
Abstract
Objective
It is well known that physical trauma to skin caused by repetitive friction is a primary component of blister formation. Although friction blisters in a wilderness setting particularly occur on the feet and ankles, they often form on the hands and fingers during such activities as white-water rafting, kayaking, and canoeing. These blisters are often incapacitating and can have disabling consequences. This article describes laboratory and clinical experiments testing the efficacy of a new bandage technology in reducing shear and friction forces on the skin.
Methods
A custom-made apparatus was used in a laboratory setting to measure and compare the surface coefficient of friction of 11 bandages. In addition, a controlled clinical study was conducted on 15 healthy, able-bodied female subjects (mean age 35 years), where the same apparatus was used to measure the coefficient of friction of the skin over the medial tibial cortex with and without the new technology device in place.
Results
This laboratory study demonstrated the new device to have the lowest surface coefficient of friction of any bandage tested (0.57). For example, the common product Moleskin was 21% higher (0.67), with all other products testing at least 64% higher (>0.94). In the clinical study, the new technology device reduced the coefficient of friction on the skin by 31% (0.225 vs 0.327), and this difference was statistically significant (
Conclusions
A bandage containing a new technology demonstrated the lowest surface coefficient of friction of any bandage tested. In addition, clinical tests performed with the same bandage demonstrated significant reduction of the coefficient of friction on the skin.
Introduction
A friction blister refers to a cleavage of the epidermal layers between the stratum granulosum and the stratum spinosum layers, leaving intact the 3 most superficial layers (stratum corneum, stratum lucidum, and stratum granulosum) to compose the roof of the blister. 1 –3
In most civilian activities, friction blisters are a painful but typically minor annoyance. They usually require only simple first aid, a short period of limited activity, and protection of the affected area with a bandage. Activities in more remote areas, however, expose individuals to risk of injuries and illnesses not usually found in the urban setting. 4 Friction blisters have historically been one of the most common of all injuries and illnesses experienced by persons participating in wilderness activities.1,5–9. Because blisters often limit individual mobility, their impact in a remote setting is potentially more serious. In addition, they provide a portal for infection. This risk is always higher in an aquatic environment.9,10
Participation by Americans in wilderness camping, backpacking, and day hiking has grown to more than 55 million persons per year.6,7 There is, however, limited epidemiological research on injuries and illnesses associated with soft tissue wounds such as blisters. The few studies available show an incidence of blisters in wilderness participation to range from 7% to 54%.4,6,7 The variance in blister incidence is somewhat reflective of the type of study and the study population. For example, in a study of experienced Appalachian Trail hikers between the ages of 34 and 51, Crouse and Josephs 6 demonstrated a 7% incidence of blister formation. The nonimmediacy with which these participants recorded their blisters perhaps contributed to this lower rate. On the other hand, Twombly and Schussman 8 focused on 343 participants in a Colorado Outward Bound School's 23-day alpine course. Their study primarily involved 15- to 18-year-olds with presumably little backpacking experience who were often outfitted in new boots purchased for the course. The authors’ data, recorded on self-administered survey forms and collected on a regular and immediate basis, indicated 46% of male participants developed a blister injury compared with 54% of the females. In a study carried out in Yosemite National Park, Kogut and Rodewald 4 obtained data from 301 experienced overnight hikers with an average age of 34 years. This study demonstrated a blister incidence of 24%.
In spite of advancements in boot and sock fit and technology available to the wilderness community, blister injuries remain a very common problem.4,6 Similarly, blister occurrence in the military is a serious problem.1,11,12 There has been little corresponding reduction in blister incidence despite attempts to improve military boot fit, style, and composition. 13 –15 The efficacy of foot powders in reducing blister incidence has not proven positive; the incidence of blisters in military marching troops actually increased with the use of such products.13,14 Modifications of the socks worn by soldiers have met with some limited success.5,16 There is, moreover, a paucity of evidence-based laboratory or clinical studies addressing the etiology and epidemiology of blister formation in the military setting.1,11,12
The complex interaction of the etiological factors associated with foot blisters, and skin breakdown in general, creates an engineering challenge: how to design interfacing technology that provides adequate mechanical stability while protecting the soft tissues from trauma. 1 Wilderness activities are primarily performed in environments at a great distance from customary medical facilities such as primary care clinics and emergency departments. This separation makes emergency preparedness for blister prevention and care in wilderness activities even more vital.
Etiology and Factors Associated with Soft Tissue Breakdown
There are a host of external factors, both mechanical and biochemical, that contribute to the development of blister formation; however, the presence of mechanical loads at the interface between soft tissues and the supporting surface is considered an initiating cause.11,12 When loads are applied to soft tissues, the underlying blood vessels are partially or completely occluded, and oxygen and other nutrients are not delivered at a rate sufficient to satisfy the metabolic demands of the soft tissue constituents (fascia, subcutaneous tissues, dermis, and epidermis). To survive, the cells must draw upon their stores of energy. The lymphatic drainage is also impaired, and the breakdown products of metabolism accumulate within both the interstitial spaces and the cells. As energy stores diminish, the cellular processes begin to fail, ionic gradients across cellular membranes begin to dissipate, and cell necrosis occurs.
Several investigators have used both animal and human models to address the etiology of soft tissue breakdown and have also suggested the existence of an inverse relationship between externally applied pressure and the time required for soft tissue ulceration. 17 –19 External pressure has long been the focus of etiological investigations on the mechanics of skin breakdown, in particular, pressure ulcer formation. 20 The effects of other etiological mechanical factors such as shear forces, friction, pressure gradients, and tissue deformation are far less studied. Other extrinsic factors known to play a key role in blister formation include temperature, moisture, and pH.3,21–23 Intrinsic factors known to compromise soft tissue include age, state of consciousness, smoking, local and systemic infection, anemia, and edema.18,24,25
Shear and Friction Effects on Blister Formation
Shear forces are nonnormal (nonperpendicular) forces that are applied tangentially to the tissue surface. Friction is a phenomenon that describes the ability of a surface to prevent motion of this shear force. The coefficient of friction refers to the ratio of shear force to normal (perpendicular) force necessary to initiate movement of the materials relative to the skin. 26 When the applied force is too much for the skin coefficient of friction to grasp, slippage occurs (Figure 1). Friction properties of human skin depend not only on the skin's texture, suppleness, and hydration levels, but also on its interactions with external support surfaces and the outside environment. 27 Indeed, the stiffness 23 and coefficient of friction23,28,29 of the stratum corneum increase with increased humidity and intermediate moisture, respectively, whereas extreme dryness and wetness will tend to decrease skin friction. 28 The injurious effects of shear forces on skin and the underlying tissues may rupture the epidermis and occlude blood and interstitial fluid flow by stretching and compressing the skin. The added effect of repetitive friction tends to abrade and heat the skin and will cause blisters. 26
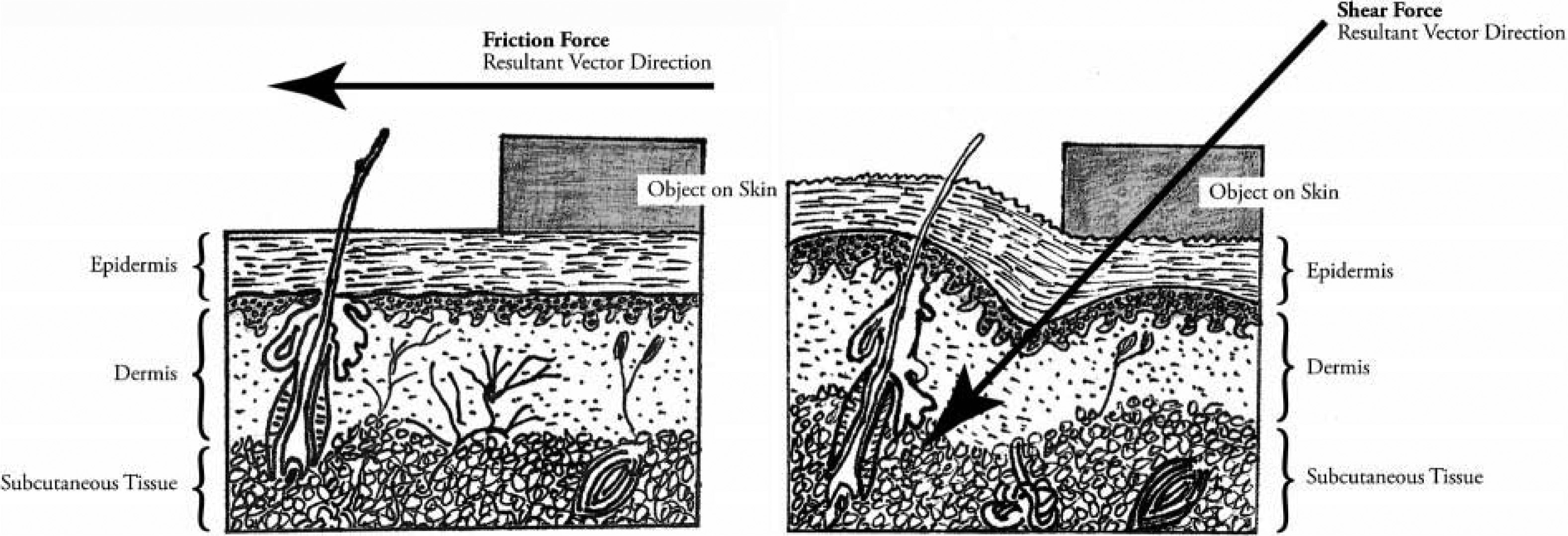
Cross-section illustration of human skin and its appendages. The resultant vector direction of a friction force affects the epidermis by dragging or rubbing the epidermis back and forth (left). The resultant vector direction of a shear force affects both the epidermis and the dermal structures at an angle (right).
The literature indicates that nonnormal loading has varying results on the integrity of soft tissues, with localized shear and high gradient pressure distributions (eg, loading of bony prominences) causing more damage than more uniformly distributed multiaxial stresses (eg, hydrostatic pressure). 30 Several investigators have shown shear force reduces the normal pressure required to produce soft tissue ischemia and breakdown.3,31–35 Bennett et al 35 demonstrated that the pressure level sufficient to occlude blood flow on the thenar eminence was reduced by approximately 50% when simultaneous shear force was applied. Other investigators demonstrated cyclical loading associated with various combinations of applied force and cycle numbers could cause soft tissue breakdown.28,29 In a study on human subjects, Naylor 28 demonstrated when slow 0.33-Hz cyclic normal and shear forces were applied to the skin, the energy required to induce a blister was greater for a low force–high number of cycles combination than for a high force–low number of cycles combination.
Treatment of Friction Blisters
Individuals participating in wilderness activities are at greater risk of skin breakdown (eg, foot blisters) because the magnitude and duration of loads is greater than what tissues usually experience.
34
Moreover, many of the loaded skin sites are ill suited and unaccustomed to mechanical load bearing, and a reduction of the force and duration of these mechanical loads is inconsistent with the functional expectations in a wilderness setting.
36
As a result, individuals participating in wilderness activities may require auxiliary products to prevent or treat skin breakdown. There are a host of products utilized for this purpose. Examples of commonly used over-the-counter products for blister treatment include Moleskin (Schering-Plough Corporation, Kenilworth, NJ), a flannel-like material coated with a pressure-sensitive adhesive pad that is cut to shape. Other newer products contain hydrocolloid gels, which maintain a moist environment for accelerated wound healing. Products suitable for use on multiple areas of the foot and ankle are often preshaped into single-unit bandages for quick application. Many currently available products have undesirable characteristics such as the following: The vast majority of products are thick in profile, usually between 20 and 35 mm (0.020 and 0.035 inches). This level of thickness can cause further skin breakdown by increasing pressure between an already-tight boot and the adjacent skin surface. Several products, such as Moleskin, do not easily conform to complex anatomical areas such as the toes or malleoli (ankles).
Most current products provide padding, a moist environment, and possibly some friction reduction. None, however, have been demonstrated to reduce shear and friction forces on the skin.
Development of the Bursatek Technology
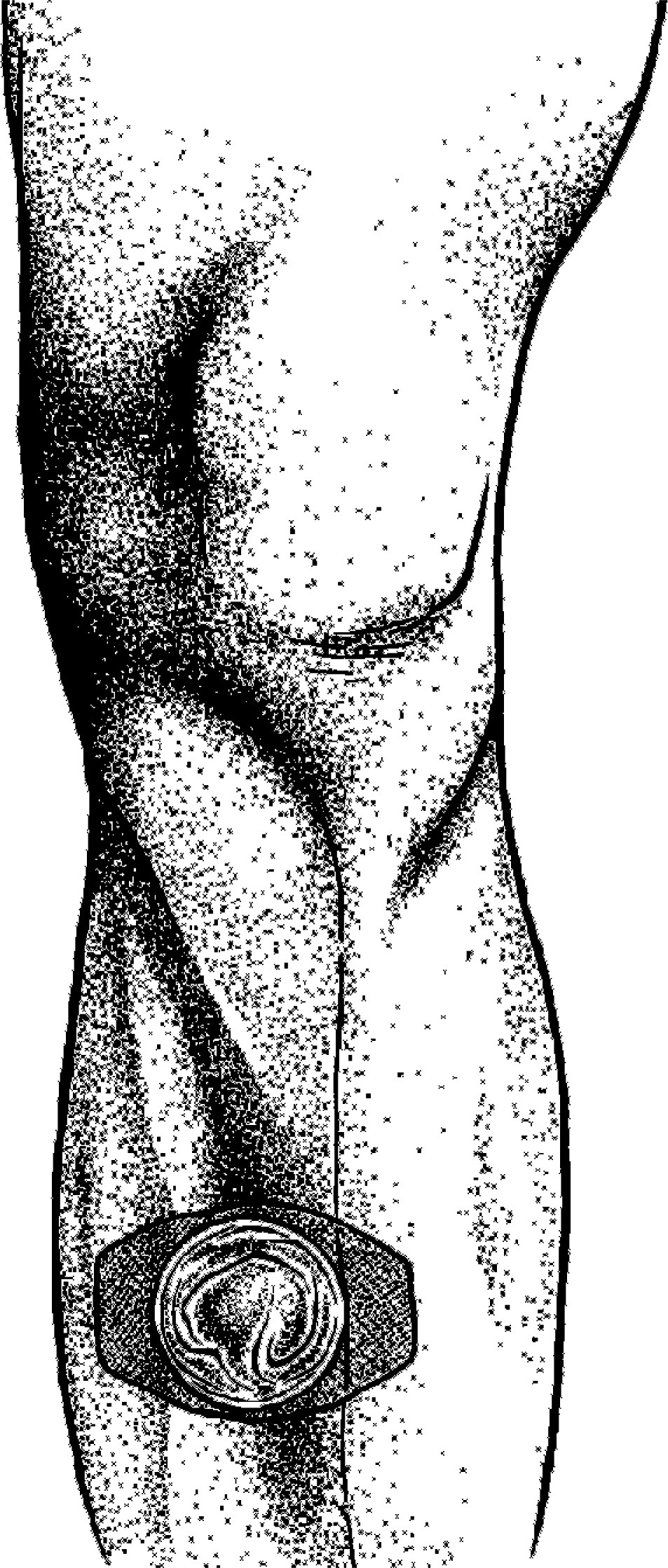
Ordinary daily activities such as sitting, walking, gripping, and sleeping expose the body's skin to pressure, shear, and friction. The human body has developed special friction- and shear-relieving anatomical structures called bursae. These small synovial membrane-lined sacs contain small quantities of fluid (Figure 2). They are located in areas where opposing surfaces move with respect to each other (eg, where tendons rub against other tendons or where soft tissue moves over bony prominences, as seen at the knee and elbow). When a force is applied to one of these areas, one surface of the bursa glides over the opposite surface. This gliding movement effectively reduces shear and friction and redirects the pressure vector (Figure 3).
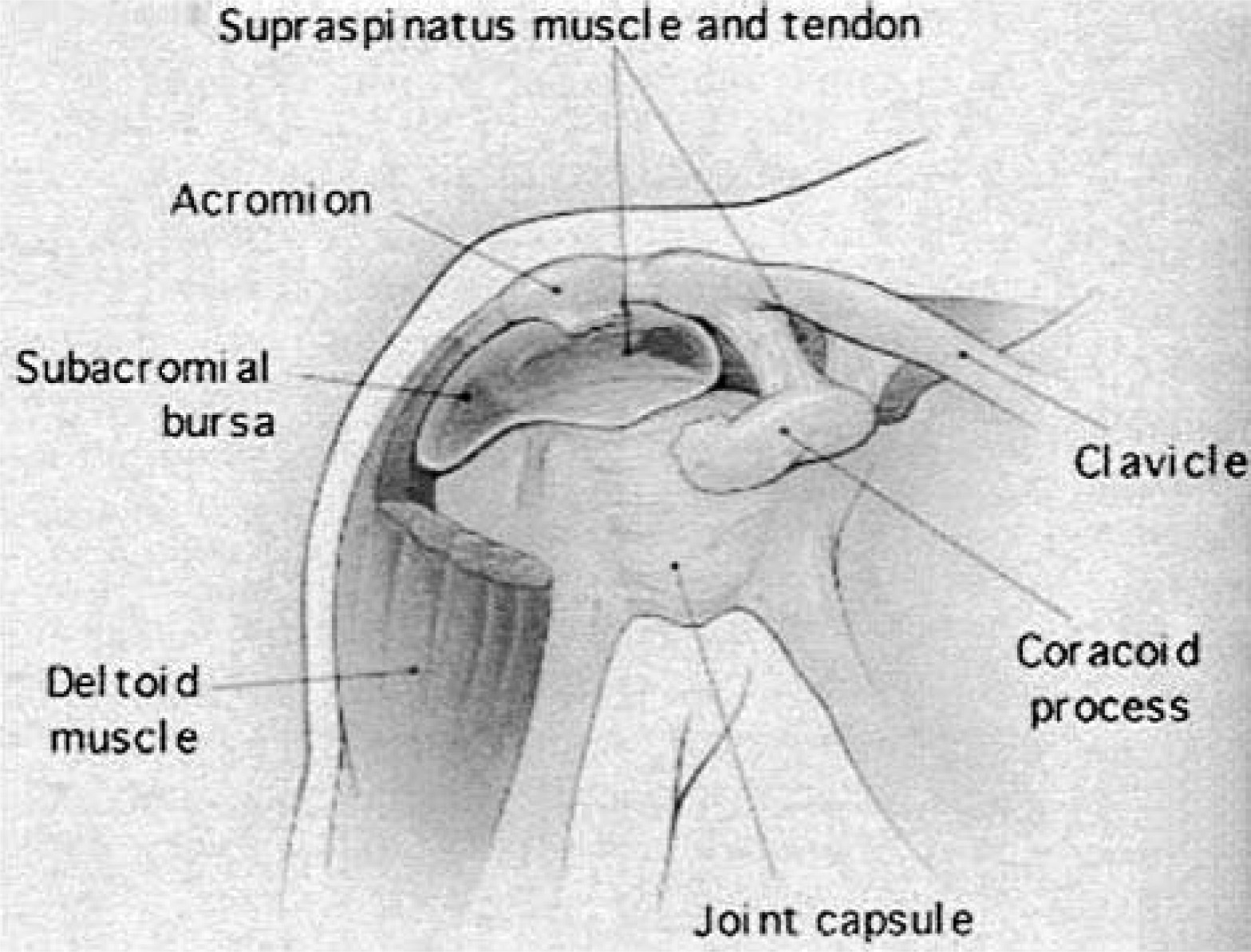
Illustration of a bursa found at the shoulder girdle.
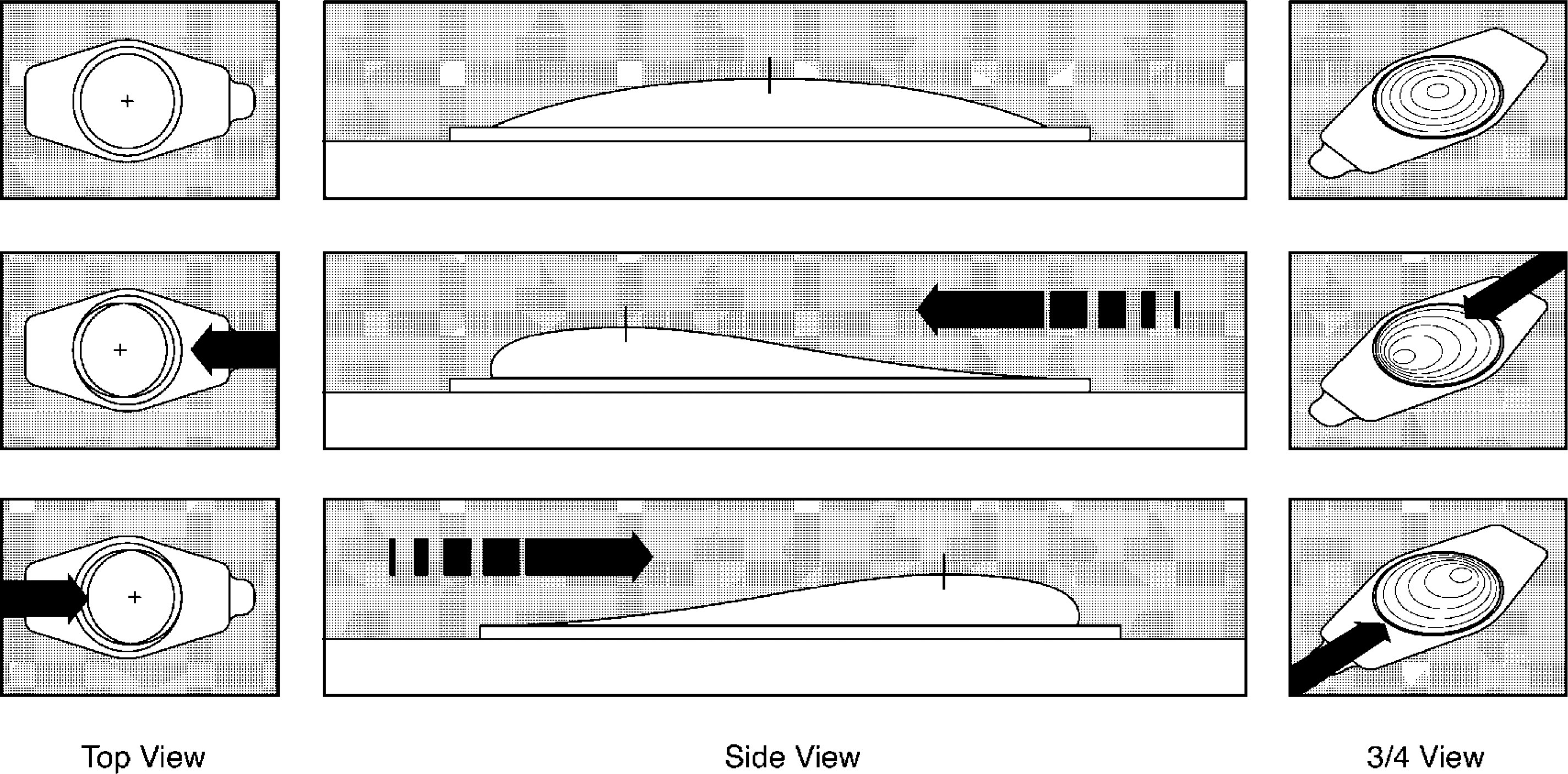
The effects of shear forces on the movement of the Bursatek dome layer. (top) The Bursatek with no load. (middle) Movement of the Bursatek dome to the left (up to 4 mm) after a leftward shear force. (bottom) Movement of the Bursatek dome to the right (up to 4 mm) after a rightward shear force.
The Bursatek bandage, used in the 2 studies presented in this work, has been modeled after the body's bursal sac. It is composed of 2 layers of breathable plastic film bonded together, except for an area in the center (Figure 4). This central dome area forms a collapsed perforated “bubble” between 2 low-friction polyethylene plastic sheets. These sheets glide freely when shear (nonnormal) or friction forces are applied (Figure 4). This has been termed the “gliding principle,” because under load the dome area is designed to travel up to 4 mm in either direction or a total of 8 mm in both directions of the XY plane. For adhesion, a pressure-sensitive adhesive is applied to the bottom of a vapor permeable (breathable) skin contact layer of the device. This polyurethane layer stretches and conforms to complex anatomical shapes as seen at the heel, malleoli, or toes.
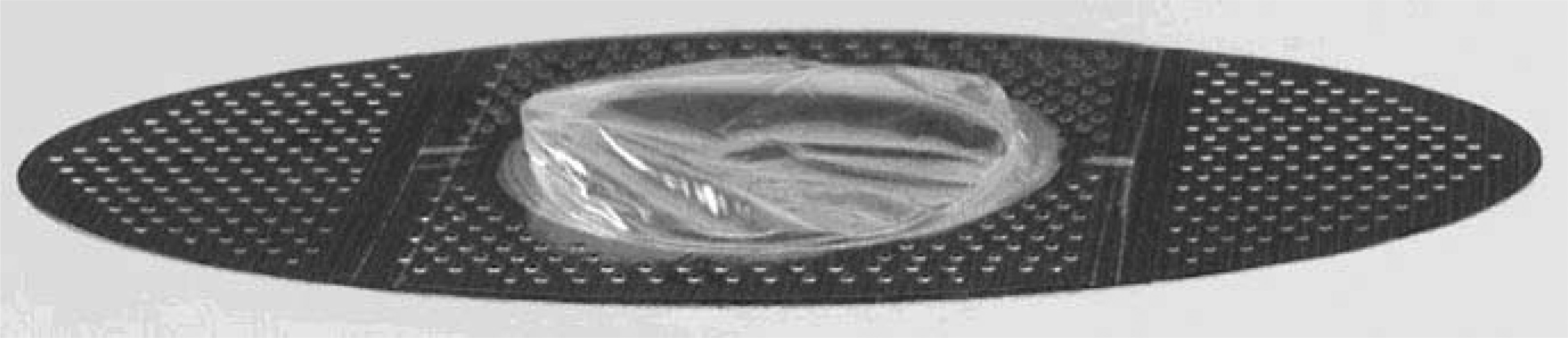
Photograph of a prototype Bursatek bandage, showing the dome flexibility, low profile configuration, and perforated border.
The first product developed utilizing Bursatek technology is the bandage device shown in Figure 4. An important design quality of this bandage is its low profile. The thickest portion of the device is over the central dome region, equal to a thickness of 152 microns (0.006 inches). Otherwise, the predominant portion around the dome area is 51 microns (0.002 inches) thick. The importance of a low-profile device is to minimize any possibility of increasing the interface pressure in a tight-fitting boot.
Methods
After the Bursatek technology was incorporated into a bandage, the authors evaluated and tested the merits of this device in 2 studies: 1) comparing the coefficient of friction of the Bursatek bandage device with commonly used products and 2) comparing the coefficient of friction on the skin of able-bodied subjects both with and without the Bursatek device in place.
Laboratory Bench Testing
A laboratory study was developed to measure the coefficient of friction of 11 bandage products. The coefficient of friction of each product was measured with a custom-made apparatus designed by the investigators (Figure 5). This apparatus consisted of a frame with an attached ball-bearing slide block to which a vertical rod was secured. A lightweight, hollowed, rigid-plastic end probe (the indentor) incorporated a cylindrical brass bushing, which fit flush over the end of the vertical rod. This allowed the end probe to glide freely in the normal plane. The end-probe tip was flat with a diameter of 1 cm and a small edge radius. Normal load was achieved by placing weights on top of the end probe. A weight rack attached on the side of the apparatus was connected over a pulley to the vertical rod by a cable. A load applied to this side rack applied a shear force to the end probe.
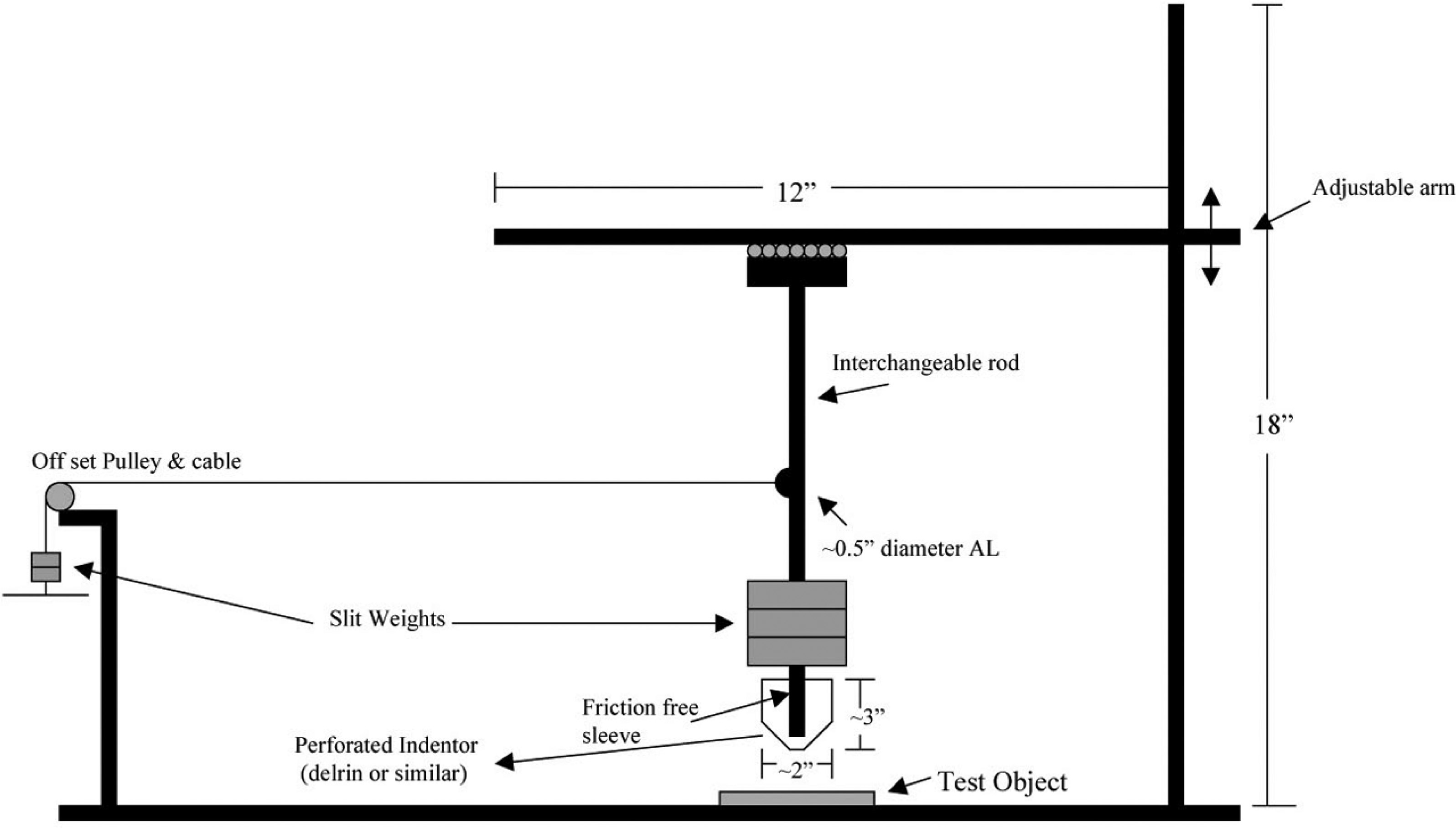
A schematic of the custom-made friction-measurement apparatus.
The Bursatek device and a sampling of 10 additional bandages and dressings commonly used to prevent and treat friction blisters were selected for this study. Each product was adhered to the aluminum apparatus surface by using the product's own pressure-sensitive adhesive to secure attachment. The first operator applied a 237-g (8.3-ounce) normal load above the indentor, then lifted and placed it carefully over the center of each product. The applied load is reasonably representative of a typical amount of normal forces experienced at the heel or toe of a foot inside a boot. A second operator then carefully added small increments of weights, between 10 and 20 g, to the offset pulley to initiate a shear force and continued to add weight with a 5-second pause between weight additions to allow for movement. This operator continually added weight until movement of the indentor occurred. The first operator focused on a finely drawn line between the ball-bearing sliding block and the apparatus frame. This operator was blinded to viewing the product tested. The test was stopped at the instant that movement of the end probe was observed (ie, the lower part of the line [sliding block] moved with respect to the upper part of the line [on the frame]). The coefficient of friction (μ) was then calculated as the ratio of the shear load (F) to the normal load (N). Tests were repeated in triplicate.
Clinical Study
The purpose of this clinical study was to evaluate the efficacy of the Bursatek bandage in reducing the coefficient of friction on the skin of able-bodied subjects. This study received human subject approval by the Institutional Review Board at Legacy Health Systems, Portland, OR.
Fifteen healthy, able-bodied female subjects were selected for testing. The subjects were recruited from established contacts in the local Newport, OR, area. Before conducting human subject testing, written informed consent was obtained from all human subjects. Legacy Health Systems approved the informed consent form.
Female subjects were selected because many routinely shave their legs and were experienced at this task. The skin over the medial tibial cortex, adjacent to the tibial crest, was selected as the site of testing, as used by Sanders et al. 31 This represents a flat and bony region that is suitable for such controlled testing and is reflective of other bony prominent areas on the human body susceptible to skin breakdown.26,37,38 By using the level of the tibial tuberosity as a zero reference, tests were performed 10 cm distal to this reference point 26 (Figure 6). All subjects shaved their legs, including the area of the test site, on the morning of the test. They were instructed to wash their legs with tap water after shaving and were directed not to apply any lotions, creams, or other materials at or near the test site. All subjects were instructed not to perform exercise or strenuous activity during the 3-hour period before the test session so that body temperature would remain at baseline levels. All subjects were required to arrive at the test location 3 hours after shaving. They entered the clinical test room 45 minutes before the scheduled test time so acclimatization to the room temperature and humidity levels could occur. They were then required to complete a short questionnaire form that included basic demographic data and a few questions relating to their ability to undertake the study. Subjects who had difficulty maintaining their knees in 5° of flexion, who participated in any exercise or strenuous activity in the 3-hour period before arrival, or who indicated past or recent skin conditions affecting the test area were omitted from the study.
A schematic representing the Bursatek device over the medial tibial cortex site at a level approximately 10 cm distal to the tibial tuberosity.
The skin test site was prepared with distilled water and wiped dry with a soft dry cloth to remove any dust, dirt, oils, or moisture. 27 The test room temperature was maintained at 23°C (73°F) and at a relative humidity of between 40% and 50% for all tests. 27 Each subject sat on a raised, cushioned chair with 1 leg extended in front and supported on a lower platform (Figure 7).

The test setting with a subject sitting on an adjustable chair with her left leg positioned for testing. An adjustable platform (lever and platform) allowed for positioning of the leg at the correct height and angle for all subjects.
Foam wedges and platform adjustment maintained knee flexion at 5° as measured by a goniometer 26 (Figure 8A). A level was used to position the medial tibial cortex to an exact level plane. The test site was located by measurement and inspection; and was tip marked with a fine indelible ink pen. This fine marking allowed for all tests to be repeated at the exact same location. Skin friction force was measured with a custom-made apparatus designed by the investigators (Figure 5).
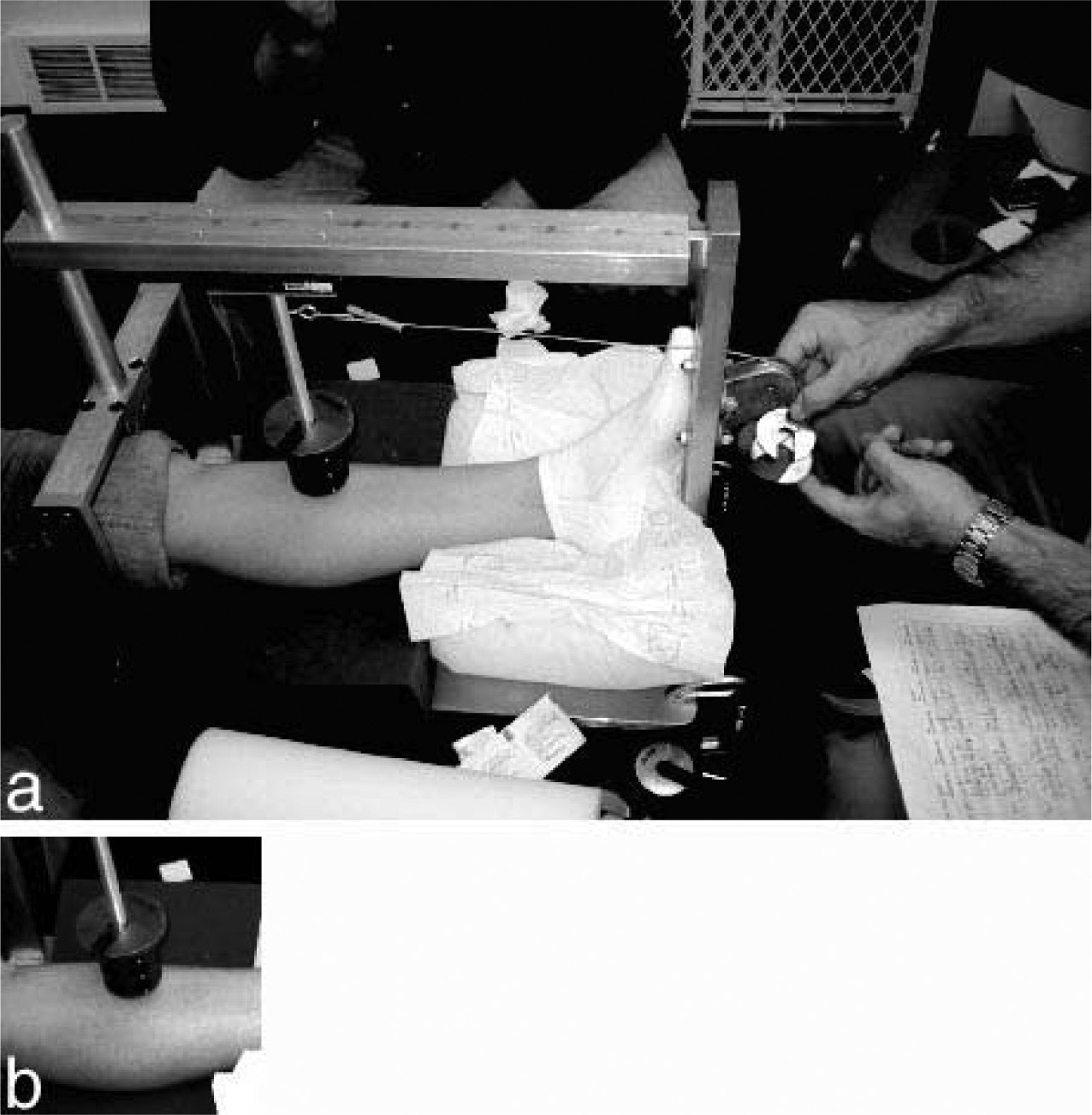
For each test, a 228-g (0.506-pound) axial load was applied to the skin test site via the end probe (Figure 8B). The end probe was placed on and exactly perpendicular to the medial tibial cortex. Small-incremental weights (between 10 and 20 g) were carefully applied to the side rack by the investigator in order to create a shear load (Figure 8A and B). The details of the test protocol are described above in the “Laboratory Bench Testing” section.
Three tests were performed on the skin test site. After each test, the loading probe was removed and then reapplied in the same location to begin the next test. The skin test site was prepared each time before the test was repeated by cleaning it with water, drying the site, and waiting 2 minutes before retesting. With the loading probe, a total of 3 tests were performed with the Bursatek bandage attached to the same skin test site. A single Bursatek bandage was used in this step. It was applied before the first test and removed only after all 3 tests were completed. Testing lasted less than 45 minutes.
Results
Laboratory Bench Testing
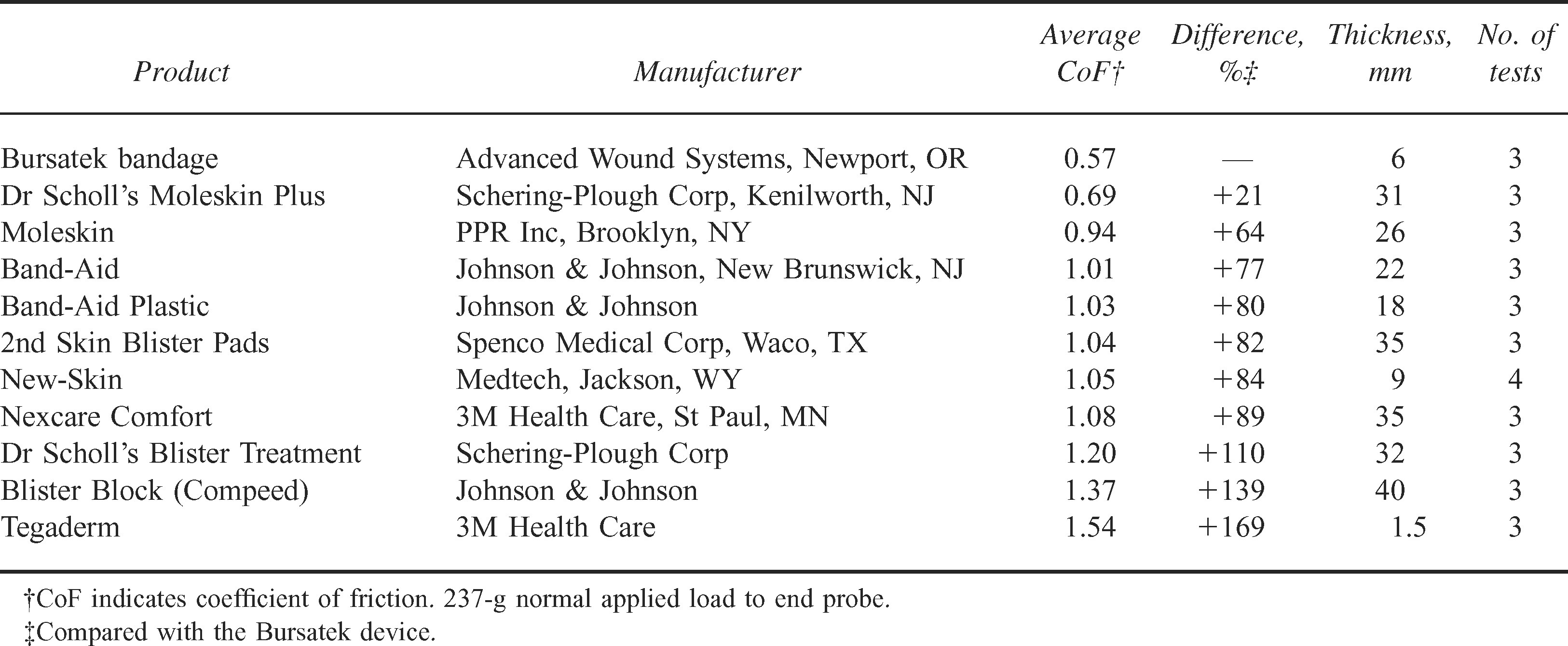
Table 1 illustrates the coefficient of friction of all 11 products tested. The Bursatek prototype bandage provided the lowest coefficient of friction compared with all other products. The next best product was Moleskin, with a coefficient of friction measuring 21% higher than the Bursatek device. All other products fared considerably worse.
Laboratory product comparisons using a custom-made friction-measurement apparatus
Clinical Study
Twenty-one able-bodied female subjects were recruited for this study. Six of these subjects were omitted from the study because of patient noncompliance contrary to protocol requirements. Specifically, the reasons for omission included the following: exceeding the study age range requirement (1 subject), not shaving the test site on the test day (1 subject), tissue edema due to pregnancy (1 subject), and unable to remain still for duration of testing (3 subjects). Table 2 shows a summary of the data collected from 15 subjects. These subjects included 2 Native Americans, 1 Black, 1 Asian, 1 Hispanic, and 10 Caucasians. Two of the 15 subjects were 18 years of age and were skeletally mature for inclusion in the study. The mean age was 35 years (range 18–40 years), mean weight was 71.9 kg (range 57–109 kg), and mean height was 164.5 cm (range 155–173 cm). The room temperature mean was 23°C with a mean relative humidity of 49%. No subjects showed any signs of sweating or discomfort during the tests.
Summary of clinical tests on able-bodied female subjects
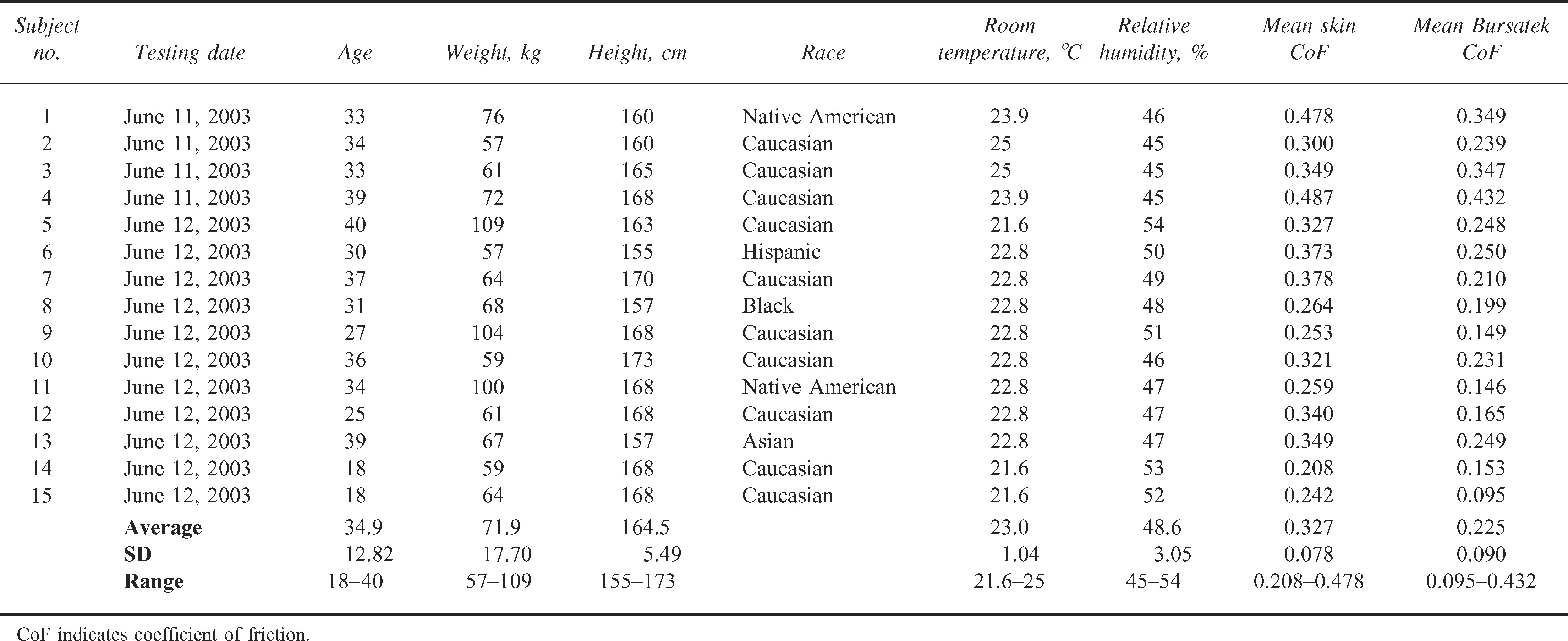
The mean coefficient of friction measured on the skin site was 0.327 (SD 0.078). The mean coefficient of friction measured with the Bursatek bandage over the skin site location was 0.225 (SD 0.090) or 31% lower. A 2-tailed, paired
Discussion
Skin blisters are often incapacitating and can have disabling consequences in the wilderness setting. It is well known that physical trauma to skin caused by repetitive friction is the primary etiological factor of blister formation. By definition, the coefficient of friction (or amount of friction force) is equal to the shear, nonperpendicular (or side-to-side) force divided by the normal (or perpendicular) force. A practical example of this definition can be envisioned by what might take place on the surface of the skin on the heel of a hiker. The friction on the heel under a hiker's boot will be equal to the ratio of the side force of skin movement allowed by the boot (skin push or tangental shear force) to the tightness of the boot (normal or perpendicular force). Placing a material on the skin that reduces the tangental shear force or skin push will reduce the coefficient of friction that the skin experiences. Conversely, reducing the shear forces will reduce the friction force on the skin.
This article presents the findings of laboratory and clinical experiments testing the efficacy of a new bandage technology in reducing shear and friction forces on the skin. When used as a bandage on a skin site, the technology provides 2 paths of mechanical relief: 1) by reducing the shear force experienced at the skin site because of the gliding ability of the collapsible dome and 2) by reducing the friction force between the bandage surface and the boot because of the low surface-friction property of the slick polyethylene dome. In both instances, the friction experienced directly on the skin is reduced.
The bench-testing data presented in this report are the first of their kind to compare the physical properties of available products used for blister prevention and treatment. Two variables were measured: surface coefficient of friction and product thickness. The desirable surface physical property is a low coefficient of friction, which will minimize trauma to the skin and thereby lower the risk of skin breakdown and blister formation. A lower product profile is also desirable because 1) increased thickness usually correlates with reduced product conformity, and 2) increased thickness usually increases tightness (interface pressure) between an already-tight boot and the adjacent skin surface. Of all products tested, the Bursatek device tested with the lowest recorded surface coefficient of friction level. The next best product tested was Moleskin, with a coefficient of friction that measured 21% higher than the Bursatek device. All other products fared considerably worse. These results are not necessarily surprising, for the Bursatek bandage is the only device capable of dynamic movement. All other products tested are composed of laminated films of material designed for barrier protection, padding, or moisture management and are not designed with the intention of gross dynamic movement. The Bursatek device also had the second lowest profile of all products tested. Although Tegaderm (3M Health Care, St Paul, MN) was the thinnest of all tested products, its coefficient of friction was the highest.
The clinical study component of this report involved the measurement of friction over the medial tibial cortex with and without the Bursatek device in place. Data were successfully collected from 15 female subjects who met the protocol requirements. Results indicated that the Bursatek device reduced the coefficient of friction at the medial tibial cortex by 31% compared with skin alone, which is a statistically significant finding. Moreover, intravariation of normal and shear load measures between tests for each subject were small and consistent, which validated the reproducibility of the test procedure and the sensitivity of the apparatus. Overall, the data collected from 15 able-bodied female subjects demonstrated feasibility of the Bursatek bandage in reducing the nominal skin coefficient of friction.
Conclusions
The results for both the laboratory bench and the clinical tests show favorable findings with the use of the Bursatek device. However, these findings are based on 2 controlled studies that focused on measurement of friction only. The authors recognize that important areas for future research should include prospective field studies to investigate the clinical merits of the Bursatek bandage for reducing the incidence of blister development and for blister management and pain reduction.
Footnotes
Funding
Funding for this research was made, in part, by an SBIR research grant, National Institutes of Health, US Department of Health and Human Services, Grant.
1
The authors invented and developed the Bursatek device described in this article. Since the completion of this research, the Bursatek device is now commercially sold under the Blistoban and Bursamed trademark names.