
Abstract
Objective:
The purpose of this study was to understand how Canadian Obstetricians/Gynaecologists (OBGYNs) diagnose and manage adenomyosis.
Methods:
This cross-sectional study was performed via an online survey distributed to 262 OBGYNs at three Canadian universities (University of Toronto, University of Calgary, and McMaster University).
Results:
A total of 137 responses were obtained out of 262 OBGYNs (52.3%) with a completion rate of 98%. Adenomyosis was a diagnosis in 6%–10% of patients seen by OBGYNs. The most common clinical symptoms included heavy menstrual bleeding (HMB) (82.8%) and dysmenorrhea (91.0%). Most participants (83%) used transvaginal ultrasound (TVUS) as first-line imaging for diagnosis of adenomyosis. Many respondents (35.8%) indicated that adenomyosis was not associated with infertility or recurrent miscarriage. Treatment considerations for all patients with adenomyosis included levonorgestrel intra-uterine system (LNG-IUS) (91.8%), hysterectomy (88.8%), expectant management (85.1%), combined hormonal contraceptives (CHC) (83.6%), tranexamic acid (81.3%), gonadotropin releasing hormone (GnRH) agonists (64.2%), depo-provera (64.2%), dienogest (57.5%), and norethisterone acetate (NETA) (40.3%). Treatments for adenomyosis in patients wishing to conceive included expectant management (85.1%), tranexamic acid (79.1%), CHC (44.8%), LNG-IUS (32.8%), and GnRH agonists (35.8%). Excision of adenomyosis would only be offered by 24% of respondents. Uterine artery embolization (UAE) would not be used in the treatment of adenomyosis by 44% of respondents. Finally, 82.8% of respondents would use improvement of clinical symptoms to follow treatment success.
Conclusion:
Practice varies across Canada despite recent emerging evidence in the diagnosis and management of adenomyosis, highlighting the need for a clinical practice guideline on adenomyosis.
Introduction
Historically, adenomyosis was a histologic diagnosis defined by the presence of endometrial glands and stroma within the myometrium with surrounding myometrial changes. 1 Recent development of radiographic criteria for adenomyosis based on transvaginal ultrasound (TVUS) and magnetic resonance imaging (MRI) have led to changes in diagnostic sensitivity and disease epidemiology. 2
TVUS is now the first-line diagnostic test for adenomyosis with a sensitivity of 83.8% and specificity of 63.9%; MRI is considered second-line when TVUS is equivocal. 3 Imaging advancements have revealed a high prevalence (30%) of adenomyosis in pre-menopausal women with the majority (80%) experiencing distressing symptoms of heavy menstrual bleeding (HMB) or dysmenorrhea.2,4,5 Reproductive outcomes, such as infertility, miscarriage, assisted reproductive therapies failure, and adverse pregnancy outcomes, have also been associated with adenomyosis. 3 In a significant number of women, adenomyosis can co-exist with other gynaecological pathology such as endometriosis and fibroids, worsening the symptom profile of any one pathology alone. 2
While hysterectomy remains the definitive treatment, current evidence supports the levonorgestrel intra-uterine system (LNG-IUS) and dienogest as effective therapies in adenomyosis.6,7 Less well-studied medical treatments include norethisterone acetate (NETA), gonadotropin releasing hormone (GnRH) agonists, combined hormonal contraceptives (CHCs), and other progestins. 6 Emerging interventional therapies include uterine artery embolization (UAE) and high-intensity focused ultrasound (HIFU) with high patient satisfaction rates.8,9 Adenomyomectomy or an excision of focal or diffuse adenomyosis may be offered to patients wishing to maintain fertility or avoid hysterectomy. 10
We aimed to determine the current practice of Canadian OBGYNs in the diagnosis and management of adenomyosis in light of emerging literature.
Materials and methods
This cross-sectional survey was disseminated to faculty OBGYNs at three large academic sites across Canada (University of Toronto, University of Calgary, and McMaster University) of which 262 were eligible based on practice scope (general OBGYN, Minimally Invasive Gynaecologic Surgery (MIGS), Reproductive Endocrinology and Infertility (REI), and Urogynaecology). The questionnaire (Supplemental Material) was developed by three of the authors. Prior to dissemination, three clinicians from other institutions with expertise in MIGS piloted the survey to optimize feasibility, clarity, and nation-wide applicability. The survey was designed to determine the knowledge and practice of Canadian gynaecologists on (1) the epidemiology of adenomyosis, (2) the symptomology of patients presenting with adenomyosis, (3) methods for diagnosis, (4) management strategies, (5) association of adenomyosis with fertility, and (6) approach to management in a patient wishing to conceive.
This open survey was hosted on two platforms in an effort to increase accessibility of the questionnaire: Google Forms and Simple Survey. A recruitment email was both centrally distributed to all faculty members and distributed at each affiliated regional hospital site. Four reminder emails were sent over a period of 6 months. There was no incentive for completion. All responses were anonymous. Two questions required a response to access the survey: (1) consent to participate and (2) practice including gynaecology; responses to all other questions were elective. There were 26 questions in total. One to two questions were displayed per page with a total of 15 pages. Question responses were a combination of multiple choice, multi-select options, yes/no, and short answer. Respondents were able to review and change their answers to previous questions. Responses were collected from February to September 2020.
The number of participants who provided consent was used to determine the participation rate. Demographic data was also collected, and survey responses were considered complete if the demographic section was completed. The data was downloaded from both survey sites into Microsoft Excel and analyzed using descriptive statistics.
This study was approved by the Research Ethics Board at Mount Sinai Hospital.
Results
Demographics
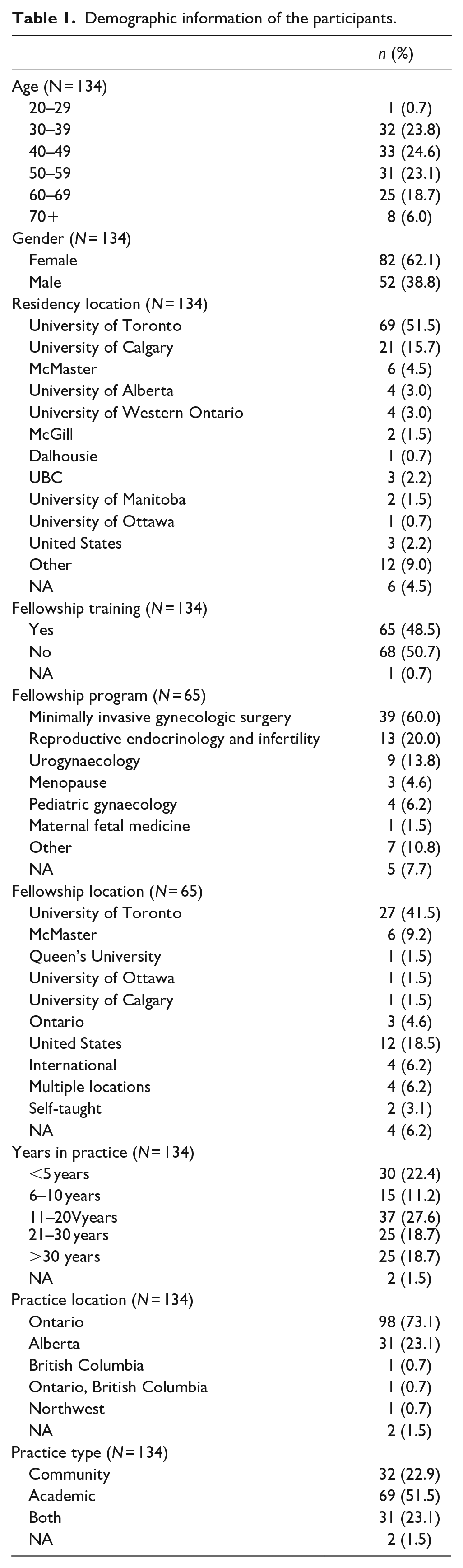
The participation rate was 52.3% with a completion rate of 98%; 134 completed responses were ultimately included in data analysis. All age range groups were represented within this study. The majority of participants completed their residency training at either the University of Toronto (51.5%) or the University of Calgary (15.7%), with nearly half (48.5%) completing additional training in the form of a fellowship. The majority (60%) of those with a fellowship completed their training in MIGS, with another 20% in REI and 13.8% in Urogynaecology. Most respondents had over 11 years of practice experience with 51.5% being in an academic setting. Demographic information is shown in Table 1.
Demographic information of the participants.
Epidemiology of adenomyosis
The majority of participants recalled diagnosing between 6% and 10% of patients with adenomyosis with a range from 0% to 50%. The distribution of age that a participant would consider a diagnosis of adenomyosis is depicted in Figure 1. Interview participants were more likely to consider a diagnosis of adenomyosis with increasing age of the patient.
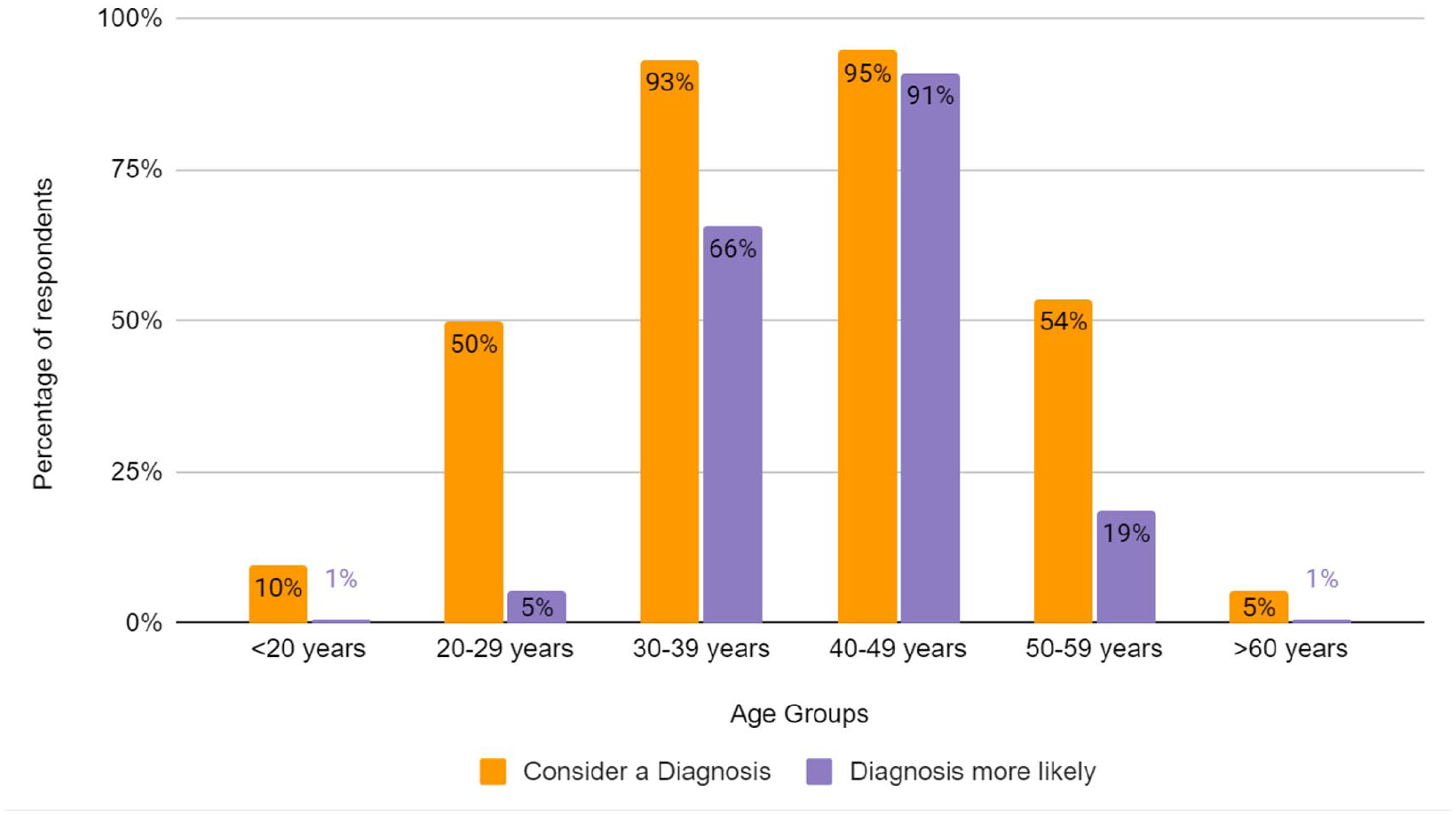
Age groups in which participants considered a diagnosis of adenomyosis (orange) compared to age groups in which they believed a diagnosis was more likely (purple). Participants were able to select all categories they believed applied.
Clinical symptoms
The most common symptoms thought to be associated with adenomyosis are illustrated in Figure 2. The two most common features of adenomyosis were felt to be dysmenorrhea (91%) and HMB (83%). Of note, only 54% of respondents felt that adenomyosis could cause infertility and only 28% of respondents thought that treatment of adenomyosis could improve fertility. Only 10% of respondents aged 50–59 thought fertility was associated with adenomyosis, compared to more than 25% in other respondent age groups. Only 10% of respondents felt that recurrent miscarriage was associated with adenomyosis.
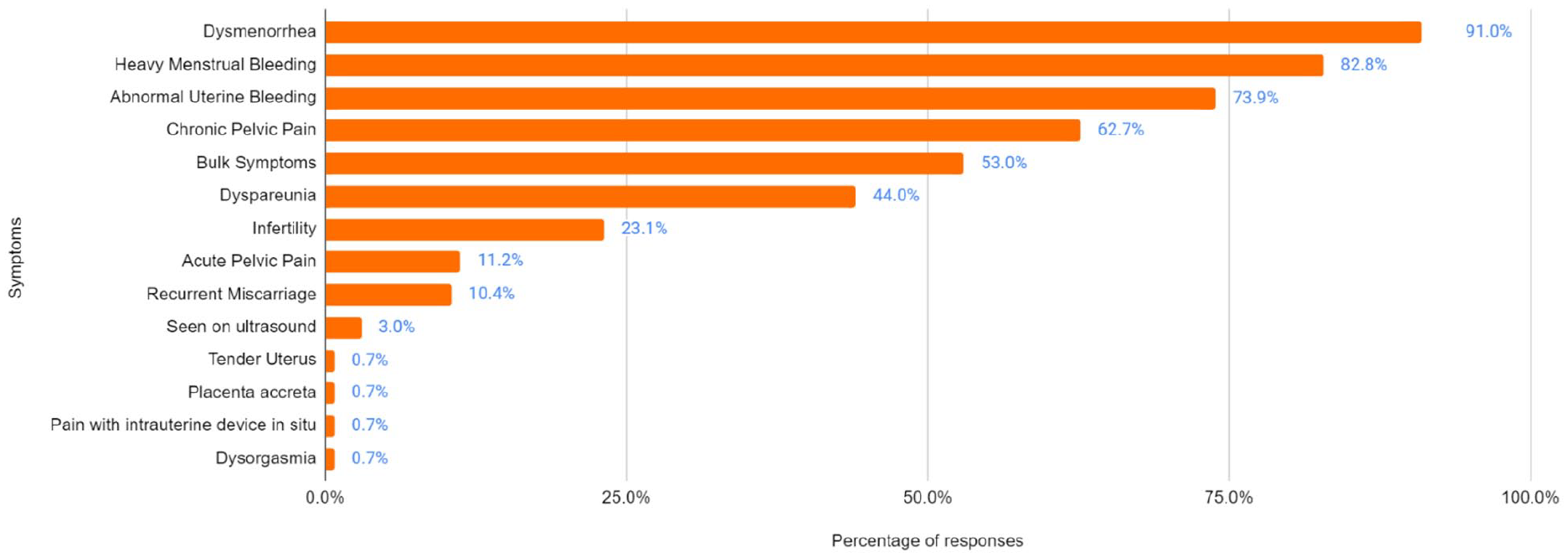
Symptoms that participants (n = 134) believed were associated with adenomyosis, in descending order. Participants were able to select all symptoms they believed applied and write in other options.
Diagnosis of adenomyosis
The majority of respondents (90%) diagnosed adenomyosis based on imaging. Clinical exam was felt to be useful in diagnosis by 75% of respondents. The majority of the respondents (83%) would order a TVUS for initial diagnosis; 7% of these respondents would also confirm the diagnosis of adenomyosis with an MRI after TVUS. Of note, a small percentage (5%) of respondents ordered an MRI as initial imaging; all these respondents were MIGS trained.
Management of adenomyosis
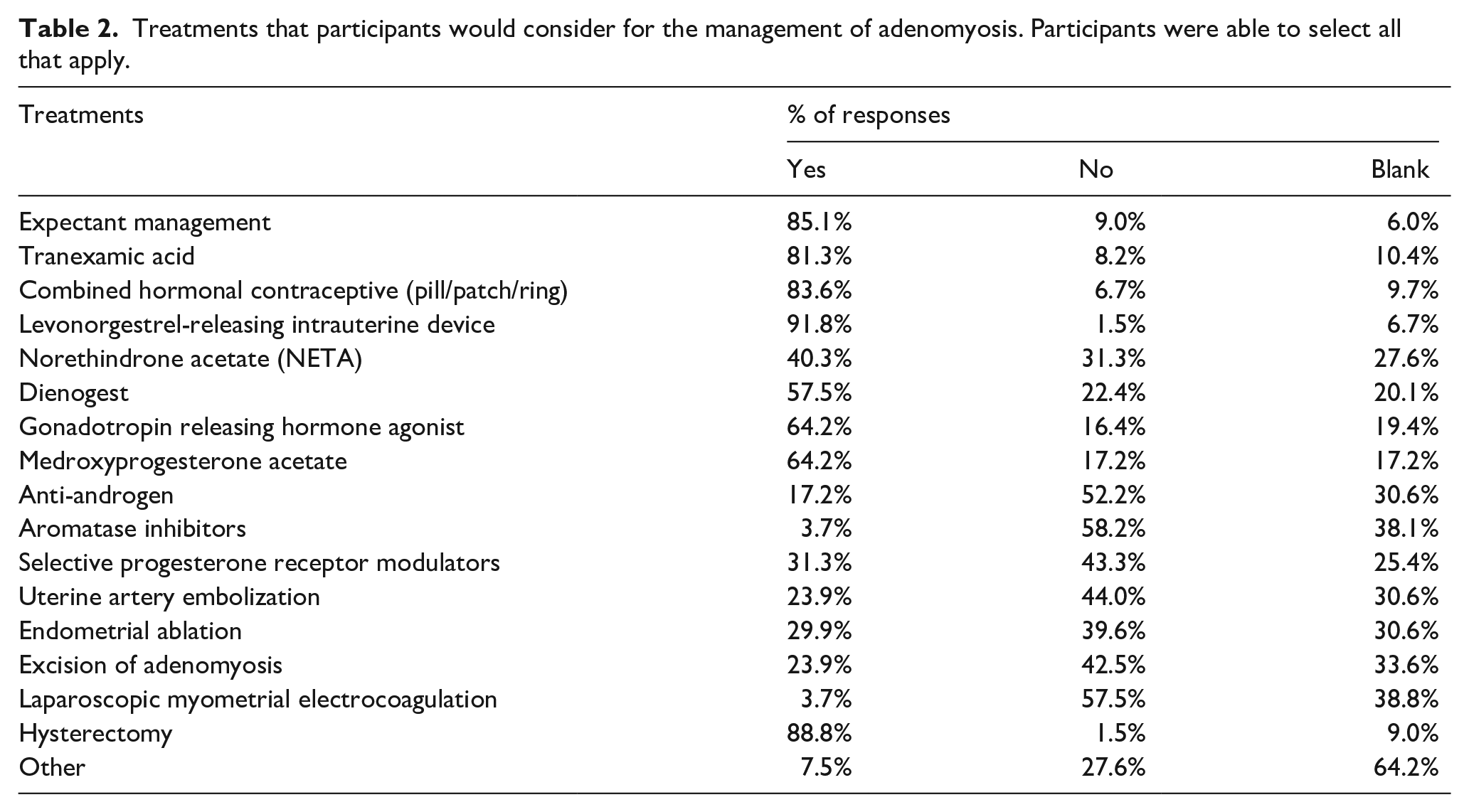
Treatments considered for adenomyosis included LNG-IUS (92%), hysterectomy (89%), expectant management (85%), CHC (84%), tranexamic acid (81%), GnRH agonists (64%), depo-provera (64%), dienogest (58%), and NETA (40%). Only 24% of respondents considered UAE and 30% would offer endometrial ablation. An adenomyomectomy would be offered by 24% of respondents overall; 68% of those who were MIGS trained would offer an adenomyomectomy while only 21% of those without MIGS training would offer adenomyomectomy. Other treatments suggested included an oral GnRH antagonist (Elagolix), NSAIDs, and HIFU.
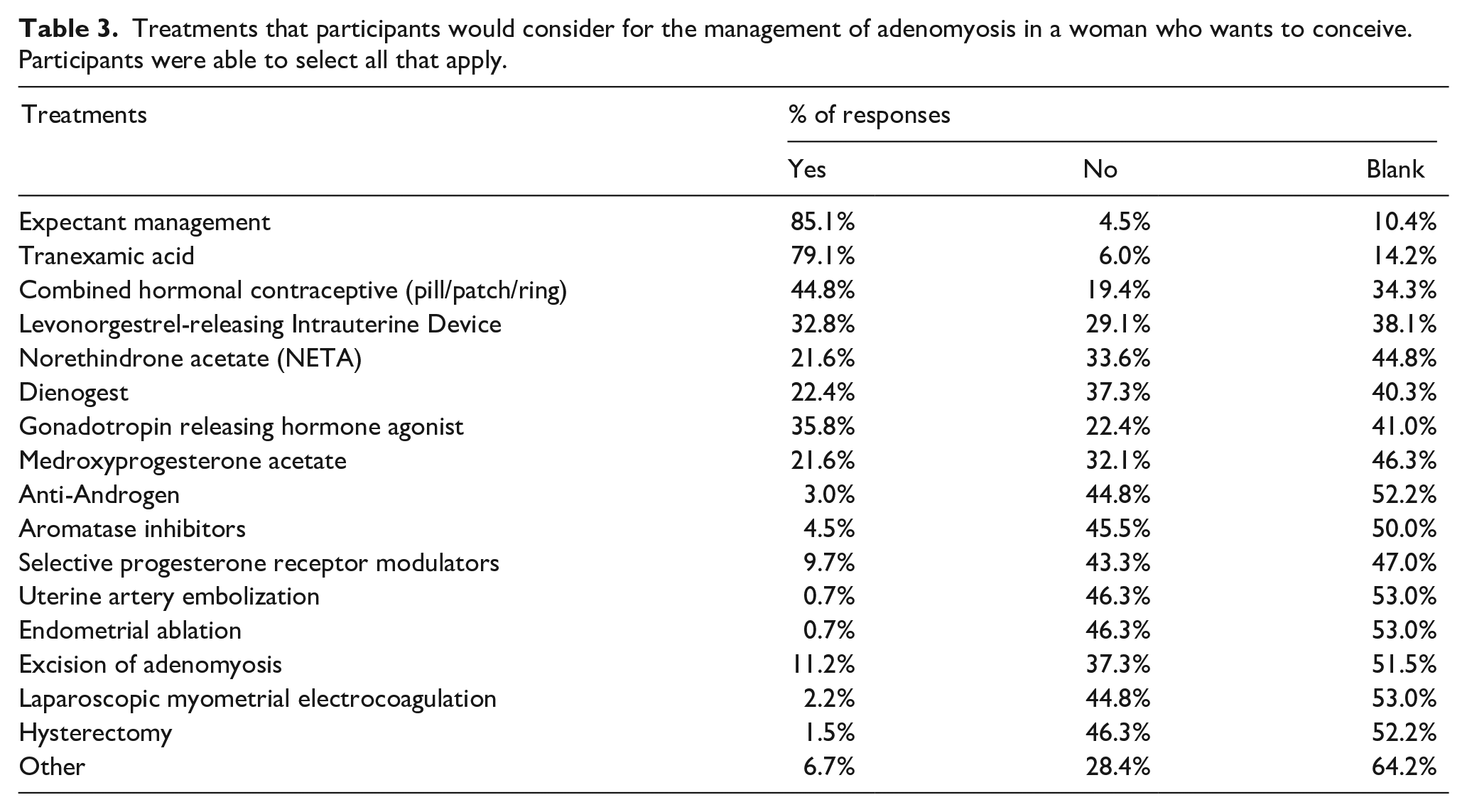
In patients wishing to conceive, treatments considered for adenomyosis included expectant management (85%), tranexamic acid (79%), CHC (45%), LNG-IUS (33%), and GnRH agonists (36%). An adenomyomectomy would only be offered by 11% of respondents; 53% of those who were MIGS trained would offer adenomyomectomy, while only 7.1% of those without MIGS training would offer adenomyomectomy. A summary of responses regarding treatments can be found in Tables 2 and 3.
Treatments that participants would consider for the management of adenomyosis. Participants were able to select all that apply.
Treatments that participants would consider for the management of adenomyosis in a woman who wants to conceive. Participants were able to select all that apply.
Follow-up
The majority of respondents (83%) measured success of treatment by improvement of clinical symptoms, while 7.5% ordered follow-up imaging (Figure 3).
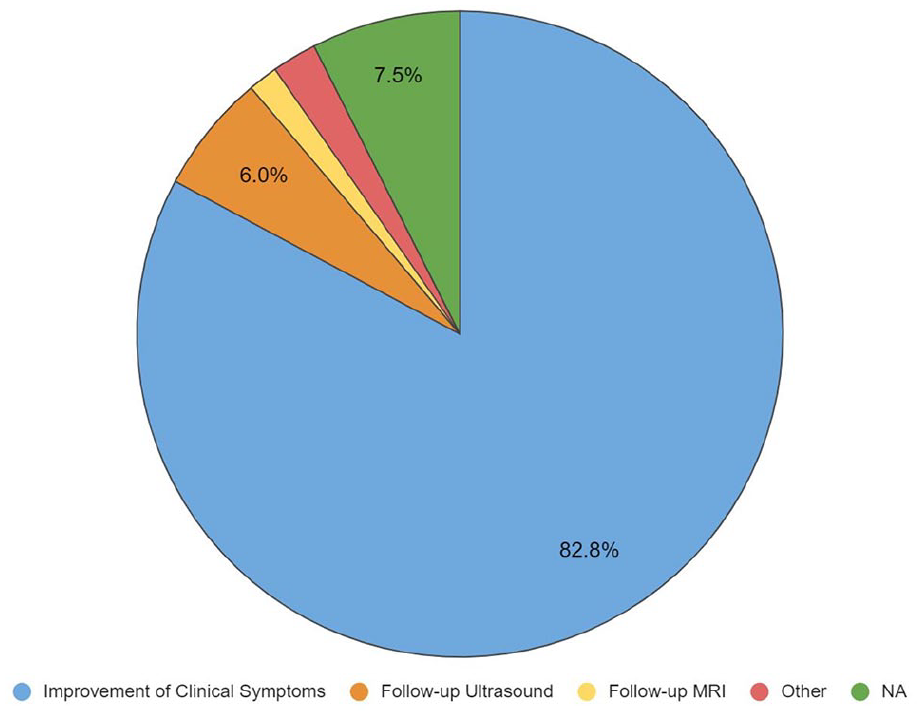
How participants would follow for treatment success.
Discussion
This study represents the first multi-center, cross-sectional survey describing the current practices in diagnosis and management of adenomyosis by Canadian OBGYNs. Given the lack of clinical practice guidelines available, this is also the first study to report current clinical practices.
In our study, adenomyosis was considered as a diagnosis in 6%–10% of patients. Interestingly, the literature reports a 15%–25% prevalence rate of symptomatic adenomyosis, which may represent underdiagnosis or a truly lower Canadian prevalence.4,5 Further, several studies have demonstrated the correlation of TVUS features of adenomyosis with symptoms of dysmenorrhea and HMB in women younger than 30.11,12 Interestingly, despite a high prevalence reported in the literature, only 6% of respondents considered adenomyosis to be a likely diagnosis in this age group.
Current literature recommends TVUS over MRI for imaging diagnosis of adenomyosis due to cost and accessibility, which is a practice widely supported by Canadian OBGYNs.3-13 The widespread use of TVUS highlights the need to adopt standardized diagnostic criteria, such as those published by the Morphological Uterus Sonographic Assessment (MUSA) group, across Canadian ultrasound facilities. 14
Current literature indicates that adenomyosis has been associated with dysmenorrhea, HMB, dyspareunia, infertility/subfertility, and recurrent pregnancy loss.15,16 Though most participants reported that adenomyosis causes dysmenorrhea and HMB, a significant number (35.8%) felt that adenomyosis does not impact fertility. Though the evidence is derived primarily from associative data, clinical consideration of the impact of adenomyosis on subfertility and recurrent pregnancy loss may benefit patients as earlier diagnosis may lead to appropriate earlier intervention and better prognosis. The current literature suggests that patients presenting with both adenomyosis and subfertility or recurrent pregnancy loss may benefit from consultation with a fertility specialist.17–19
Though the only curative treatment for adenomyosis is hysterectomy, studies now suggest that many patients require symptomatic treatment prior to the completion of childbearing. 15 Canadian OBGYNs regarded LNG-IUS, CHC, tranexamic acid, dienogest, and GnRH agonists as primary medical therapies.
The LNG-IUS was considered as a possible medical treatment by nearly all physicians in our study (91.2%). Randomized controlled trials have compared the LNG-IUS to both the gold-standard of hysterectomy and to CHC, where the LNG-IUS reduced blood loss and pain, as well as increased quality of life.6,20 Though the majority of respondents would use dienogest (57.5%), there was a high proportion that would not (22.4%). Dienogest has been shown to reduce pelvic pain in patients with adenomyosis, although it may cause irregular bleeding.21–23 GnRH agonists have been shown to be more effective in dysmenorrhea reduction compared to letrozole and dienogest. 6 CHCs are also an effective treatment, but have only been compared to LNG-IUS, which ultimately had a greater effect on symptomatic adenomyosis. 24
There are limited studies assessing the efficacy of NETA and depo-provera, though they are widely considered by the majority of respondents. 25 Similarly, despite the lack of well-controlled and specific studies assessing NSAIDs and tranexamic acid for adenomyosis, our study indicated that these are still widely used therapies.6,26 Given the diversity in considered clinical therapies, this calls for more high quality research studies comparing effective therapies in the treatment of adenomyosis.
In terms of procedural and surgical management of adenomyosis, respondents were less likely to consider those techniques as valid therapies. While it has been shown that UAE leads to significant long-term symptomatic improvement of adenomyosis in 57%–67% of patients, most study participants (44%) would not consider UAE as a treatment option. 27 HIFU is another option that has been well-studied in the treatment of adenomyosis but was not specifically included in our survey due to its limited availability in Canada.9,28
Though the literature is controversial, endometrial ablation is thought to have a reduced efficacy in women with adenomyosis as deeper endometrial glands can persist and proliferate. 27 Our results indicate that 29.9% of physicians would still perform an endometrial ablation for the treatment of adenomyosis, though 39.6% of physicians would not. Although the evidence is supportive of surgical excision for focal adenomyosis, especially in women desiring fertility, most respondents (42.5%) would not perform an excision of adenomyosis. 27 Those who were MIGS trained were more likely to offer adenomyomectomy, which likely reflects the surgical complexity of the procedure and the need for specialized training.
Limitations of this study include sampling and response bias. By sampling from three academic sites within two provinces, the broader spectrum of Canadian practice may not have been captured. In addition, gynaecologists with more familiarity with adenomyosis may have disproportionately participated, contributing to response bias.
Conclusion
Given the significant impact of adenomyosis on a woman’s life and imaging advancements leading to earlier diagnosis of this condition, appropriate diagnosis and conservative management of this condition during a woman’s reproductive lifetime is becoming more necessary for adequate patient care. Data supports the benefit of making the diagnosis of adenomyosis, and directing treatment specifically at this condition, rather than at the broader symptoms of HMB and pelvic pain. Further, standardization of TVUS diagnostic and reporting criteria would aid in improving both clinical and research diagnosis. This study highlights the current variation in practice amongst Canadian OBGYNs. There is a need for more research on directed conservative therapies for women with adenomyosis as there are therapies in use that may be beneficial but are not represented in the current literature. Lastly, given the practice variation across Canada, this study highlights the need for a specific national guideline to direct the diagnosis and management of adenomyosis.
Supplemental Material
sj-pdf-1-pev-10.1177_22840265221093263 – Supplemental material for Current diagnosis and management of adenomyosis in Canada: A survey of Canadian gynaecologists
Supplemental material, sj-pdf-1-pev-10.1177_22840265221093263 for Current diagnosis and management of adenomyosis in Canada: A survey of Canadian gynaecologists by Madalina Maxim, Ebernella Shirin Dason, Crystal Chan, Lea Luketic, Qixuan Li, Ella Huszti, Ari P. Sanders and Mara Sobel in Journal of Endometriosis and Pelvic Pain Disorders
Supplemental Material
sj-pdf-2-pev-10.1177_22840265221093263 – Supplemental material for Current diagnosis and management of adenomyosis in Canada: A survey of Canadian gynaecologists
Supplemental material, sj-pdf-2-pev-10.1177_22840265221093263 for Current diagnosis and management of adenomyosis in Canada: A survey of Canadian gynaecologists by Madalina Maxim, Ebernella Shirin Dason, Crystal Chan, Lea Luketic, Qixuan Li, Ella Huszti, Ari P. Sanders and Mara Sobel in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Author contributions
ED, CC, and MS researched literature and conceived the study. ED was involved in protocol development and gaining ethical approval. All authors were involved in subject recruitment. MM and ED were involved in data analysis and writing the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board (IRB) on November 8 2018. Approval number/ID: 18-0246-E.
Informed consent to participate
Written informed consent was obtained from all subjects before the study.
Informed consent to publish
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.