
Abstract
Objective
To survey the incidence of blister formation in a group of military recruits and to determine the efficacy of a new commercially available blister prevention plaster (Blist-O-Ban).
Methods
Questionnaires were completed by 100 male recruits, and the same 100 were entered into a field trial. Due to illness, 2 did not complete the study. Premarch foot condition was documented. Each participant acted as his own control. Foot side and plaster site were randomly selected, and plasters were applied according to a strict protocol. Participants were re-examined for blisters after a 16-km hike with pack, and the condition of the feet was documented. A χ2 test was used to analyze the results.
Results
Ninety-eight volunteers with 101 Blist-O-Ban application sites participated. Twenty-seven participants developed a total of 46 blisters. Heel and toe blisters accounted for more than half of all blisters. None of the bandage application sites developed blisters, and 99 out of 101 bandages remained well adhered to the application sites.
Conclusions
When applied according to strict protocol, the new blister prevention bandage remained well-adhered to application sites and prevented the formation of foot blisters even in humid tropical conditions.
Introduction
Foot blisters are very common in military recruits undergoing basic training. Blisters cause significant discomfort and may lead to loss of training time. Blisters limit a soldier's mobility and, therefore, may be life threatening in times of actual conflict or war. Morbidity is potentially increased as hot, humid, tropical field conditions increase the possibility of cellulitis and sepsis. Foot blisters are caused by friction between footwear and the skin of the foot. 1 We studied the efficacy of a commercially available adhesive bandage in the prevention of blisters in a group of recruits in a tropical setting. Blist-O-Ban (BOB) (SAM Medical, Newport, OR) was chosen, as it has a very low coefficient of friction, 2 thus reducing interface friction forces that might cause blisters. A prior study using BOB 3 was carried out in a temperate climate with moderate humidity where bandages may adhere better than in a tropic environment. To our knowledge, BOB has not been tested in a hot, humid, tropical environment.
Methods
Study Population
The study was performed with permission from Major (Dr) Nicholas Chua, DMO 9 DIV/INF and endorsed by Chief Army Medical Officer Colonel (Dr) Benjamin Seet. One hundred adult Chinese males, aged 18–19 years, were recruited for the trial. Participation was voluntary, and all participants were informed of the survey and study prior to data collection and trial. All were based at the School of Basic Military Training (SBMT) in Pulau Tekong, Singapore. They had completed 7 weeks (70%) of basic military training (BMT) at the time of the study. No participants had any previous experience with BOB prior to the trial. They had all received standard Army instruction on blister prevention strategies (eg, use of foot powder and the 2-sock system). 1
A preliminary survey (Appendix A; available at
A trial side test foot was randomly selected for bandage application. Selection was done by drawing lots out of a bag. There were 50 slips of paper with “left foot” printed on them and 50 slips with “right foot” printed on them. Once the lot was drawn, the selection was noted, and the slip of paper set aside. This allowed each participant to serve as his own control. If the participant had no previous blister or hot spot experience, BOBs were applied to randomly selected sites on the test foot again by drawing lots. However, if any participants were prone to blisters or hot spots in particular areas, BOBs were applied to those injury prone sites on the trial side test foot. Therefore, a single participant could have more than one BOB applied to the test foot. BOB bandages are commercially available in 3 sizes: small, medium, and large. Based on the concept that a larger coverage area would provide greater protection, we elected to limit our study to the use of medium- and large-sized BOBs. Small BOBs specifically designed for use over the toes and interdigital areas were not used in this study. Each foot was then examined and the premarch foot condition documented. Bandage application was performed according to the protocol detailed below.
BOB Application Protocol
BOBs were applied according to the protocol recommended by the manufacturer. The area of bandage application was cleansed with alcohol and allowed to air-dry. A thin layer of liquid adhesive (Mastisol; Ferndale Laboratories Inc, Michigan) was then applied to the skin and allowed to dry till tacky. The Mastisol was applied beyond the perimeter of the BOB “footprint” to ensure bandage edges did not curl up or dislodge during activity. All BOBs were carefully applied to avoid creases. Talcum powder was then sprinkled over the application area to neutralize any Mastisol extending beyond the bandage margins. Neutralizing with talcum powder is critical to prevent adhesion of socks or footwear to the skin or BOB, both of which could increase blistering. In accordance to standard Army instructions for blister prevention, all participants were encouraged to use talcum powder on their feet and employ a 2-sock system; however, this was left to the discretion of the soldier. All participants wore standard issue military socks and boots.
Postmarch Foot Examination
All feet were examined within 1 hour of the end of the march, after the participants had performed their mandatory “cool down” exercises and stretches and rehydrated themselves. The condition of the feet was documented using a survey form and digital photographs. The feet were assessed by 2 teams of 2 researchers each. We defined a blister as an area with vesicle formation; broken skin or fresh blisters that had been deroofed by friction trauma were also considered as blisters. Areas with erythema without vesicle formation were considered as “hot spots.” Researchers were not blinded, as BOBs were not removed prior to postmarch examination. Photographs were reviewed by 2 researchers (SST, KSK), and only those feet with obvious vesicle formation and corroborating data in the postmarch examination form were accepted as having blisters.
Results
Preliminary Survey Results
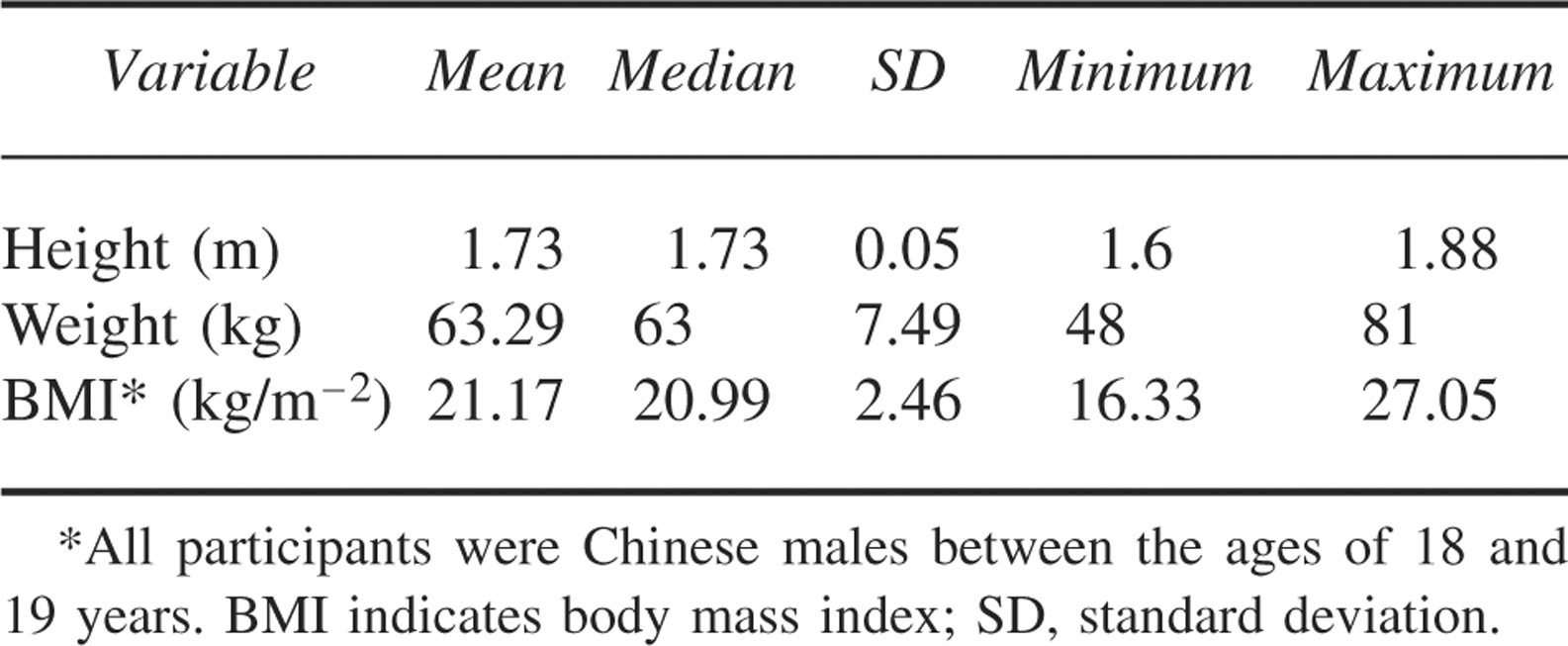
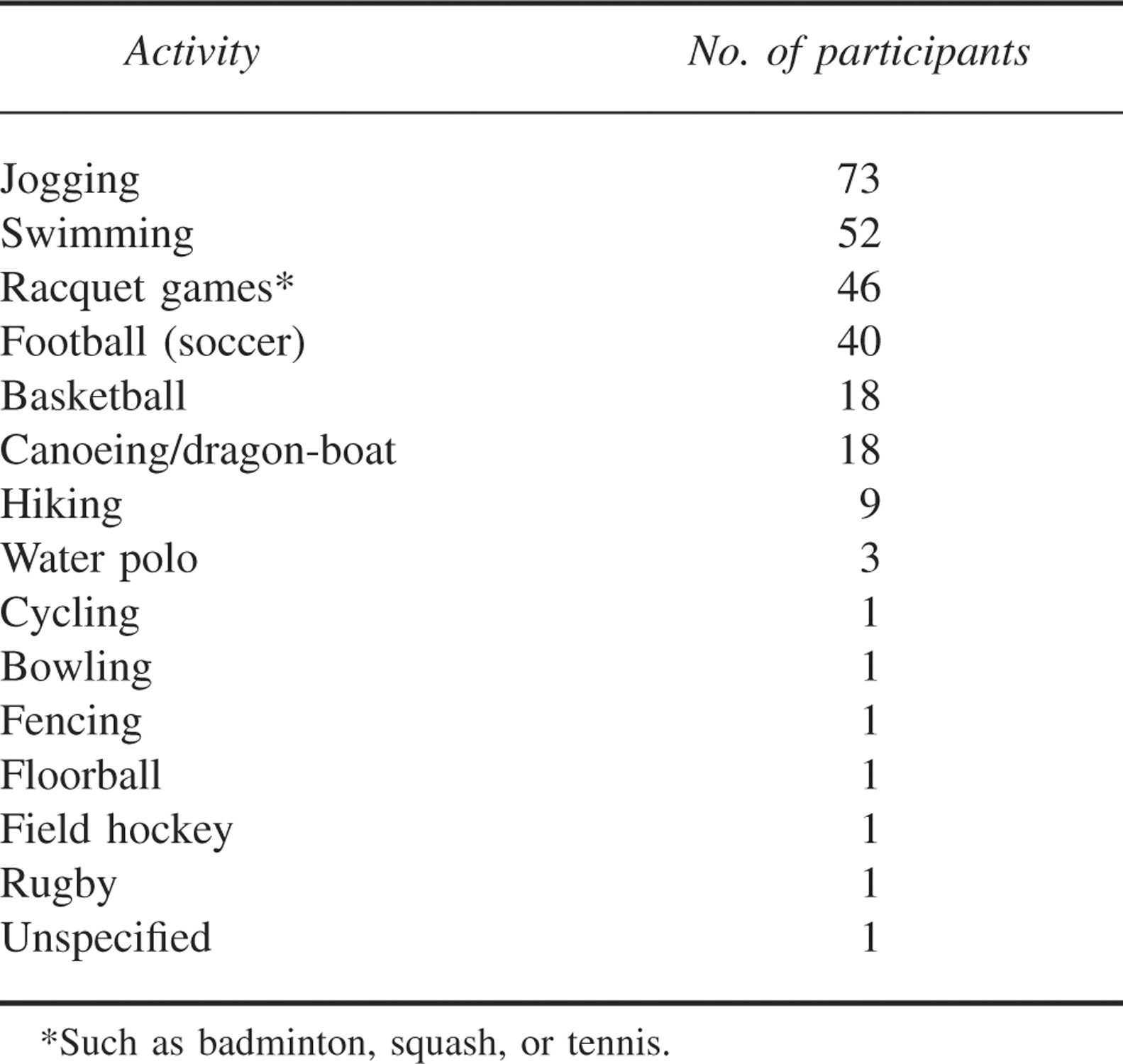
Body mass index (BMI) of the participants ranged from 16.33 to 27.05, with a mean of 21.17 (Table 1). Seventy-one percent of the respondents said they exercised regularly, with 66% exercising 3 times or more per week. The most common activity was jogging (n = 73), followed by football (soccer; n = 40) (Table 2). Only 9 participants said they hiked regularly. Forty-six participants played racquet sports. For water-based sports, 52 participants swam, while 18 either canoed or took part in dragon boat races. Under the miscellaneous category, basketball was most common (n = 18), followed by water polo (n = 3), cycling (n = 3), volleyball (n = 1), floor ball (n = 1), fencing (n = 1), bowling (n = 1), high-jump (n = 1), field hockey (n = 1), and rugby (n = 1). There was 1 unspecified sport in the “other” category.
Demographic data*
Types of physical activity
Ninety-three percent of the participants reported having experienced foot blisters with exercise. Three percent reported they developed foot blisters every time they exercised. Seven recruits said they had no history of foot blisters. Eighty-four percent of the historical foot blisters occurred on the toes, while 45% were reported to have occurred on the heel and sole (equally distributed between these 2 areas). Only 14% of the blisters occurred on the instep. Ten percent of the respondents experienced foot blisters in only 1 location, and 18% reported having blisters over 3 or more locations.
Field Trial Results
Two participants dropped out of the 16-km march field trial for medical reasons unrelated to blisters, leaving 98 study participants. Weather conditions on the day of the trial were cloudy with a light drizzle, hot (air temperature 28–30°C) and humid (70%–80% relative humidity). The trial was conducted during a 16-km hike over easy terrain. Each participant carried a back-pack (weight 18–20 kg).
Sites of BOB Application
There were 98 participants, with 101 BOB application sites. Anatomic location of the BOB application is summarized in Table 3. There was no significant difference with respect to site or side of BOB application (P > 0.05). Heel and toe application sites accounted for 35% of all sites on each foot. Of all the BOBs applied, 1 completely separated from the skin, and 1 was partially displaced. There was no blister formation at either of these sites. All other BOBs remained well-adhered.
Blist-O-Ban application sites*

Blister Formation
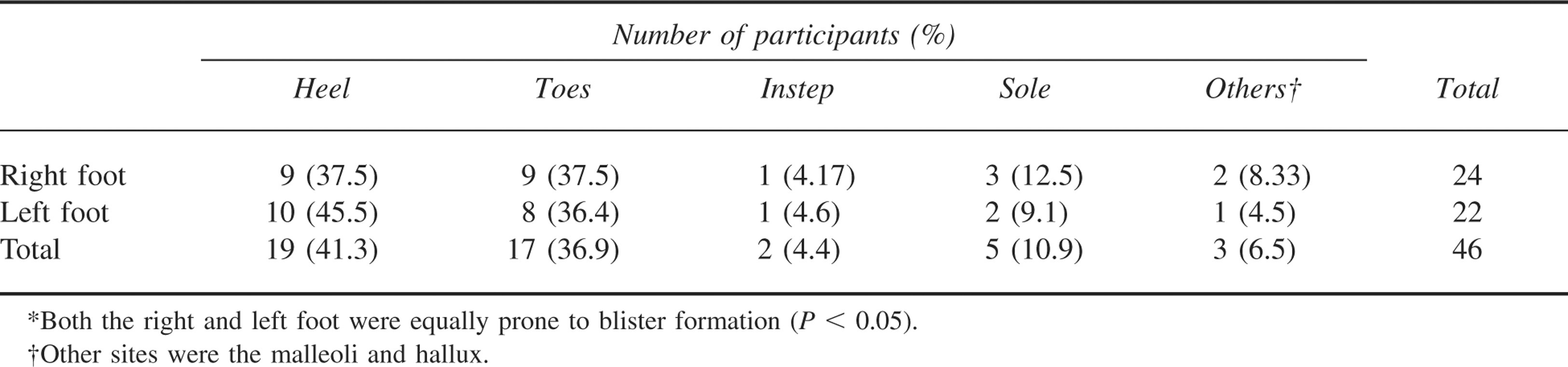
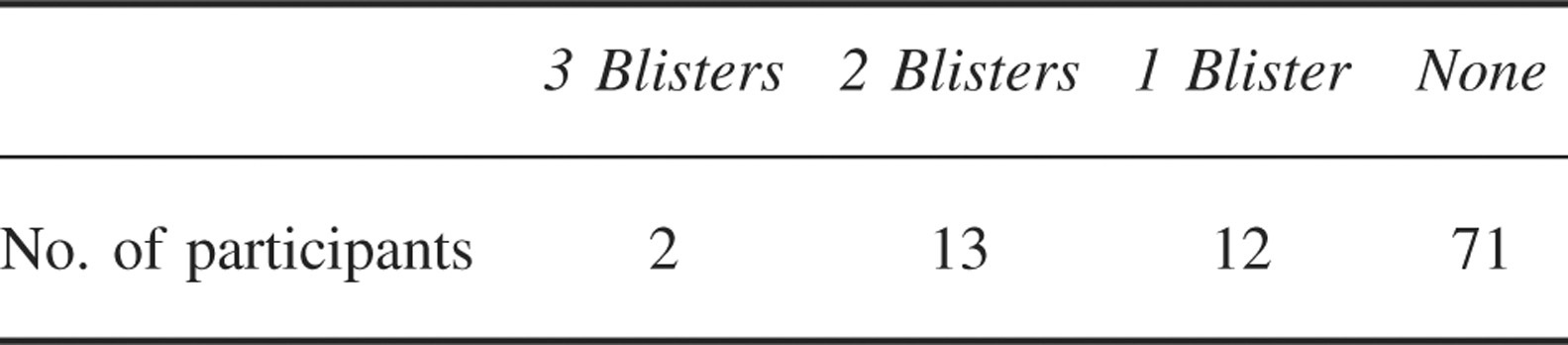
Twenty-seven participants developed a total of 46 blisters during the march (Table 4). The number of blisters per participant is summarized in Table 5. Only 2 participants developed blisters over the instep. An unexpected blister site was located over the inferior aspect of the lateral malleoli. This area corresponded to the creases in the military boots worn by our participants. There were no blisters at BOB-protected sites.
Postmarch blister sites*
Blister formation per participant
Discussion
In a hot, humid environment, there is increased sweating. Moist skin is prone to maceration and blister formation, and the feet are no exception. The use of antiperspirants with emollients has been shown to reduce irritant dermatitis but does not reduce the accumulation of total foot sweat or the incidence or severity of blisters. 4 The most common blister sites in our participants were on the toes (either interdigital or the lateral aspect of the fifth toe) and heels, followed by the sole of the foot over the second metatarsal head. On the right foot, heel and toe blisters accounted for 37.5% each of blisters, and on the left foot, heel and toe blisters accounted for 45.5% and 36.4%, respectively. All blisters occurred over sites not protected by BOBs, suggesting that the BOB effectively reduced friction directly below the application site. The participant with the partially displaced BOB had it applied to the sole, just under the second metatarsal head. He had pre-existing healed blisters but no new blister formation after the trial (Figure). In one participant, the BOB that was applied to the sole came off completely, but there was no blistering caused either by the absence of the plaster or the curled up plaster within his sock. We made no attempt to protect the interdigital areas of toes and lateral aspects of the fifth toes, as we elected not to use small BOBs in our study.
It was our expectation that most blisters occurred over the heel, instep and sole areas—areas better covered by the medium and large BOB. However, slightly over a third of our participants developed blisters over the toes, either on the dorsum of the fifth toe or between the second and third toes, third and fourth toes, and fourth and fifth toes (one participant each). There were at least 5 participants who had either premarch erythema over the dorsum of the fifth toes or developed erythema postmarch, but this did not amount to actual blister formation.
Many strategies have been used to reduce the incidence of blisters, ranging from the use of antiperspirant foot powder4,5 to lubricating barriers, such as petroleum jelly, the 2-sock system, 6 or special adhesive bandages. All the aforementioned strategies attempt to reduce the stress applied to the stratum corneum by reducing the coefficient of friction (CoF). In a laboratory study conducted by Polliack and Scheinberg 2 BOB had a CoF of 0.57 compared to other commercially available products, which had CoFs ranging from 0.69 to 1.54. 2 Using a 2-sock system or thicker socks without making adjustments in footwear size may have the converse effect of actually increasing pressure points (and possible blister formation). Conversely loose boots with foot slippage may also increase frictional forces. 7
Obesity increases the incidence of foot and ankle problems, which may in turn lead to abnormal gait and blister formation. 8 Our study group had BMIs within the normal range. Greater exposure to exercise or training (and therefore increased frictional stress to the areas concerned) over time thickens the skin of hands or feet, reducing the tendency to form blisters. Factors that tend to increase blister formation include foot abnormalities, such as pes planus and hallux valgus, as these create pressure points at the instep and medial aspect of the first metatarsal head, respectively. 9
Blisters cause significant discomfort and downtime for victims. A recent study suggested that military recruits with blisters were 50% more likely to experience an additional training injury. 10 Therefore, blisters should be prevented as much as possible.
Limitations
In the protocol for BOB application, we did not apply talcum powder to corresponding areas on the control foot. This may have confounding effects, as the control foot may not have been as dry. However, in tropical conditions, regardless of the quantity of talcum powder applied, the foot never stays dry.
Researchers were not blinded, as BOBs were not removed prior to postmarch examination. This was a logistics issue, as the participants had to be released for further military duties within 2 hours of the end of the march. We did not have the time to have a researcher remove the BOB, clean the foot, and send the participants for examination and complete documentation within the time allowed for the trial. Premarch feet had pre-existing healed blisters. Postmarch feet showed no new blisters following the trial.
Conclusion
Blist-O-Ban was effective when applied prophylactically before activity. Several BOBs may be applied on the same foot if there is more than 1 at-risk area. Use of Mastisol after proper degreasing enabled the BOB to remain on the foot to prevent blisters throughout the 5-hour activity in hot and humid conditions. Interdigital blisters may have been prevented if small BOBs had been applied. Importantly, proper footwear sizes and blister reduction strategies should be made known and available to persons involved in vigorous activities, such as military training, marching, or long-distance races or hikes.
Footnotes
Acknowledgments
The corresponding author is also Director of Wilderness First Aid (WFA), Singapore, which teaches wilderness first aid. WFA Singapore is a re-seller of first aid products, which include but are not limited to Blist-O-Ban. Blist-O-Ban was purchased from SAM Medical at bulk purchase price for this study.