Abstract
Objective
To quantify awareness of altitude sickness in a sample of trekkers in Nepal and identify strategies for increasing knowledge in that population.
Methods
Sixty-five high-altitude trekkers were surveyed. Demographic data were gathered. Respondents were asked about their experience in high-altitude environments, and they answered clinical-vignette questions designed to test their abilities to recognize and identify treatments for common symptoms of altitude sickness. An altitude-awareness score was generated by tabulating correct answers to questions. Scores were correlated with demographic data.
Results
Respondents who scored highest (
Conclusion
This study suggests that a large population of at-risk high-altitude travelers may be relatively naïve to the dangers of altitude sickness. Overall, respondents were interested in learning more about altitude sickness. Physicians and the Internet are the most attractive sources of information for this population.
Introduction
Altitude sickness is a general term describing a heterogeneous group of disorders, ranging in severity from headache or disordered sleep to life-threatening pulmonary or cerebral edema. It is a common condition among travelers to altitude and may occur at heights as low as 1500 m (4921 feet). 1 Its incidence at moderate altitudes in the American West has been estimated at 18% to 66%,2,3 whereas in one series, 47% of trekkers flying to Lukla before ascending to Mt Everest base camp in the Khumbu region of Nepal (altitude of approximately 5200 m) were affected. 4
The recent upsurge in outdoor recreation and adventure travel has exposed an unprecedented number of individuals each year to the dangers of high-altitude sickness. Millions of persons recreate annually in the American West, and popular destinations in Asia, South America, and Africa receive hundreds of thousands of visitors each year. Travelers to such areas routinely exceed altitudes of 4000 m (13 124 feet) and in some cases can ascend to over 5000 m (16 404 feet).
Wider access to high-altitude destinations has led to a change in the characteristics of the travelers visiting them. 5 No longer are the mountains the sole provenance of those with experience and expertise. Travelers to such areas today are frequently young, poorly equipped, and largely naïve to the dangers to which they expose themselves.
This study quantifies the extent of experience with and interest in altitude-related sickness among a sample of trekkers in Nepal. Questions were designed to identify how physicians might best educate such trekkers in order to limit mortality and morbidity caused by altitude sickness.
Methods
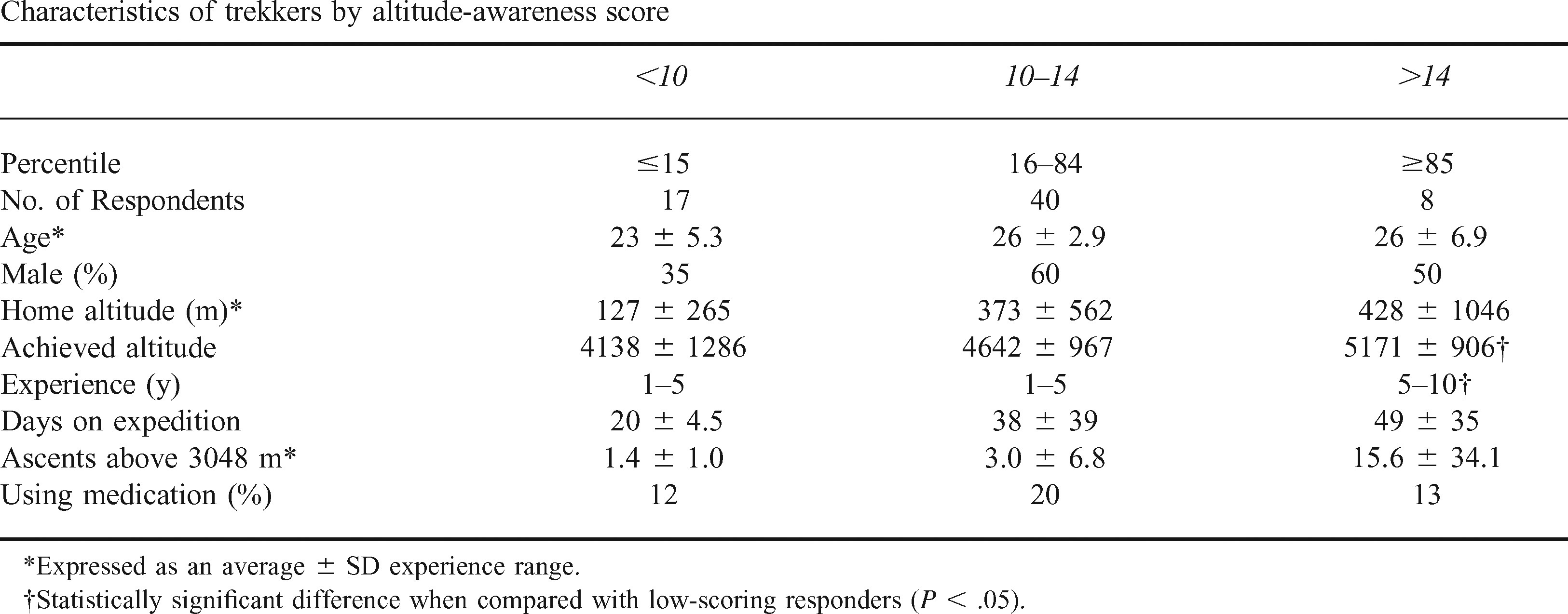
Characteristics of trekkers by altitude-awareness score
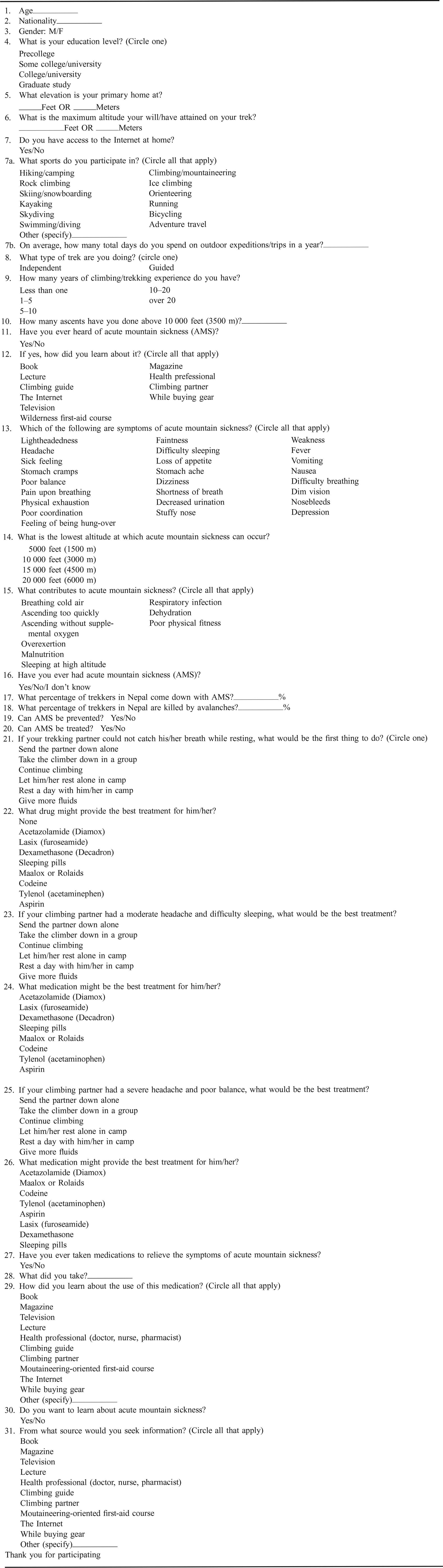
A convenience sample of trekkers was approached in April 1999 while on the trail of the Annapurna trek, a popular route in western Nepal. Data were not collected regarding the number of days respondents had been on the trail. Trekkers were offered the chance to participate in the study, which was described as “a test of knowledge of altitude sicknesses.” Participants were excluded if they refused to take part or if they could not speak and read English. A written survey instrument consisting of a combination of multiple-choice and fill-in questions was administered to eligible subjects (Appendix). Data on response rate were not collected.
The survey identified demographic data such as age, nationality, and level of schooling. Data were collected about the altitude the respondents attained or would attain on their current trek. They answered questions about their extent of experience in the outdoors and with extremes of altitude.
Respondents identified symptoms of altitude sickness in a series of multiple-choice questions. They picked actions and medications appropriate to a number of scenarios featuring altitude sickness. An “Altitude-Awareness Score” was computed based on their correct answers (maximum score = 20). Respondents were asked to estimate their risk of contracting altitude sickness or of dying in an avalanche while in Nepal. Finally, they were asked whether they were interested in learning more about altitude sickness and, if so, where they would seek such information.
Results were collated and analyzed by SAS software (SAS Inc, Cary, NC) upon our return to the United States.
Results
Sixty-five trekkers responded to our survey. Respondents represented 14 countries and were an average age of 25 years (SD ± 4.52). Seventy-one percent (
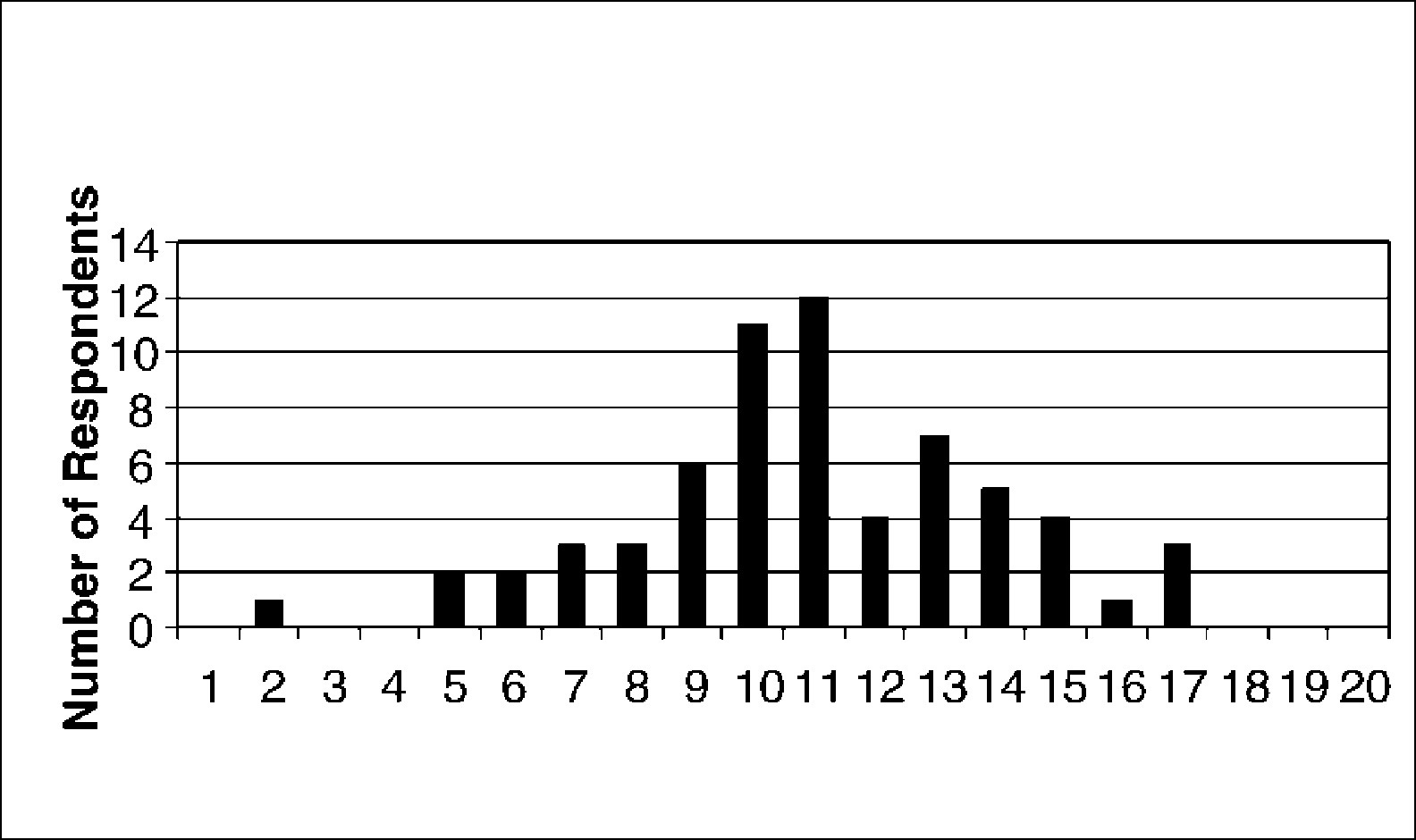
Frequency distribution of altitude attained among survey respondents.
Respondents had varied understandings of altitude sickness. Most (78%,
Other answers were categorized regarding the altitude-awareness score. To give the study the greatest practical significance, we sought to identify differences that might exist between very highly knowledgeable respondents and others who were just “below average.” To accomplish this, highly knowledgeable respondents were defined as those scoring in the top 15%, whereas less highly informed respondents were defined as those with scores in the bottom 25% (Table). Respondents with higher awareness scores tended to be older men who had more ascents above 3048 m (10 000 feet). High scorers had significantly more years of experience, averaging 5 to 10 years (
In general, respondents’ risk assessment was fair. Their average estimate of their chance of becoming ill with acute mountain sickness was 26% (SD ± 18.48), correlating well with a real risk of 23% to 47%. 2 Respondents rated the danger of dying in an avalanche at 2.8% (SD ± 2.7) as opposed to a real risk of just 0.0005% (5 in 1 million).
Respondents within the sample showed great interest in learning more about altitude sickness, with 73% (
Discussion
The current worldwide popularity of outdoor recreation has put increasing numbers of persons at risk for the mortality and morbidity associated with high-altitude sickness. Although the literature has clearly delineated the dangers that extreme altitudes confer, 6 few laypersons may have benefited from this information. In particular, many participants in high-altitude recreation, including trekkers, skiers, and mountaineers, may be relatively naïve to the dangers to which they expose themselves. 7
The syndrome of altitude sickness is particularly amenable to a program of primary prevention. Although treatments for individuals with altitude sickness are effective, in many cases the remoteness of the individuals leaves them without care. The most advanced forms of mountain sickness, high-altitude pulmonary edema and high-altitude cerebral edema, are difficult to treat and often are deadly. 8 Altitude sickness is easily preventable. 9 Medications such as Diamox (acetazolamide) and nifedipine and careful acclimatization can prevent altitude sickness in all but the most extreme circumstances.10,11
This study, based on a small sample of trekkers, suggests that even basic skills of recognition and treatment of altitude sickness are absent in an at-risk population. This was true despite our sample's generally high level of education. Respondents were engaged in treks to the greatest extremes of altitude in the world, and most were aware of the existence of altitude sickness. Despite these facts, respondents underestimated their risk of falling ill by up to 50% and were unprepared to recognize or treat their symptoms if they did. Interestingly, this same population tended to overestimate their risk of dying in an avalanche (on average, a 5000-fold overestimation.) This may reflect the media's disproportionate coverage of avalanche deaths.
The population surveyed was interested in educating themselves more about the dangers of altitude sickness. This study suggests that a large population of outdoor enthusiasts would seek out and benefit from education about the dangers of altitude sickness. Education programs might decrease the mortality and morbidity associated with acute mountain sickness. 12 Such programs could be made available on the Internet or distributed through the offices of health care providers. A motivated and educated patient population such as the one sampled here might be able to make good use of resources that become available to them.
This study is limited by its small number of respondents. A larger study could more fully characterize the levels of awareness in a population of trekkers. Respondents were not asked about previous medical training, an important potential cofounder. This sample is also limited by the country in which it was taken. One does not need to demonstrate aptitude in outdoor skills to buy a trekking permit in Nepal, and no informational literature is provided to educate trekkers. Overall awareness might be greater if a population were sampled in a country that made tourist education a higher priority.
In addition, establishing the validity of a new survey is always difficult, and we did not explicitly test that in our study. However, respondents with high-altitude awareness scores tended to have greater experience in mountaineering. Conversely, younger and more inexperienced responders tended to have lower scores, lending the suggestion of validity to our measuring instrument.
Further work must also be done in effecting and measuring outcomes. A program focused on educating travelers to the dangers of altitude sickness could be effective in improving knowledge. 13 Increased awareness might also reduce mortality and morbidity associated with altitude sickness. Future interventional studies should focus on such topics.
Each year the press spotlights a daring rescue in which ill travelers are plucked from peril on some remote mountainside. Although such episodes make for appealing news copy, they are expensive and dangerous. Altitude-related sicknesses comprise only a small proportion of the risks that beset travelers, but they are prevalent and potentially fatal. It is time for physicians to educate their patients to the dangers associated with the extremes of altitude.
Footnotes
Appendix
The questionnaire is part of a medical study examining trekkers and acute mountain sickness (AMS). Responses are strictly confidential, and your time in answering this survey will hopefully result in minimizing the dangers of mountaineering. Thank you for your time.