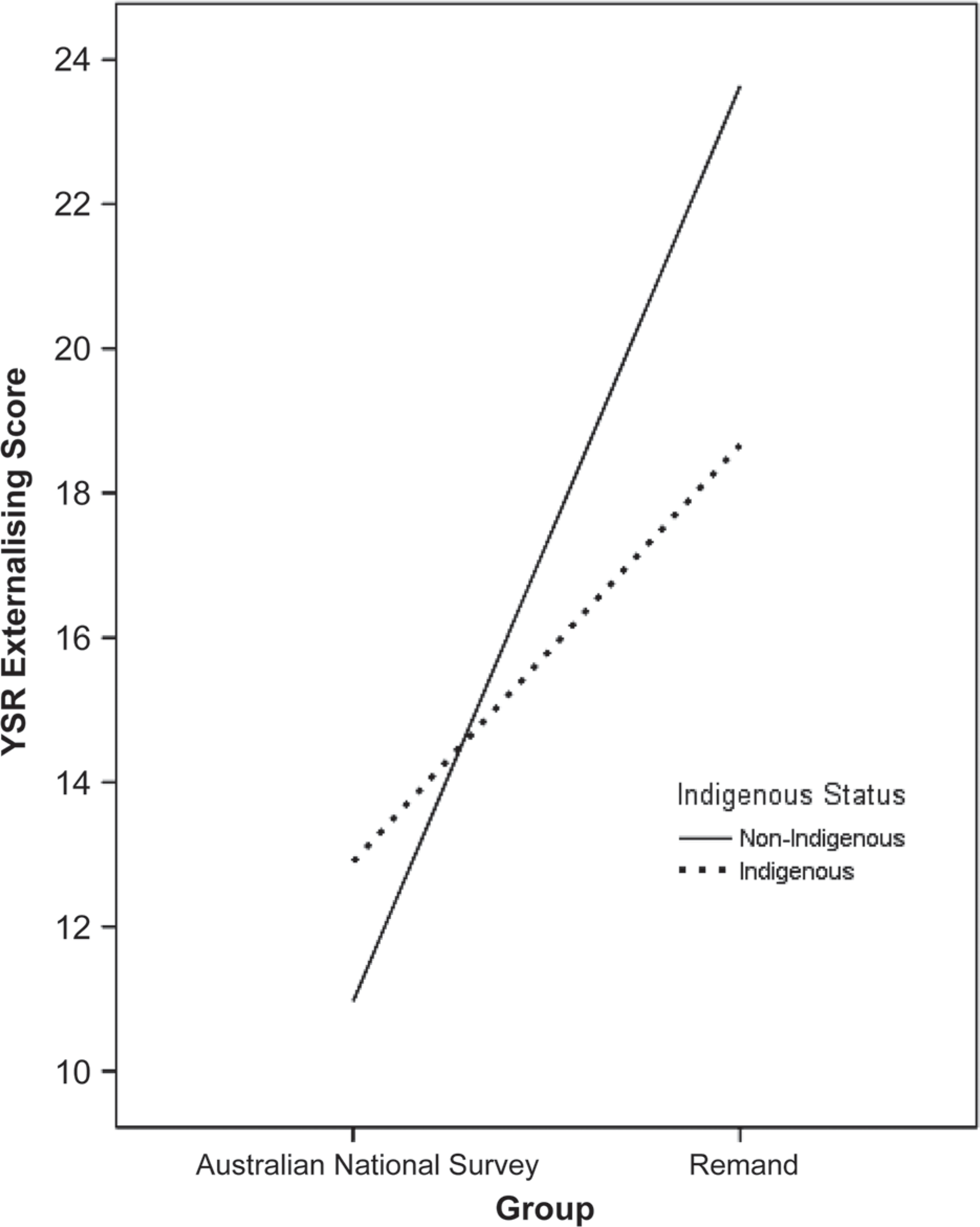
Mean differences on the YSR externalising score by remand and indigenous status.
Suicidal ideation and behaviour
Significantly more adolescents on remand than in the community reported suicidal ideation and behaviour, and suicide attempts requiring treatment (Table 5). The prevalence of suicide attempts requiring treatment was approximately 6 times greater in the remanded group than in the national survey (5.3 vs. 0.9%). With the exception of suicidal ideation, differences between the groups remained statistically significant (P < 0.05) after adjusting for the demographic characteristics of the two groups.
Percentage of adolescents reporting suicidal ideation and behaviour
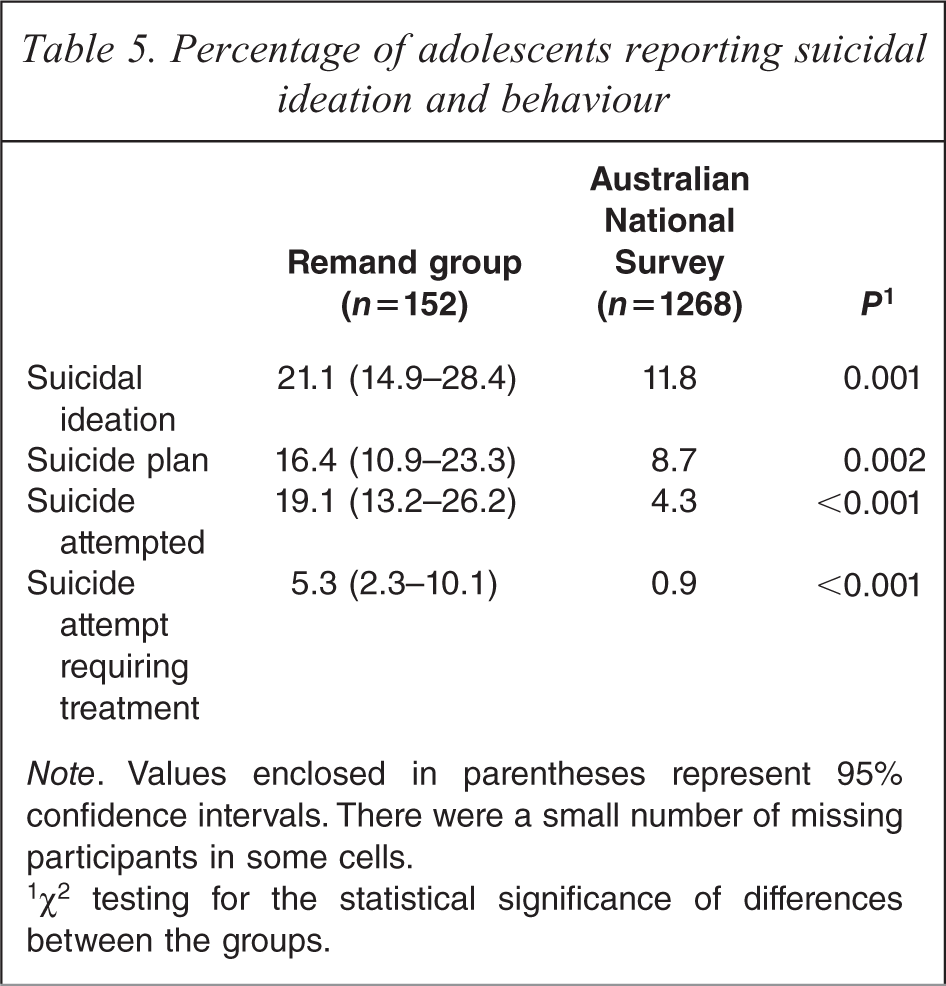
Note. Values enclosed in parentheses represent 95% confidence intervals. There were a small number of missing participants in some cells.
1 χ2 testing for the statistical significance of differences between the groups.
Among adolescents on remand, significantly more females reported suicide attempts requiring medical treatment during the previous year than were reported by males (Females = 19.2%, Males = 2.4%, χ2 = 12.2, P < 0.001). However, there were no statistically significant differences in the frequency of reports of suicidal ideation, making a suicide plan, or suicide attempts not requiring medical treatment reported by females versus males on remand. There were also no statistically significant differences between the prevalences of suicidal ideation and behaviour reported by Indigenous and non-Indigenous adolescents.
Health-quality of life
The mean Child Health Questionnaire (CHQ) scores reported by adolescents are shown in Table 6. Given the prevalence of mental health problems reported on the YSR, it is not surprising that adolescents on remand reported on the CHQ that they had a poorer self-esteem than adolescents in the community. However, differences were not restricted to these areas. As compared to adolescents in the community, adolescents on remand also had significantly lower mean scores on the General Health Perceptions, Pain and Discomfort, and Global Health Scales, and the CHQ scales assessing the extent to which adolescents perceived that their physical or mental health problems interfered with school or peer activities. According to Cohen [30], an effect size of 0.2 can be considered a small effect size, 0.5 a medium effect and 0.8 a large effect. It can be seen that effect sizes describing mean differences between CHQ scores across the remand and community groups were generally in the range described as a medium effect.
Mean (SD) Child Health Questionnaire Scores
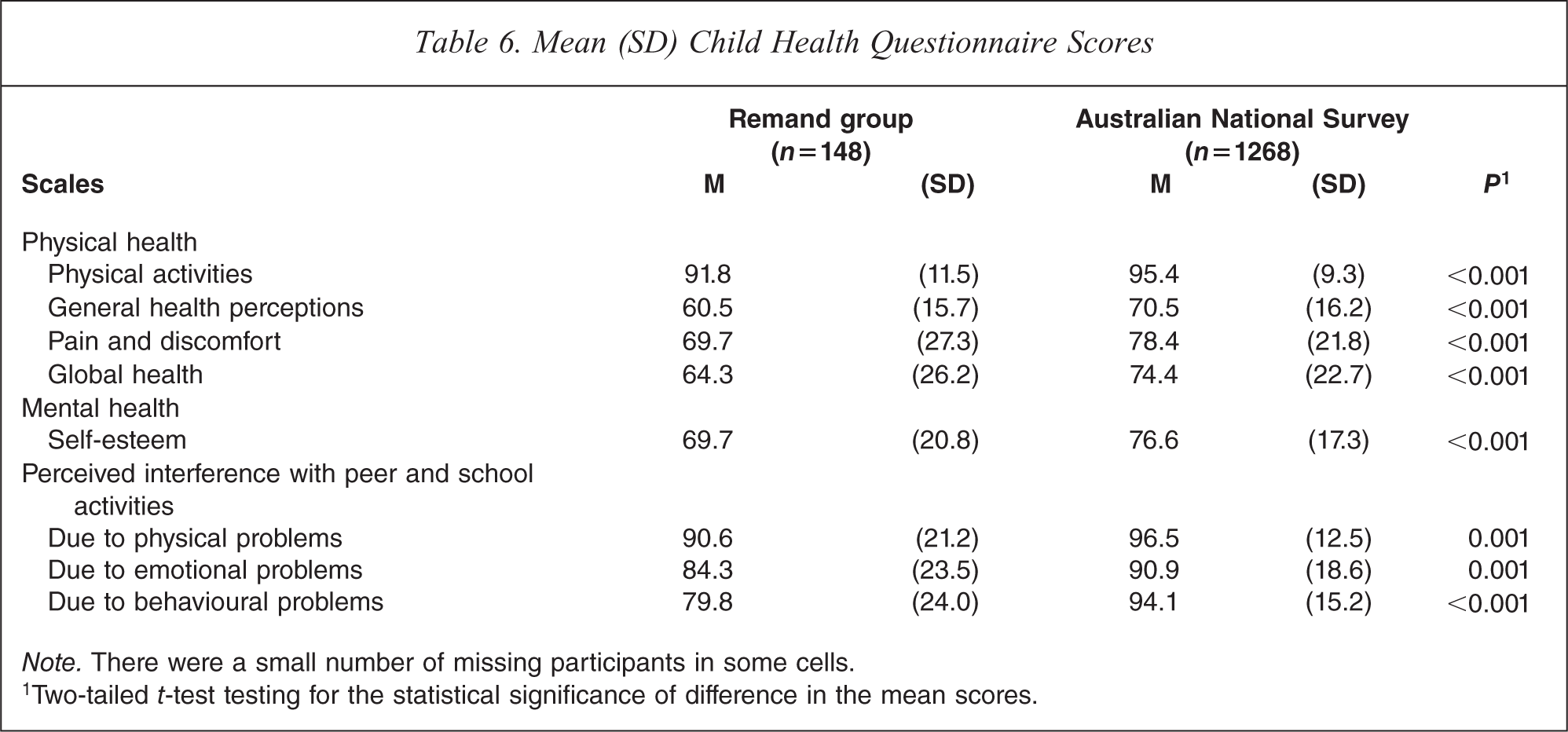
Note. There were a small number of missing participants in some cells.
1Two-tailed t-test testing for the statistical significance of difference in the mean scores.
Discussion
Results from the present study show that as compared to adolescents in the community, adolescents on remand have poorer mental and physical health, experience greater family adversity, and have a poorer attendance at school. Emotional and behavioural problems experienced by adolescents on remand significantly interfere with their schooling and peer activities.
The high prevalence of mental health problems reported by adolescents on remand was not limited to externalising problems. Rather, they experienced more problems than adolescents in the community in all areas assessed by the Youth Self Report [10]. Furthermore, they reported a significantly higher prevalence of suicidal ideation and behaviour than was reported by adolescents in the community. For example, they reported 6 times more suicide attempts that resulted in an injury requiring treatment by a health professional. This is concerning given the increased risk of completed suicide among adolescents with a history of suicidal ideation and behaviour [31].
Three findings are evident with Indigenous adolescents. First, the proportion of Indigenous adolescents in the remand group was 10 times greater than that in the community group. Second, consistent with results for non-Indigenous adolescents, Indigenous adolescents on remand had a significantly higher prevalence of externalising problems than Indigenous adolescents in the community. However, differences between the prevalence of internalising problems experienced by Indigenous adolescents in the remand and community groups were less evident. Third, within the remand group, Indigenous adolescents had significantly fewer externalising problems than non-Indigenous adolescents. This was a different pattern to that in the community where there was little difference in the level of externalising problems reported by Indigenous and non-Indigenous adolescents. There are two possible explanations for this pattern. First, it is possible that Indigenous adolescents with lower levels of externalising problems are being apprehended by police in the community. Second, it is possible that alternative placements are more difficult to find for apprehended Indigenous adolescents than non-Indigenous adolescents. The Children's Protection Act 1993 in South Australia incorporates a placement principle which requires Indigenous adolescents to be placed with Indigenous carers [32]. Although, substantial efforts are made to find alternative placements for Indigenous adolescents who are apprehended, these placements are difficult to find. It is possible that this difficulty is increasing the proportion of Indigenous adolescents with lower levels of externalising problems who are held on remand.
To the best of our knowledge, this is the first study that has used the same methodology to directly compare the prevalence of problems among males and females on remand with the prevalence reported for males and females in the community. Consistent with results from previous studies, females on remand in the present study reported a higher prevalence of internalising problems than males [3,12,26–29]. However, there were no significant Group by Gender interactions for any of the YSR scores across the remand and community groups. This suggests that the difference in the prevalence of internalising problems reported by males and females on remand reflects a general pattern of gender differences in the community, rather than being a specific characteristic of adolescents on remand. While these results may seem to be inconsistent with findings of McCabe et al. [33] who reported no difference in the mean internalising YSR T scores between male and female ‘adjudicated delinquents’ in the care of juvenile justice, mental health or welfare services in California (N = 625, age = 6–17 years), it must be borne in mind that McCabe et al. [33] employed T scores which, by definition, are adjusted for differences in male and female scoring patterns, making it unlikely that differences will be found across gender groups [10,20]. When comparing prevalences of problems across adolescents of different gender, it is necessary to use YSR raw scores.
Limitations of the present study include the use of self-reports as the sole source of information about the mental health and wellbeing of adolescents. It is also possible that the study underestimated the extent of problems amongst adolescents on remand because those with more severe levels of aggression or distress were excluded from the sample. A strength of the study is that all adolescents are remanded to a single youth training centre in South Australia. This means (barring the possible placement bias discussed above) that the level of mental health problems in the study reflects that of all remanded adolescents drawn from a population of approximately 1.2 million.
The findings from the present study pose a major challenge for our community. The problems exhibited by adolescents on remand are not limited solely to externalising problems which may have contributed to their incarceration. Rather, adolescents on remand are experiencing a wide range of health, educational and social problems. Many have experienced significant family adversity including parental separation, and the death or jailing of a parent. Almost 50% of the adolescents on remand had ceased living with their parents and no longer attended school. The substantial and wide-ranging problems experienced by adolescents on remand cause significant distress for the adolescents and their families, and for victims of their crimes. Furthermore, the financial costs of managing adolescents with conduct disorders are very high [34–36]. For example, Scott et al. [36] reported that between the age of 10 and 28 years the cumulative costs of public services in Great Britain used by individuals with conduct disorders were 10 times higher than those with no problems. These costs were not restricted to a single agency but included education services, health services, foster and residential care, and the costs of juvenile justice programs.
This study represents only a first step in the process required to address the typically poor outcomes experienced by adolescents on remand. The high prevalence of mental health problems and health-risk behaviours among adolescents on remand is a significant issue as mental health problems are commonly chronic conditions and adolescence is a time when life-long patterns of health-related behaviours are established. Repeat offending is also a major problem amongst adolescents held on remand. A better understanding of the nature and aetiology of these problems is an essential prerequisite for the development of more effective approaches to reduce criminal behaviour and improve mental health and well-being. However, the research base in this area in Australia is not strong. As a result, although a number of innovative approaches such as greater use of Diversion Courts, earlier mental health assessment and more frequent diversion to community-based programs have been initiated, little empirical evidence is available about the effectiveness of these programs.
Footnotes
Acknowledgements
The study was funded by the Australian Rotary Health Research Fund. The authors would also like to thank Linda Frost for helping with data collection and staff at the Magill Training Centre for facilitating the research process.