
Abstract
Systemic therapy improves disease-free survival in patients with breast cancer, but does not cure patients with advanced or metastatic disease, and fails to benefit the majority of patients with localized breast cancer. Intrinsic resistance to chemotherapy is emerging as a significant cause of treatment failure and evolving research has identified several potential causes of resistance, such as drug efflux pumps, disregulation of apoptosis and cancer stem cells. Building upon preclinical models, drugs designed to reverse resistance to therapy are currently under investigation in clinical trials for the treatment of breast cancer.
Keywords
Although progress has been made in the treatment of breast cancer [1], it is clear that systemic therapies, such as chemotherapy, benefit a minority of patients with localized breast cancer and, with few exceptions, fail to cure patients with metastatic disease. This is largely due to the cancer cell resistance to therapy. The role of intrinsic versus acquired resistance to systemic therapy still remains largely unanswered. In fact, there is ever growing controversy over how to define intrinsic and acquired resistance. This is largely owing to the use of clinical doctrine to define subtypes of resistance. As such, intrinsic resistance was defined as a lack of tumor response to initial therapy and acquired resistance as tumors that initially responded to treatment and later relapsed. During early clinical observations, relapse was attributed to acquired mutations, possibly caused by treatment itself. Later, work that built upon the clonal selection of drug-resistant bacteria, demonstrated the same clonal selection process for cancer cells [2]. Although this continued to be described as ‘acquired resistance’, it was clear that a subpopulation of cancer cells were intrinsically resistant to therapy and could account for tumor recurrence even in patients whose tumors initially responded to therapy

Three models of chemotherapy resistance.
With time, the list of therapeutic agents effective in the treatment of breast cancer has grown
Overview of therapy for localized & advanced breast cancer
Treatment of breast cancer depends upon disease stage (i.e., the presence and size of invasive component, local nodal involvement and the presence or absence of distant metastasis) and pathologic features of the primary tumor, such as receptor status and tumor grade. Patients who have no clinical evidence of distant metastasis by physical exam or radiologic imaging are said to have localized disease; however, if left untreated with systemic therapy, a proportion of these patients will relapse after surgical resection of their tumor. The proportion of cancers that relapse usually do so owing to small deposits of metastatic cancer cells that are too small to be detected with conventional imaging techniques. In patients with localized breast cancer, the chance of developing disease recurrence or relapse is heavily dependent upon the number of axillary lymph nodes involved, the size of the primary tumor and pathologic features of the primary tumor. Although a weak prognostic predictor for recurrence, receptor status is important for the prediction of response in systemic therapy and estrogen receptor (ER), progesterone receptor (PR) and the human EGF receptor (HER)2 should be measured in all patients with invasive disease. Patients with early-stage localized breast cancer are usually recommended to undergo surgical resection of the primary tumor (i.e., mastectomy or breast conserving surgery) and evaluation of the ipsilateral axillary nodal basin (i.e., sentinel lymph node biopsy and/or complete axillary node dissection). After definitive surgery, patients may receive radiation therapy to the remaining breast tissue/chest wall and draining lymph nodes in order to reduce the risk of local recurrence. Systemic adjuvant therapy given after surgical resection of the primary tumor and lymph node metastasis has been demonstrated to reduce the risk of breast cancer recurrence by 30–50% and is recommended for patients with a significant risk of disseminated disease based upon unfavorable characteristics of the primary tumor, such as the presence of lymph node involvement [7,8]. Adjuvant therapy may consist of 5 years of endocrine therapy alone, if the primary tumor carries low-risk features and is hormone receptor positive. In the absence of medical contraindications, adjuvant chemotherapy should be recommended for the treatment of high-risk hormone receptor-positive patients and for the majority of patients who undergo surgical resection of hormone receptor-negative tumors. In addition, targeted therapy with the monoclonal antibody trastuzumab is indicated in patients with HER2-positive tumors.
Approximately a quarter of patients with localized breast cancer present with locally advanced disease owing to a tumor size of more than 5 cm, presence of fixed axillary or ipsilateral supraclavicular, infraclavicular or internal mammary lymph node involvement and/or presence of skin involvement (stage IIb or III disease). Without systemic therapy, these patients have up to an 80% chance of recurrence after surgical resection [9]. In addition, some patients may not be candidates for breast-conserving surgery, or even mastectomy, owing to the size of tumor or extent of skin involvement. In these patients, the use of chemotherapy or, in select cases, endocrine therapy prior to surgical resection (termed neoadjuvant therapy) is usually recommended.
Since the administration of neoadjuvant chemotherapy allows response assessment in an intact primary tumor, it is often considered in the absence of locally advanced disease for the treatment of patients who are candidates for adjuvant chemotherapy (i.e., triple-negative breast cancer or involved lymph nodes). When systemic therapy is given in the neoadjuvant setting, the effects of treatment are directly observed and therapy can be altered based on tumor response, which results in less patient exposure to the toxicity of ineffective therapy. This is not the case when adjuvant therapy is administered after surgical resection of the tumor, so neoadjuvant therapy should be strongly considered in patients for whom chemotherapy or trastuzumab-based therapy is indicated to reduce the risk of systemic recurrence (i.e., known lymph node-positive disease and/or primary tumors >1 cm in size that are either HER2-positive or hormone receptor negative). Most patients treated with neoadjuvant chemotherapy will have either a complete or partial response in the primary tumor and/or draining lymph nodes [10]. By decreasing the size of the primary tumor, patients may require a less extensive operative procedure or, in some cases, unresectable tumors become candidates for surgical resection. In addition, from a research perspective, neoadjuvant therapy in patients with locally advanced disease provides an invaluable opportunity to obtain tissue before and after therapy to correlate tumor response with molecular parameters.
Patients with advanced breast cancer are those diagnosed with distant metastasis to the bone, nonadjacent lymph nodes or visceral organs either at the time of initial breast cancer diagnosis (stage IV) or as a relapse after treatment of localized breast cancer. Prognosis in patients with advanced breast cancer varies depending upon: the location and extent of metastatic disease, elapsed time from original diagnosis and development of metastatic cancer and the receptor status of the primary tumor and/or metastatic disease. In general, advanced breast cancer carries a median survival of approximately 2 years after documentation of metastasis. Poor prognostic indicators include visceral organ involvement, CNS involvement, ER/PR/HER2-negative disease and a short disease-free interval from the time of original diagnosis. The treatment for the majority of patients with advanced breast cancer is considered palliative in nature, although durable complete remissions have been achieved in a small number of patients [11].
In patients who have hormone-receptor positive metastatic cancer without extensive visceral organ involvement or symptoms necessitating rapid response to therapy, a trial of endocrine therapy is indicated as first line therapy. Several endocrine therapies have demonstrated benefit in the advanced setting
Causes of intrinsic drug resistance in breast cancer
As mentioned previously, cancer cell resistance to commonly prescribed therapies accounts for an overwhelming majority of breast cancer-related deaths. It is hoped that studying the etiology of cancer cell resistance will result in the opportunity to develop novel chemotherapy compounds or targeted therapy combinations to improve survival outcome.
Alterations in target proteins & intracellular drug concentrations
Targeted therapy for the treatment of breast cancer logically requires the expression of target proteins, such as ER and HER2. Clinical data have validated that the absence of ER is associated with a low likelihood of benefit from endocrine therapy [8,12]. Based upon preclinical data, it is also assumed that HER2 overexpression is necessary for a response to trastuzumab-targeted therapies [13]. Loss of receptor expression while receiving targeted therapy has been documented for both ER and HER2 and this loss has been associated with worsening prognosis [14,15].
Although chemotherapy is not historically considered ‘targeted therapy’, since the mechanisms of action for many chemotherapy drugs have been elucidated, alterations in target proteins have been implicated in drug resistance. Anthracyclines and taxanes are the most active chemotherapy agents for the treatment of breast cancer. Anthracyclines bind topoisomerase II (topo-II), inhibit DNA replication and induce DNA fragmentation, which eventually leads to programmed cell death or apoptosis [16]. Taxanes bind β-tubulin and promote microtubule stabilization leading to mitotic arrest and induction of apoptosis [17]. Modulation of target proteins, such as topo-II (anthracyclines) and β-tubulin (taxanes), has been implicated in drug resistance.
Commonly used breast cancer therapies
Anthracyclines†
Taxanes†
S-fluorouracil†
Cyclophosphamide†
Methotrexate†
Gemcitabine
Vinorelbine
Capecitabine
Ixabepilone
Tamoxifen
Aromatase Inhibitors†
Fulvestrant
Megesterol
Trastuzumab†
Lapatinib
Bevacizumab
Preclinical models have suggested that both the expression of topo-II and the nuclear localization of the enzyme may be important factors for anthracycline sensitivity [18]. Topo-II levels have correlated with response in some cell lines [19]; however, tumor samples demonstrate a wide range of topo-II expression and protein levels have little predictive value in treated patients [20,21]. Clinical trials measuring the expression of topo-II and response to anthracyclines demonstrated mixed results, with some studies showing an improved response in tumors with high expression of topo-II and others showing no association [18].
Taxanes affect microtubule formation, which leads to disruption in mitosis and intracellular trafficking. Microtubules are formed from the alignment of heterodimers of α- and β-tubulin. Based upon variability in the C-terminus, several different isotypes of β-tubulin have been described, each with notable differences in assembly properties and drug-binding capabilities [22]. Class III β-tubulin has slower polymerization rates, forms less stable microtubules and is less sensitive to the stabilization effects of taxanes in multiple cell lines, including breast cancer cell lines [23]. Some clinical studies have associated high βIII-tubulin levels with poor response to taxanes [24], while others have found no such association [25].
Even though both anthracyclines and taxanes act upon different cellular processes, they both require sufficient intracellular drug concentrations to exert their effect. The ATP-binding cassette (ABC) transporters are energy-dependent, membrane-bound proteins that serve as drug efflux pumps [26]. Although 48 human ABC genes have been identified and subdivided into several distinct groups (ABCA–ABCG), little is known about the role of many of these transporters in chemotherapy resistance [27,28]. Drug efflux pumps also play an important role in detoxification, as evidenced in their tissue distribution in brush boarder membranes of intestinal cells, the biliary canalicular membrane of hepatocytes, the luminal membrane in the proximal tubules of the kidney and the epithelium of the blood–brain barrier [27].
P-glycoprotein (P-gp) is the product of the multidrug-resistance gene (
Deregulation of apoptosis
Although inhibition of proliferation is an important goal for breast cancer therapy, most drugs that eradicate the disease do so by inducing apoptosis. Several molecular pathways play a role in modulating the antiapoptotic effect of breast cancer treatments.
The Bcl-2 family of proteins are regulators of programmed cell death (PCD) or apoptosis
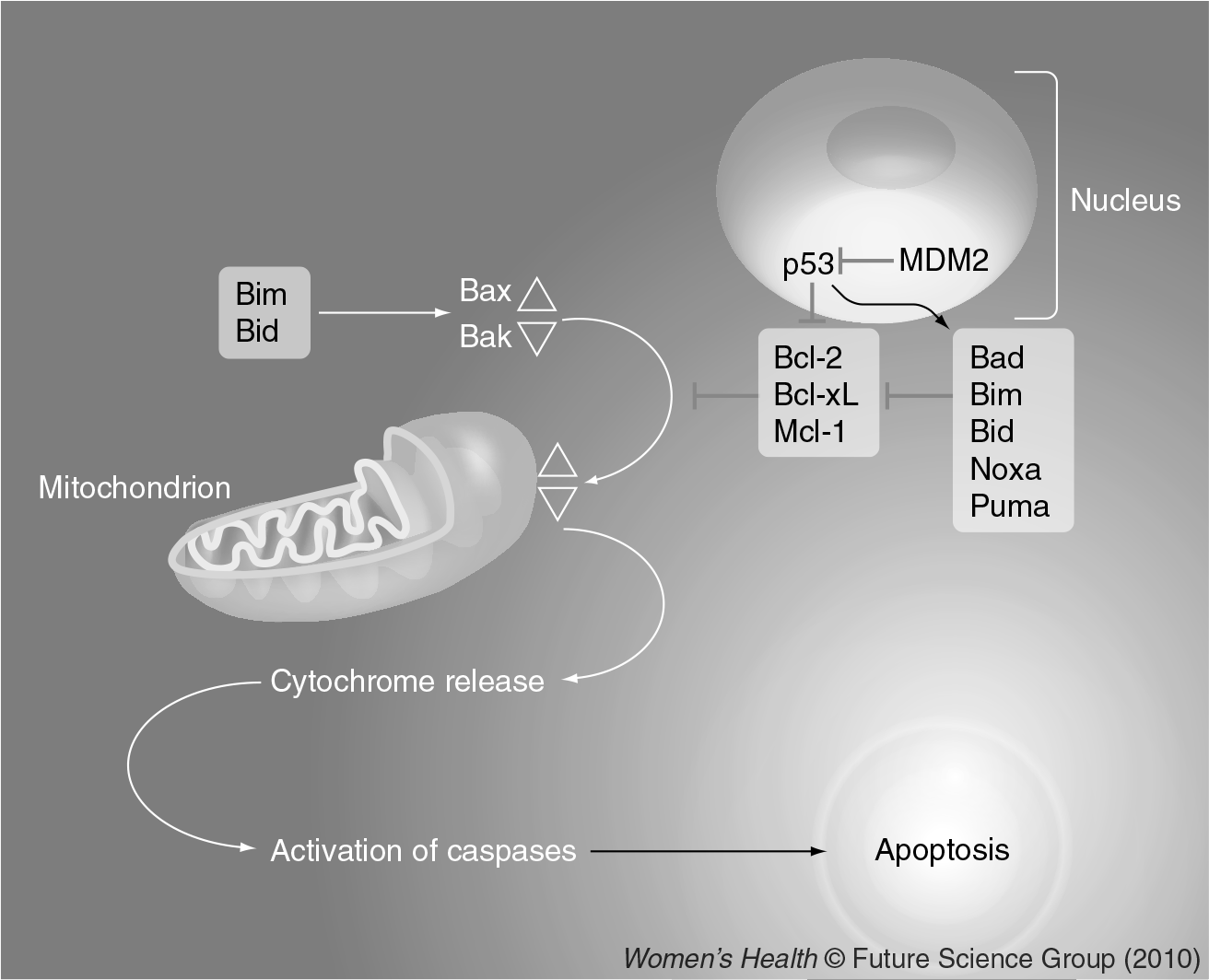
Apoptosis: intrinsic pathway.
Bcl-2 is a 26-kDa cation channel protein that localizes to the mitochondrial, endoplasmic reticulum and nuclear membranes [35] and exerts its effect by regulating mitochondrial membrane permeabilization. Cells that overexpress Bcl-2 are protected from the cytotoxic effects of chemotherapy and irraditation and numerous preclinical studies suggest that Bcl-2 may be an important therapeutic target to reverse therapy resistance [33,36,37]. Bcl-2 is commonly expressed in epithelial malignancies, such as breast cancer, often in the absence of chromosomal translocations or gene rearrangements. Reports of expression of Bcl-2 in breast carcinoma vary, with 40–80% of invasive carcinomas expressing levels of Bcl-2 protein detected using immunohistochemistry [38–41]. Several studies have associated Bcl-2 expression with chemotherapy resistance [40,42,43]. Preclinical models have also established that downregulation of Bcl-2 protein leads to an increase in apoptosis and improved response to chemotherapy [44].
Cellular stress induces activation of p53, which causes restraint of cell cycle progression and promotion of apoptosis if cellular damage cannot be repaired. Bax, Noxa and Puma can be transactivated by p53 and p53 can also inactivate Bcl-2 and Bcl-XL [45]. MDM2 inhibits p53 activity through multiple mechanisms including inhibition of transcriptional activity, export to the cytoplasm and proteasomal degradation.
The phosphatidylinositol 3-kinase (PI3K)/Akt pathway is also involved in the regulation of apoptosis

PI3K/Akt pathway activation.
The PI3K/Akt pathway is often activated in HER2+ tumors, mostly owing to heterodimerization of HER2-positive with HER3 [51]. In addition, mutations in the
The IGF receptor-1 is also important in the regulation of apoptosis. IGF1R is a heterotetrameric protein that consists of two polypeptide chains containing an extracellular α-subunit and β-subunit [62]. Ligands, such as IGF-I and IGF-II, signal through IGF1R and can this can lead to activation of the PI3K pathway and regulation of Bcl-2 protein expression. IGF1R shares similar homology to the insulin receptor (IR) and can form hybridized IGF1R and IR complexes, which demonstrate higher ligand binding affinity [63].
Activation of the IGF pathway induces cell migration and evasion of apoptosis in both normal mouse mammary cells and breast cancer cells grown
Role of cancer stem cells in therapy resistance
Emerging data have provided evidence that, in some breast cancers, multipotent tissue-specific stem cells or their progeny can undergo malignant transformation and are thus designated cancer stem cells or cancer-initiating stem cells (CSCs) [70]. CSCs can be isolated using flow cytometry with specific cell surface markers (CD44+/CD24-/low). CSCs possess the ability to self-renew, differentiate and undergo epithelial-to-mesenchymal transition, a key step in cancer metastasis. Although these cells make up only a small population of untreated primary breast carcinomas, they are enriched in residual breast tumors sampled after neoadjuvant chemotherapy, suggesting intrinsic resistance to treatment [71,72].
Genomic analysis of cell lines has identified a gene expression signature for CD44+/CD24-/low CSCs [71]. When pre- and post-chemotherapy breast primary tissue samples were compared, the post-treatment samples had statistically higher correlations with the CSC signature compared with pre-treatment samples. This signature was weighted for PI3K signaling, which has been implicated in breast CSC viability [73]. The Notch and Hedgehog pathways are each involved in embryogenesis and control growth, dedifferentiation and survival in CSC [74]. Activation of Notch occurs through ligand binding and subsequent cleavage of the receptor by γ-secretase [75]. The Hedgehog pathway consists of the Hedgehog ligands (Dhh, Ihh and Shh) and three transmembrane receptors, patched 1 protein, Smoothened (Smo) and Hedgehog-interacting protein [76]. Ligand binding to Patch1 results in Smo activation and subsequent downstream signaling.
Novel agents to overcome drug resistance
First-generation inhibitors of P-gp, such as verapamil, quinidine or cyclosporine, were active in preclinical models, but were found to be weak inhibitors that were toxic at the high doses needed to inhibit drug efflux in patients. Quinidine had no benefit combined with epirubicin for the treatment of breast cancer [77]; however, verapamil showed improvement in overall survival and response rate when combined with vindestine and 5-fluorouracil [78]. Eventually, pharmacokinetic interactions and off-target effects ended further development of these agents. Second-generation inhibitors, such as PSC-833, were mainly tested on nonbreast cancer patients, but resulted in significant pharmacokinetic interaction necessitating reduced chemotherapy dosing [79]. The interaction was not seen in all patients, so underdosing of treatment may have accounted for negative therapeutic outcome. Third-generation inhibitors, such as LY-335979 and XR-9576, bind P-gp with greater affinity and are associated with less pharmacokinetic interaction [80]. The role of these agents in combination with chemotherapy for the treatment of breast cancer needs to be further defined through clinical trials; however, an early randomized Phase II study did not show clinical benefit [81]. Novel formulations of chemotherapy agents, which are poor substrates for MDR1, such as the epothilones, have demonstrated clinical benefit in a subset of patients with anthracycline-and taxane-resistant metastatic breast cancer [82–84]. Epothilones, such as ixabepilone, have also shown activity in βIII-tubulin-overexpressing xenografts [23].
Preclinical models have demonstrated that downregulation of Bcl-2 was observed with the administration of antisense Bcl-2, which enhanced the cytoxicity of chemotherapy [37]. Although the use of antisense technology seemed promising, most subsequent clinical trials in solid tumors did not meet their specified clinical end points of improved efficacy as a single agent or in combination with chemotherapy [85]. These negative results are probably due to drug delivery issues from antisense therapy rather than Bcl-2 as a target.
There are several reasons to suggest that inhibiting Bcl-2 function with small molecule inhibitors could be more advantageous for the treatment of solid tumors. First, the smaller molecular size of these drugs may allow for improved tumor penetration. Second, the anti-Bcl-2 effects require much lower concentrations of drug to exert their effect in cancer cells. Finally, the oral route of administration allows a more practical dosing schedule that may improve the prolonged administration required for maximum drug exposure.
Preclinical models have demonstrated that IGF1R inhibition with antibodies or antisense approaches suppresses growth and induces apoptosis in breast cancer xenograft models [65,66]. Inhibition of IGF1R with small molecule inhibitors has shown added antitumor activity when combined with endocrine therapy and chemotherapy in preclinical models. Ongoing trials are accruing patients with metastatic disease in order to determine if these drugs will be of added benefit in combination with endocrine therapy or chemotherapy for the treatment of breast cancer.
Inhibition of the PI3K pathway through inhibition of mTOR has shown benefit in a select group of patients with metastatic breast cancer. Everolimus has demonstrated a response rate of 9.2% in heavily pretreated patients with metastatic breast cancer [86]. Although a randomized Phase II study showed early evidence of benefit when letrozole was combined with everolimus in patients with ER- and/or PR-positive metastatic breast cancer, a later randomized Phase III trial failed to confirm these findings [87,88]. Phase I/II studies of temsirolimus in combination with chemotherapy or trastuzumab are ongoing in patients with metastatic breast cancer.
Cancer stem cells may be inhibited by targeting pathways such as PI3K, Notch or Hedgehog. Activation of the Notch signaling pathway involves γ-secretase, and inhibitors of this enzyme are now in early phase clinical trials. The Hedgehog pathway can be targeted by inhibiting Smo, and inhibitors of Smo are showing activity against basal cell carcinoma, a tumor type frequently dependent upon the Hedgehog pathway, in early phase clinical trials [89]. Ongoing studies are planned or are currently accruing patients to study the inhibition of stem cells using γ-secretase or Smo inhibitors in combination with endocrine therapy or chemotherapy for the treatment of patients with advanced breast cancer.
Future perspective
Intrinsic resistance to breast cancer therapy is a complex problem with multiple etiologies. Although the use of preclinical models has enhanced the study of intrinsic resistance, data from clinical trials are scarce but emerging. The clinical paradigms for studying breast cancer resistance are also improving with the increased use of neoadjuvant chemotherapy and further development of molecular technologies to study residual disease after therapy. Promising agents are in early phase clinical trials and will hopefully result in greater response and improved time-to-progression for patients with breast cancer.
Executive summary
Topoisomerase II expression and/or localization may influence response to anthracyclines.
Expression of βIII-tubulin has been associated with poor response to taxanes and may be overcome using novel compounds, such as epothilones.
Drug efflux pumps have been linked to chemotherapy resistance, but targeting these agents with inhibitors has been challenging. Clinical trials are ongoing with third-generation inhibitors.
The B-cell lymphoma 2 family of proteins are regulators of apoptosis, commonly expressed in breast cancer; they are associated with chemotherapy resistance and can be targeted using small molecular inhibitors.
The PI3K pathway also regulates apoptosis and inhibitors of this pathway have demonstrated response in a subset of patients with metastatic disease.
IGF1 receptor-1 is a membrane-bound receptor involved in the regulation of apoptosis. Monoclonal antibodies and low-molecular-weight inhibitors are currently under investigation in combination with chemotherapy and hormonal therapy for the treatment of advanced breast cancer.
Multipotent stem cells can undergo malignant transformation and are the cause of intrinsic resistance in a subset of breast cancers.
Novel therapeutic agents targeting the Notch and Hedgehog pathways may prove beneficial for the treatment of resistance related to cancer stem cells.
Footnotes