
Abstract
In the early days, all mucosal invasions of abdominal organs were considered to be one pathological condition of uncertain origin, termed adenomyoma. It was only in the 1920s that endometriosis and adenomyosis were clearly separated and it took approximately 80 years to put forward a new theory reunifying their pathogenesis. Today, identification of adenomyosis is carried out exclusively through vaginal ultrasonography and MRI. These techniques have made a careful evaluation of a distinct anatomical structure and the inner myometrial layers underlying the endometrium, termed the junctional zone, possible. Adenomyosis is characterized by a homogeneous thickening of this portion of the myometrium. When this hyperplasia is associated to an alteration of spiral arterioles' angiogenesis, then both adenomyosis and endometriosis may develop. Evidence is being accumulated that pre-eclampsia, fetal growth restriction and premature delivery may be linked, together representing a new, major obstetrical syndrome characterized by a modified uterine environment around the time of nidation. A dozen different medical or surgical techniques are utilized for the treatment of adenomyosis and novel approaches are being tested. These include use of inhibitors of angiogenesis that have been shown to cause reduced neo-angiogenesis, a significant modification of gene expression and a decrease in the percentage of active lesions. Encouraging results have also been obtained with the levonorgestrel-releasing intrauterine system.
Pathologists identified the presence of glandular structures within the context of uterine leiomyomata almost 150 years ago. However, for decades the vast majority refused to acknowledge that these glandular entities were of endometrial origin and described them as originating from a number of structures including mesonephros, parts of the Wolffian system (medullary cord or duct), embryonic germs or Müller's ducts [1]. In spite of great uncertainty regarding their origin, all mucosal invasions were considered as one entity (irrespective of whether they were described in a way that would identify them today as endometriosis or adenomyosis; this pathological entity was termed adenomyoma). Therefore, the early history of adenomyosis is interwoven with the early history of endometriosis, and it was not until the mid-1920s that the two were finally distinguished from one another [2]. It must be mentioned that there was a notable exception to the general belief: as early as the first decade of the 20th Century, Thomas S Cullen, often derided by the best pathologists of the time, had the intuition that the ‘epithelial invasion’ observed throughout the reproductive tract were endometrial in nature [3,4].
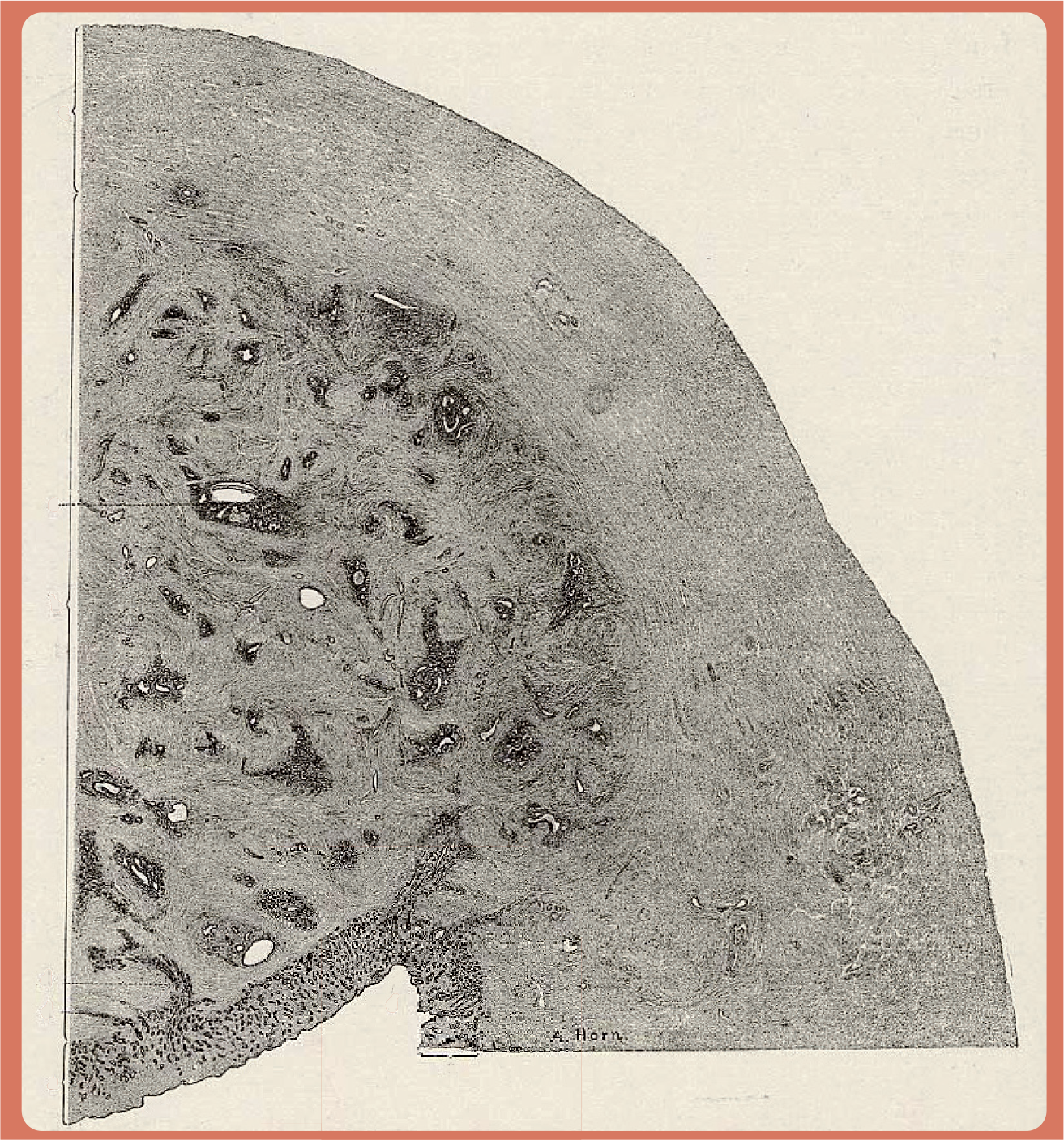
Surgical specimen showing the presence throughout the myometrium of endometrial glands.

Surgical specimen showing a more limited infiltration of endometrial glands into the myometrium.
Despite this, it was not until 1972 when Bird finally provided a definition that remains valid to this day [5]: “adenomyosis may be defined as the benign invasion of endometrium into the myometrium, producing a diffusely enlarged uterus, which microscopically exhibits ectopic, non-neoplastic, endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium” (

Microphotograph of a surgical specimen showing invagination of endometrium basalis into the junctional zone myometrium and deep location of endometrial glands and stroma surrounded by hypertrophic myometrium.
It is almost paradoxical that it took until the beginning of the 21st Century to put forward a new theory re-unifying the pathogenesis of the two conditions. Indeed, following Cullen's intuition [3,4] and Sampson's contribution to the understanding of extrauterine invasions, which he termed ‘endometriosi’ [7,8], a relentless search was initiated to gather evidence in support of the ‘retrograde menstruation theory’. This hypothesis totally separated endometriosis from adenomyosis, and throughout the 20th Century efforts focused on the characterization of ectopic implants [9].
Only in recent years, with the introduction of new imaging techniques and molecular diagnostic tools, has it become clear that adenomyosis and endometriosis may represent different phenotypes of a more profound disorder characterized by impaired cellular responses to ovarian sex steroids throughout the reproductive tract. Although advances in our understanding of the cross-talk between steroid hormone receptors and cell surface signaling pathways are of particular relevance to the pathogenesis of endometriosis, the search for a molecular definition of this syndrome has barely started [2]. Another breakthrough in our understanding of these benign endometrial invasions took place when epidemiological evidence from a recent retrospective study suggested that women with endometriosis carried a decreased risk of pre-eclampsia [10]. For decades it has been known that pre-eclampsia is characterized by defective deep placentation [11] and this new finding has raised the question of whether adenomyosis and endometriosis may be linked to modifications of the angiogenic process leading to deep hemochorial placentation in the human.
MRI played a vital role in developing the new unified theory because it provided a unique tool to identify a new pathophysiological entity, not yet evidenced in morphological studies of the uterus: the endomyometrial junctional zone (JZ).
Today, this new knowledge is generating new theories and, hopefully, will soon result in new therapeutic options. For this reason it is useful to summarize new findings and new hypotheses that are the basis of any new treatment strategy.
Incidence of adenomyosis & endometriosis
The incidence of endometriosis is estimated to be between 6 and 10% of all women, and 35 and 50% of women with pelvic pain and infertility [12]. On the other hand, the incidence of adenomyosis is under discussion since different imaging criteria are used. Kunz et al., found a prevalence of adenomyosis in 70% of women with endometriosis, compared with 9% in healthy controls [13]. This is in contrasts to a previous study by Bazot et al., in which only 27% of women with pelvic endometriosis had adenomyosis on preoperative MRI [14]. Using this technique, De Souza et al. detected discrete and diffuse patterns of adenomyosis in 54% of young women with infertility and dysmenorrhoea or menorrhagia [15].
Clinical diagnosis
Cullen provided a detailed clinical picture of adenomyomas, identifying two main symptoms: lengthened menstrual periods, which, as the disease progresses, may be replaced by a continuous hemorrhagic discharge; and a great deal of pain [4]. Contrary to Cullen's assertion, today a clinical diagnosis of adenomyosis is considered almost impossible. Studying all cases admitted during 1 year for hysterectomy for any indication, Cocuzzi et al. found, over a total of 528 cases, an incidence of histologically certified adenomyosis of 11.2% [
It is fair to say that Cullen admitted difficulties in arriving at a preoperative diagnosis. He wrote, “in the early years of our investigations we also failed to detect it clinically, but in the early and fairly advanced stages of the process so definite are the symptoms that the hospital assistant now frequently comes and says that a given case has all the signs of an adenomyoma and that he feels sure that this is the cause of the bleeding” [3].
Although aspecific, pelvic pain is an important symptom in many affected women; its pathogenesis is similar to that observed in deep nodular endometriosis. It is the presence of small hemorrhages as manifested by MRI that may cause pain [16].
In a recently published study of a subset of the American ‘Study of Women's Health Across the Nation’, investigators tried to identify, in hysterectomized women undergoing the menopausal transition, possible symptoms specific for adenomyosis [17]. Adenomyosis was found in 48% of 137 patients and, in these women, frequency of symptoms was similar in those with and without evidence of adenomyosis. The same prevalence of fibroids was observed in the presence or absence of adenomyosis (37 vs 43%); endometriosis (3 vs 5%); abnormal bleeding (27 vs 33%) or chronic pelvic pain in the presence of fibroids (12 vs 17%). They concluded that adenomyosis is an incidental finding, and not the source of the symptomatology.
Therefore, the hypothesis is advanced that adenomyosis, similarly to endometriosis, is an ovarian steroid hormone-dependent process; it remains basically physiological unless recurrent bleeding in the ectopic implants causes progressive disease and symptoms. Diagnosis should take into account the detection of chronic bleeding, and efficient medical treatment can be achieved by amenorrhea without the induction of hypoestrogenism [16].
In the past, a diagnosis of adenomyosis was occasionally made using hysterosalpingography and hysteroscopy; it is today widely accepted that the only two practical ways to reach a valid diagnosis are transvaginal sonography (TVS) and MRI.

35-year-old woman with diffuse thickening of the myometrium junctional zone. Measuring more than 12 mm in thickness, indicating the presence of adenomyosis (sagittal T2-weighted image).

A 35-year-old woman with focal thickening of the posterior wall of the myometrium junctional zone.
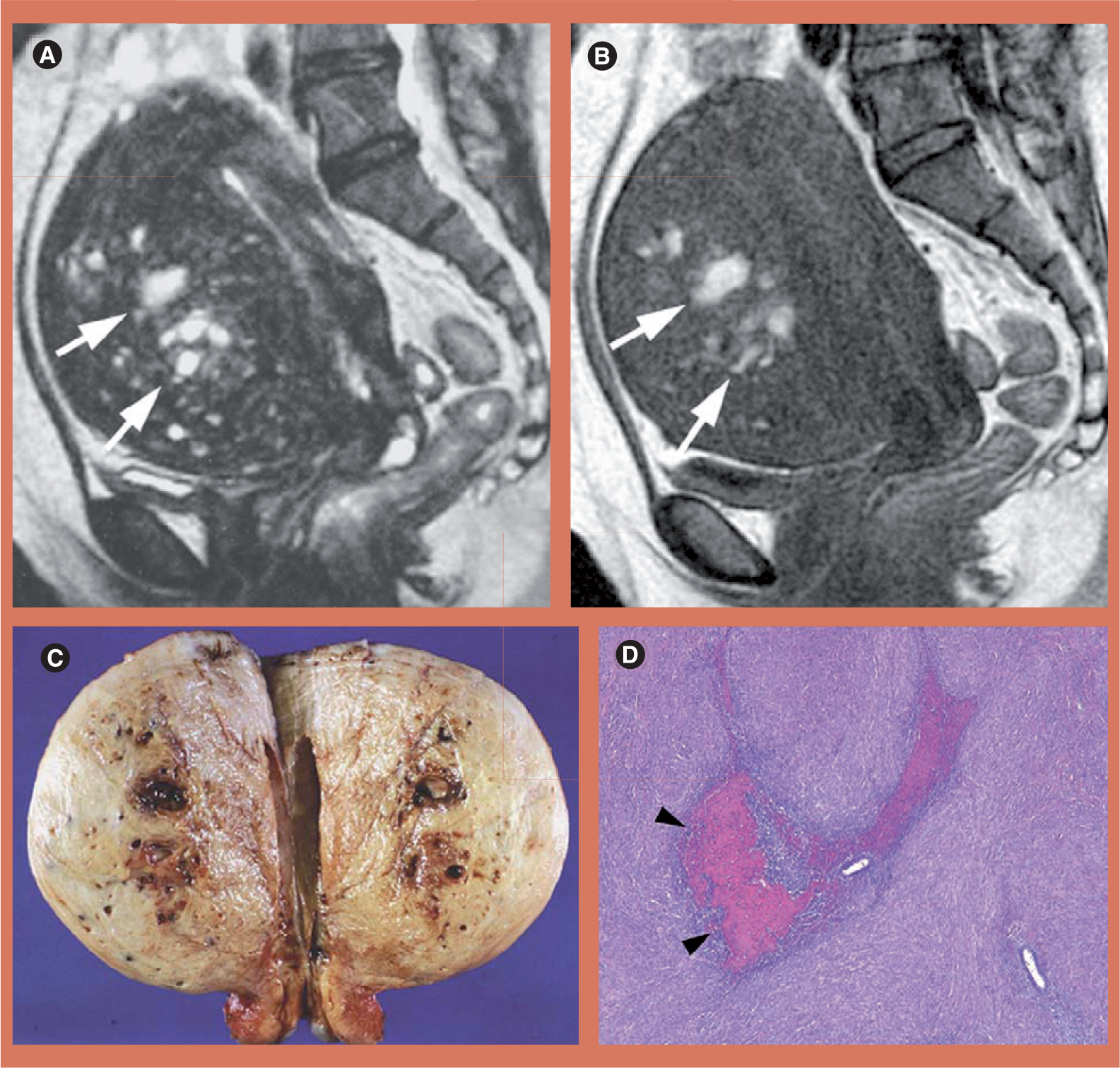
A 52-year-old woman with hemorrhagic foci of adenomyosis.
Endomyometrial junctional zone
Modern imaging techniques, both TVS and MRI, have also made possible for the first time a careful evaluation of the inner myometrial layers underlying the endometrium; these have been termed the JZ and appear to be a distinct anatomical structure, despite the lack of histological distinction on light optic microscopy. This portion of the myometrium presents a number of specific characteristics, such as the endometrium is of Müllerian origin, while the outer myometrium is of non-Müllerian, mesenchymal derivation; it has structural and functional differences with the outer myometrium and functional similarities with the endometrium [18].
The normal appearance of the JZ has been described on TVS or MRI using different terminology, but always as a regular inner layer of the myometrium, measuring 5 mm or less in thickness [19,20]. It is still unclear whether the JZ undergoes cyclical changes in thickness, mimicking those of the endometrium; whereas some time ago Wiczyk et al. described changes with a maximum growth between days 8 and 16 of the cycle [21], more recently, Hauth et al. could not identify significant differences in thickness between the follicular and luteal phase [20]. Another important feature of the JZ is that its thickness (similar to that of the endometrium but not that of the outer myometrium) increases with age between 20 and 50 years [20].
Substantive data demonstrate functional dissimilarities between the myometrium JZ and the outer myometrium. In postmenopausal women, both in those with and without adenomyosis and in those taking oral contraceptives or gonadotropin-releasing hormone analogues, suppression of ovarian activity decreases the zone's thickness. In contradistinction to this, hormone-replacement therapy may cause the reappearance of the typical anatomy of the JZ [22]. In normally menstruating women, uterine peristaltic activity, measured by variations in myometrial contractility waves, indicates that it originates exclusively from the JZ, while the outer myometrium remains quiescent [23,24]; in addition, uterine peristalsis is primarily hormone dependent (it is dependent on both estrogen and progesterone [25]) and its activity is likely to play a role in sperm transport, as well as in the nidation process.
In conclusion, although further validation is required, there seems to be sufficient evidence that the ‘zonal–endometrial’ complex plays an important role in uterine receptivity and the nidation and placentation processes, to the point that studying the relative signal intensity of uterine layers is a good predictor of the outcome of assisted conception [26].
Adenomyosis & the junctional zone
The thickness of the JZ of the myometrium physiologically increases with age; in normal women it grows from 0.5 to 0.8 cm, whereas in those with adenomyosis or fibroids it grows from 0.5 to 1.1 cm [20]. Thus, it is obvious that widening of the JZ is not primarily caused by adenomyosis per se, but rather by physiological hyperplasia.
When studying the myometrium JZ in women with adenomyosis, several important facts have been discovered. First, adenomyosis typically presents as either diffuse or focal thickening of the inner myometrium or an ill-defined myometrial nodule of low-signal intensity on T2-weighted MRI scans [27]; second, it is characterized by a homogeneous thickening of the myometrium JZ and this feature has become the standard parameter for the diagnosis of even mild forms of the condition. While a normal JZ is described as having a thickness (on T2-weighted MRI scans) of between 5 and 12 mm, the presence of a JZ measuring more than 12 mm in thickness, with hemorrhagic high-signal myometrial spots, is highly predictive of histological adenomyosis (defined as the presence of glandular and stromal extension of more than 2.5 mm below the endomyometrial junction on low-power field) [28].
This thickening of the myometrium JZ observed in MRI is thought to be the consequence of inordinate inner myocyte proliferation and/or angiogenesis, and the suggestion has been made that the disruption of JZ architecture precedes and predisposes for the subsequent development of adenomyosis [24]. This assumption is supported by the observation that, while adenomyosis is regarded as a condition typical of older, multiparous women, irregular JZ thickening is not an uncommon finding in young, symptomatic women [29].
Adenomyosis may present itself with varying degrees of severity, ranging from simple JZ thickening to more diffuse and nodular lesions involving the entire uterine wall. Finally, it can take the form of an adenomyoma, a focal thickening or a nodular structure at the junctional zone or within the myometrium, with low-signal intensity on T2-weighted MRI scans.
Adenomyosis & endometriosis
The relationship between these two endometrial disorders seems to have gone in a full circle; at the beginning of the 20th Century only one pathological definition (adenomyoma) was utilized to describe the presence of heterotopic epithelial cells, stroma and glands. To use the words of Kelly and Cullen: “In cases of adenomyoma of the uterus, we usually find a diffuse myomatous thickening of the uterine muscle. This thickening may be confined to the inner layers of the anterior, posterior or lateral walls, but in other cases the myomatous tissue completely encircles the uterine cavity. This diffuse myomatous tissue contains large or small chinks, and into these the normal uterine mucosa flows. If the chinks are small, there is only room for isolated glands, but where the spaces are goodly in size, large masses of mucosa flow into and fill them. We accordingly have a diffuse myomatous growth with normal mucosa flowing in all directions through it. The mucosa lining the uterine cavity is perfectly normal” [30].
Then came Sampson [7,8], and endometriosis was born. From there on, the two entities remained distinct, although a link persisted since, at times, one was termed endometriosis interna and the other endometriosis externa. Then, with the identification and characterization of the myometrium JZ, connections between them began to reappear. In 1995, a study by Salamanca and Beltran investigating inner myometrial contractility in women with endometriosis found a predominantly retrograde pattern of subendometrial contractions during menstruation [31]. After this, Kunz et al., using MRI, established a significant correlation between increased JZ thickness and peritoneal endometriosis [13]. As previously mentioned, they calculated a prevalence of diffuse and focal adenomyosis in 79% of all patients with endometriosis; this reached 90% in women younger than 36 years, a prevalence of 28% in their total control group (women without endometriosis) and only 9% in their healthy control group.
These data support the hypothesis that JZ hyperplasia precedes adenomyosis and endometriosis [32]. However, this did not explain why JZ hyperplasia may develop in some women at a young age. Recently, a new link seems to have been found in a common predisposing factor: an alteration of spiral arteriole' angiogenesis.
Angiogenesis, adenomyosis & endometriosis
Menstrual cycles produce waves of active angiogenesis within the endometrium, with development of arterioles and a capillary network. Kohnen et al. found that this involves a spatially regulated process of vascular smooth cell differentiation, which is under the influence of a number of factors [33]. Very recently, Goteri et al. demonstrated that, in women with adenomyosis, VEGF (a major mediator of angiogenesis and vascular permeability), hypoxia-inducible factor (HIF)-1α expression and microvessel density were increased, particularly in epithelial cells, when comparing heterotopic versus normotopic endometrium in the same woman [34]. Kang et al. have now suggested that VEGF may play a key role in the development of adenomyosis; investigating four VEGF polymorphic alleles this group found significant differences between adenomyosis patients and a control group in the allele frequencies and genotype distributions [35]. They concluded that two alleles of the VEGF gene (22578A and 21154A) could significantly decrease the risk of adenomyosis and might potentially be protective factors for adenomyosis development.
Further evidence linking adenomyosis to abnormal angiogenesis comes from a study by Tokyol et al. who investigated the expression of COX-2 and matrix metalloproteinase (MMP)-2 in patients with this condition [36]. They observed that, while the quantity and intensity of COX-2 expression in endometrium did not vary during the menstrual cycle in normal women, in patients with adenomyosis it was higher both during the follicular and secretory phases.
The eutopic endometrium in patients with endometriosis is abnormal [37–39] and evidence is beginning to emerge that pre-eclampsia, fetal growth restriction and premature delivery are linked and that together, they may represent a major obstetrical syndrome characterized by a modified uterine environment near the time of nidation [10,40].
Therefore, zone hyperplasia, adenomyosis and endometriosis may be related to an aberrant angiogenesis in the myometrial JZ. In this respect, histological examination shows that the subendometrial halo, as observed by TVS, is a distinct compartment of the myometrium comprising tightly packed muscle cells with increased vascularity [41].
Under the circumstances, a hypothesis can be formulated that ovulatory menstrual cycles during early reproductive life have an angiogenic priming effect that will permit successful deep placentation, but under certain circumstances can also lead to uterine disorders.
Menstruation preconditioning hypothesis
While the debate over menstruation is certainly not over, there are scientists who view it as serving no purpose other than to reinitiate the endometrial cycle in the absence of pregnancy. However, menstruation and pregnancy are both inflammatory conditions that cause a degree of physiological ischemia/reperfusion tissue injury, albeit much more so in pregnancy. It can be speculated that menstruation may not have been an evolutionary coincidence, but serves to protect uterine tissues from the profound hyperinflammation and oxidative stress associated with deep placentation. This process of preconditioning provides a novel paradigm for understanding how reproductive disorders impact on pregnancy outcome, while, on the other hand, in the absence of pregnancy they may cause uterine reproductive disorders [42].
In the light of newly acquired knowledge, the question then arises as to whether spontaneous ovulatory menstrual cycles have a functional role in priming the uterine vascular microenvironment to secure the rapid spiral artery remodeling and deep placentation before a first pregnancy. With regard to this, it has been well documented that the risk of pre-eclampsia is reduced for second and later pregnancies; this protective effect is achieved even if pregnancy is terminated during the first trimester. A large epidemiological study recently confirmed this fact: the protective effect of two induced abortions is similar to that commonly observed after a first term pregnancy [43]. As previously mentioned, there seems to be a common predisposing factor linking, adenomyosis, endometriosis and pregnancy complications: the preconditioning of the uterus for successful deep placentation.
Cyclic endometrial decidualization and the subsequent menstrual shedding are therefore examples of the physiological preconditioning necessary to prepare the uterus for a dramatic vascular remodeling, reactive oxygen species production and the hyperinflammation associated with deep hemochorial placentation. Indeed, decidualization in the human offers a unique example of rapid angiogenesis starting in the midluteal phase. Remodeling of myometrial JZ spiral arteries is a complex process and has been reviewed recently by Brosens et al. [44], both in the event of normal and abnormal gestations. They reported that decidualized cells are a major source of angiogenic growth factors whose levels decrease with increasing gestational age, suggesting that decidual angiogenesis may play a role in the initial spiral artery remodeling. Decidual uterine natural killer cells are potent secretors of an array of angiogenic factors and regulate trophoblast invasion both in vitro and in vivo by production of the IL-8 and interferon-inducible protein-10 chemokines [45].
In addition, using MRI, the myometrium JZ was found to be significantly thicker on T2-weighted imaging in patients with endometriosis when compared with age-matched control subjects [29]; however, Power Doppler ultrasound studies have demonstrated that endometriosis is associated with increased endometrial and JZ blood flow during the late secretory phase of the cycle [46]. The most compelling evidence for cyclic endometrial preconditioning comes from the observation that stromal purified cells from eutopic endometrial biopsy material from patients with and without endometriosis exhibit different responses to a decidualizing stimulus, even after prolonged culture [47,48].
These findings have immediate practical applications: they raise the real possibility of identifying, prior to conception, not only women at risk of adverse pregnancy outcome, but also those at risk for disorders such as endometriosis and adenomyosis. This could be achieved by uterine perfusion studies, epigenetic analysis or endometrial gene expression profiling during the late secretory phase of the menstrual cycle [43,49].
Adenomyosis & fertility
Whilst adenomyosis is increasingly diagnosed in women with endometriosis, the precise role of adenomyosis in infertility remains controversial and whether adenomyosis per se causes infertility is unknown.
The first experimental evidence that adenomyosis may cause infertility comes from Barrier et al. [50]. In 2004, they published a case–control study in a population of captive baboons and found that adenomyosis was associated with the presence of lifelong infertility (odds ratio: 20.6). Their conclusion was that the condition is strongly associated with primary infertility in baboons, even in the absence of coexisting endometriosis.
In the same year, Zangos et al. assessed uterine morphology and function in some 40 women with symptomatic endometriosis [51]. Adenomyosis was diagnosed on T2-weighted MRI scans in 85.4% of these women; patients showing signs of adenomyosis tended to show a longer history of symptomatic endometriosis. Finally, these women showed a reduced uterotubal transport capacity proportional to the severity of adenomyotic changes, indicating a possible link with infertility.
The current consensus is that, for successful conception, JZ contractions at the time of implantation should be minimal. Excessive JZ contractions have been shown to reduce implantation rates in both spontaneous and stimulated cycles [52–54]. A low frequency contraction of the JZ before embryo transfer (ET) during IVF cycles is associated with a higher implantation rate and a higher clinical and ongoing pregnancy rate [55], while a significantly lower clinical pregnancy rate occurs if five or more contractions per minute are observed immediately after ET [56,57].
Therefore, the question arises as to whether abnormal contractility is associated with reduced fertility. Women with endometriosis demonstrated a significant increase in JZ contractions and a disruption in the pattern of contractility in comparison with healthy controls [54,58]. Leyendecker's group [59] demonstrated that in women with endometriosis, the mechanism of rapid sperm transport is compromised. The evidence for disrupted sperm transport in women with endometriosis and/or adenomyosis is quite convincing, but probably of greater importance is the increased contractility or hyperperistalsis [59,60].
Stem cells & the junctional zone
The uterus has a remarkable capacity for vascular regeneration, not only after each menstrual cycle, but also, and to a greater extent, after delivery. The fact that JZ spiral arteries are capable of complete involution in the puerperium and that those with atherosclerotic lesions return to normal, has important implications in the field of vascular pathology.
Recent studies have provided evidence for the existence of human endometrial stem/progenitor cells. Chan et al. demonstrated clonogenicity of endometrial-derived cells by generating single-cell suspensions of epithelial and stromal cells from hysterectomy samples [61]. In addition, Schwab et al. demonstrated that the frequency of clonogenic epithelial and stromal cells did not differ between phases of the menstrual cycle; also, there was no significant change in the number of clonogenic cells isolated from inactive endometrium [62]. Since inactive endometrium contains only a basal layer, while the functional layer is absent, these data suggest that putative endometrial stem/progenitor cells reside along the endometrial–myometrial border [63].
Obviously, these preliminary findings open up new research avenues and, in light of this, Sasson and Taylor [64] have posed a series of questions awaiting a response:
Which cell lineages – epithelial, stromal or myometrial – are generated by endometrial stem cells?
What is the physiological role of endometrial stem cells and what are their niches in pathologic processes?
Do endometriotic implant locations differ in their proclivity to originate from bone marrow-derived stem cells versus uterine-derived stem cells?
Does retrograde menstruation of endometrial stem cells seed the pelvis, whereas hematologic dissemination can seed both the pelvis and distant sites that are not directly accessible to menstrual flow?
Does the primary defect in the endometriosis pathway lie in the stem cell, or does disregulation within the niche permit aberrant biological processes to function in the stem cell?
Does ectopic stem cell differentiation have a function in the pathogenesis of other gynecological diseases, such as adenomyosis, chronic pelvic pain and gynecological cancers?
Treatment of adenomyosis
In a recent review, Yang et al. list 12 different medical or surgical techniques for the treatment of adenomyosis; by and large these modalities are identical to those utilized in cases of endometriosis [65].
It is beyond the scope of this review to discuss classic treatments of adenomyosis; however, the few novel approaches to the treatment, medical or surgical, of this condition will be summarized below.
Surgical approaches
In a recent paper, Rabinovici and Stewart reviewed new interventional techniques that have been introduced over the last few years in order to find an adequate noninvasive therapy for adenomyosis [66]. They warn that there are no evidence-based data to guide us in using minimally invasive therapy, since most data regarding these evolving therapies come from the inadvertent treatment of adenomyosis in studies designed to treat uterine leiomyomata. For this reason, all data are from case reports or small case series. An additional problem is represented by the lack of an agreed imaging definition of adenomyosis, and so therapies that do not excise the uterus have no ‘gold standard’ for comparison.
Nonetheless, some reports suggest that there may be efficacy in techniques such as uterine artery embolization and MRI-guided focused ultrasound surgery (MRIgFUS).
Uterine artery embolization
In 2001, Siskin et al. retrospectively evaluated the MRI appearance and clinical response of patients undergoing uterine artery embolization (UAE) for the treatment of menorrhagia due to adenomyosis [67]. Of the 15 patients in the study, five had diffuse adenomyosis without evidence of uterine fibroids, one had focal adenomyosis without evidence of uterine fibroids and the remaining nine had adenomyosis with one or more fibroids. At 12 months follow-up, 92.3% patients reported significant improvement in symptomatology and quality of life. Postoperative MRI revealed significant reductions in median uterine and fibroid volume and mean JZ. Larger, prospective studies are needed to establish the safety and efficacy of this procedure in women with adenomyosis.
Several reports followed, mostly from the Far East, which confirmed that UAE is an effective therapy for adenomyosis.
Worth mentioning is a South Korean study that investigated UAE in women with adenomyosis, but no fibroids [68]. They observed significant improvements in dysmenorrhea and menorrhagia with a decrease in uterine size in most patients. In addition, MRI evaluation produced results suggestive of coagulation necrosis of adenomyosis in the majority of patients.
Another important study was conducted in South Korea to evaluate the return of fertility; unfortunately, of the initial series of 94 patients, only six desired to become pregnant; five of them succeeded with one case of premature rupture of the membrane [69].
Larger studies specifically applying surgical techniques to the conservative management of adenomyosis are needed, provided that adequate solutions are found for the diagnosis and improved technical parameters are determined.
MRI-guided focused ultrasound surgery
Recently, Fukunishi et al. evaluated the thermal ablative effects of MRIgFUS on adenomyosis in improving clinical parameters in 20 premenopausal women; since adenomyosis symptoms are similar to those of uterine myomata, they used the symptom severity score questionnaire available for evaluating the effect of MRIgFUS on myoma [70]. They reported that most adenomyotic lesions could be satisfactorily ablated close to the serosal surface or the endometrium and, at 6 months, the mean uterine volume had decreased by 12.7%. Symptom severity score improved significantly during the 6 months of follow-up and no serious complications were observed.
Therefore, it seems that MRIgFUS represents a new, safe and effective method for the ablation of adenomyotic tissue.
Medical approaches
As previously stated, a constant feature of medical therapy for adenomyosis is that, over the years, it has mimicked that which has been applied to endometriosis. At present, medical therapy of adenomyosis can be attempted for symptomatic relief, especially in premenopausal women and in women who wish to become pregnant.
Two novel approaches discussed below are either already available or will soon be ready for large-scale trials.
Inhibitors of angiogenesis
New knowledge of a modified angiogenesis in heterotopic uterine mucosa in case of endometriosis and adenomyosis is opening the way for a new treatment line. Starting from the observation that dopamine and its agonists, such as cabergoline (Cb2), promote endocytosis of VEGF receptor (VEGFR)-2 in endothelial cells, thereby preventing VEGF–VEGFR-2 binding and reducing neoangiogenesis, the group of Pellicer et al. has now evaluated in an animal model the antiangiogenic properties of Cb2 on the growth of established endometriosis lesions [71]. After treatment with Cb2, they found a significant decrease in the percentage of active endometriotic lesions and of cellular proliferation index, associated to a reduced neoangiogenesis, and a significant modification of gene expression.
In women with suspected (nonhistological) diagnosis of adenomyosis, after insertion of a levonorgestrel-releasing intrauterine system, VEGF expression is substantially reduced in eutopic endometrial glands and stroma; however, it is not known whether the same occurs in the heterotopic glands [72].
Another approach aimed at inhibiting angiogenesis has been studied by the group of Creatsas using pentoxiphylline, a phosphodiesterase inhibitor [73]. In an animal model, they evaluated changes in morphology and in the expression of VEGF-C and of the receptor for tyrosine kinase, Flk-1 (a VEGF receptor) and observed a significant reduction in the mean volume of the endometriotic implants per animal when compared with the control group. Their conclusion was that pentoxiphylline may cause suppression of endometriotic lesions by suppressing angiogenesis through VEGF-C and Flk-1 expression.
A preliminary clinical confirmation of the usefulness of pentoxiphilline in the treatment of endometriosis-associated infertility comes from Creus et al. [74]. In a prospective, randomized, controlled, blind trial, a group of patients was randomly assigned, immediately after laparoscopic surgery, to treatment with either oral pentoxiphylline (800 mg/day) or an oral placebo. These women were then observed for the occurrence of pregnancy for 6 months. In the approximate 100 patients who completed the study, the 6-month overall pregnancy rates were 28 and 14% in the pentoxiphylline and placebo groups, respectively (p = 0.1). These findings provide preliminary clinical evidence to suggest that new experimental treatment approaches toward endometriosis, that are based on immunomodulation deserve further attention. Well-designed multicenter trials are warranted to confirm or refute these results.
For completeness, it must be mentioned that almost 20 years ago, Steinleitner et al. used an animal model for endometriosis (the golden hamster) to determine the effect of pentoxiphylline on early reproductive performance [75]. At laparotomy, they subjected groups of animals to either excision of the right uterine horn, or excision of the right uterine horn with explantation of four 2-cm2 uterine fragments onto the left uterine mesentery. Surgically treated hamsters and nonsurgically treated controls were subjected to ovulation induction 6 weeks later; subsequently, the animals were divided into groups for periovulatory treatment with either pentoxiphylline (2.5 mg/kg) or placebo. Fertilization rates in surgical and nonsurgical control groups exceeded 90%. Fertilization was significantly impaired in saline-treated animals bearing uterine explants (mean of 2.3 ± 1.9%). Administration of pentoxiphylline dramatically reversed this effect (99.0 ± 0.7% mean fertilization rate). Thus, an important role for immunomodulators in eliminating the adverse influence of endometrial explants on fertilization was evidenced; Steinleitner even suggested that, “the periovulatory administration of nonteratogenic immunomodulatory agents may provide an alternative to conventional treatment for endometriosis.”
Levonorgestrel-releasing intrauterine system
In 1997, Fedele et al. utilized the levonorgestrel-releasing intrauterine system (LNG-IUS) for relief from adenomyosis-associated menorrhagia [76]. In 23 women with recurrent menorrhagia and adenomyosis diagnosed with TVS, the insertion of the system induced amenorrhea in two, oligomenorrhea in three, spotting in two and regular flows in the remaining 16 women after 1 year. Significant increases in hemoglobin, hematocrit and serum ferritin were also observed. This small trial documented that the LNG-IUS produces the same positive effects on excessive bleeding also when adenomyosis is present.
A single case was then published of a patient in whom a diagnosis of adenomyosis had been made, for whom conservative therapy initiated with mefenamic acid was unsatisfactory. The patient suffered from menorrhagia, dysmenorrhea and an enlarged uterus. A marked decrease in uterine size occurred within 12 months of insertion accompanied by resolution of the menorrhagia and dysmenorrhea. This is the first description of successful treatment of the full symptomatology of adenomyosis [77].
Very recently, a full-scale trial aimed at evaluating the efficacy of the LNG-IUS in the treatment of the full range of symptoms of adenomyosis, was conducted by Sheng et al. [78]. In 94 women with moderate or severe dysmenorrhea, as diagnosed by TVS, improvements were documented for dysmenorrhea (using a visual analog scale [VAS]), uterine volume and serum CA125 levels, over a period of 36 months. They observed a continuous and significant drop in VAS from the baseline score (p < 001). The uterine volume decreased significantly from 113.8 ± 46.9 ml to 87.7 ± 35.8 ml (p < 001) at 12 months and serum CA125 levels were significantly reduced from 6 months onwards (p < 001). Given these encouraging results, additional studies are now warranted.
According to Farquhar and Brosens, there are several mechanisms that could explain the role of the LNG-IUS in adenomyosis [79]. First of all, following insertion of the system there is a decidualization of the endometrium and this is followed by atrophic changes that produce a marked reduction in menstrual blood loss. Through absorption within the myometrium, the progestin also acts directly on the adenomyotic foci. In addition, downregulation of estrogen receptors, in both glandular and stromal endometrial layers, occurs shortly after placement of the device and persists for at least the first year of use. Adenomyotic deposits are then reduced in size, uterine contractility improves and the uterine size decreases. The LNG-IUS positive effect on dysmenorrhea is probably mediated through a reduction of prostaglandin production within the endometrium; reduction in the size and activity of adenomyotic tissue may also account for the improvement in dysmenorrhea.
Gonadotropin-releasing hormone analogues
In 2002, Imaoka et al. investigated a possible role of gonadotropin-releasing hormone analogues for the treatment of diffuse adenomyosis, as evidenced by MRI. They administered the analogue over a 6-month period to 31 patients with MRI features suggestive of diffuse adenomyosis and concluded that use of gonadotropin-releasing hormone analogues is associated with a decrease in myometrium JZ width. Furthermore, asymmetric adenomyosis with high-signal intensity foci appears to be the most sensitive to hormonal therapy [80].
Conclusion
No reliable clinical diagnosis of adenomyosis is feasible and, until recently, the condition could be identified only at inspection and examination of the surgical specimen. Today, modern imaging techniques, both TVS and MRI, have made possible for the first time a noninvasive identification of adenomyosis. The first new features identified through new imaging techniques are the inner myometrial layers underlying the endometrium, termed the JZ. These appear to be a distinct anatomical structure, despite the lack of histological distinction on light optic microscopy; in women with adenomyosis there is a homogeneous thickening of the myometrium JZ and this feature has become the standard parameter for the diagnosis of even mild forms of the condition.
Following the identification of the myometrium JZ, a close relationship between the two endometrial disorders, adenomyosis and endometriosis, has been re-established and today a new hypothesis links both endometriosis and adenomyosis to the same predisposing factor: an alteration of spiral arteriole' angiogenesis.
The hypothesis has been formulated that ovulatory menstrual cycles during early reproductive life have an angiogenic priming effect that will permit successful deep placentation, but also under certain circumstances can lead to uterine disorders.
The precise role of adenomyosis in infertility remains controversial, and whether adenomyosis per se causes infertility is unknown, although changes in inner myometrial contractility, as observed in the two endometrial disorders, are associated with reduced fertility.
Future perspective
Recently, new knowledge has been acquired that will influence therapeutic strategies. In particular, two novel techniques will improve medical treatment over the next few years and even produce a preventive strategy: the first are angiogenesis inhibitors and the second is the levonorgestrel-releasing intrauterine system, Mirena (Schering Pharma, Berlin, Germany).
A new development capable of revolutionizing therapy is the identification of endometrial stem cells. Several questions have arisen as a result: which cell lineages are generated by endometrial stem cells; what is their physiology and what are their niches in pathologic processes. Does retrograde menstruation of endometrial stem cells seed the pelvis, whereas hematologic dissemination seeds both the pelvis and distant sites; and does the primary defect in the endometriosis pathway lie in the stem cell, or does disregulation within the niche permit aberrant biological processes to function in the stem cell?
Executive summary
Prevalence of adenomyosis is under discussion since different imaging criteria are used.
In different studies, the prevalence varies between 27 and 70% in women with endometriosis and has been estimated at 54% in young women with infertility, dysmenorrhea or menorrhagia, and 9% in healthy controls.
Today, a clinical diagnosis of adenomyosis is considered almost impossible.
Although aspecific, pelvic pain is an important symptom in many affected women.
In candidates for hysterectomy, the presence of adenomyosis does not modify the incidence of fibroids, endometriosis, abnormal bleeding or chronic pelvic pain.
Inner myometrial layers underlying the endometrium have been carefully evaluated, thanks to modern imaging techniques, both transvaginal sonography and MRI.
Named the junctional zone (JZ), inner myometrial layers appear to be a distinct anatomical structure, despite the lack of histological distinction on light optic microscopy.
This portion of the myometrium demonstrates functional similarities with the endometrium.
Its thickness (similar to that of the endometrium, but not that of the outer myometrium), increases with age between 20 and 50 years.
In women taking oral contraceptives or gonadotropin-releasing hormone analogues and in postmenopausal women, suppression of ovarian activity decreases the thickness of the JZ.
In normally menstruating women, uterine peristaltic activity originates exclusively from the JZ, while the outer myometrium remains quiescent.
On MRI scans, adenomyosis is accompanied by either diffuse or focal thickening of the inner myometrium, or an ill-defined myometrial nodule of low-signal intensity.
It is characterized by a homogeneous thickening of the myometrium JZ and this feature has become the standard parameter for the diagnosis of even mild forms of the condition.
Thickening of the myometrium JZ observed in MRI scans is thought to be the consequence of inordinate inner myocyte proliferation and/or angiogenesis.
It seems that disruption of JZ architecture precedes and predisposes for the subsequent development of adenomyosis.
Relationship between adenomyosis and endometriosis seems to have gone full circle: in the early days, only one pathological definition (adenomyoma) was utilized to describe both
Following the identification of endometrial foci in the peritoneal cavity and ovaries, the two entities remained separated.
With the identification and characterization of the JZ of the myometrium, connections between them began to reappear and a high prevalence of diffuse and focal adenomyosis was found in patients with endometriosis.
It seems that JZ hyperplasia precedes adenomyosis and endometriosis and that both have a common predisposing factor: an alteration of spiral arteriole' angiogenesis.
Menstrual cycles produce waves of active angiogenesis within the endometrium, with development of arterioles and a capillary network.
In women with adenomyosis, VEGF, hypoxia-inducible factor-1α expression and microvessel density are increased, particularly in epithelial cells, when comparing heterotopic versus normotopic endometrium in the same woman.
Eutopic endometrium in patients with endometriosis is abnormal and evidence is beginning to emerge that pre-eclampsia, fetal growth restriction and premature delivery are linked and they may also be related to the two menstrual disorders.
Menstruation and pregnancy are both inflammatory conditions that cause a degree of physiological ischemia/reperfusion tissue injury.
Spontaneous ovulatory menstrual cycles seem to have a functional role in priming the uterine vascular microenvironment to secure the rapid spiral artery remodeling and deep placentation before a first pregnancy.
Preconditioning the uterus for successful deep placentation, may represent the common predisposing factor linking, adenomyosis, endometriosis and pregnancy complications.
Decidualized cells are a major source of angiogenic growth factors and decidual angiogenesis may play a role in the initial spiral artery remodeling.
Endometriosis (and possibly adenomyosis) is associated with increased endometrial and JZ blood flow during the late secretory phase of the cycle.
Adenomyosis is increasingly diagnosed in women with endometriosis, but the precise role of adenomyosis per se in infertility remains controversial.
Adenomyosis is strongly associated with primary infertility in baboons, even in the absence of coexisting endometriosis.
Excessive JZ contractions have been shown to reduce implantation rates in both spontaneous and stimulated cycles and this phenomenon is present in patients with adenomyosis.
Sperm transport in women with endometriosis and/or adenomyosis is also disrupted.
There is increasing evidence of the existence of human endometrial stem/progenitor cells.
Endometrial-derived cells in single-cell suspensions of epithelial and stromal cells from hysterectomy samples show clonogenicity.
It is not known which cell lineages are generated by endometrial stem cells, or what is their physiological or pathological role.
New knowledge on the genesis of adenomyosis is generating new treatment strategies.
On the surgical front, uterine artery embolization and focused ultrasound surgery seem promising even in women desiring pregnancy.
Several innovative medical approaches are also being attempted: use of angiogenesis inhibitors and of the levonorgestrel-releasing intrauterine system and treatment with gonadotropin-releasing hormone analogues.
Footnotes
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.