
Abstract
White scorpion (Hottentotta tamulus) stings are an emerging health hazard in northern Sri Lanka and are increasingly recognized particularly during the last decade. The stings are usually harmless; however, fatal cardiovascular sequelae ensues following severe envenomation. It is often difficult to identify this miniature creature and its site of sting due to its nature of habitat and nonspecific local symptoms that develop after the sting. Here, we report a patient who had developed a blistering skin lesion soon after the sting which is not reported in the literature to date by the sting of this particular species. Recognizing it would help the clinicians of this subcontinent to consider scorpion sting as a differential diagnosis for the above presentation in the future.
Introduction
Sri Lanka is a tropical island situated close to the southern tip of India. There are about 1750 species of scorpions described, which belong to 13 families described in the world. Sri Lanka is a home for 18 scorpions under 3 families. Mesobuthus tamulus (Indian red scorpion) and Heterometrus swammerdami are species of scorpion of clinical importance. While all scorpions are venomous, only one species native to Sri Lanka is fatal to humans. 1 White scorpion (Hottentotta tamulus) of Buthidae family, a fat-tailed scorpion, is the only deadly venomous scorpion in Sri Lanka. It is usually known as “red scorpion” in the Indian subcontinent and was noted in Sri Lanka in 1990s said to be after the arrival of Indian Peace Keeping Force in 1987 from India. There were cases reported with Hottentotta tamulus stings since the end of civil war in 2009 with 22 confirmed hospital admissions in the calendar year 2013. 1 These bites are generally harmless and vary from localized inflammation to wide range of autonomic dysfunctions. However, they sometimes lead to serious clinical sequelae such as acute myocardial infarction, acute pulmonary edema, cardiogenic shock, and death. 2 Skin blisters are rarely observed and were not reported in the literature. Here, we report a cutaneous blistering lesion following white scorpion bite in Sri Lankan man.
Case report
A 30-year-old man was admitted with painful blistering skin lesion on the dorsum of the hand after a white scorpion (Hottentotta tamulus) sting, 2 h prior to the admission to hospital. On examination, he was hemodynamically stable with a pulse rate of 84 per minute and blood pressure of 110/80 mm Hg. He did not have any autonomic symptoms. His lungs were clear on auscultation. Oxygen saturation was 100% on ambient room air. A blistering skin lesion (Figure 1(a)) appeared at the site of sting after the admission. He did not apply anything as a home remedy or first-aid measure. The white scorpion brought by the patient is shown in Figure 1(b). He was treated with oral prazosin hydrochloride 0.5 mg three hourly. Paracetamol was used for pain relief, and ice pack topical anesthetic agent was applied locally to the blistering skin lesion. He was closely monitored for possible systemic complications. However, he has not developed pulmonary edema, hypertensive crisis, and myocardial ischemia. On the seventh day of admission, his blistering skin lesion was subsided spontaneously.
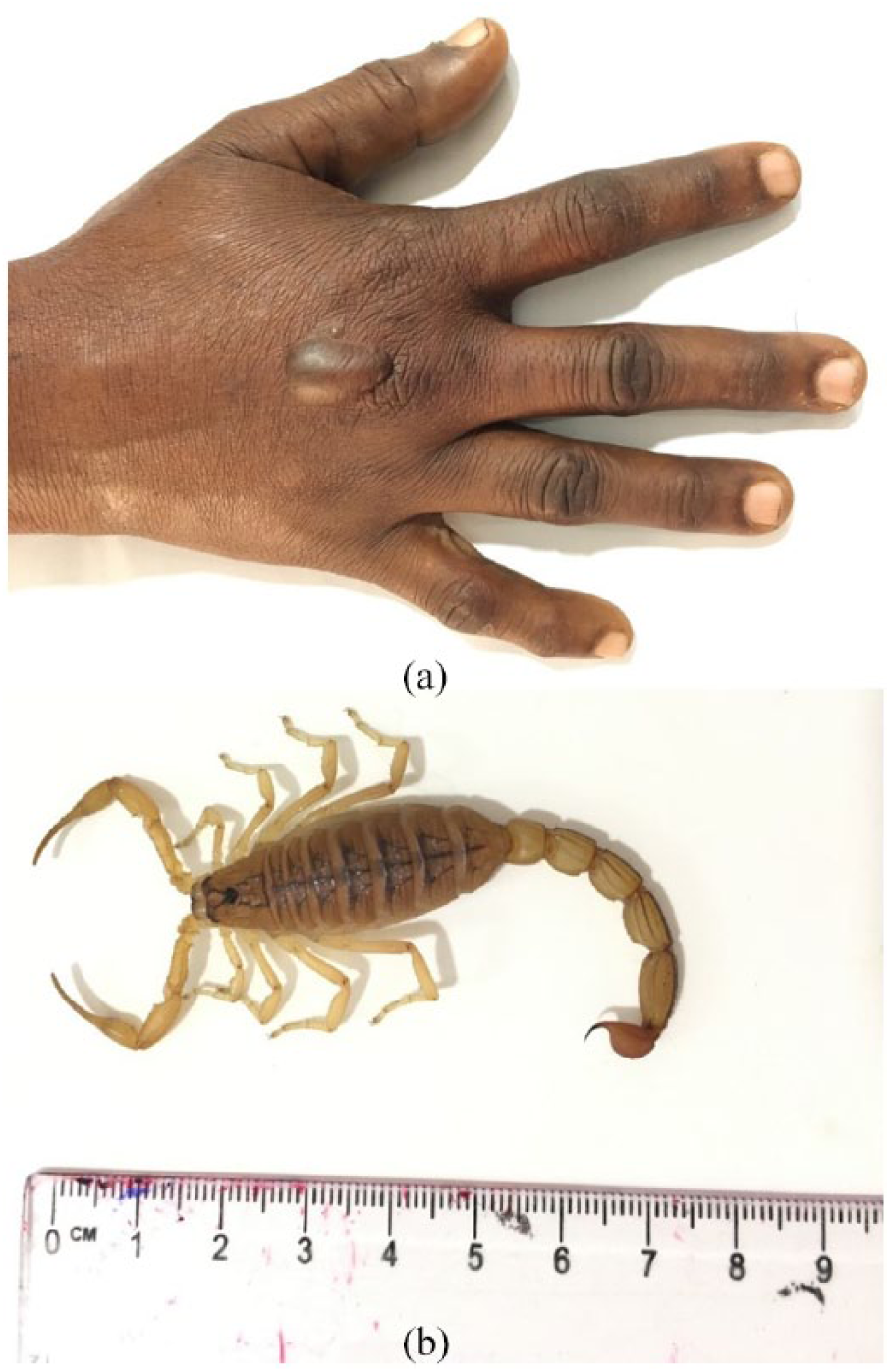
(a) A blistering skin lesion appeared at the site of sting following white scorpion (Hottentotta tamulus) bite and (b) the morphological appearance of white scorpion (Hottentotta tamulus).
Discussion
Hottentotta tamulus stings observed in Northern Province of Sri Lanka were usually associated with overactivity of autonomic nervous system such as changes in pulse rate and blood pressure, sweating, diaphoresis, pulmonary edema, and rarely leading to acute coronary events. 3 The ingredients of venom of Hottentotta tamulus include several low-molecular-weight, water-soluble, antigenic complex mixture of neurotoxin, cardiotoxin, nephrotoxin, hemolysins, histamine, and other chemicals. 4 These substances inhibit protease, angiotensinase, succinate dehydrogenase, ribonuclease, and 5-nucleotidase which can produce a synergic effect in the ion channels called “autonomic storm” that reflects the stimulation of the autonomic system. 5
The venom produces clinical manifestation range from minor local tenderness to multisystem failure which occurs within a few minutes after the sting and usually progress to a maximum severity within 5 h and lasts for 24–72 h. The signs of the envenomation are determined by the scorpion species, venom composition, and the victim’s physiological reaction to the venom. The most important clinical effects of envenomation are neuromuscular, neuroautonomic, or local tissue effects. The primary targets of scorpion venom are voltage-dependent ion channels, of which sodium channels are the best studied. 5 Autonomic excitation leads to cardiopulmonary effects observed after some scorpion envenomations. 3 Acute coronary syndrome, acute pulmonary edema, hypertensive crisis, and cardiogenic shock are life-threatening complications of victims leading to mortality.
Local tissue effects vary among species. Itching, edema, and ecchymoses with burning pain are commonly observed local manifestations. 6 Local manifestation of a sting may be minimal in 50% of cases of neurotoxic scorpion stings. The cutaneous blisters or tissue necrosis are rarely heard of scorpion stings of Indian subcontinent. A sharp burning pain sensation at the sting site, followed by pruritus, erythema, local tissue swelling, and ascending hyperesthesia, may be reported. A macule or papule appears initially at the sting site, occurring within the few hours of sting with varying size depending on the severity of envenomation which progresses to a purpuric plaque that will necrose and ulcerate. These are secondary to venom activation of kinins and slow-releasing substances. 4 However, blistering skin manifestation was not reported in literature to date from this part of the world and skin blister could be added to the array of clinical manifestation of white scorpion sting.
The immediate application of ice bag rapidly causes vasoconstriction and reduces pain and would slow down the absorption of venom. 7 The topical anesthetic agent is more effective than opiates and ice application. Prompt treatment with prazosin hydrochloride could significantly reduce the life-threatening complications of scorpion stings. 8
Conclusion
The white scorpion toxin contains polypeptides which cause sympathetic and parasympathetic stimulation leading to signs and symptoms ranging from localized to systemic manifestation which are described in literature. However, a blistering skin manifestation was not reported in literature and skin blister could be added to an array of clinical manifestations of white scorpion sting.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.