
Abstract
A 16-year-old girl was seriously stung on her abdomen by a jellyfish as she jumped on her small surfboard. She and her mother identified the animal from photographs as Chrysaora fuscescens. Within several minutes the girl developed a massive abdominal cutaneous eruption composed of hundreds of punctuate erythematous papules and macules, which persisted for 5 to 7 days. Persistent urinary incontinence and biliary dyskinesia appeared over the following night. It is theorized that a systemic uptake of venom occurred percutaneously after contact of the jellyfish tentacles with her abdominal skin. The result was an injury to the urinary and biliary bladders. This is the first case report of such sequellae after topical contact with a marine animal. The causal relationship of these abnormalities with the sting is suggested by their temporal association. The gallbladder disorder required surgical intervention, but spontaneous resolution of the urinary bladder dysfunction occurred within 20 months.
Introduction
Venoms from several different species of jellyfish induce immediate and delayed symptoms 1 that can vary in duration and affect several different organs. Serious internal lesions of muscles, nerves, and the heart can result from significant external stings because of toxin uptake from the venom-coated threads that penetrate the skin. These tissues are particularly vulnerable to the mixture of proteins and polypeptides contained in the venoms. The mechanism of action of the venoms’ toxins on nerves or muscle includes interference with ion transfer, suppression of action potentials, and membrane pore production. 2 –4 In the case reported below, persistent urinary incontinence and biliary dyskinesia followed a widespread abdominal sting by a jellyfish.
Case Report
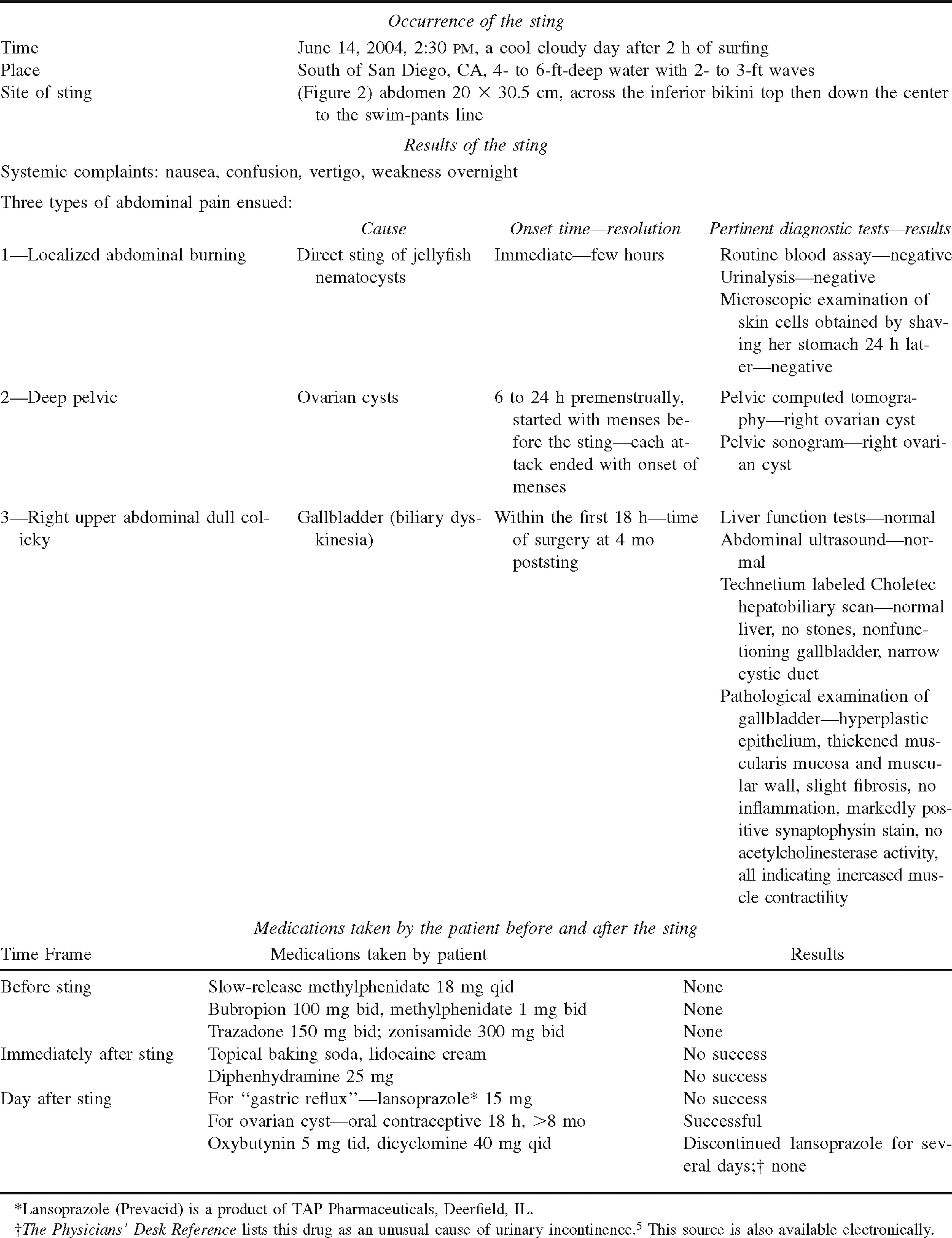
A detailed summary of this patient's illness is presented in Table 1. A 16-year-old girl who had no allergies and was healthy except for Asperger syndrome (a mild autism with temporal lobe epilepsy, bipolar mood swings, and attention deficit disorders) jumped on a small surfboard, only to be stung by a jellyfish. At 2:30
Clinical characteristics of the patient and the sting
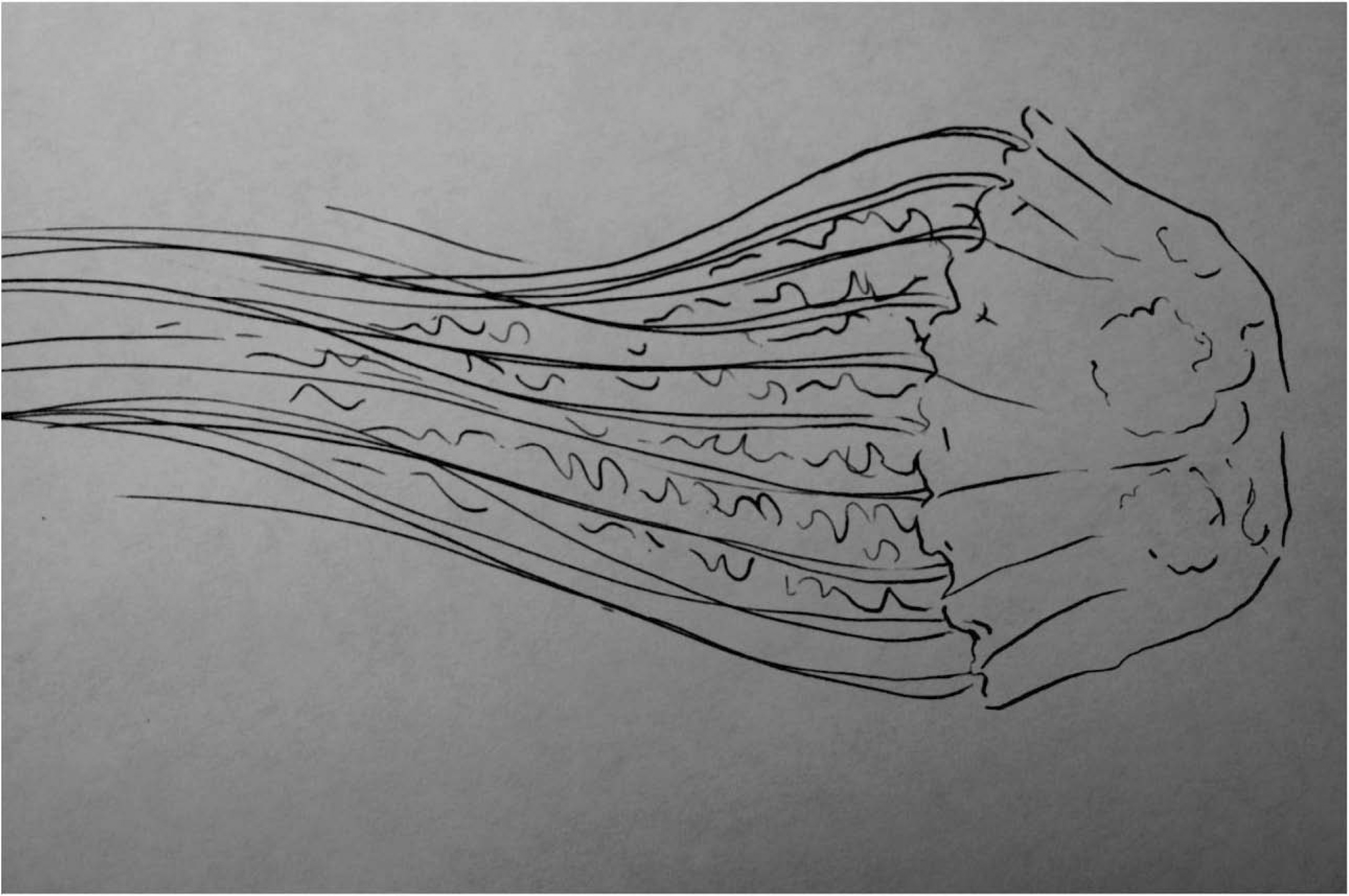
Line drawing of Chrysaora fuscescens medusa. The bell diameter is as large as 30 to 40 cm with 24 tentacles hanging from its edge in groups of 3.

Diagram of the extent of the rash. Figure drawn by the patient.
The next morning the patient began to eat despite a newly appearing deep right upper quadrant epigastric burning with cramping. In the hotel, her mother administered lansoprazole 15 mg orally, without effect. Within a few hours the patient observed that her right upper abdominal pain was exacerbated with eating. It persisted as she and her mother returned inland to their Arizona home. The patient's cutaneous local burning spontaneously subsided by afternoon, though the dermatitis persisted several more days. The mother attributed this rash to the medusa's sting.
Early in the day after the sting, the patient experienced urinary incontinence, which she had never experienced before. This event required protective diapers. A day later, her urologist administered oxybutynin and dicyclomine, without benefit (Table 1). The patient's history and an unobstructed sphincter indicated by normal urological examination suggested the diagnosis of inhibited detrussor contractions with urge incontinence.
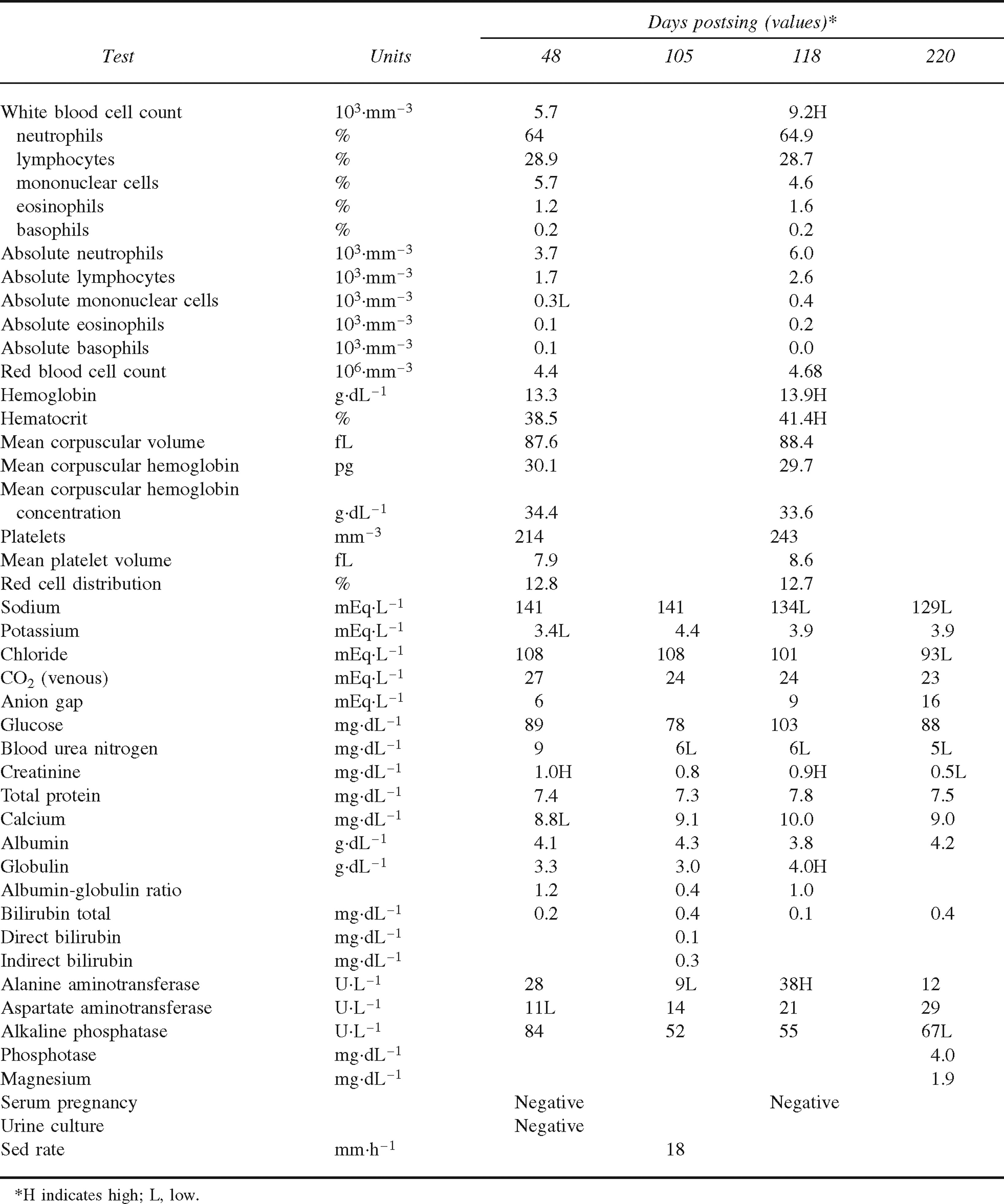
The patient required short hospitalization during the next few weeks, and specialists in gastroenterology, urology, neurology, and psychiatry made multiple visits. She had normal liver function tests, blood surveys, and urinalyses throughout her illness (Table 2). Her gastroenterologist ordered an abdominal ultrasound examination and a technetium labeled Choletec hepatobiliary scan, which were interpreted as a normal liver, a nonfunctioning gallbladder, and a narrow cystic duct but no gallstones.
Routine blood and urine tests
Another complication was the onset of premenstrual deep pelvic pain, which began with the patient's menses 2 weeks before the sting. These cramping pains, which she could differentiate, lasted until her menstrual flow. Pelvic computed tomography and a sonogram ordered by the gynecologist demonstrated a right adnexal ovarian cyst. These cramps were successfully treated with oral contraceptives (Table 1) and were thought to be unrelated to her sting.
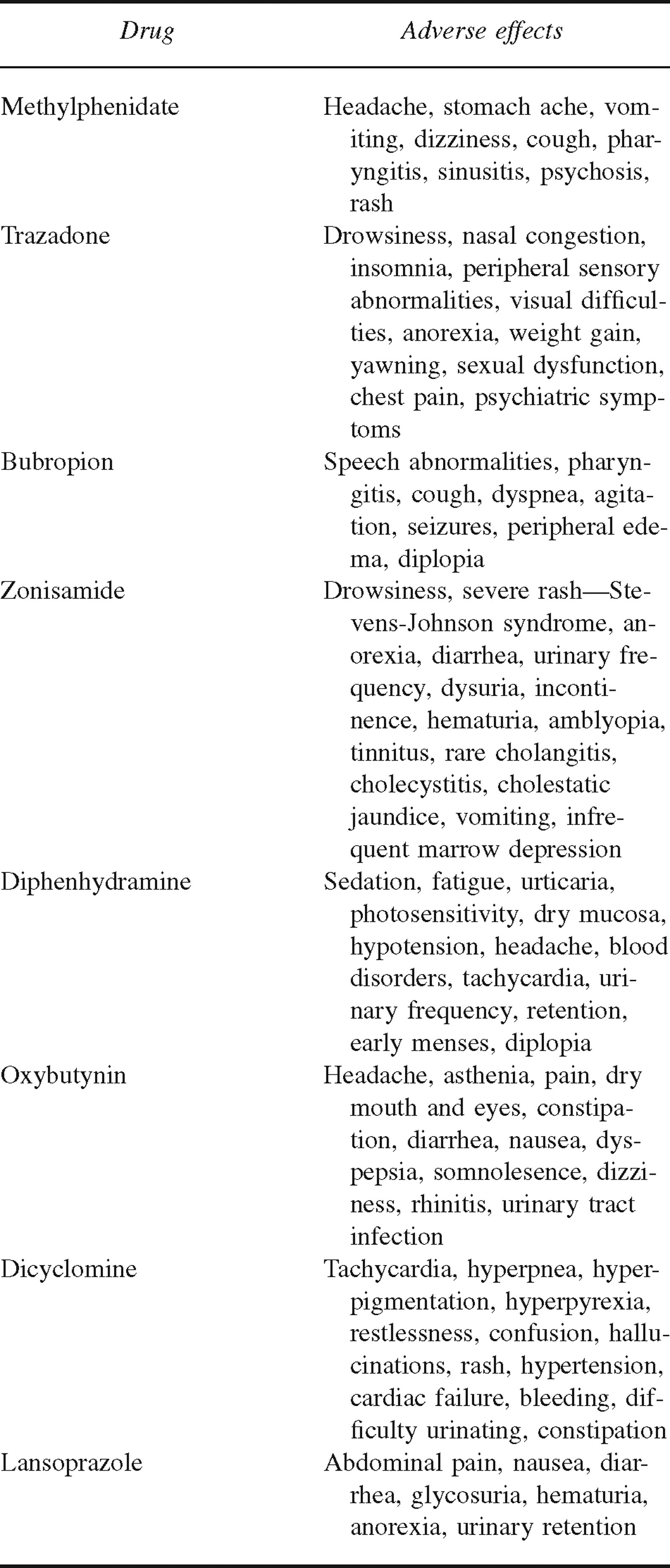
The patient had been receiving a combination of psychotropic medications regularly up until the morning of the sting (Table 1). The medications she received were not thought to be complicating factors, as several had been discontinued before symptom onset and others were stopped after the sting without improvement (Table 3). 5
Common adverse effects of drugs taken by the pa tient before and immediately after her sting
After 4½ months of frequently recurring right upper abdominal pain, the diagnosis of biliary dyskinesia was made. 6 This diagnosis was supported by the lack of evidence of gallstones, the normal liver function tests, and the finding of a nonfunctioning gallbladder upon scan. These data, coupled with the continual recurrence of gallbladder-type pain, resulted in a decision to perform a laparoscopic cholecystectomy. Intraoperative cholangiograms documented rapid free flow of bile into the duodenum without obstruction or filling defect. A previous upper gastrointestinal radiographic series was interpreted as no anatomic abnormality but trace gastroesophageal reflux. The operation successfully resolved the patient's pain. Pathological examination of the gallbladder revealed a hyperplastic epithelium, thickened muscularis mucosa and muscular wall, slight fibrosis, and no inflammation, which all indicated increased muscle contractility compatible with biliary dyskinesia.
During this period the patient had remedial bladder exercises, which to date (20 months) have resolved her incontinence. She was not capable of undergoing any interventional bladder diagnostic tests or therapy because of Asperger syndrome. At present, 2 years later, her health is as it was before the sting except that she is without a gallbladder and the Asperger syndrome has advanced to include 3 grand mal seizures in the past year.
Discussion
Toxic reactions to peripheral nerves and various muscular tissues after jellyfish stings are common, but massive local envenoming of the abdominal skin by a jellyfish antedating profound effects on viscera of the urinary and biliary tracts has not been previously reported. We hypothesize that the large area of tentacle-skin contact shown by the eruption permitted significant systemic venom uptake via vascular and lymphatic routes. The toxic substances circulated back to afflict the abdominal viscera. Indeed, the close temporal relationship between the sting and the visceral paralysis supports their cause-and-effect relationship.
The reason for the susceptibility here of the urinary bladder and gallbladder is unknown and awaits future elucidation. The urinary bladder and gallbladder are essentially smooth muscles with nerve and blood supply. Some ideas on the pathogenesis of the patient's disabilities in our case report may be discerned from past investigations on the effect of jellyfish venoms on various forms of nerves and muscle tissues as well as vascular flow.
Both autonomic and peripheral nerves can be damaged by coelenterate venoms.2,7,8 Clinical dysfunction of the autonomic nervous system from jellyfish venoms has been reported only once. 9 A 52-year-old Chinese fisherman was stung by an unidentified jellyfish on both thighs in August 1983 off Penang, Malaysia. Acutely he had dyspnea, cough, palpitations, and profuse lacrimation. Gastric enlargement with normal bowel sounds followed, but constipation and a nonemptying distended urinary bladder developed 2 hours after the sting and persisted for 2 to 3 days. Further indication of scattered autonomic injury was the fact that nocturnal erections were absent for nearly 1 week. The R-R interval (distance between two successive R-waves) on his electrocardiogram did not change during breathing or carotid stimulation, and lacrimation was depressed for 1 month.
Peripheral nerve damage with mononeuritis multiplex affecting skeletal muscle groups is well known after jellyfish stings and can require 4 to 6 months of convalescence. 8 On in vitro smooth muscle, jellyfish venoms directly introduced into a bathing medium have a more complicated biphasic effect, exhibiting spasm at lower doses and atonia at higher doses. 2 Several cases of smooth muscle symptoms after jellyfish envenomation have also been described, including 2 cases of paralytic ileus after jellyfish stings in Asia.10,11 In one of the cases, the gut paralysis occurred minutes after a left lower forearm sting and lasted 4 hours; in the other case, a wide sting on the arms, legs, and back resulted in ileus developing after 3 hours and persisting for 5 days.
Other sites of abnormal smooth muscle function after stings include several cases of vascular spasm at the injury sites that produced significant ischemia because of vascular wall closure 12 and an ophthalmological abnormality of prolonged blurred vision persisting for 1 week in a young woman. 13 This reaction could have been produced from autonomic nerve or smooth muscle impairment. Again, if smooth muscles were the target, the exact symptoms would be dose dependent, with lower doses producing spasm or increased activity and higher doses resulting in atonia as mentioned earlier. 2
We have reported an unusual case of possible smooth muscle or nerve dysfunction after an abdominal jellyfish sting. There has been a previous case of urinary bladder dysfunction induced by jellyfish venom, but there are no previously reported cases of gallbladder dysfunction. 9 In our case report, what makes the patient's sting dramatic is the florid cutaneous triggering eruption and its close temporal occurrence to massive visceral complications. Although these facts suggest a causal relationship between the sting and the abdominal abnormalities, definitive proof would depend upon future corroboration.
Footnotes
Acknowledgments
The authors wish to acknowledge the aid of Drs April Deng and John Petrali, Baltimore, MD, in interpreting the gallbladder specimens; Dr Henry W. Burnett of Winston-Salem, NC, and Drs Melissa L. Strogatz and Mark G. Burnett of Philadelphia, PA, for assistance with the planning and the manuscript; and Ms Anita Descault and Veronica Williford for some investigative work and preparation of the manuscript.