
Abstract
Affective disorders are often accompanied by circadian rhythm disruption and the major symptoms of mental illness occur in a rhythmic manner. Chronotype, also known as circadian preference for rest or activity, is believed to exert a substantial influence on mental health. Here, we review the connection between chronotypes and affective disorders, and discuss the potential underlying mechanisms between these two phenomena.
1 Introduction
The circadian rhythm is a universal feature of living organisms and influences nearly every biological process [1, 2]. The circadian rhythm is controlled by the endogenous circadian clock and entrained by the external environment. Although human beings work and rest with a period of ˜ 24 h, the timing of activity and rest varies among the population [3]. Some individuals tend to get up early and go to bed early while others prefer sleeping late and waking up late. This circadian preference can be defined as the chronotype of an individual.
Individual chronotypes are regarded as rather stable traits with a normal distribution of morningness vs. eveningness in the general population. About 40% of the adult population belong to the morning-type or evening-type categories, while approximately 60% of the population has no preference [4]. Chronotype is influenced by many factors, including age, gender, heredity, social constraints, and environmental factors [5 –7]. The most commonly used measures to assess chronotypes are subjective self-reports such as the Morningness-Eveningness Questionnaire (MEQ) and Munich ChronoType Questionnaire (MCTQ) [8, 9]. MEQ assesses the “feeling best” rhythm and the preferred time of individuals in various situations. MCTQ reflects the mid-sleep point on free days, which is calculated as the midpoint between sleep start time and end time on free days and strongly correlates with MEQ scores [10]. In addition, the chronotype of an individual can be measured objectively by recording one’s daily activity with devices such as acti-watches or by assessing the timing of dim light melatonin onset (DLMO) [11]. Subjective approaches are easier to manipulate in larger samples while objective methods are believed to be more accurate. Some studies have compared these two types of methods and found them to be significantly correlated, albeit with some minor differences [12, 13]. In recent years, with the advancement of high-throughput RNA profiling techniques, it was shown that a significant portion of the genome exhibits rhythmic expression, which is driven by the circadian clock [14]. Therefore, rhythmic transcriptomes in human periphery blood cells can also be used as an indicator of circadian phase, which is another objective method to assess chronotype. Algorithms such as TimeSignature and BodyTime have been developed to estimate the human circadian phase based on gene expression in blood monocytes [15, 16]. Partial least squares regression has been applied to analyze the transcriptomic profiles of human blood cells to predict melatonin rhythm phase [17].
Chronotype influences many aspects of health given the extensive effects of circadian rhythm on behavior and physiology [5]. Circadian rhythm disruption has been widely observed among patients with affective illnesses. Abnormalities in core body temperature rhythm and melatonin secretion were reported in patients with bipolar disorder (BD) [18]. The daily rhythm of hundreds of genes in the human brain that are involved in essential physiological events, including the sleep/wake cycle and metabolism, were found to be profoundly dysregulated in major depressive disorder (MDD) [19]. Circadian disruption is reliably associated with various adverse mental health conditions and well-being in large populations [20]. In recent years, a growing number of studies indicate a link between affective disorders and chronotype, which we will discuss in detail in this review.
2 Chronotype and major depressive disorder
MDD, which is also known as unipolar depressive disorder, is defined as one or more major depressive episodes and the lifetime absence of mania and hypomania [21]. A great number of studies support the conclusion that eveningness is associated with depressive disorder and the severity of depressive symptoms in patients with depressive disorder. Depressed patients showed more evening preference than controls [22]. Adults with current MDD had an increased chance of having a later chronotype in a Netherlands cohort study which included 676 currently depressed patients, 831 remitted patients, and 437 healthy controls [23]. Young patients (age 12–30) with depression also exhibited greater evening preference and a larger proportion of them are “extreme evening” chronotypes [24]. The chronotype of hospitalized patients with depressive syndromes were also investigated. Eveningness was directly associated with elevated depression severity in depressed inpatients [25, 26]. Consistently, depressive symptoms were significantly more serious in evening-type individuals than morning-type individuals during admission. Moreover, eveningness was related to greater subjective cognitive impairment in 804 individuals with self-reported symptoms of unipolar depression [27]. Cognitive symptoms were also significantly more obvious in eveningtypes vs. morning-types for inpatients [28]. In addition, studies have evaluated the relationship between suicidality and chronotype in patients with MDD. Compared to morning-type participants, evening-type participants exhibited a higher tendency toward suicidality [29, 30].
Moreover, eveningness was demonstrated to be associated with a higher incidence of depressive states and increased depressive symptom severity in the general population. In a large general adult population consisting of 10,503 Finnish participants, eveningness was significantly associated with a greater likelihood of being diagnosed with depressive disorder, antidepressant medication, and the severity of depressive symptoms [31]. In another study, eveningness was associated with an increased likelihood of depression among 100,402 individuals within the UK Biobank cohort [32]. In many studies from different countries conducted on both students and adults, individuals with the evening chronotype reported increased depression [33 –37]. Evening-type individuals with a phase delay of molecular oscillations estimated by the temporal profile of clock gene mRNA expression in hair follicles were 20 times more likely to be depressed than control individuals in a study including 528 undergraduate students in the US [38]. Among 1,068 medical students in Mexico City, depressive symptom severity was higher in non-morning chronotypes and the evening chronotype was associated with depression [39]. In addition, the evening chronotype was associated with elevated symptoms of depression in adolescents in a cross-sectional study and a longitudinal study encompassing a 48-month assessment [40, 41]. Given these data, it can be concluded that evening-types are more likely to report depressive symptoms and depressive disorder in both adults and adolescents from many different countries.
Delayed sleep phase syndrome (DSPS) is characterized by a habitually delayed sleep–wake schedule as compared to a conventional or socially acceptable one. In a study including 90 DSPS patients, 64% were in a moderate or severe depressive state, indicating that there is a high prevalence of depressive symptoms among evening-type patients [42]. There were no significant differences in the occurrence of depressive disorders between the individuals with DSPS and those with merely an evening preference, suggesting that mood is primarily influenced by having an evening chronotype, rather than a sleep complaint [43].
3 Chronotype and seasonal affective disorder
Mood is easily affected by seasonal light changes [44, 45]. Seasonal affective disorder (SAD) is a seasonal pattern of recurrent major depressive episodes generally occurring in autumn/winter and remitting in spring/summer [46]. As light treatment is the most-preferred therapy for SAD and light resets the phase of circadian rhythm, differences in chronotypes have long been considered as a possible cause of SAD [47]. Individuals with syndromal or subsyndromal SAD are more likely to be evening type while evening-type individuals are more susceptible to SAD than morning-type individuals. In a population sample of 4,905 Finnish adults, participants with symptoms of SAD had significantly increased odds of having evening chronotypes [48]. In 3,435 Russian adolescents aged 10–20 years old, there were significant differences in chronotype between individuals with or without SAD. Later sleeping and waking times were observed in both males and females with SAD [49]. A group of 327 adult participants with DSPS were 3.3 times more likely to report SAD when compared with 331 controls [50]. During polar nights, Chinese expeditioners at Zhongshan Station experienced delayed circadian rhythm and sleep phase, exhibiting altered chronotype as well as an increased incidence of sub-syndromal SAD [51]. In a study testing the effects of high-density negative air ions in treating SAD, subjects with a morning chronotype responded better than those with an evening chronotype [52].
Despite these findings, some studies report a lack of significant links between chronotype and SAD. Morning-evening preference was not found to be associated with SAD for 101 young participants in Poland between 20 and 30 years of age [53]. In another investigation, the success of light therapy was not dependent on the chronotype of 132 SAD patients tested, suggesting that the anti-depressive effect of morning light cannot be explained by a phase shift of the biological clock [54]. However, these studies used relatively small samples and need to be further validated.
The seasonality of mood can be defined as the annual mood variation of an individual. It is associated with chronotypes in both the general population and patients with affective disorders. Evening-type participants received higher mood seasonality scores than intermediate and morningtypes in a study investigating the relationship between circadian preference and mood seasonality in 1,539 adolescents [55]. In another study, 1,715 university students with enhanced seasonality of mood were more likely to be evening-types [56]. A positive association was also found between worse mood and phase delay in winter across 3 years among a random community sample with 244 adults in Melbourne [57]. Similarly, a study of 469 young Finnish adults found that diurnal preference toward eveningness was more likely to be associated with seasonal variations in mood and behavior, compared to those with diurnal preference toward morningness [58]. On the other hand, morningness was associated with lower seasonality of mood in 489 old Order Amish individuals [59]. It has also been demonstrated that a higher level of depression significantly correlated with larger seasonal changes and seasonality was more prevalent in the bipolar group and was associated with evening preference [60, 61].
4 Chronotype and bipolar disorder
BD is a severe mental illness which is characterized by alternating manic or hypomanic and major depressive episodes, separated by euthymic periods when symptoms are reduced or absent. BD patients display mood states ranging from extreme mania to severe depression and show both of these opposite symptoms simultaneously during mixed states [62]. In a large number of studies evaluating chronotypes in both adult and adolescent BD patients, BD was usually associated with evening preference [13, 63]. BD patients showed delayed chronotype (daytime midpoint) and greater midpoint variability than healthy controls [64]. One study assessed the chronotype of children and adolescents with BD, and no difference was found when comparing BD children (age 7–17) and controls. However, BD adolescents (age 13 and older) displayed significantly greater eveningness compared to their peers [65]. In the general population, late chronotype is also associated with bipolarity (bipolar tendency). In a group of 302 individuals, evening-types displayed significant bipolarity or mood fluctuations [66]. Another study based on 1,449 web questionnaires also supported the conclusion that eveningness is associated with bipolarity [67].
Moreover, evening preference is associated with different stages of BD. In a sample of 752 French euthymic BD patients, the number of participants having an evening chronotype was double of that with morning chronotype [68]. Brazilian and French outpatients with BD were significantly more likely to show an evening preference than control subjects when in remission [69, 70]. However, chronotype did not significantly differ between 119 remitted BD patients and 136 control individuals in a study conducted in the US. In this study, healthy controls were significantly younger than BD patients and circadian differences were probably was masked by the influence of age [71]. In Asian countries, eveningness chronotype has been reported to be associated with frequent recurrences of episodes associated with BD [72].
Evening chronotype is associated with increased mood symptoms in BD patients, including depression and mania. In an Arctic population including BD patients and their healthy relatives, lifetime manic behavior was increased among subjects with “the night owl” chronotype [73]. BD patients with elevated depressive mood scores were more likely to be evening-types [74]. In addition, patients with rapid cycling BD were more phase-delayed than control subjects [75]. Lithium is an effective mood stabilizer for alleviating mood symptoms in BD, but some patients are unresponsive to it. Compared to lithium non-responders, lithium-responsive BD patients showed morningness preference [76]. Additionally, BD patients treated with lithium exhibited an increased morning preference [77]. Independent of mood state and treatment, evening preference has a stable association with BD, implying that an evening chronotype may be a trait marker for BD [78].
The chronotype difference between BD subtypes have been investigated as well. Bipolar I disorder (BD-I) involves periods of severe mood episodes from mania to depression while bipolar II disorder (BD-II) involves milder episodes of hypomania that alternate with periods of severe depression [62]. Korean patients with BD-I showed a significantly greater preference for evening than control individuals [79]. Among BD-I patients, younger participants and those with rapid changes in mood were significantly more likely to exhibit evening preference [80]. Evening preference was also more prevalent in BD-II patients in Korea [61]. Moreover, 43 Korean patients with BD-II showed more eveningness than 106 patients with BD-I [81]. However, this has been controversial as another study failed to detect significant differences in morningness-eveningness scores between 134 BD-I cases and 56 BD-II cases in the US [74]. The subjects in these two studies were from different countries and the sample size for BD-II was relatively small, thus the results need further validation.
5 Chronotype and anxiety disorder
Individuals with anxiety disorders are excessively fearful, anxious, or avoidant of perceived threats in the environment, such as social situations or unfamiliar locations, or internal causes. The fear or anxiety is marked, persistent, and impairing [82]. Eveningness was found to be associated with anxiety disorders in a number of studies. Patients with anxiety disorders were more likely to be evening-types based on a study consisting of 1,468 inpatients [83]. According to the data from a large cohort in the Netherlands consisting of 1,944 participants, late types were more likely to be anxious and the severity of anxiety tended to be increased in the late group [23]. There was a significant association between chronotype and anxiety, and eveningness significantly predicted increased anxiety [84]. Female nurses with eveningness-oriented preference appeared to be more prone to demonstrating anxiety than those with morningness [85]. Among 641 healthy Korean individuals, evening-type subjects were more likely to possess anxious temperaments, which might contribute to their vulnerability for affective disorders [86].
Consistently, evening-types also reported more symptoms of anxiety in young individuals. Eveningness was associated with elevated anxiety in adolescents and incoming college students [40, 87, 88]. Among college students, the eveningtype group also displayed a larger proportion of anxiety and suffered from increased anxiety symptoms than the other two chronotypes [34, 89, 90]. In a study including 1,406 adolescents, anxiety was associated with eveningness during weekdays but not on the weekend, and a greater proportion of evening-types were found in the high-anxiety group [91]. However, no significant connection was found between circadian phase preference and anxiety in a US sample of 838 undergraduate college students [92]. A lower prevalence rate of psychiatric disorders in this population may account for this discrepancy.
6 Clock gene variants underlying chronotype and affective disorders
These associations between chronotype and various affective disorders imply that there is a role for altered circadian clock in the pathological processes of affective disorders. Therefore, many studies have searched for the potential contribution of clock genes in mood regulation, and a number of genetic variants associated with both chronotypes and affective disorders have been identified (Table 1).
Clock gene variants associated with both chronotype and affective disorders.
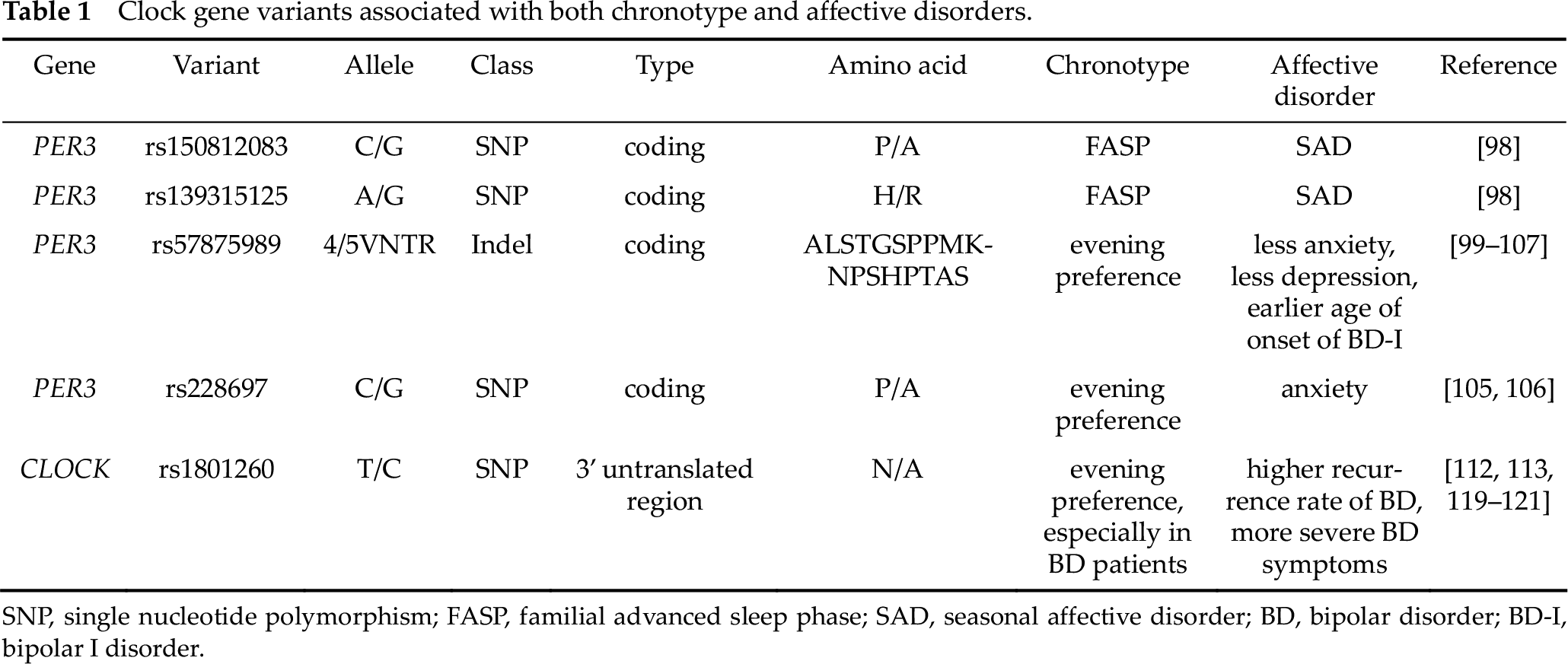
SNP, single nucleotide polymorphism; FASP, familial advanced sleep phase; SAD, seasonal affective disorder; BD, bipolar disorder; BD-I, bipolar I disorder.
The human PERIOD3 (PER3) gene is believed to serve as a link between circadian rhythm and mood regulation. PER3 shares several highly conserved domains with PER1 and PER2, acting as their dimerizing partner [93, 94]. Unlike its paralog Per1 and Per2, Per3 was shown to be non-essential for the endogenous circadian clock in mice [95]. Multiple studies demonstrated that PER3 is involved in sleep regulation and may influence circadian preference [96, 97]. Familial advanced sleep phase (FASP) is a human behavioral phenotype defined by early sleep time and early morning awakening. Thus, individuals with FASP are extreme morning-types. Three FASP subjects have been found to carry two rare variants in the PER3 gene (PER3-P415A/H417R). These individuals also displayed elevated Beck Depression Inventory scores, Global Seasonality Scores, and Problem Severity Scores, which are strongly suggestive of SAD. At the molecular level, these variants lead to decreased PER3 protein levels and destabilized PER1 and PER2 proteins, which may contribute to alterations in the clock phase [98]. Transgenic mice carrying human PER3-P415A/H417R displayed about 4 h of phase delay under extreme short photoperiod (4 hours light: 20 hours dark, 4L20D), but not under normal lighting conditions (12 hours light: 12 hours dark, 12L12D). In addition, increased despair-like behaviors were observed in hPER3- P415A/H417R transgenic mice on both tail suspension test and forced swim test under 4L20D (unpublished result). PER3-P415A/H417R are the only verified clock gene variants which regulate the phase of circadian rhythm (chronotype) and mood. In most cases, eveningness, not morningness, is associated with SAD, but PER3-P415A/H417R individuals displayed advanced sleep phase whereas hPER3-P415A/H417R transgenic mice exhibited delayed phase. Further mechanistic characterizations will be required to explain the discrepancy between human and mouse phenotypes, as well as how advanced sleep phase is linked to SAD in individuals carrying PER3- P415A/H417R alleles.
The most-studied variant of PER3 is a length polymorphism (rs57875989) located on exon 18. These coding-region variable number tandem repeats (VNTRs) encode an 18-amino-acid tandem motif which is repeated 4 (PER34) or 5 (PER35) times [99]. Four-repeat allele has been linked to DSPS and extreme evening preference [100] and this correlation has been replicated in several studies [101 –103]. However, this association between PER3 polymorphism and diurnal preference appeared to attenuate with age and was significant only in the youngest group (18–29 years old) [104]. In a group of 380 undergraduate and graduate students, the frequency of the 4-repeat allele was higher in evening-types and lower in morning-types, whereas PER3 4/4 and PER3 5/5 genotypes are less frequent in morning-types and in evening-types, respectively [105]. PER3 VNTR has also been reported to be associated with affective disorders. Individuals carrying a PER34 allele displayed more anxiety [105]. In addition, PER34/4 was significantly associated with depression and evening preference in another study consisting of 546 undergraduate subjects [106]. In a sample of 99 patients affected by BD-I, PER3 VNTR influenced the patients’ age at onset of illness: earlier age of onset in PER3 5/5 individuals and later age in PER3 4/4 [107]. As PER3 VNTR motif contains clusters of potential phosphorylation sites for the key clock kinase casein kinase 1, this polymorphism could influence the stability and nuclear localization of PER3. It was predicted that decreased or increased phosphorylation levels associated with PER3 4/4 and PER3 5/5 lead to a lengthened or shortened period length, respectively [105]. This altered period length can result in altered phase under light-dark conditions, which manifests as morning/evening chronotypes in the human population.
A single nucleotide polymorphism (SNP) of PER3, rs228697, was significantly associated with evening preference and anxiety in a population of 380 undergraduate and graduate students [105]. At this site, mutation from C to G leads to a proline-to-alanine substitution at amino acid 864 of the protein and may change the tertiary structure of PER3 [105]. The frequency of the G allele and the distribution of GG homozygous alleles were higher in evening-types. Individuals homozygous for GG were more likely to be the evening type and were more likely to be anxious. In another study including 546 undergraduates, GG homozygous individuals also reported significantly higher anxiety and evening preference [106].
The human circadian locomotor output cycles kaput gene (CLOCK) is a central component of the circadian clock. CLOCK protein consists of 846 amino acids, acting both as a transcription factor as well as perhaps an acetyltransferase [108, 109]. rs1801260 (3111T/C) is the most-studied SNP of the human CLOCK gene. It is located at position 3111 in the 3’ untranslated region, a region important for mRNA stability. Clock knockout mouse embryonic fibroblasts transfected with human CLOCK-3111C showed increased levels of CLOCK and Per2 mRNA levels [110]. In luciferase reporter assays conducted on human cells, the luciferase gene was expressed significantly higher when it was fused to the 3’-UTR region of CLOCK carrying the 3111C SNP, strongly suggesting that 3111C increases the level of CLOCK mRNA [111]. Rs1801260 was reported to be associated with a delay in preferred timing of activity and sleep. Subjects carrying the C allele exhibited a significant evening preference in more than 400 American and Japanese participants [112, 113]. However, this variant is neither associated with evening preference nor DSPS in the UK and Brazilian population, as well as in 415 unrelated women in northeastern Greece [114 –116]. The C allele was associated with late chronotype and severe depression in patients with affective disorders, although case-control investigations were not able to identify an association between CLOCK rs1801260 and mood disorders [117, 118]. Compared to T/T homozygotes, carriers of the C allele displayed a delayed sleep onset in 39 bipolar depressed inpatients [119]. This polymorphism may exert an influence on BD recurrence, as the recurrence rate in homozygotes for the C allele was nearly double than homozygotes for the T allele and heterozygotes in 101 BD-I patients [120]. In 87 depressed patients with BD-I, rs1801260*C carriers showed higher rates of suicidal ideation and increased depression severity than patients with T/T homozygotes [121].
Despite the discrepancies found in human genetics data, ClockΔ19 mutant mice were able to recapitulate the manic symptoms of BD patients. ClockΔ19 mutation results in an A to T nucleotide transversion at a splice donor site, causing a skipping of exon 19 and subsequently deletion of 51 amino acids in the CLOCK protein [109]. ClockΔ19/Δ19 mice displayed a lengthened circadian period and an overall behavioral profile that was strikingly similar to bipolar patients in the manic state. ClockΔ19/Δ19 mice showed a greater preference for a range of rewarding stimuli, including rewarding electrical stimulation and sucrose. Accordingly, these Clock mutant mice were extremely hyperactive and exhibited increased exploration on the open field test and increased swimming in the forced swim test, suggesting reductions in both anxiety and depression-like behaviors. Lithium, a commonly prescribed mood stabilizer for treating mania, was able to reverse manic-like behavior of the Clock mutant mice [122, 123]. Reduced anxietyand depression-related behaviors of ClockΔ19/Δ19 mice were only observed during the daytime, revealing a profound manic-like phenotype emerging during the day followed by a period of euthymia at night. This rapid mood-cycling coincided with abnormal daytime spikes in dopaminergic activity, tyrosine hydroxylase (TH, the rate-limiting enzyme in dopamine synthesis) levels, and dopamine synthesis in the ventral tegmental area (VTA) of ClockΔ19/Δ19 mice. Daytime inhibition of TH by Alpha-methyl-DL-p-tyrosine methyl ester (AMPT) reversed manic-like behaviors in ClockΔ19/Δ19 mice. At the molecular level, CLOCK acted as a negative regulator of TH transcription in the VTA. In short, ClockΔ19 mutation enhanced dopamine synthesis, leading to manic-like behavioral states during daytime [123, 124]. Overall, these results imply that CLOCK may indeed regulate both chronotypes and mood states in humans.
7 Discussion and conclusion
In summary, it appears that under the majority of the circumstances, the evening chronotype is associated with affective disorders, increased severity of symptoms, such as worse depressive or anxious mood, higher seasonality scores, increased bipolarity, and higher suicidality or suicidal ideation.
Social schedules, such as school and work, exert profound influences on chronotypes. In most cases, school and work starts relatively early in the morning. Evening chronotypes tend to go to bed late but have to get up at a relatively early time on school/work days, thus accumulating sleep debts which lead to increased sleep on free days. Therefore, late chronotypes display a larger difference in sleep timing between work and free days. The discrepancy in sleep/wake times between work and free days reflects differences between actual sleep/wake times and endogenous circadian phase, which is described as social jetlag [125]. Social jetlag leads to sleep disturbances, such as poor sleep quality and daytime sleepiness, which may be critical risk factors for various affective disorders. Eveningness may result in suffering from more social jetlag and accompanying sleep disturbances. However, a study found that there was no difference in social jetlag between patients with MDD and healthy controls [126]. Chronotype was reported to significantly correlate with specific subtypes of anxiety disorders, but did not predict these anxiety subtypes after controlling for insomnia [37]. In a survey including 1,403 students (undergraduates and graduates), insomnia, nightmares, and circadian phase delay were associated with increased depression, anxiety, and other symptoms [127]. There were statistically significant associations between insomnia and depression, whereas weak associations were detected between chronotype and depression [127]. These findings imply that the sleep disturbances in evening-types may be a major contributor to the development of anxiety and depression.
However, sleep problems are not the sole contributing factor, as some studies reported that eveningness is associated with depression, independent of sleep [30, 36, 128]. Eveningness was found to be associated with an increased risk of remission to depression or depression severity even after adjusting for insomnia severity in MDD and BD patients, supporting the significant and independent role of circadian factor in contributing to depressive symptoms [25, 30]. In a study including 1,814 participants, evening preference was associated with an increased incidence of depressive states, even after adjusting for differences in sleep parameters [36]. Another study also supported that evening chronotype per se was an independent risk factor for higher negative emotionality, regardless of the effects of time spent in bed and sleep complaints [128].
Chronotypes may regulate mood by adjusting phase relationship between sleep and other physiological rhythms. Individuals with evening preference displayed phase delays in core body temperatures and melatonin rhythms when compared with morning-types [129, 130]. It has been reported that the interval between circadian phase of melatonin or core temperature rhythms and usual wake time was longer in morningtypes. Thus, while evening-types wake up at a later clock hour than morning-types, morningtypes actually wake up at a later circadian phase [131]. In addition, the variance of circadian phase was greater among subjects with delayed sleep types [132]. For evening-types, the relative delay of melatonin or core body temperature rhythms against sleep phase leads to internal desynchronization and thus may increase the risk for affective disorders. Indeed, some circadian interventions have been reported to be effective for reducing depressive symptoms, such as light therapy and chronotherapy [133, 134].
In addition, eveningness is linked to mood dysregulation. Cognitive reactivity is the extent to which negative thoughts become activated when mood is low, and it is a vulnerability marker of affective disorders. Cognitive reactivity may mediate the effects of chronotype on depression status, even when controlling for insomnia [135]. In addition, eveningness has been reported to be associated with impaired emotional regulation (i.e. reduced cognitive reappraisal and increased expression suppression) after controlling for factors, including sleep quality. This may confer a risk for future depression [136].
Both chronotypes and affective disorders are affected by multiple genetic and environmental factors. Some clock gene polymorphisms have been reported to be associated with chronotype and affective disorders, providing some insights regarding how chronotypes may affect mood, but the underlying mechanisms need further characterization. In recent years, neurobiological research has revealed key circuits regulating mood, providing new directions to investigate for circadian rhythm and mood regulation. In the future, a combination of approaches at molecular, cellular, circuit, and system levels shall facilitate further elucidation of the mechanisms underlying the connections between chronotype and affective disorders.
Footnotes
Conflict of interests
All contributing authors have no conflict of interests related to this paper.
Acknowledgements
This work was supported by grants from the Natural Science Foundation of China (No. 31930021, No. 31671360) to Luoying Zhang, and China Postdoctoral Science Foundation (No. 2018M632826) to Qiang Gao.