
Abstract
Adenomyosis is described as the benign invasion of endometrium into the myometrium, with endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium. It may affect 20% of female population and most widely seen among perimenopausal and multiparous women. Its etiopathogenesis, diagnosis, clinical findings and current various treatment options will be discussed in this article.
Keywords
Definition & etiopathogenesis
Adenomyosis is traditionally described as ‘the benign invasion of endometrium into the myometrium, producing a diffusely enlarged uterus which microscopically exhibits ectopic non-neoplastic, endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium’. Adenomyosis may be present in diffuse or focal forms, named as adenomyotic cysts or adenomyomas, subsequently. It is shown to be affecting 20% of female population, but is most prevalent among perimenopausal and multiparous women [1–4]. Adenomyosis was first described in 1860 by the German pathologist Carl von Rokitansky when he observed endometrial glands in the myometrium, calling it ‘cystosarcoma adenoid uterium’ [5]. In 1925, Frankl used the term ‘adenomyosis’ as it does not imply an inflammatory process to the situation where ‘the direct connection of the endometrium with the islands of mucosa located in the musculature can be established in serial sections’. Therefore, adenomyosis came to be identified as an entity separate from endometriosis [4]. However, the year was 1972 when the clearest definition of adenomyosis was made by Bird et al. [5,6] as “benign invasion of endometrium in the myometrium, producing a diffusely enlarged uterus, which microscopically exhibits ectopic, non-neoplastic, endometrial glands and stroma surrounded by hypertrophic and hyperplastic myometrium”.
The diagnosis of adenomyosis can now be made by using less invasive techniques such as ultrasound and MRI and analysis of histological specimens obtained at hysteroscopic biopsy. Although the diagnosis is usually made in women in their forties and fifties with symptoms, adenomyosis is being found incidentally in younger women undergoing infertility evaluations or who have signs and symptoms of dysmenorrhea and menorrhagia [5].
Various theories about the etiopathogenesis of adenomyosis have been proposed so far. However, the exact cause is still unknown. The first and most popular hypothesis is that adenomyosis develops from invagination of endometrium into the myometrium. It is proposed that, invagination may occur due to weakened myometrium from tissue trauma during previous pelvic surgery, thus enabling the active endometrial tissue to grow into the injured lining [7]. A second theory is that adenomyosis develops de novo from embryologic misplaced pluripotent Mullerian remnants. A third theory suggests that invagination of the basalis proceeds along the intramyometrial lymphatic system, leading to adenomyosis. In addition to those, a recently proposed theory is that adenomyosis originates from bone marrow stem cells that are displaced through the vasculature [5,8]. Steroid hormones have also been emphasized in the pathogenesis, mostly focusing on local rather than systemic hyperan-drogenism [9]. The P450 aromatase protein was localized in adenomyotic glands and mRNA for aromatase CYP450 was localized in adenomyotic tissue homog-enate as well [10]. The action of aromatase on androgen precursors [11] and estrone sulfatase acting to convert estrone-3-sulfate to estrone [12] may be involved in the pathogenesis; also relatively higher E2 levels which are detected in menstrual blood compared with peripheral blood in women with adenomyosis may be associated with these findings [13]. Some evidence also suggests altered 17β-hydroxysteroid dehydrogenase type 2 in the endometrium in women with adenomyosis resulting in increased conversion of E2 to estrone during the secretory phase of the cycle [14].
Diagnosis & clinical findings
Clinical findings of menorrhagia and dysmenorrhea associated with an enlarged uterus suggest the presence of adenomyosis. However, the diagnosis is made by histologic examination. Enlarged globular uterus that can be observed macroscopically, is caused by the smooth muscle cell hyperplasia and hypertrophy due to the presence of proliferative ectopic endometrial tissue in the myometrium. Adenomyosis can also be observed as adenomyomas, which arise in focal forms of circumscribed nodular aggregates of smooth muscle, endometrial glands and stroma, or can also present as a polypoid mass within the endometrial cavity [15]. Adenomyosis tends to be a diffuse process arising most frequently in the posterior wall, less frequently in the anterior wall and rarely in the cornua or areas near the cervical os [5]. The criterion for minimal depth of invasion is not certainly established; however, most studies suggest the use of a cutoff value of 2.5 mm below the basalis layer [16]. Diagnostic hysteroscopy is not useful in providing pathognomonic signs of adenomyosis, even though some evidence suggests that various hysteroscopic findings such as irregular endometrium with pitting endometrial defects, increased vascularization and cystic hemorrhagic lesions may be associated with the process [17].
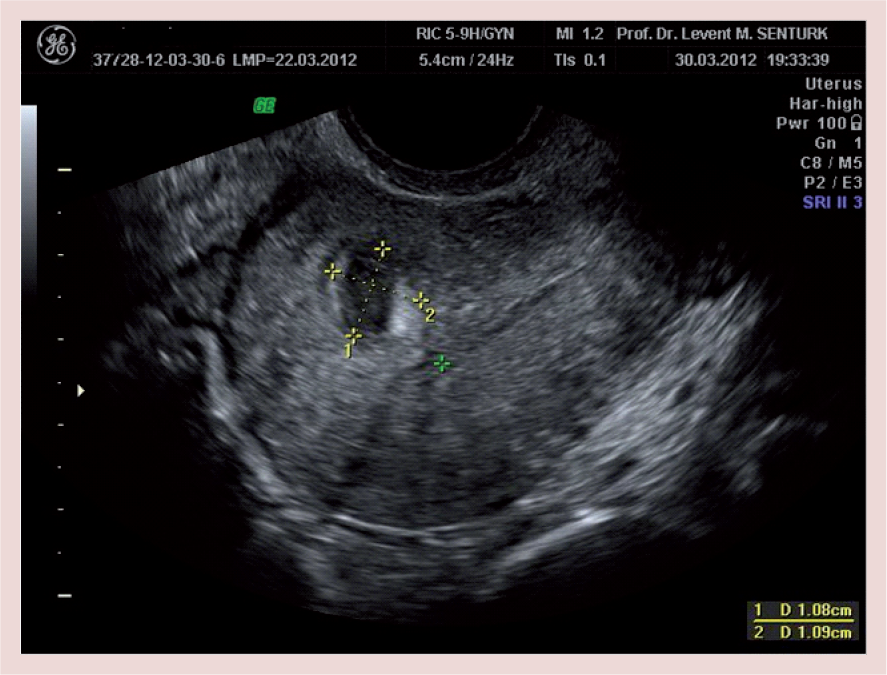
Although the diagnosis of adenomyosis is made histologically, several imaging techniques have been useful in the differential diagnosis including ultrasound and MRI. Both transvaginal ultrasound (TVUS) and transabdominal sonography characterize adenomyosis by identifying myometrial cysts (1–7 mm round anechoic areas), distorted and heterogeneous myometrial echogenity and poorly defined foci of abnormal myometrial echogenity [5,18]. The most sensitive ultrasound finding of adenomyosis is the presence of ill-defined myometrial heterogeneity (sensitivity, 88%; accuracy, 75%) while the most specific ultrasonographic feature (specificity, 98%; accuracy, 78%) is the presence of myometrial cysts [4]. Findings at MRI include a large asymmetric uterus without leiomyomas, thickening of the junctional zone (JZ) from 8 to 12 mm, or an abnormal ratio of JZ to myometrial thickness greater than 40%. The JZ is the innermost myometrial layer, which is distinct at light optic microscopy but lacks histologic distinction. Thickening of the JZ on MRI is the consequence of inordinate inner myocyte proliferation, a process that has been referred to as ‘junctional zone hyperplasia’ [5,18].
The use of 3D ultrasound which enables assessment of the lateral and fundal aspects of the JZ and provides clearer visualization of endometrial protrusion into the myometrium has been reported recently [19]. Using 3D TVUS, the best markers are related to the JZ myometrium. A difference (JZdi) of greater than or equal to 4 mm between the area of maximum thickness (JZmax) and the area of minimum thickness (JZmin) and its distortion and infiltration had high sensitivity (88%) and best accuracy (85 and 82%, respectively). Overall, for 2D and 3D TVUS, the accuracy was 83 and 89%; sensitivity was 75 and 91%; specificity was 90 and 88%; positive predictive value was 86 and 85%; and negative predictive value was 82 and 92%, respectively [20]. Therefore, it seems that a diagnosis of adenomyosis might be achieved when one or more of the following sonographic findings are present: poor definition of the endometrial-myometrial interface; a globular uterine enlargement; myometrial anterior-posterior asymmetry; subendometrial echogenic linear striations; intramyometrial cysts; a heterogeneous myometrial echo texture; and Doppler flow visualization of radial arteries running through (not around) the myometrial lesions
Sensitivity of TVUS gradually decreases to as low as 33% when fibroids are present, in particular when the volume of the myoma is greater than 300 ml [23]. However, overall review of the literature demonstrates that TVUS exhibits sensitivity of 53–89% and specificity of 50–99% for the diagnosis of adenomyosis when no fibroids are present [5,18,23–24]. In cases with coexistent adenomyosis and fibroids, MRI demonstrated sensitivity of 67% and specificity of 82% compared with sensitivity of 87% and specificity of 100% when fibroids were absent. In summary, TVUS is an excellent first-choice imaging method for use by experienced sonographers; however, MRI can be used as an adjunct in cases with coexisting uterine abnormalities. The combination of both techniques offers the highest sensitivity for preoperative diagnosis [5,23].
Because the diagnosis of adenomyosis is made by histologic analysis, the exact incidence has not been accurately determined. In various studies, the prevalence has been reported to range from 5 to 70% [25]. Results of a meta-analysis reported the probability of adenomyosis with a normal TVUS as 9.1% (95% CI: 7.3–11.1) and the probability with an abnormal TVUS as 66.2% (95% CI: 61.6–70.6) [26]. Overall, the mean frequency of adenomyosis at hysterectomy is approximately 20–30% [27,28]. Clinical series have demonstrated an increased frequency of adenomyosis in multiparous patients [28,29]. Pregnancy may be a risk factor due to the invasive nature of the trophoblasts into the myometrium during implantation. Vercellini et al. [28], observed that the frequency of adenomyosis was directly associated with the number of pregnancies. Some studies have suggested that trauma from pelvic surgery may trigger invagination of the adenomyotic tissue. Parazzini et al. [27], also observed higher rates of adenomyosis in patients who had undergone dilation and curettage. 70–80% of adenomyosis cases are reported in women in the fourth and fifth decades of life. 5–25% of adenomyosis cases are observed in patients younger than 39 years, and only 5–10% occur in women older than 60 years [5,25]. Early menarche and obesity are also suggested as risk factors [30]. Fifty percent of women with symptoms have menorrhagia, 30% have dysmenorrhea and 20% have metrorrhagia. Less common symptoms include dyspareunia and chronic pelvic pain [7,15]. Endometriosis is observed in 6–22% of patients with adenomyosis, and myomas are concurrently observed in 35–55% of patients [7]. In a retrospective case–control study, comparing leiomyoma and adenomyosis cases, Taran et al. revealed the independent association between adenomyosis and history of depression (57.1 vs 24.7%), younger age (41.1 vs 44.3 years), pelvic pain (52.9 vs 21.1%) and dysmenorrhea (65.7 vs 42.3%) in a multivariable unconditional logistic regression analysis comparing women with leiomyomas [29]. Moreover, women with adenomyosis were more likely to have a history of depression (52.6 vs 22.2%) and endometriosis (26.3 vs 2.8%) compared with women with leiomyomas in a second multivariate model where all subjects had the uterus weighing more than 150 g.
Treatment of adenomyosis
The standard treatment of adenomyosis is hysterectomy. However, the major issue is treating symptomatic women with conservative medical or surgical options to maintain fertility. Up to now, there exists no medical therapy to treat symptoms of adenomyosis while allowing patients to conceive. Medical treatments using suppressive hormonal treatments such as continuous use of oral contraceptive pills, high-dose progestins, the levonorgestrel-releasing intrauterine system (LNG-IUS), danazol and GnRH (gonadotropin-releasing hormone) agonists can temporarily induce regression of adenomyosis.

Various diagnostic criteria for adenomyosis on 2D transvaginal ultrasonography such as ‘poor definition of the endometrial-myometrial interface’, ‘a globular uterine enlargement’, ‘myometrial anterior-posterior asymmetry’, ‘subendometrial echogenic linear striations’ and ‘intramyometrial cysts’.
Continuous use of oral contraception in patients with symptoms of adenomyosis such as dysmenorrhea and menorrhagia may benefit from induction of amenorrhea. Use of high-dose progestins such as continuous oral norethindrone acetate or subcutaneous depot medroxyprogesterone as suppressive hormonal agents can also help temporarily in inducing regression of adenomyosis. However, there are no randomized controlled trials on these agents up to now [5].
The most promising medical therapy based on the literature is the LNG-IUS because of its ability to provide hormonal suppression to improve symptoms, with a low profile of adverse effects, while enabling women to maintain future fertility. The LNG-IUS releases 20 µg of levonorgestrel daily and seems to be an effective treatment for adenomyosis. The LNG-IUS has proved to decrease symptoms of dysmenorrhea and menorrhagia, increasing the hematocrit concentration following 3 months of treatment. The use of LNG-IUS is associated with decidualization of the endometrium and is also thought to act directly on adenomyotic deposits by downregulating the estrogen receptors. This, in turn, reduces the size of adenomyotic foci, improves contractility of the uterus to decrease blood loss and improves dysmenorrhea by reducing prostaglandin production within the endometrium. Studies have demonstrated that use of the LNG-IUS results in improvement of symptoms such as menorrhagia and dysmenorrhea, and radiologic changes in adenomyotic uterus. However, none of these studies were randomized controlled trials, and patients were not followed up after removal of the IUD. In a recent prospective randomized clinical trial, it has been reported that LNG-IUS demonstrates significant and comparable improvements in hemoglobin levels to hysterectomy in treating adenomyosis-associated menorrhagia during the first year. Although both treatments lead to improvements in health-related quality of life, LNG-IUS seems to have superior effects on psychological and social life [31]. Therapy with the LNG-IUS may be beneficial in women who desire to conceive after removal of the IUD [16,32–34]. Adverse effects include breakthrough bleeding, headache, breast tenderness, acne and weight gain [5].
Danazol, a 19-nortestosterone androgen derivative with progestin-like effects, induces direct inhibition of ovarian enzymes responsible for estrogen production and pituitary gonadotropin secretion. After systemic treatment with danazol, estrogen receptors are decreased, which may contribute to reduced uterine size and improvement of symptoms. Experience with the use of systemic danazol therapy in patients with adenomyosis is limited due to the adverse effects, which includes weight gain, muscle cramps, reduced breast size, acne, hirsutism, oily skin, decreased high-density lipoprotein levels, increased liver enzyme concentrations, hot flashes, mood changes, depression and deepening of the voice [35]. Igarashi evaluated 14 women who received a danazol-loaded IUD containing 300–400 mg danazol [36]. Thirteen of these 14 women experienced improvement in dysmenorrhea and menorrhagia. Following removal of the danazol-loaded IUD, three of four infertile patients were able to conceive [36]. Cervical injections of danazol have also been successful with 60% improvement in subjective symptoms such as bleeding, pain and dyspareunia, and a decrease in uterine size [37]. No adverse effects were noted as a result of local administration of danazol [36,37].
Several case series reported that infertile patients with adenomyosis who had received short-term treatment with GnRH agonists were able to conceive within 6 months of cessation of therapy. Results demonstrated a reduction in uterine volume and amenorrhea and relief of severe dysmenorrhea. However, on discontinuation of therapy, symptoms recurred and uterine volume increased to the initial volume [38–42]. Although, aromatase inhibitors have been successfully used in the treatment of severe endometriosis [43], there are yet no reported studies examining its role in the treatment of adenomyosis [5].
It has been widely suggested that adenomyosis is not associated with infertility [44]. Indeed, infertility is considered as a less frequent complaint because uterine adenomyosis is usually diagnosed in the fourth and fifth decade of life. Nevertheless, an increasing number of women defer their first pregnancy until later in their 30s or 40s. Therefore, adenomyosis is more frequently encountered throughout the diagnostic workup of infertility treatment options. In addition to this, adenomyosis is currently not considered a widely accepted cause for implantation failure during IVF treatment [45], since vast majority of gynecologists do not screen or treat the condition before embarking on IVF/ICSI (intracytoplasmic sperm injection) cycles on a routine basis [46]. Most of the studies focusing on the effects of adenomyosis on IVF/ICSI cycles have all used long downregulation protocol. It is suggested that long downregulation protocol establishes a period of estrogen deficiency that may temporarily inactivate adenomyosis and normalize some of the distorted endometrial functions seen in the condition, thus enabling the observation of absence of any affect of adenomyosis on implantation. A very recent study has shown a clear implantation deficit in a cohort of ultrasound diagnosed adenomyosis patients exclusively undergoing GnRH antagonist ovarian stimulation for IVF cycles. These results suggest to consider using long (preferably very long downregulation: 3–6 months duration) downregulation in the ovarian stimulation as the preferred IVF treatment option in adenomyosis patients, especially if they have already failed several GnRH antagonist cycles [44]. Based on results from this and other previous studies [47,48], which failed to show a negative effect of using a long downregulation protocol on pregnancy outcome in patients with adenomyosis, it may be reasonable to consider a long downregulation ovarian stimulation protocol as the preferred IVF treatment in these patients, especially with an accompanying history of several cycle failures with GnRH antagonist administration. The results of the study with the highest quality also obtained prospective controlled evidence stating reduced rates of implantation, clinical pregnancy and ongoing pregnancy, along with increased rates of first-trimester miscarriage after antiretroviral therapy (ART) in women with adenomyosis diagnosed on ultrasound when compared with controls [49]. As the authors, we have experienced successful pregnancies in several patients with adenomyosis diagnosed with ultrasonography, using ultra-long downregulation (3 months) protocol in ART
In addition to those, as a consequence of the destruction of the normal architecture of the JZ myometrium, abnormal uterotubal sperm transport has been hypothesized to be the main reason for adenomyosis-associated subfertility [50,51]. In studies that evaluated the function of uterotubal sperm transport by hysterosalpingoscintigraphy (HSSG), spontaneous pregnancy rates or pregnancy rates after intrauterine insemination were reported to be as low as 10% among the subjects with a negative HSSG (no or minimal uterotubal sperm transport) [51,52]. An abnormal HSSG was more prevalent in women with diffuse adenomyosis (78%) than in women with focal adenomyosis (54%) or women without adenomyosis (37%) in a subanalysis of 50 patients with endometriosis. This finding suggested a dose–response relationship between the degree of adenomyosis and the degree of abnormal uterotubal transport [51].
HOXA10 gene expression in the endometrium was recently shown to be significantly lower during the midsecretory phase in women with adenomyosis compared with fertile controls [53], similarly to the leukemia inhibitory factor [54]. However, none of these studies were able to exclude the presence of endometriosis clearly. Nonetheless, this gene and its expression seem to be involved in impaired implantation in women with adenomyosis.
In women who have completed childbearing, less invasive surgical procedures such as endometrial ablation and resection have been demonstrated to improve symptoms of menorrhagia, with a mean failure rate of 20%. Higher failure rates are noted if adenomyosis has penetrated more than 2.5 mm from the basalis layer [55]. Other conservative surgical treatments such as adenomyotic muscle excision, reduction and electrocoagulation can be performed but are usually not as effective as hysterectomy because of the difficulty in completely excising or coagulating the foci. The outcomes of these procedures have demonstrated low pregnancy rates because of reduction in uterine volume and scarring. In women who wish to maintain fertility, excision can be performed if sufficient myometrium is left and if scar formation does not interfere with uterine expansion [56–58]. The rate of spontaneous abortion (38.8%) were reported to be higher than in the general population after the excisional procedure. This is likely due to uterine scar tissue formation, which can affect the gestation capability of the uterus [59]. However, a small study demonstrated that conservative treatment with adenomyoma excision (mean size: 55 mm) resulted in a 70% pregnancy rate (49 of 71 patients), with relief of symptoms of menorrhagia and dysmenorrhea [60,61]. In another prospective case series followed for 10 years from June 1998 to August 2008, 104 women with severe adenomyosis verified histologically and with MRI were analyzed [56]. Of 26 women who wished to conceive, 16 became pregnant, 14 (53.8%) went to term and delivered a healthy baby and there were no cases of uterine rupture.
Newer techniques such as uterine artery embolization (UAE) and ‘magnetic resonance-guided focused ultrasound surgery’ need further study and are not appropriate currently for the patients seeking fertility. Popovic et al. [62] recently published the results of a review of 15 studies with data of 511 women with adenomyosis and adenomyosis associated with uterine leiomyomas. In this analysis, short-term outcomes regarding symptom relief after UAE for pure adenomyosis and adenomyosis with uterine leiomyomas range from 83.3 to 92.9%, respectively. In the long term, patients report significant symptomatic improvement of 64.9 (in pure adenomyosis) and 82.4% (in adenomyosis with leiomyomas). In general, improvements were reported by 387 patients (75.7%) and the median follow-up was 26.9 months. Even though, not all of the studies involved did report the exact number of complications, 37 hysterectomies were reported among 280 patients (13.2%). Still, hysterectomy stands as a treatment option which offers full relief of symptoms associated with adenomyosis, compared with UAE [62].
Magnetic resonance-guided focused ultrasound surgery is a new noninvasive technique for ablation of soft tissue that has been successfully used to treat leiomyomas and experimentally to treat adenomyosis. In 2004, the procedure was approved by the US FDA for the treatment of myomas. Magnetic resonance–guided focused ultrasound surgery has helped to overcome problems in precisely focusing the sonographic waves on a specific target due to the excellent anatomic resolution and high-thermal imaging sensitivity of MRI. This noninvasive procedure is now beginning to be used in patients with adenomyosis. Treatment of diffuse and generalized adenomyosis may be difficult, however, a case report demonstrated a successful outcome in focal disease, with marked reduction in bleeding and followed by an uncomplicated pregnancy and delivery [63,64]. However, it will be wise to keep in mind that currently, hysterectomy remains the standard treatment for adenomyosis in women who have completed childbearing.
Conclusion
Adenomyosis is described as the benign invasion of endometrium into the myometrium, with endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium. It may be present in diffuse or focal forms. Adenomyosis may affect 20% of female population and most widely seen among perimenopausal and multiparous women. Menorrhagia, dysmenorrhea and metrorrhagia are the major clinical symptoms whereas dyspareunia and chronic pelvic pain may be summarized as the less common symptoms. It has been widely suggested that adenomyosis is not associated with infertility. However, based on the limited available evidence, the presence of a causal association between adenomyosis and subfertility may be suggested. Adenomyosis is associated with lifelong infertility in baboons and is also associated with impaired reproductive outcome following ART. Moreover, a dose–effect relationship between the degree of abnormal uterotubal contractility and the degree of adenomyosis has been demonstrated. The standard treatment of adenomyosis is hysterectomy. Up to now, there exists no medical therapy to treat symptoms of adenomyosis while allowing patients to conceive. In women who have completed childbearing, less invasive surgical procedures such as endometrial ablation and resection have been demonstrated to improve symptoms of menorrhagia. Newer techniques such as uterine artery embolization and ‘magnetic resonance-guided focused ultrasound surgery’ need further study and are not appropriate currently for the patients seeking fertility. Hysterectomy still stands as a treatment option which offers full relief of symptoms associated with adenomyosis, compared with the newer techniques.
Future perspective
Over the next 5–10 years, ultra-long downregulation protocols will be preferred during IVF/ICSI cycles for women with suggestive symptoms or signs of adenomyosis. In the meantime, the diagnosis of adenomyosis should be standardized according to the internationally agreed criteria. Moreover, potential consequences of adenomyosis in terms of poor obstetrical outcome, such as spontaneous miscarriage, preterm birth, intrauterine growth retardation, preeclampsia, eclampsia, placental bed and adherence abnormalities as well as obstetrical haemorrhages should be studied with well-designed studies. Finally, the effect of new surgical techniques and new pharmacological agents on the quality of life of patients with adenomyosis should be evaluated.
No writing assistance was utilized in the production of this manuscript.
Executive summary
Adenomyosis is described as the benign invasion of endometrium into the myometrium, with endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium.
Adenomyosis may affect 20% of female population and most widely seen among perimenopausal and multiparous women.
Menorrhagia, dysmenorrhea and metrorrhagia are the major clinical symptoms whereas dyspareunia and chronic pelvic pain may be summarized as the less common symptoms in women with adenomyosis.
The presence of a causal association between adenomyosis and subfertility may be suggested. Adenomyosis is associated with lifelong infertility in baboons and is also associated with impaired reproductive outcome following antiretroviral therapy. Moreover, a dose–effect relationship between the degree of abnormal uterotubal contractility and the degree of adenomyosis has been demonstrated.
Up to now, there exists no medical therapy to treat symptoms of adenomyosis while allowing patients to conceive.
In women who have completed childbearing or who do not wish to have baby for the moment, use of levonorgestrel-releasing intrauterine system, less invasive surgical procedures such as endometrial ablation and resection have been demonstrated to improve symptoms of menorrhagia.
Newer techniques such as the uterine artery embolization and ‘magnetic resonance-guided focused ultrasound surgery’ need further study and are not appropriate currently for the patients seeking fertility.
The standard treatment of adenomyosis is hysterectomy.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.