
Abstract
High altitude cerebral edema (HACE) is a life-threatening condition that can affect people who ascend to altitudes above 2500 m. Altered mental status and the presence of ataxia distinguishes HACE from acute mountain sickness (AMS). We describe a patient with subtle cognitive dysfunction, likely due to HACE that had not fully resolved. When he initially presented, the patient appeared to have normal mental status and was not ataxic. The diagnosis of HACE was missed initially but was made when further history became available. Cognitive dysfunction was then diagnosed based on abnormal performance of a clock drawing test. A formal mental status examination, using a clock drawing test, may be helpful in assessing whether a patient at high altitude with apparently normal mental status and with normal gait has HACE.
Keywords
Introduction
High altitude cerebral edema (HACE) and high altitude pulmonary edema (HAPE) are life-threatening conditions that can affect people who ascend to altitudes above 2500 m. 1 Altered mental status and the presence of ataxia distinguishes HACE from acute mountain sickness (AMS). 2 Patients with AMS or HAPE may be able to continue ascent after treatment, but patients with HACE are advised to descend.
We describe a patient with subtle cognitive dysfunction, likely due to HACE that had not fully resolved. Because the patient had neither altered consciousness nor ataxia when he first presented, the diagnosis was initially missed. The diagnosis of HACE was made only after additional history was obtained from the patient’s trekking partner. Continuing cognitive dysfunction was confirmed by the patient’s inability to complete a clock drawing test. We share this case because we believe that drawing a clock is a simple test that could be used when assessing patients with high altitude illness.
Description of the Case
A fit 49-year-old man consulted one of the authors (I.Q.) at the Himalayan Rescue Association (HRA) clinic in Manang at 3540 m on the Annapurna trekking circuit in the Nepal Himalayas. The day before he presented, he reached Thorong Phedi where he spent the night at an altitude of 4550 m. He planned on waking early the next morning to cross the Thorong La (Thorong Pass), 5416 m. On arrival at Thorong Phedi he developed a slight headache. He woke, as planned, at 3:00
Twelve hours later, at 3:00
At Manang (3540 m) normal resting Sp
At 5:00
At 8:00
As before, the patient was talking normally. He still had normal tandem gait. He was able to count backwards from 20 to 1. When asked to draw a clock face he demonstrated difficulties. His first attempt was a tiny circle, despite having been asked to use the whole sheet of paper. On the second attempt, he started the numbers with 1 in the correct position and managed to reach 11, where 7 o’clock should have been. He asked whether he should draw a 12- or 24-hour clock. After being told to draw a standard 12-hour clock face, he continued, skipped the number 12, added the number 13, and continued to 22 before giving up (Figure 1).
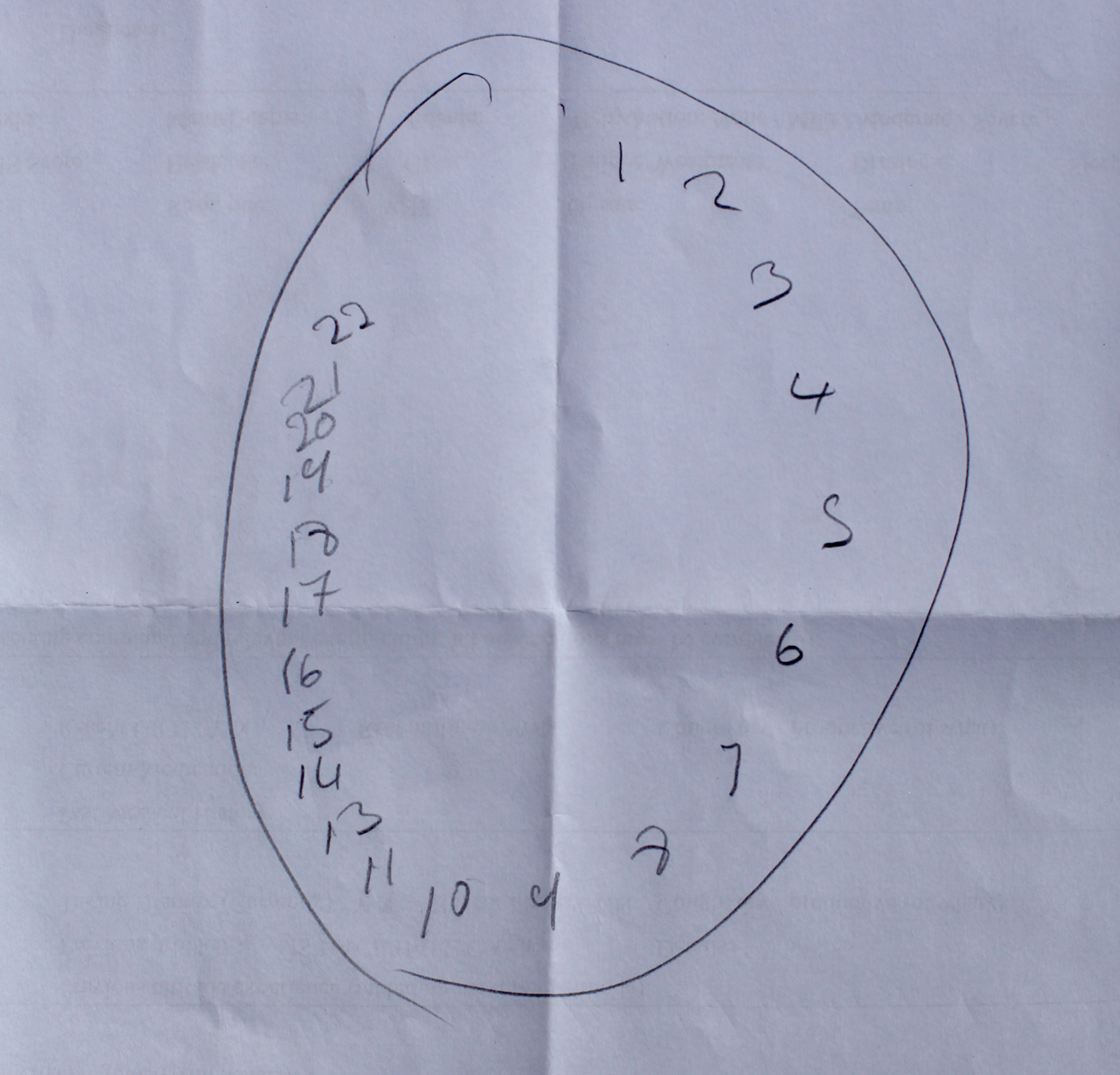
Abnormal clock face drawn by the patient on day 1.
Based on the new information and the abnormal clock drawing test, the patient was diagnosed with HACE that had not completely resolved. He was treated with oral dexamethasone 8 mg and was observed in the clinic overnight, on supplemental oxygen. At 6:45
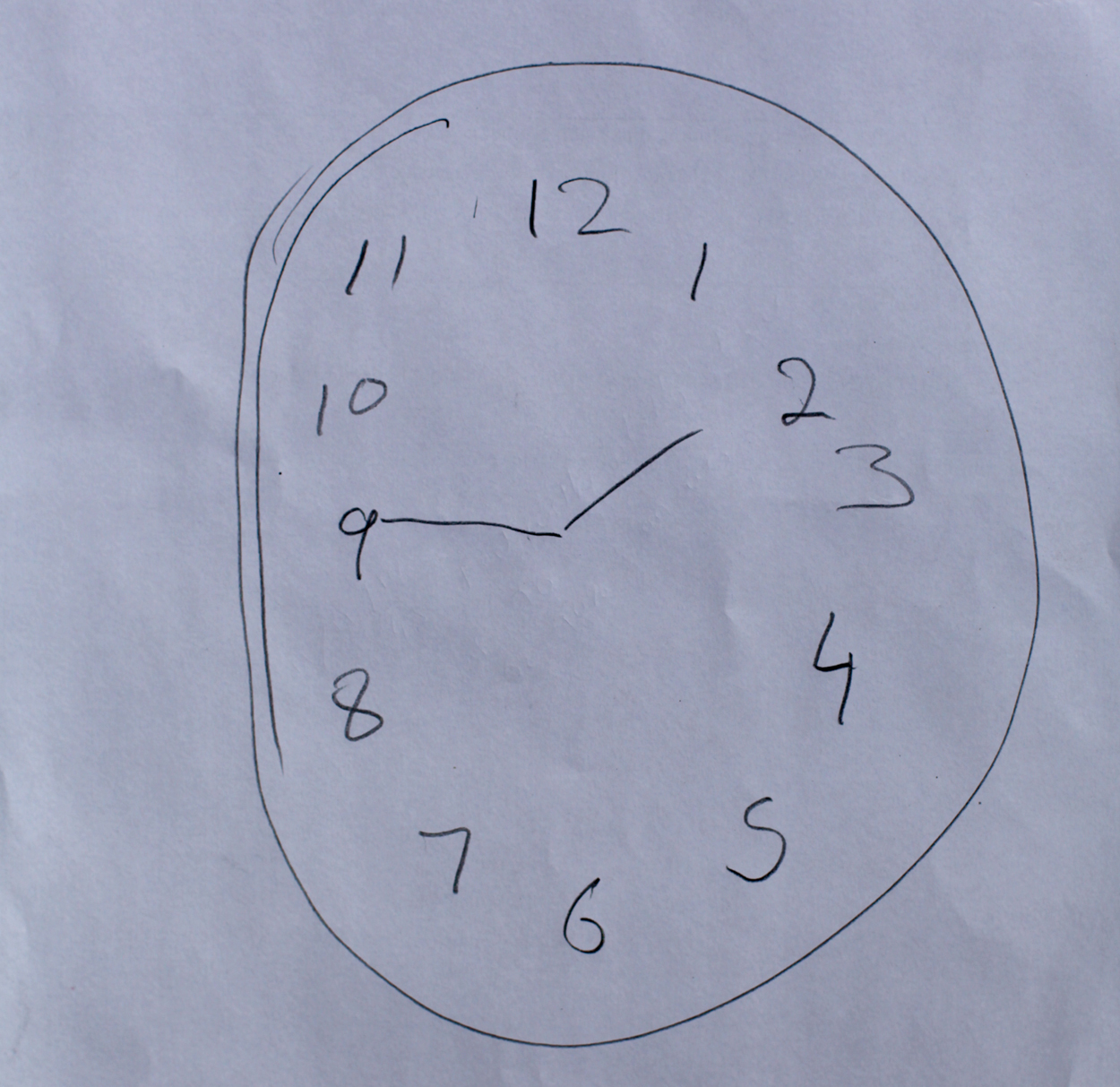
Normal clock face drawn by the patient on day 2.
Although the patient was keen to continue his trek back up to the Thorong La Pass, it seemed safer to evacuate him by helicopter than to encourage him to continue up or down, on foot or on horseback. He spent 1 night in the hospital in Kathmandu. He was discharged without imaging of the brain. He felt tired and unwell for another day or 2 before feeling completely recovered.
Discussion
The patient presented feeling generally unwell, after having had a headache. This presentation suggested residual symptoms of AMS. His oxygen saturation was normal for the altitude, but he desaturated on exertion, suggesting a diagnosis of HAPE. Consistent with practice previously described at an HRA clinic, he was treated for HAPE with multiple vasodilators. 3 In response to previously reported cases, the HRA has since issued guidelines for treatment of HAPE that call for use of only a single vasodilator and that recommend against use of multiple vasodilators.
When we first assessed the patient we did not elicit the history of stumbling gait and altered behavior. Informal assessment of mental status during the initial evaluation combined with the observation of normal tandem gait led to the conclusion that the patient did not have HACE. Five hours after the initial presentation, the patient’s trekking partner gave new information that strongly suggested a diagnosis of HACE. On further assessment, the patient was able to count backwards but was unable to draw a clock face. Ten hours later, after treatment for HACE, he was able to draw a normal clock face.
The differential diagnosis of headache at high altitude associated with a reversible neurologic deficit included seizure, migraine equivalent, transient ischemic attack, hypoxic encephalopathy, and HACE. The clinical symptoms were atypical for seizure or migraine equivalent. Cerebral hypoxia seemed unlikely because his resting Sp
Clock drawing is usually used as a screening tool for cognitive dysfunction in dementia. Its use has also been described in patients with hepatic encephalopathy and traumatic brain injury. 4 We are not aware of previous use of a clock drawing test in patients with HACE. The brain regions used in clock drawing have been studied mainly in patients with dementia. Multiple cortical and subcortical areas and their connections are involved. The abnormal clock drawing test was evidence of cognitive dysfunction that had previously been missed. The patient’s abnormal clock drawing indicates spatial planning deficits, perseveration, and conceptual deficits. 4
This case was a near miss because the initial assessment did not elicit subtle signs of cognitive dysfunction. The patient did not seem confused, but no formal attempt was made initially to assess his mental status. Had the trekking partner not provided additional information, there would have been no further testing of cognitive function.
Patients treated for AMS or HAPE can safely resume ascent soon after recovering. Re-ascent in patients with HACE is not recommended until the patient is completely asymptomatic and is no longer taking dexamethasone. 1 Because dexamethasone has a long duration of action, re-ascent the following morning would have been ill-advised. Had the patient ascended the morning after being treated for HACE, as he was keen to do, he would have been at risk of redeveloping HACE with potentially fatal consequences. We believe that if a formal cognitive test had been used in the initial assessment, the results would have been abnormal and the diagnosis of HACE would have been considered.
The clock drawing test is easy to administer, even in an austere environment. Although clock drawing has not been studied for the diagnosis of HACE, a formal mental status examination, using a clock drawing test, may be helpful in assessing whether a patient at high altitude with apparently normal mental status and with normal gait has HACE.
Footnotes
Acknowledgments
We would like to thank the patient for allowing us to present this case, the volunteers and staff at the HRA Manang Clinic (Tracy Quigley, RGN; Carolyn Kelly-Smith, MD; Thaneshwar Bhandari; and Indira Ojha) for their assistance in caring for the patient, and Dr. Buddha Basnyat, Medical Director of the HRA, for his encouragement in publishing this case report. The patient was seen while Dr. Ian Quigley was a volunteer at the HRA Manang Clinic.